1
Fifth stage
Pediatric
Lec-5
د.بسام
6/12/2015
NEONATAL JAUNDICE
Hyperbilirubinemia is a common and, in most cases, benign problem in neonates.
Nonetheless, untreated, severe indirect hyperbilirubinemia is potentially neurotoxic,
whereas conjugated direct hyperbilirubinemia often signifies a serious hepatic or systemic
illness.
Jaundice is observed during the 1st wk of life in approximately 60% of term infants and
80% of preterm infants, this is because of the followings:-
The color usually results from:-
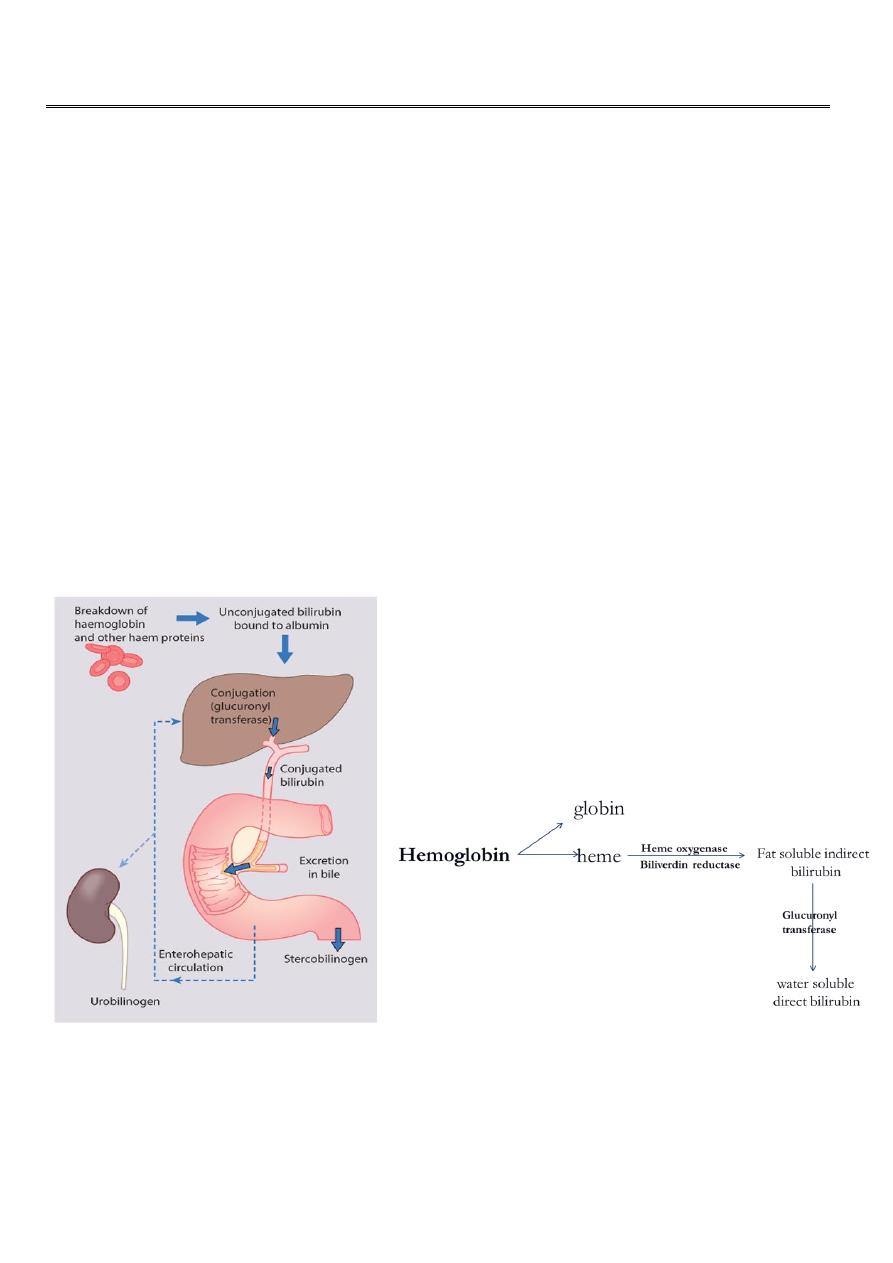
Either the accumulation in skin of unconjugated, lipid-soluble bilirubin pigment (indirect
reacting) formed from hemoglobin by the action of heme oxygenase, biliverdin reductase,
and nonenzymatic reducing agents in the reticuloendothelial cells, Or the jaundice may also
be due to deposition of the pigment after it has been converted in the liver cells by the
enzyme uridine diphosphoglucuronic acid (UDP)-glucuronyl transferase to the water-
soluble direct reacting bilirubin.
The unconjugated form is neurotoxic in infants at certain concentrations and under various
conditions. Conjugated bilirubin is not neurotoxic but indicates a potentially serious
disorder.

