DISORDERS OF THE SPINAL NERVES AND SPINAL CORD
DR. BASHAR SHAKER
Medicine
-The spinal cord and spinal roots may be affected by intrinsic disease or by disorders of the
surrounding meninges and bones.
-The clinical presentation of these conditions depends on the anatomical level at which the cord
or roots are affected, as well as the nature of the pathological process involved.
-It is important to recognize when emergency surgical intervention is necessary and to plan
investigations to identify such patients.
COMPRESSION OF THE SPINAL CORD
-Acute spinal cord compression is one of the most common neurological emergencies
encountered in clinical practice.
-A space-occupying lesion within the spinal canal may damage nerve tissue either directly by
pressure or indirectly by interfering with blood supply.
-Oedema from venous obstruction impairs neuronal function, and ischaemia from arterial
obstruction may lead to necrosis of the spinal cord.
-The early stages of damage are reversible but severely damaged neurons do not recover; hence
the importance of early diagnosis and treatment.
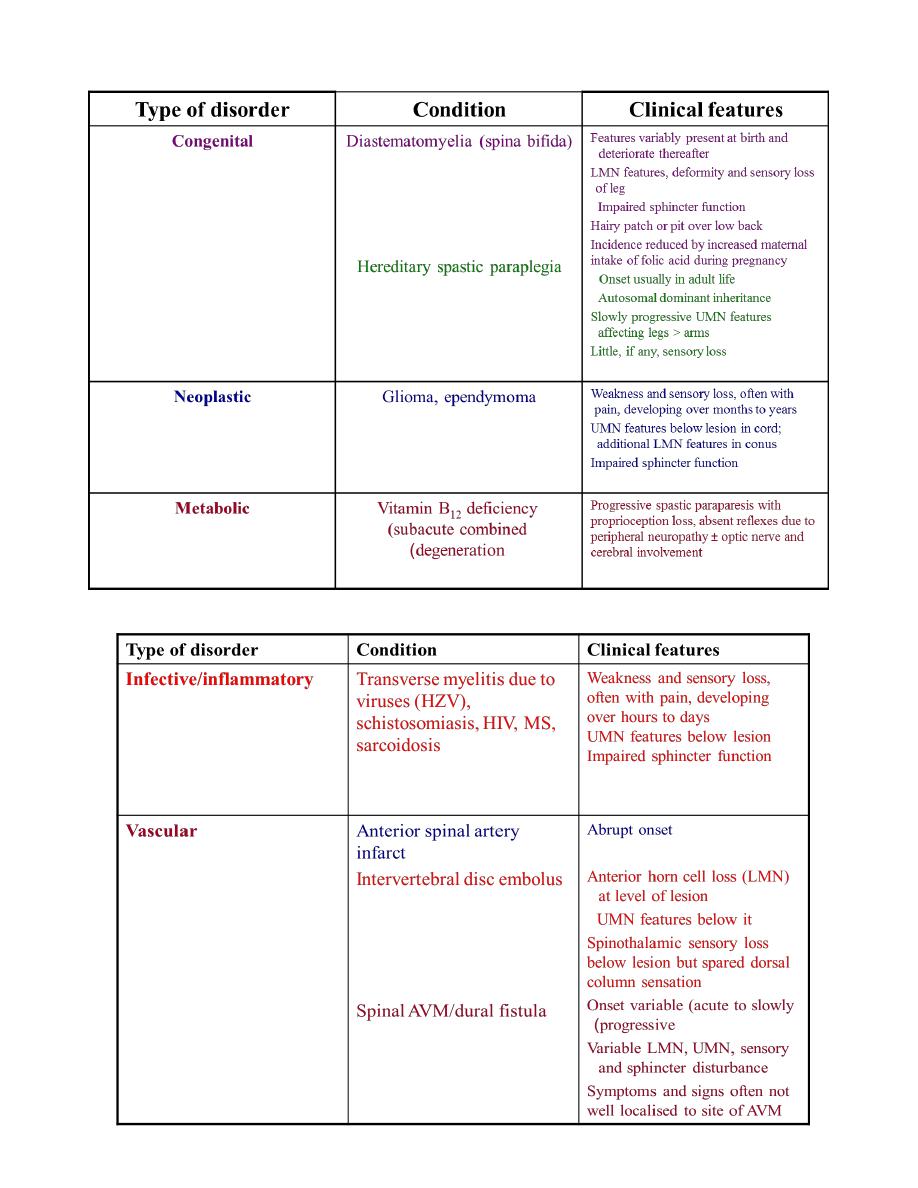
