Local and Regional Anesthesia
ByProf. Dr. Muneer S. Al-Badrany
Lectures in Veterinary Anesthesia
Muneer S. Al-Badrany
Types of anesthesia
Local analgesiaRegional analgesia
Surface application
Intra and subdermal infiltrationField analgesia
Perineural injection
Spinal block
Subararchnoid
epiduralPosterior
InteriorInhalation
General anesthesiaParental
Local AnestheticIt is an agent that interrupts pain impulses in specific region of the body without a loss of patient consciousness. Normally, the process is completely reversible

The Ideal Local Anesthetic
Water soluble/stable in solution
The action must be reversible
Should be rapid onset action
It should be stable
Can resterilization
− Non-irritating to nerve
− Low systemic toxicity
− It should have sufficient potency
− Adequate duration of action
− No post anesthetic side effects
− Vasoconstriction
Local anesthesia
Based on the DurationShort acting
Procaine(E)Chloroprocaine(E)
Benzocaine(E)
Medium acting
Lidocaine(A)
Mepivacaine(A)
Cocaine(E)
Long acting
Bupivacaine(A)
Etidocaine(A)
Ropivacaine(A)
Tetracaine(E)
Or Amithocaine
Local Anesthesia classification
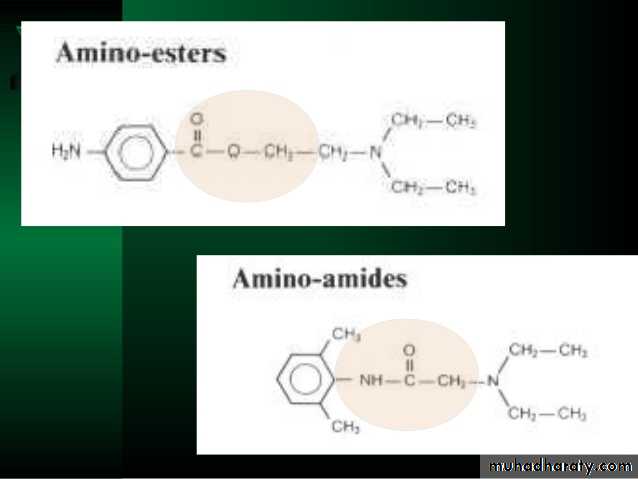
esters
amides
based on their chemical structure.
Lignocain
bupivacaine
procaine
Amides are metabolized by hepatic enzymes
the esters are broken down by plasma cholinesterase, an enzyme produced by the liver
Many local anaesthetics produce vasodilation, which increases the speed of uptake of these drugs into the bloodstream, reducing their efficacy at the site of administration, and also potentially increasing their toxic side effects.
Consequently, local anaesthetics are commonly combined with a vasoconstrictor – usually adrenaline – to maintain their concentration at the administration site.
Local analgesic agents may be applied directly into the eye (conjunctiva), onto mucous membranes (larynx, urethra, nasal passages) or onto the skin, including
the external ear canal.
Proxymetacaine may be used on the eye (e.g. to allow
removal of a foreign body) or
lignocaine gel or spray on the mucous membranes
(e.g. to facilitate endotracheal intubation in cats).
Local anaesthetic creams,
for example, EMLA® cream, may be applied to the skin before intravenous catheterisation .
Topical or surface application
Splash’ blocks
Local anaesthetics are flooded or dripped onto surgical sites and wounds at the end of a procedure.Intra-articular or synovial blocks
Local anaesthetics (or opioids) are instilled into the affected joint cavity following surgery. Intra-articular blocks are used commonly in horses to aid in the diagnosis of lamenessThe intradermal or subdermal tissues are infi ltrated by injection with a local anaesthetic agent.
This is useful only for minor procedures, and normally sedation and/ or manual restraint are also required.
Local toxicity may delay tissue healing.
Infi ltration of local anaesthetic agents can be used to produce linear blocks,
ring blocks
and field blocks.
These techniques are more commonly used in large
animals such as cattle and sheep.
