Cushing’s Syndrome
Stephen Ou R2May 17, 2013
Learning Objectives
Discuss the different etiologies of hypercortisolism.Recognize the clinical manifestations of Cushing’s syndrome
Understand the screening tests for Cushing's syndromeEstablishing the cause of Cushing’s Syndrome.
DefinitionsCushing’s syndrome: constellation of symptoms associated with cortisol excess.
Cushing’s disease: Cushing’s Syndrome due to pituitary ACTH hypersecretion.
Clinical Manifestations
Most Specific Nonspecific
• Spontaneous Bruising
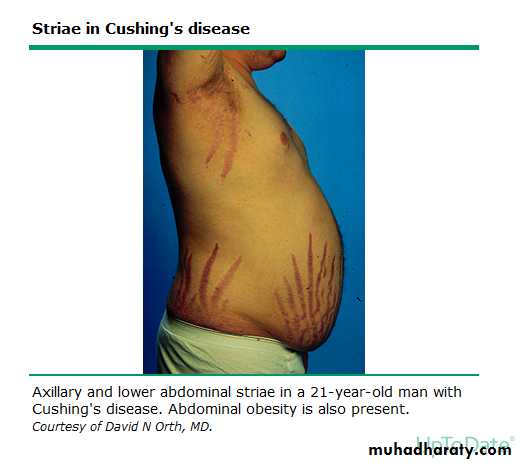
• Proximal Myopathy• Abdominal striae
• Central obesity w/ extremity wasting
• Dorsocervical fat pads (“Buffalo Hump”
• Round facies (“Moon Facies”)
• DM
• HTN
• Obesity
• Oligomenorrhea
• Osteoporosis
• Depression
• Insomnia
• Psychosis
• Impaired Cognition
• Hirsutism
• Fungal Skin Infections
• Nephrolithiasis
• Polyuria
Clinical Manifestations
of Cushing’s Syndrome
Facial Plethora i.e. “Moon Facies”
Dorsocervical fat pad i.e. “buffalo hump”It’s not always Cushing’s
Other common conditions associated with high cortisol levelsPregnancy
Etoh dependence
Morbid Obesity
Depression
Poorly controlled Diabetes
Physical stress/Malnutrition/Chronic Exercise
Bottom line: There are many other causes of hypercortisolism (Best to test in the outpatient setting)
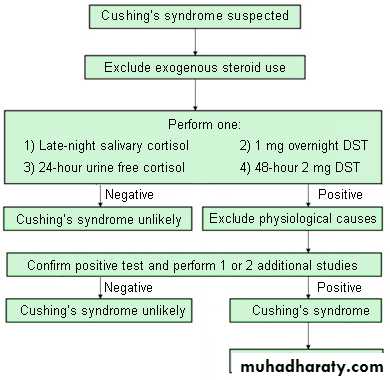
Diagnosis of Cushing’s Syndrome
Obtain a careful history to exclude exogenous glucocorticoid use.
Perform at least two first-line biochemical tests to obtain the diagnosis:
Urine free cortisol (UFC) (at least two measurements)
Late-night salivary cortisol (two measurements)
1-mg overnight Dexamethasone Suppression Test (DST)
Longer low-dose Dexamethasone Suppression Test (LDDST) (2 mg/d for 48 h)
Algorithm for testing
Case Vignette
A 67 year old woman is evaluated weight gain, hypertension and T2DM over the last 2 years. She has also developed muscle weakness of the lower extremities over the last 6 months. Physical exam is notable for a BP of 154/92, facial hirsutism, obesity, abdominal striae, proximal weakness and peripheral edema. Laboratory studies notable for potassium of 2.9 meq/L. Which of the following diagnostic tests should be performed next?Adrenal CT
C- peptide measurementGlutamic acid decarboxylase antibody titer
Pancreatic MRI
24-hour urine free cortisol excretion.
Case Vignette
A 67 year old woman is evaluated for a 2-day history of severe muscle weakness of the bilateral upper extremities. She has also experienced significant weight gain, developed hypertension and T2DM over the last 2 years. She also developed muscle weakness of the lower extremities 6 months ago. Physical exam is notable for a BP of 154/92, facial hirsutism, central obesity, abdominal striae, proximal weakness and peripheral edema. Laboratory studies notable for potassium of 2.9 meq/L. Which of the following diagnostic tests should be performed next?
Adrenal CT
Hemoglobin A1cGlutamic acid decarboxylase antibody titer
Pancreatic MRI
24-hour urine free cortisol excretion.
Take Home Points
There are a number of different causes of hypercortisolism including Cushing’s SyndromeThe clinical manifestations of cushing’s syndrome vary in specificity
Diagnosing Cushing’s syndrome includes the use of at least two first line biochemical tests.References
UpToDate: sections on cushing’s syndromeEpidemiology and clinical manifestations of Cushing’s syndrome
Establishing the diagnosis of Cushing’s syndrome
Establishing the cause of Cushing’s Syndrome
The Diagnosis of Cushing’s Syndrome: An Endocrine Society Practice Guideline. JCEM 2008 May; 93(5): 1526-1540.