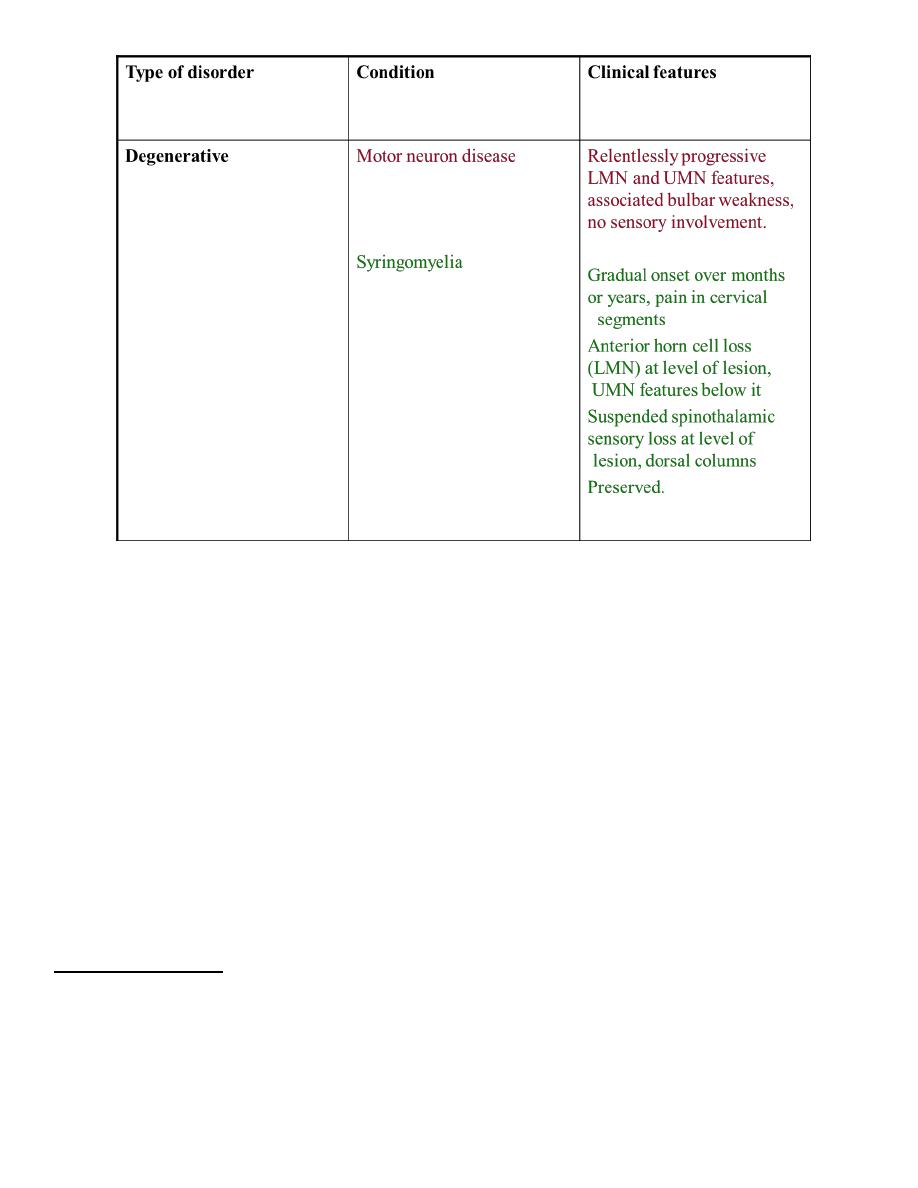
CAUSES
Clinical features
The onset of symptoms of spinal cord compression is usually slow (over weeks), but can be
acute as a result of trauma or metastases, especially if there is associated arterial occlusion.
SYMPTOMS
Pain Localised over the spine or in a root distribution, which may be aggravated by
coughing, sneezing or straining
Sensory Paraesthesia, numbness or cold sensations, especially in the lower limbs,
which spread proximally, often to a level on the trunk
Motor Weakness, heaviness or stiffness of the limbs, most commonly the legs
Sphincters Urgency or hesitancy of micturition, leading eventually to urinary
retention
-Pain and sensory symptoms occur early, while weakness and sphincter dysfunction are usually
late manifestations.
-The signs vary according to the level of the cord compression and the structures involved.
-There may be tenderness to percussion over the spine if there is vertebral disease, and this may
be associated with a local kyphosis.
-Involvement of the roots at the level of the compression may cause dermatomal sensory
impairment and corresponding lower motor signs.
