


Diseases of tongue
Classification of tongue
Aglossia and MicroglossiaMacroglossia
Ankyloglossia
Lingual varices
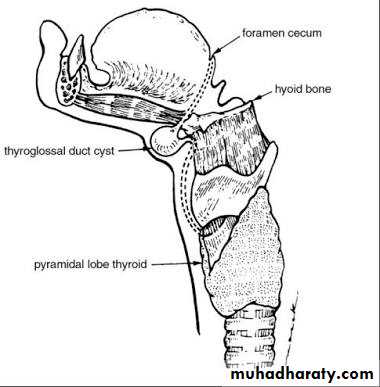
Lingual thyroid
Tongue thrusting
Cleft tongue
• Congenital


II. Depapilation of tongue
• Local disease:-• Traumatic injuries
• Allergic stomatits
• Chronic candidiasis
• Iron deficiency anemia
• Pernecious anemia
• Plummer-vinson’s syndrome
• Folic acid deficiency
• Diabetes
• Syphilis
• Zoster infection
• Neurological
• Glossodynia
• Paralysis

• Fissured tongue
Median rhomboid glossitisBenign migratory glossitis
Hairy tongue

IV. Cyst
Anterior median lingual cystBronchojenic cyst
Epidermoid and dermoid cyst
Gastric mucosal cyst
Thyroglossal duct cyst



V. Benign tumor
FibromaRhabdomyoma
Granular cell tumor
Leiyomyoma

VI. Premalignant lesions and conditions
Lichen planusOral submucous fibrosis
Leukoplakia


VII. Malignant tumors
Squamous cell carcinomaMalignant melanoma
Malignant lymphoma
Metastatic tumor
Sarcoma
VIII. Miscellaneous
Pigmentation of tongue



Developmental disorders
• Ankyloglossia:-• Fixation of tongue to the floor of mouth causing restricted movement
• Syndromes associated
• Robinow syndrome
• orofacial digital syndrome

• Aglossia:-
• This developmental condition is seen in rare conditions• This is mostly observed by complete absence of tongue
• Associated syndromes
• Adactylia syndrome of tongue with absence of digits