Local infiltration
A local anaesthetic agent is injected directly around a nerve, for example
Perineural infiltrationHead
Supra orbital NB
Upper eye lids
Infraorbital NB
Master muscle, Upper lips, Nostrils
Mental NB
Lowe lips, Inscier teeth
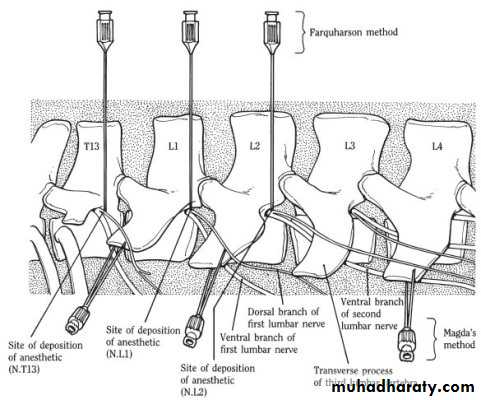
Trunk
Paravertebral NB
T13, L1, L2, L3
Limbs
Fore limbs
Low volar
High volar
Median
Ulnar
Hind limbs
Low planter
High planter
Posterior tibial
EPIDURAL INJECTION SITES
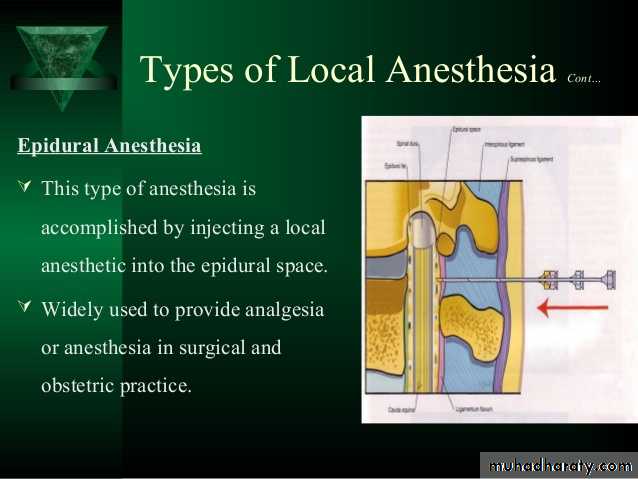
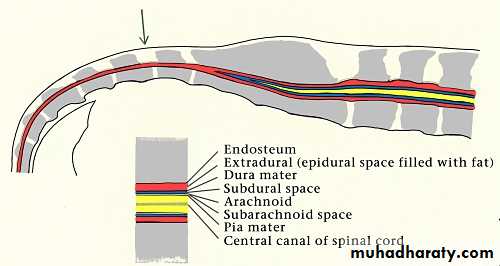
The lumbosacral intervertebral space is the most common location for epidural injection in small animals. Located between the vertebral periosteum and the dura mater, this space contains nerves of the cauda equina, fat, blood vessels, lymphatics, and, in some species, the end of the spinal cord with the remaining meninges (pia and arachnoid mater).
Access to the lumbosacral intervertebral space involves inserting a spinal needle through skin, subcutaneous fascia, and the ligamentum flavum, which forms the dorsal wall of the epidural space in dogs and cats. Below the dura mater lay the arachnoid mater and the pia mater. The subarachnoid space contains cerebrospinal fluid (CSF); injection into the subarachnoid space is referred to as intrathecal or spinal injection and typically is not purposefully performed in small animals. Thoracic epidural injections are used with some frequency in people and have been described in veterinary species but are not commonly used in dogs and cats.
Lumbosacral epidural anesthesia with local anesthetics provides complete anesthesia to the caudal half of the body by blocking the intradural spinal nerve roots and the peripheral layer of the spinal cord.1 This technique is useful for pelvic and hindlimb orthopedic procedures, perineal and anal surgeries, exploratory laparotomy, and cesarean section. In addition to complete anesthesia, at least some sympathetic and motor blockade is produced with local anesthetics. Lidocaine, mepivacaine, and bupivacaine consistently cause motor blockade, while motor blockade is less intense and of shorter duration with levobupivacaine and ropivacaine. The duration of motor blockade is generally shorter than the duration of analgesia, and, depending on the procedure and local anesthetic chosen, motor function usually returns by the time a patient recovers from anesthesia.1-3
Perform epidural injections in heavily sedated or anesthetized animals. The injection site is usually at the lumbosacral space in dogs and cats and can be performed with a patient in either sternal or lateral recumbency.
TECHNIQUE
• Epidural injection is easier to achieve with the patient in sternal recumbency, with the hindlimbs flexed at the hips and stifles and hocks extended so the legs are positioned alongside the body. This position makes the lumbosacral space easier to identify.

Position the patient

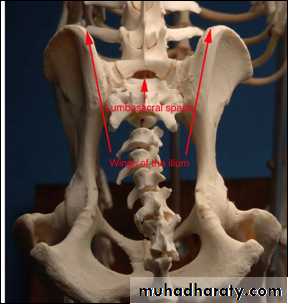
Locate the lumbosacral space by palpating the most anterior aspect of both iliac crests with your thumb and middle finger; the imaginary line connecting them passes through the lumbosacral intervertebral space. With your index finger, palpate the space as a depression immediately caudal to the dorsal spinous process of L7 and immediately cranial to the fuse
Once you have identified the lumbosacral space,
clip the hair, andsurgically prepare the area.