-Interruption of fibres in the spinal cord causes sensory loss
SIGNS
Cervical, above C5
Upper motor neuron signs and sensory loss in all four limbs
Diaphragm weakness (phrenic nerve)
Cervical, C5 to T1
Lower motor neuron signs and segmental sensory loss in the arms; upper motor neuron
signs in the legs
Respiratory (intercostal) muscle weakness
Thoracic cord
Spastic paraplegia with a sensory level on the trunk
Conus medullaris
Lesions at the end of the spinal cord cause sacral loss of sensation and extensor plantar
responses
Cauda equina
Spinal cord ends at approximately the T12/L1 spinal level and spinal lesions below this
level can only cause lower motor neuron signs by affecting the cauda equina
INVESTIGATION OF ACUTE SPINAL CORD SYNDROME
1. Plain X-rays of spine may show bony destruction and soft-tissue abnormalities and are
an essential initial investigation
2. Chest X-rays may provide evidence of systemic disease
3. MRI of spine is the investigation of choice; myelography also localises the lesion and,
with CT in suitable cases, defines the extent of compression and associated soft-tissue
abnormality
4. CSF should be taken for analysis at the time of myelography. In cases of complete spinal
block this shows a normal cell count with a very elevated protein causing yellow
discoloration of the fluid (Froin's syndrome). Acute deterioration may develop after
myelography and the neurosurgeons should be alerted before it is undertaken.
5. Serum B
12
6. Needle biopsy is required prior to radiotherapy to establish the histological nature of the
tumour.
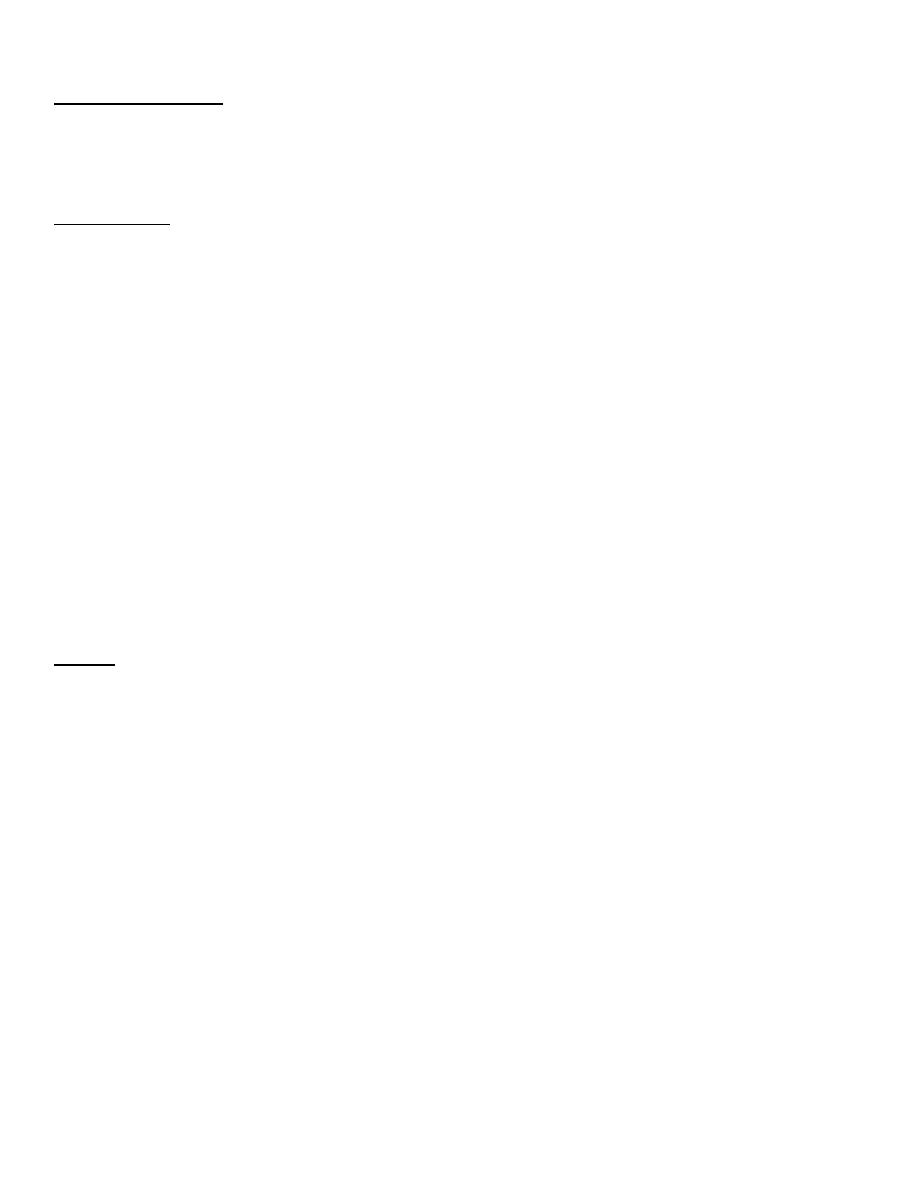
Loss of vertebral pedicle (arrow) by bony
erosion of an osteolytic metastasis ------ >
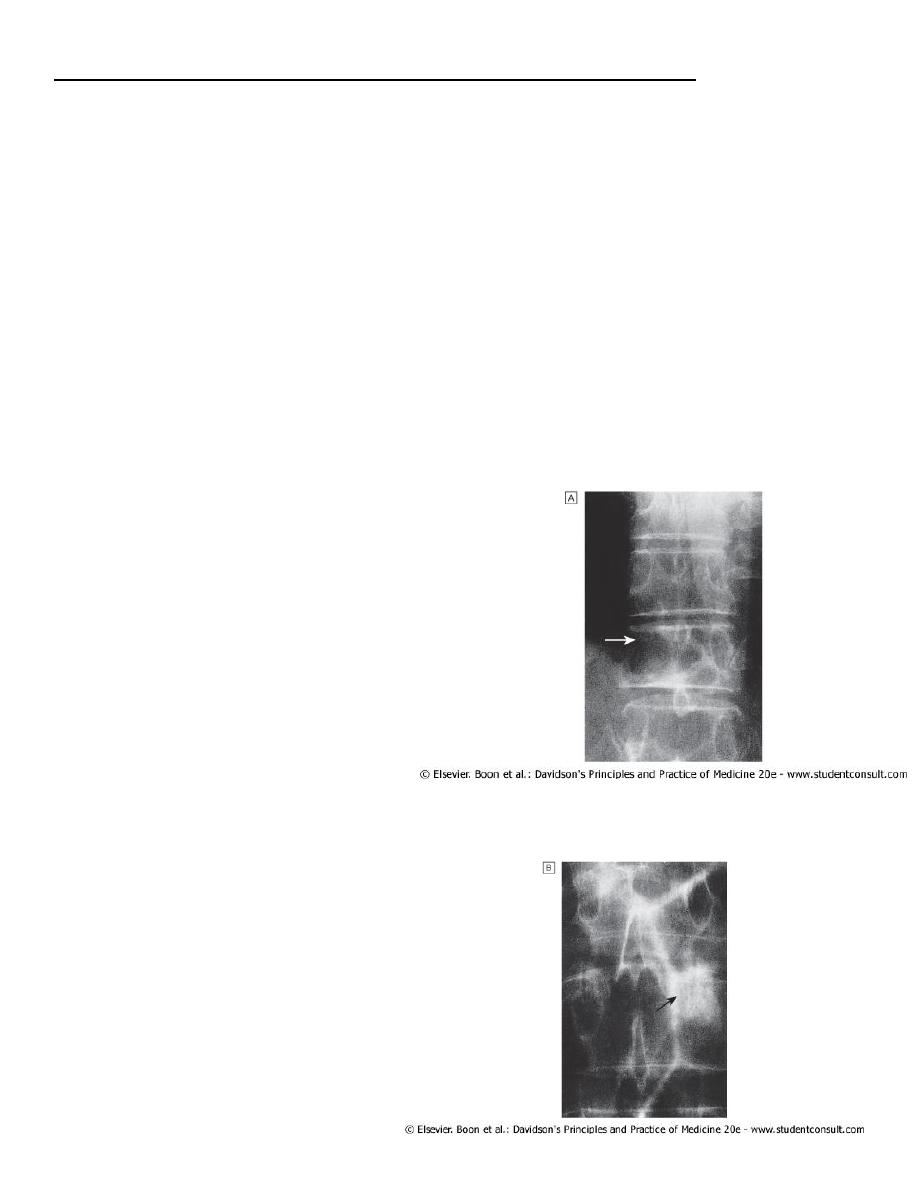
An osteosclerotic metastasis ------- >
Management