• Microglossia:-
• This is a rare disorder• There is tiny or rudimentary tongue development in oral cavity
• Size of tongue determines the growth and size of mandibular arch
• This disorder develops as an isolated case but in most cases it occurs in association with other congenital syndromes
• Oromandibular limb hypogenesis syndrome
• Hypoglosssia- hypodactylia syndrome
• Microglossia without limb deformity can occur but also with partial anodontia.
Normal size of tongue appears abnormally large
Occurs in maxillary retrusion restricted growth of nasopharynxLymphangioma restricted to the tongue or in continuity with cystic hygroma of the neck is most common cause
Can also occur in enlarged tonsil or adenosis
Habitual posturing of tongue
There is no real increase in bulk
Seen in cretinism(hypothyroidisim) and in happy puppet syndrome(Angelman syndrome)
Relative macroglossia
Apparent macroglossia
• Macroglossia:-
• Abnormally large tongue
Blockage of pharyngeal airway due to macroglossia result in obstruction sleep apnea
Treatment :-Removal of the cause
Surgical reduction or trimming maybe required
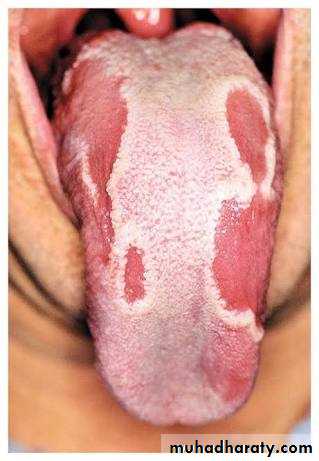
• Hairy tongue:-
It is unusual condition, which occurs due to hypertrophy of filliform papilla of tongue along with loss of normal desquamation processEtiology:-
poor oral hygiene
fungal infection
Heavy smoking
chronic illness
In extreme cases may produce a thick, leathery coating on tongue surface and this condition is often known as earthy encrusted tongue
Hypertrophid filliform papilla may grow up to ½cm long or up to 2cm.
In many cases it produces halitosis
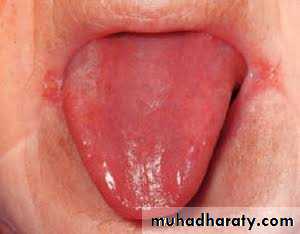
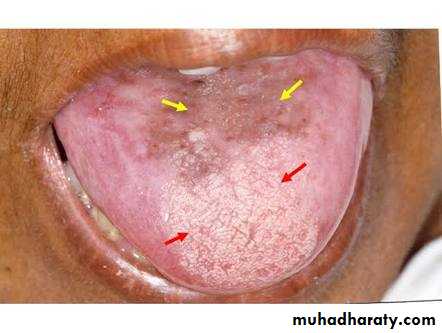
• Benign migratory glossitis (geographic tongue):-
• It is multifocal, partly irregular areas of depapilation of tongue• Characterized by frequent remission and recurrence
• Exact etiology is unknown
• Positive family history
• Female predilection is more
• Clinically present multiple, irregular, well demarcated, smooth partly erythematous areas on the dorsum of the tongue with desquamation of filliform papillae
• Mostly painless but in few occassions may produce glossodynia during taking spicy and citrus fruits
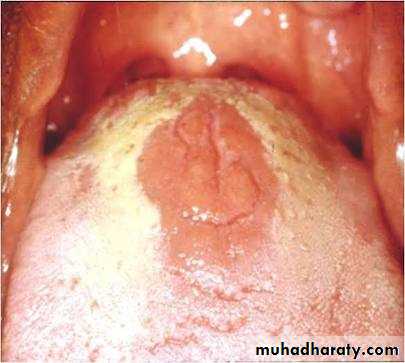
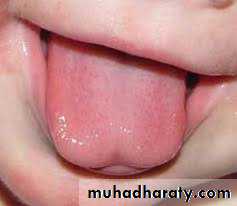
7. Median rhomboid glossitis:-
It is an asymptomatic, elongated, erythematous patch of atrophic mucosa on the middorsal surface of the tongueMostly seen among adults, rarely found in children
Site :- anterior to foramen caecum and circumvallet papillae
Lesion appears diamond or lozenges shaped
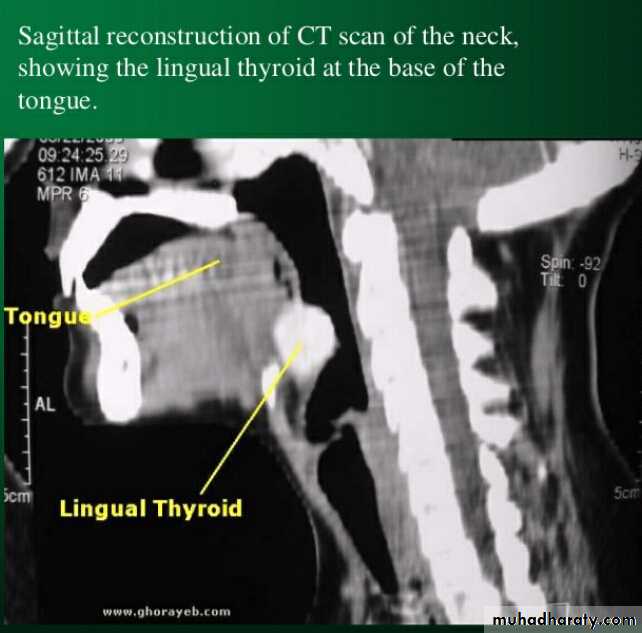
• Lingual thyroid nodule:-
• Dysphonia• Dysphagia
• Dyspnea
Treatment :- surgical excision