Place a sterile transparent drape over the area,
tear a small opening in the drape at the injection site, and use a sterile disposable 2.5- to 7.5-cm, 20- to 22-ga spinal needle and sterile gloves.
If the procedure is being performed in an awake but sedated patient, inject 0.5 to 1 ml 2% lidocaine (with sodium bicarbonate solution added to the local anesthetic in a 1:9 ratio of bicarbonate to lidocaine to reduce the pain of injection) subcutaneously at the site of the spinal needle insertion and wait five to 10 minutes before inserting the spinal needle at this site.
Prepare the site
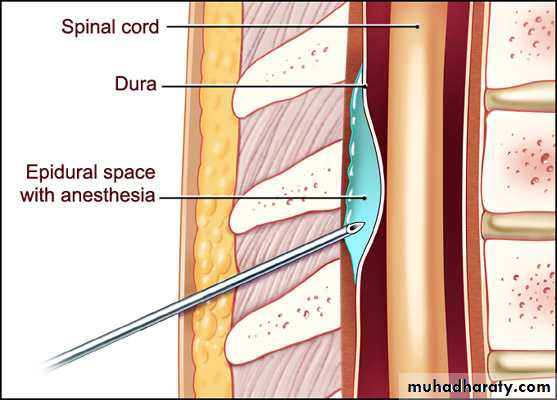
• Insert the needle
• Using your nondominant hand to confirm the landmarks and the lumbosacral space, position the spinal needle over the midline with your dominant hand . Midline positioning is critical to avoid contact with the transverse processes of the L7 vertebra. Direct the needle bevel cranially, and advance the needle, with stylet in place, perpendicular to the skin. Position your dominant hand so that it is in contact with the animal when penetrating the skin to provide counterpressure and to avoid pushing the needle in too far.
. It is often helpful to hold the stylet with the index finger of your dominant hand to keep it from being pushed out of the spinal needle by the subcutaneous tissues. If the needle encounters bone, withdraw it slightly, redirect it caudally or cranially, and advance it again. You may need to adjust the needle angle to facilitate correct placement in the epidural space
The diameter of the lumbosacral epidural space is 2 to 4 mm in medium-sized dogs and < 3 mm in cats.
As the needle is advanced, you usually feel a popping sensation as the skin is penetrated and then a second pop as the needle penetrates the ligamentum flavum and enters the epidural space.
Advance the needle no farther since most of the blood vessels lie in the ventral part of the spinal canal and it is more likely that a vessel will be penetrated if advanced too far.
Occasionally, you will see the tail twitch or hindlimb movement as the epidural space is entered, indicating the needle has contacted the cauda equina. In this case, the drug may be injected without redirecting the needle.
In cats, the spinal dura mater frequently extends to S1-S2, so it is more likely that the dura and arachnoid will be punctured if the needle is advanced too deeply, entering the subarachnoid space.
Once the epidural space has been entered, remove the stylet, and inspect the hub for blood or CSF.
If you see blood, a venous sinus has been penetrated and the needle should be withdrawn and repositioned.
If CSF is present, you have entered the subarachnoid space and can withdraw or reposition the needle or, alternatively, inject one-fourth to one-half of the calculated volume of the drug.
The maximum dose of local anesthetic that can be administered spinally (intrathecally) is < 1 ml/10 kg, and only preservative-free drugs should be injected spinally.4
Confirm needle placement

if no blood or CSF is observed in the hub, inject a test dose of 0.5 to 1 ml of air or saline solution with a sterile syringe to check for resistance to injection (Figure 4). In our practice, we use glass syringes because they provide less resistance to injection; however, plastic syringes may be used. If the epidural space has been correctly entered, there should be no resistance to injection of the air or saline solution. If the plunger pushes back, the needle has not been correctly positioned.
If the epidural injection of a local anesthetic is successful, relaxation of the external anal sphincter and tail is observed. In an awake patient, hindlimb ataxia, as well as a lack of response to the flexor pinch reflex of the pelvic limbs, develops. Generally, once the toe reflexes have disappeared, anesthesia adequate for abdominal surgery is present. In anesthetized patients, a lack of response to surgical stimulation, as well as a lower requirement of inhalant anesthesia to maintain surgical anesthesia, is a good indicator of a successful local anesthetic epidural. Patients receiving epidural opioids alone will still respond to acute pain stimuli and will not exhibit muscle relaxation. Epidural opioid administration often results in reduced requirement for supplemental analgesics in awake patients and reduced requirement for volatile anesthetics in anesthetized patients.