Treatment and prognosis depend on the nature of the underlying lesion.
Benign tumours should be surgically excised, and a good functional recovery can be
expected unless a marked neurological deficit has developed before diagnosis.
Extradural compression due to malignancy is the most common cause of spinal cord
compression in developed countries and has a poor prognosis, although useful function
can be regained if treatment is initiated within 24 hours of the onset of severe weakness
or sphincter dysfunction.
Surgical decompression may be appropriate in some patients, but has a similar outcome
to radiotherapy.
Spinal cord compression due to tuberculosis is common in some areas of the world, and
requires surgical treatment if seen early. This should be followed by appropriate anti-
tuberculous chemotherapy for an extended period.
Traumatic lesions of the vertebral column require specialised neurosurgical treatment.
INTRINSIC DISEASES OF THE SPINAL CORD
CERVICAL SPONDYLOSIS
-In the cervical spine, some degree of osteoarthritic degenerative change is a normal
radiological finding in the middle-aged and elderly.
-Degeneration of the intervertebral discs and secondary osteoarthrosis (cervical spondylosis) is
often asymptomatic, but may be associated with neurological dysfunction.
-The C5/6, C6/7 and C4/5 vertebral levels and C6, C7 and C5 roots, respectively, are most
commonly affected
CERVICAL SPONDYLOTIC RADICULOPATHY
Compression of a nerve root occurs when a disc prolapses laterally, which may develop acutely
or more gradually due to osteophytic encroachment of the intervertebral foramina.
Clinical features
-The patient complains of pain in the neck that may radiate in the distribution of the affected
nerve root.
-The neck is held rigidly and neck movements may exacerbate pain.