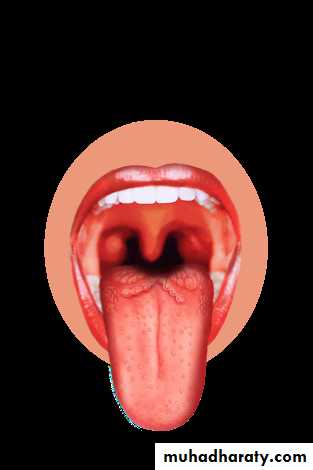
• Cleft tongue:-
• It develops usually due to partial or complete failure of union between two later lingual swellings during embryogenesis• In most cases it is asymptomatic condition sometimes irritation at the bottom of the cleft
• Cleft tongue may occur as a feature of orofacial digital syndrome.
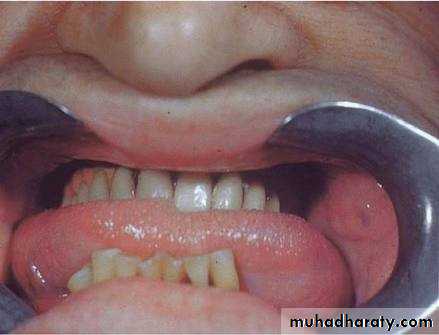
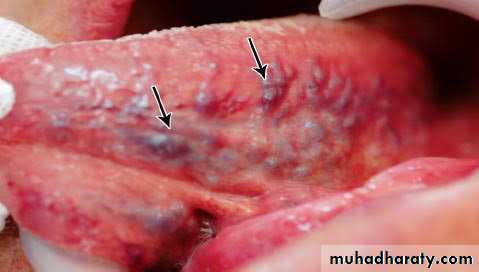
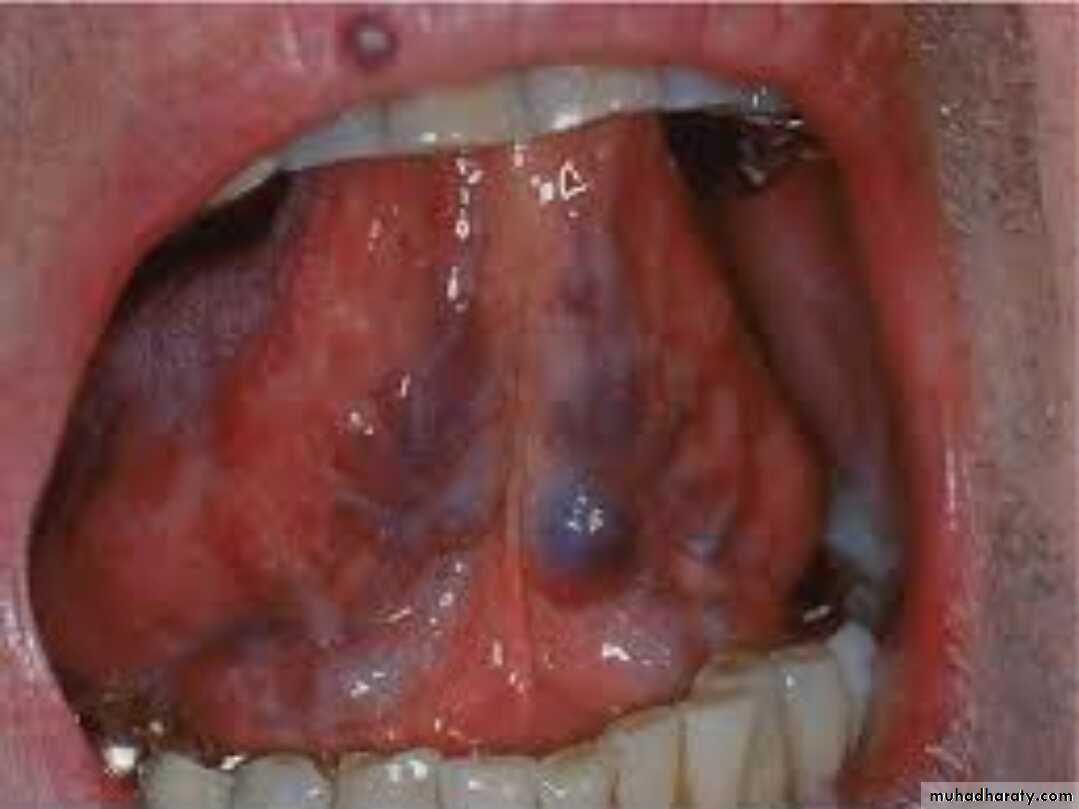
• Lingual varices:-
• Varix is a dilated, tortous vein which is often subjected to increased hydrostatic pressure but it is poorly supported by the surrounding tissue• Varicosities observed in location like ventral surface of tongue, floor of mouth, lip, buccal mucosa and commissure, etc.
• Clinically appears small round, purplish nodule, lateral to the sublingual vein which is usually also deflected
• Common among old age people.
• The lesion interestingly has no bleeding tendency either.
• Presence of lingual varices before the age of 50 indicates premature aging
• Treatment: no treatment is required
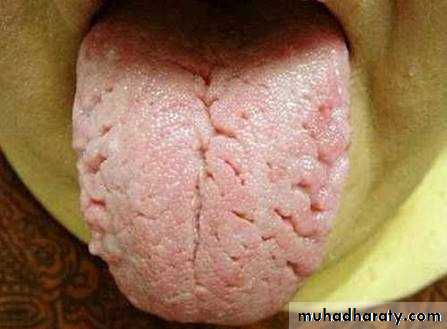
• Fissured tongue (scrotal tongue):-
• Congenital developmental malformation characterised by presence of numerous shallow or deep grooves (fissures)on dorsal and lateral surface of tongue.• Etiology:- exact etiology is unknown
genetic defect
vitamin deficiency
trauma
• it may be normal variation of tongue architecture.
• More common among males
• Average depth is 6mm
• Associated syndromes : Melkersson’s Rosenthal syndrome
• Treatment:- brushing of tongue to eliminate debris that irritate
• Iron deficiency Anemia:-
• Chronic microcytic hypochrmic type anemia• Atrophic glossits with patchy or diffuse loss or flattening of tongue papillae and glossodynia
• Tongue appears smooth, bald and red with glazed appearance it may be tender and having burning sensation
• A manifestation of iron deficiency anemia is Plummer Vinson syndrome.
• Pernicious Anemia:-
• Chronic pregressive megaloblastic anemia of adults and is caused by deficiency of an intrinsic factor in stomach• Glossitis :- inflammation of tongue
• Glossodynia:- burning sensation of tongue
• Glossopyrosis:- also used to describe burning sensation in the tongue
• Beefy red tongue with areas of patchy ulcerations on dorsum and lateral borders
• Sometimes, atrophy and inflammation of filliform papillae produce a bald appearance of tongue condition is known as hunter’s glossitis.
• Thyroglossal duct cyst:-
• Uncommon development cystic lesion arising from the embreyonic remnants of thyroglossal tract• Occurs primarily in children and young adults
• Neoplasm including carcinomas have been reported to develop from the cyst
• Cyst moves during swallowing
• Treatment:- surgical excision along with the tract.
• Rhabdomyoma:-
• Benign neoplasm of striated (skeletal) muscle and these are extremely rare• Often develops from the base of the tongue
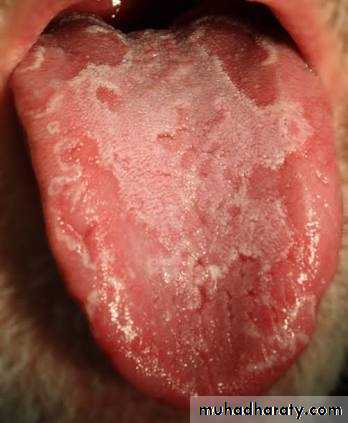
• Lichen planus:-
• It is a common chronic mucocutaneous disease, which probably arises due to abnormal immunological reaction the disease have some tendency to undergo malignant transformation• clinically exhibits numerous intrlacing white keartotic lines, which often produces typical lace like or annular pattern against any erythematous base
• A tiny white elevated dot like structure is frequently present at the intersection of white line called as striae of Wickmann
• Normally occur in bilaterally symmetrical pattern
• Treatment:- topical steroids- flucolinonide
• systemic administration- methyl prednisol