Observe patient response

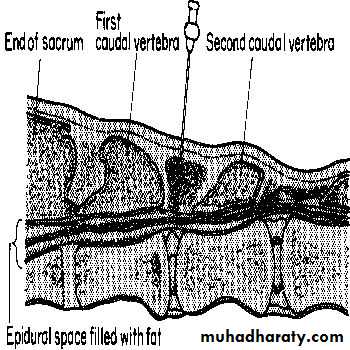
Caudal epidural anaesthesia involves injection of local anaesthetic and/or other appropriate drugs into the epidural space at the sacro-coccygeal or first intercoccygeal junction in order to produce analgesia of the tail, perineum, genitalia and pelvic viscera.
• Locate the first intercoccygeal space by either:
• Raising and lowering the tail and palpating the depression and movement between the first and second coccygeal vertebrae: the first intercoccygeal space is the first obvious articulation caudal to the sacrum.• Or Standing to one side of the animal, along the line of the croup observe the prominence of the sacrum and caudal to this the next prominence which is the spine of the first coccygeal vertebra; the first intervertebral space is the depression immediately behind this prominence.
or
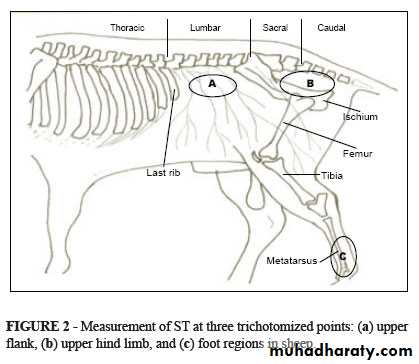
Palpate the caudal prominence of the tuberosity of the ischium and move about 10-11 cm forwards in a medium sized cow. A line drawn over the animal at this point will pass through the depression between the first and second coccygeal spines. (

• Anatomy of the epidural space:
• The epidural space has a large amount of epidural fat that is inside the vertebral bone column. Even with a short period of weight loss the amount of epidural fat will not be affected. The spinal cord is surrounded by the meninges with the pia mater adhered to the spinal cord. The arachnoid and the dura mater are a combined layer, placing the cerebrospinal fluid between the pia mater and the arachnoid/dural layer. There is a venous plexus on the ventral floor of the vertebral column that will occasionally be entered. The vertebral level at which the cord and the dural sac (meningeal layers) end is variable in the dog, cat and horse. In the dog the cord ends at L6-L7 and the dural sac at L7-S2. In the cat, they usually end further caudally (about one more vertebra). In the horse, they end at the location of S2The indication is to provide analgesia and anesthesia caudal to the diaphragm. It is an excellent means to provide anesthesia and analgesia to the pelvis, pelvic limbs and perineum. In all species, anesthesia is utilized with local anesthetics administered in such volumes that they inactivate action potentials in the spinal cord caudal to the branching of the sciatic and femoral nerves. Analgesia, on the other hand, may include local anesthesia, but it has a much broader application.
Indications:
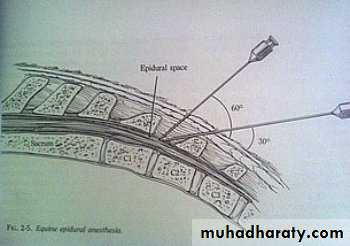
Equine Technique:
Caudal (low) epidural is the most common technique performed in equine patients. Crainal (high) epidurals are contraindicated. The volume of fluid to be injected like in small animals, should be kept to a minimum, in order to minimize effects of motor control of the patient. The technique is similar to the technique in the bovine patient. Injection is through the space between the first and second coccygeal vertebrae or the sacrocaudal (first intercoccygeal) vertebral space. In general, this is usually cranial to the long tail hairs. .A divot can be palpated in this region with your thumb or index finger while moving the tail up and down with the opposite hand After preparing the area in routine sterile fashion, a skin bleb is made to allow location and entry of the needle. The hanging drop technique can be used in equine patients as well when performing an epidural block. An 18-20 gauge, 3 inch spinal needle is preferred. The needle can be inserted at a 30-60 degree angle from the perpendicular line through the vertebrae. Generally, a volume of 3-7 mls of local anesthetic/analgesic agent is infused.
Additionally, a continuous epidural catheter can be placed in similar format using a commercial epidural catheter kit for treatment of long-standing or chronic pain conditions in the hindlimbs