- Paraesthesia and sensory loss may be found in the affected segment and there may be lower
motor neuron signs, including weakness, wasting and reflex impairment
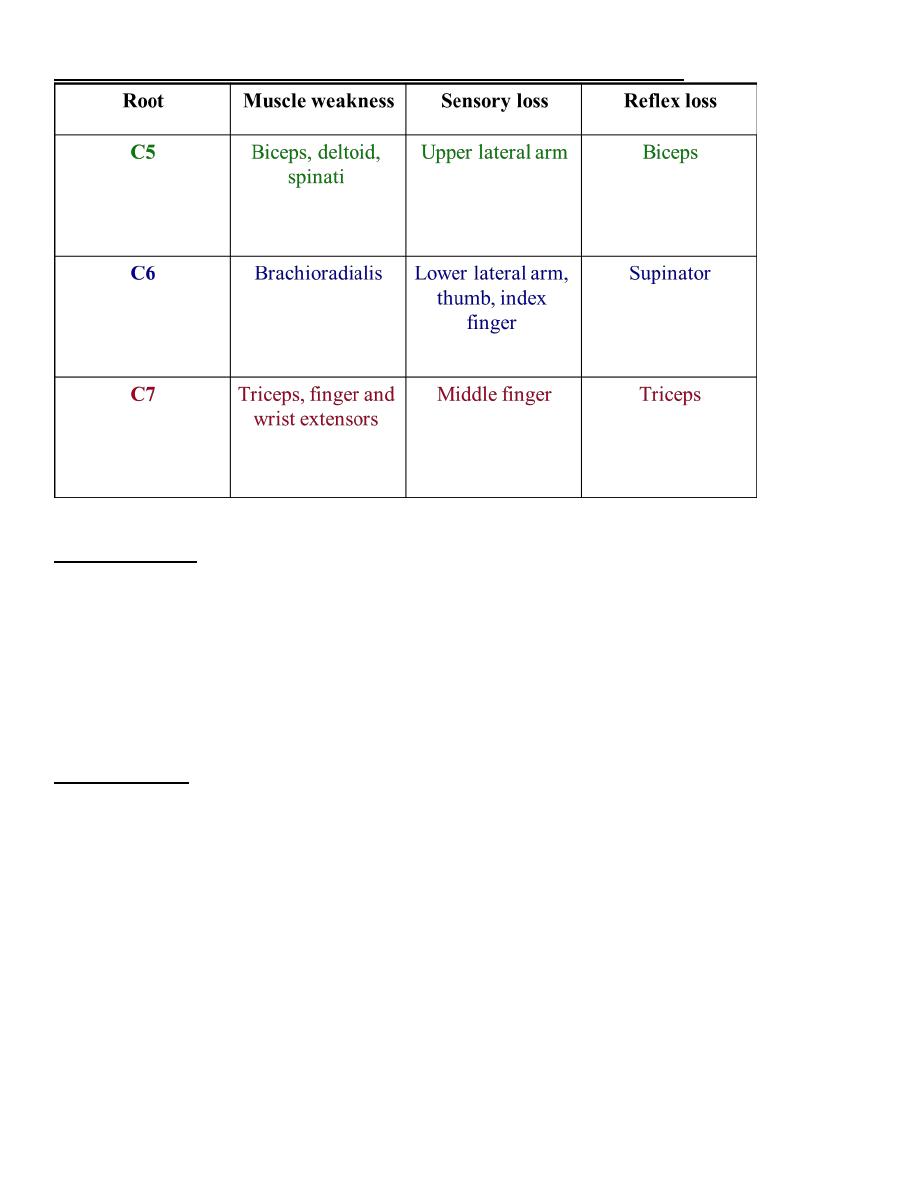
PHYSICAL SIGNS IN CERVICAL ROOT COMPRESSION
Investigations
1. Plain X-rays, including lateral and oblique views, should be obtained to confirm the
presence of degenerative changes and to exclude other conditions, including destructive
lesions.
2. If surgery is contemplated, MRI is required.
3. Electrophysiological studies rarely add to the clinical examination, but may be necessary
if there is doubt about the differential diagnosis between root and peripheral nerve
lesions.
Management
Conservative treatment with analgesics and physiotherapy results in resolution of symptoms in
the great majority of patients, but a few require surgery in the form of foraminotomy or disc
excision.
CERVICAL SPONDYLOTIC MYELOPATHY
Dorsomedial herniation of a disc and the development of transverse bony bars or posterior
osteophytes may result in pressure on the spinal cord or the anterior spinal artery which supplies
the anterior twothirds of the cord
Clinical features
-The onset is usually insidious and painless, but acute deterioration may occur after trauma,
especially hyperextension injury.
-Upper motor neuron signs develop in the limbs, with spasticity of the legs usually appearing
before the arms are involved. Sensory loss in the upper limbs is common, producing tingling,
numbness and proprioception loss in the hands, with progressive clumsiness.