• Oral submucous fibrosis:-
• oral submucous fibrosis is the most predominant precancerous condition arising in the oral cavity, oropharynx, nasopharynx and oesophagus, etc.• The disease is characterized by juxta-epithelial inflammatory reaction in the oral mucosa , followed by a fibro-elastic transformation of the lamina propria leading to mucosal atrophy, rigidity and trismus.
• Burning sensation on in mouth particularly during taking hot and spicy food
• There can be excessive salivation or xerostomia
• Stiffness of lips, tongue which unables the patient to blow whistle or even
• Depapilation of tongue with recurrent or sometimes persistent glossitis
• Later on tongue becomes stiff and shows restricted movements
• Treatment:- stoppage of habbit
• extraction of 3rd molar• intralesional injection of collagenase
• corticosteroids
• fibrinolytic agents
• Leukoplakia:-
• It is a white patch or plaque which cannot be scrapped off or stripped off easily and which cannot be characterised clinically or pathologically as any other disease and it is not associated with any physical or chemical agent .• Etiology:- smoking
• syphilis
• sharp tooth
• sepsis
• spirit
• spices
• Confined to anterior 2/3rd of tongue and it gradually spreads on the dorsum of tongue
• Appearance:- fissured or cracked, due to contraction of underlying scarred tissue by chronic inflammation
• Sign:- affected areas of tongue shows milky-white patches with cracked fissures
• In course of time atrophy leads to hypertrophy
• The thickened papilla disappears and white membrane is worn off
• The surface becomes smooth and red

• Malignant:- squamous cell carcinoma
• 60% from the anterior 2/3rd of tongue and remainder from base• Etiology :- chronic physical and dental trauma
• alcohol
• tobacco smoke
• candidiasis
• syphilis
• sepsis
• Site:- lateral border