-Sensory manifestations in the legs are much less common.
-The neurological deficit usually progresses gradually and disturbance of micturition is a very
late feature .
Investigations
-Plain X-rays confirm the presence of degenerative changes, and MRI or myelography may be
indicated if surgical treatment is being considered.
-MRI may also show areas of high signal within the spinal cord at the level of compression.
-Imaging of the cervical spine should be considered if there is diagnostic doubt or if surgery is
contemplated.
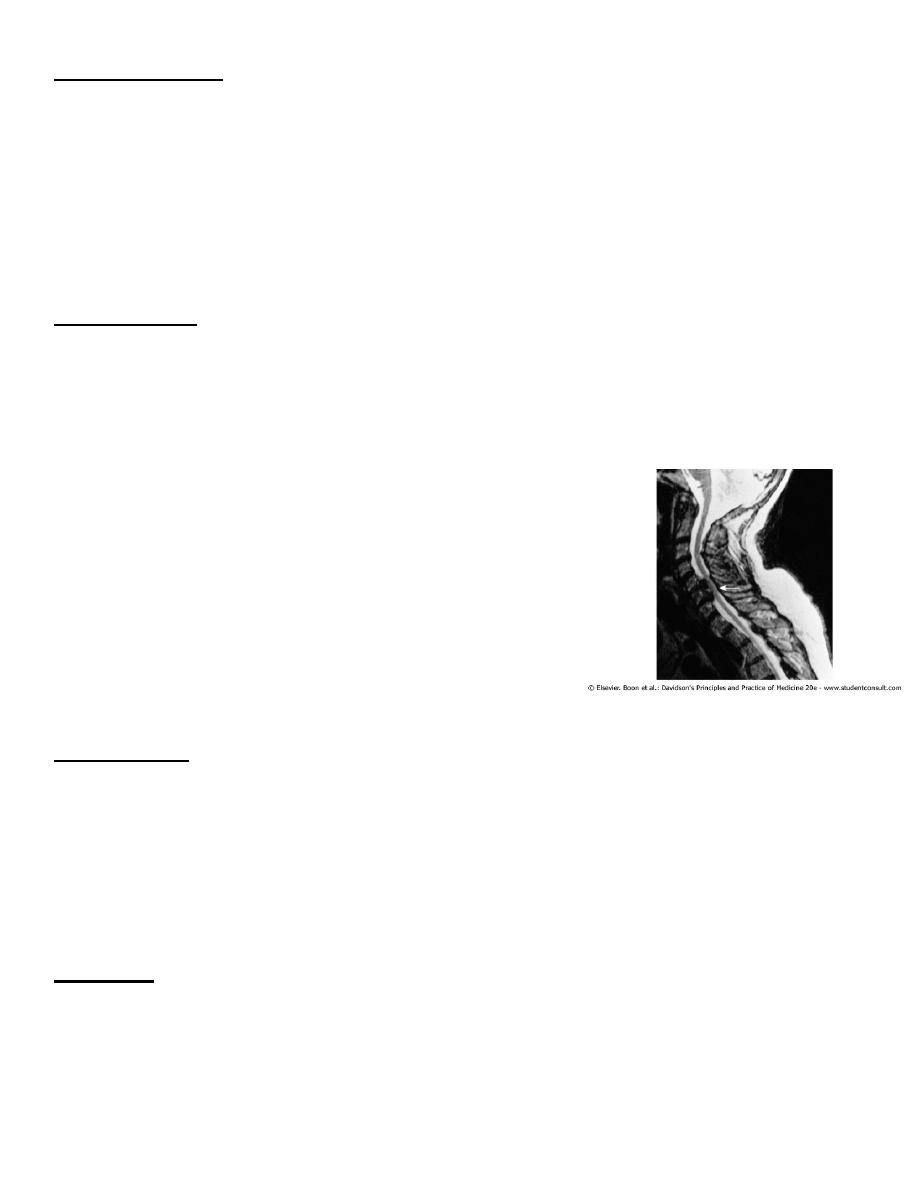
MRI showing cervical cord compression (arrow) in cervical
spondylosis ------- >
Management
- Surgical procedures, including laminectomy and anterior discectomy, may arrest progression
of disability but may not result in neurological improvement.
- The judgement on whether surgery should be undertaken may be difficult.
- Manipulation of the cervical spine is of no proven benefit and may precipitate acute
neurological deterioration.
Prognosis
The prognosis of cervical myelopathy is variable. In many patients the condition stabilises or
even improves without intervention, but if progressive disability does develop, surgical
decompression should be considered.
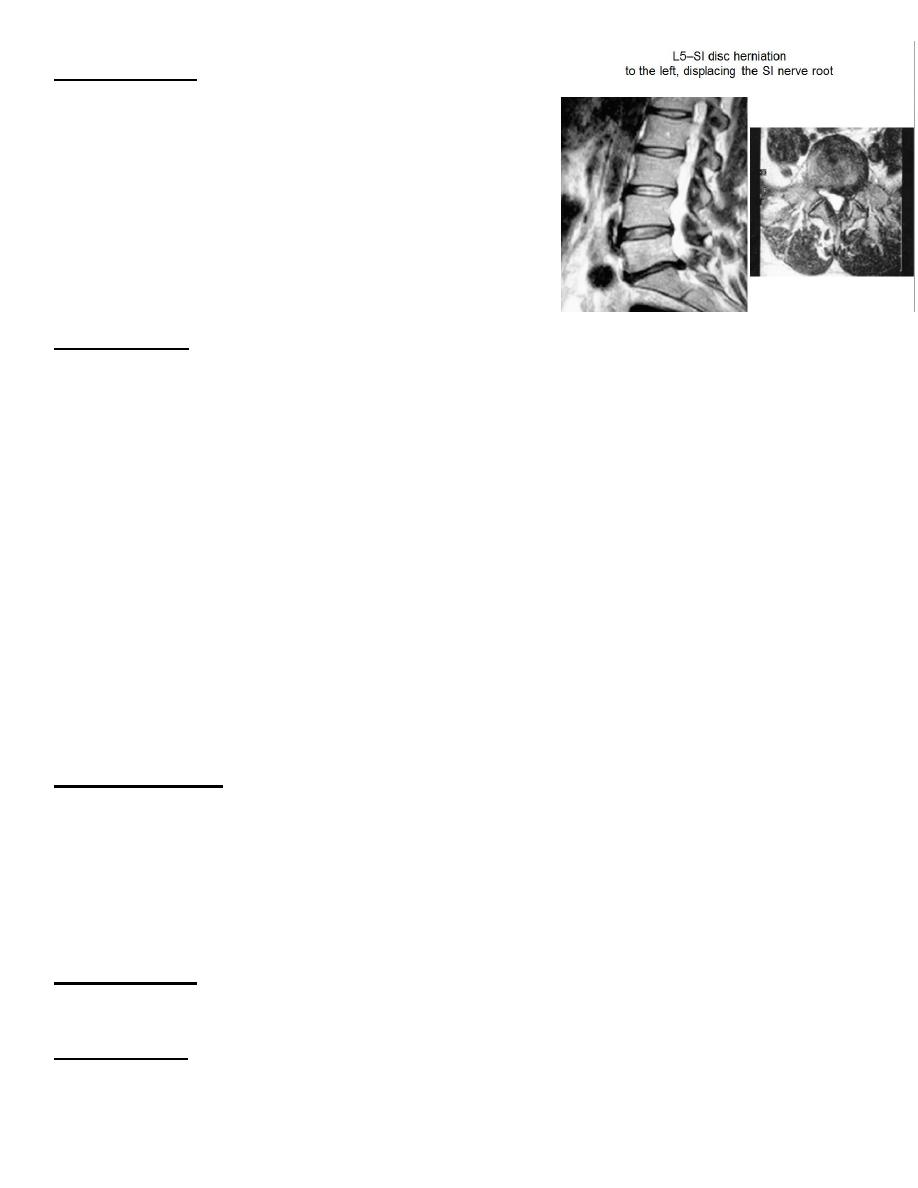
LUMBAR DISC HERNIATION
-Acute lumbar disc herniation is often precipitated by trauma, usually by lifting heavy weights
while the spine is flexed.
-The nucleus pulposus may bulge or rupture through the annulus fibrosus, giving rise to
pressure on nerve endings in the spinal ligaments, changes in the vertebral joints or pressure on
nerve roots.
Clinical features
The onset may be sudden or gradual. Alternatively, repeated episodes of low back pain may
precede sciatica by months or years. Constant aching pain is felt in the lumbar region and may
radiate to the buttock, thigh, calf and foot. Pain is exacerbated by coughing or straining but may
be relieved by lying flat.
The altered mechanics of the lumbar spine result in loss of lumbar lordosis and there may be
spasm of the paraspinal musculature. Root pressure is suggested by limitation of flexion of the
hip on the affected side if the straight leg is raised (Lasègue's sign). If the third or fourth lumbar
roots are involved, Lasègue's sign may be negative, but pain in the back may be induced by
hyperextension of the hip (femoral nerve stretch test).
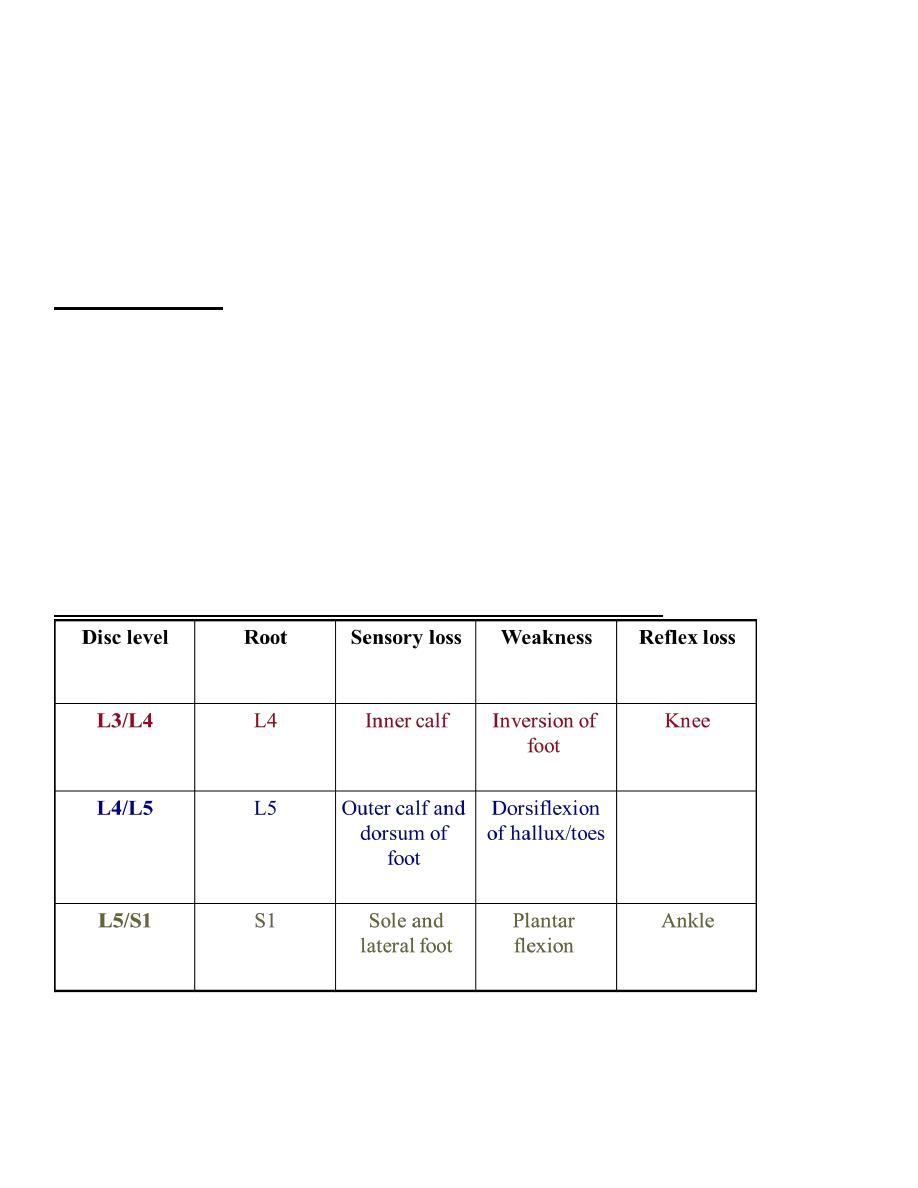
PHYSICAL SIGNS IN LUMBAR ROOT COMPRESSION
Investigations
- Plain X-rays of the lumbar spine are of little
value in the diagnosis of lumbar disc disease,
although they may show other conditions such as
malignant infiltration of a vertebral body.
- CT, especially using spiral scanning techniques,
can provide helpful images of the disc protrusion
and/or narrowing of the exit foramina.
- MRI is the investigation of choice if available,
since soft tissues are well imaged.
Management
- Some 90% of patients with sciatica recover with conservative treatment with analgesia
and early mobilisation; bed rest does not help recovery.
- The patient should be instructed in back-strengthening exercises and advised to avoid
physical manoeuvres likely to strain the lumbar spine.
- Injections of local anaesthetic or corticosteroids may be useful adjunctive treatment if
symptoms are due to ligamentous injury or joint dysfunction.
- Surgery may have to be considered if there is no response to conservative treatment or if
progressive neurological deficits develop.
- Central disc prolapse with bilateral symptoms and signs and disturbance of sphincter
function requires urgent surgical decompression.
LUMBAR CANAL STENOSIS
This is due to a congenital narrowing of the lumbar spinal canal exacerbated by thedegenerative
changes that commonly occur with age.
Clinical features
The patients, who are usually elderly, develop exercise-induced weakness and paraesthesia in
the legs (cauda equina claudication). These symptoms progress with continued exertion, often
to the point that the patient can no longer walk, but are quickly relieved by a short period of
rest. Physical examination at rest shows preservation of peripheral pulses with absent ankle
reflexes. Weakness or sensory loss may only be apparent if the patient is examined immediately
after exercise.
Investigations
Myelography, CT orMRI will demonstrate narrowing of the lumbar canal
Management
Extensive lumbar laminectomy often results in complete relief of symptoms and recovery of
normal exercise tolerance