2
Unconjugated hyperbilirubinemia may be caused or increased by any factor that:
1. Increase the load of bilirubin to be metabolized by the liver as in hemolytic anemias,
polycythemia, shortened red cell life as a result of immaturity or transfused cells or use of
oxytocin during delivery, infection, enterohepatic circulation.
2. Damages or reduces the activity of the transferase enzyme (genetic deficiency, hypoxia,
infection, hypothermia and thyroid deficiency).
3. Competes for or blocks the transferase enzyme as drugs and other substances requiring
glucuronic acid conjugation for excretion).
4. Reduction of bilirubin uptake by liver cells (genetic defect, prematurity).
Diferential diagnosis of neonatal jaundice:-
Neonatal jaundice may be either:-
-Indirect hyperbilirubinemia.
-Direct hyperbilirubinemia (when the direct bilirubin is more
than 20% of the total serum bilirubin.
Indirect hyperbilirubinemia:-
1. Physiologic jaundice(icterus neonatorum).
2. Pathologic (mainly hemolytic).
3. Breast milk jaundice.
Physiologic jaundice:-
Causes:
-There is marked physiological release of haemoglobin from the breakdown of red cells
because of the high Hb concentration at birth.
-The red cell life span of newborn infants (70-90 days) is markedly shorter than that of
adults (120 days).
-Hepatic bilirubin metabolism is slow during the first few days of life.

3
Criteria of physiologic jaundice:
- It starts during the 2
nd
or the 3
rd
day of life.
- The peak of jaundice in fullterm baby is at the 2
nd
to 4
th
day of life, while in preterm
baby it peaks at 5
th
to 7
th
day of life.
- Decline to below 2mg/dl by the 7
th
day of life in term & by the 10
th
day in preterm baby.
- Jaundice disappear completely within 2 weeks of life.
- The raise in the bilirubin is less than 5 mg/dl/24 hours.
- The peak level of bilirubin is less than 12mg/dl, although 10% of these babies having
higher bilirubin level as in babies of diabetic mothers, prematurity, polycythemia, vit k
administration, male sex, Down syndrome, cephalhematoma, cutaneous bruising
oxytocin during labor, dehydration and calory deprivation, delay bowel motion.
Pathologic Jaundice(hemolytic):-
The criteria of this jaundice are:-
- It starts during the 1st 24 hr of life.
- The rise in serum bilirubin is more than 5mg/dl/24 hr.
- The serum bilirubin is higher than 12mg/dl.
- Jaundice persist for more than 2 weeks.
- May be positive family history of hemolytic disease, pallor, hepatosplenomegaly, signs
of kernecterus.
- Lab. findings may show evidence of Rh or ABO incompatability low hemoglobin,
reticulocytosis, and may be a positive Coombs test.
Breast milk jaundice:
An estimated of 2% of breast fed term infants develops an elevated level of uncongugated
bilirubin after the7th day of life reaching maximal concentrations as high as 10-30mg per dl
during the 2nd & 3rd week.If breast feeding continued the hyperbilirubinemia gradually
decrases & then may persist for 3-10 weeks at lower levels. These infants show no signs of
illness and kernicterus is very rarely reported.
The milk of some of these mothers contains a non esterified long chain fatty acids which
acts as an inhibitory substances to glucuronyl trasferase conjucating activity.In others the
milk contains a glucuronidase that may be responsible for jaundice.

4
Kernicterus:
Is a neurologic syndrome results from a deposition of uncongugated bilirubin in the brain
cells particularly in the basal ganglia, hippocumpus,and cerebellum. Lipid soluble indirect
bilirubin may cross the blood brain barrier and enter the brain by diffusion.
The factors which increase the toxic effects of elevated levels of unconjugated bilirubin in
the serum are:-
- Factors that reduce the retention of bilirubin in the circulation i.e increase of free bilirubin
in the circulation as in:- (hypoproteinemia, displacement of bilirubin from its binding sites
on albumin by competitive binding of drugs such as sulfisoxazole and acidosis, increased
free fatty acid concentration secondary to hypoglycemia, starvation, or hypothermia).
- Factors that increase the permeability of the blood-brain barrier or nerve cell membranes
to bilirubin or increase the susceptibility of brain cells to its toxicity, such as asphyxia,
prematurity, hyperosmolality, and infection.
Clinical features:
signs & symptoms of kernicterus usually appear in the 1
st
week of life although kernicterus
can occur at any time during the neonatal period.
The early signs may be subtle & indistinguishable from sepsis, asphyxia, hypoglycemia or
intracranial hrg which are:-
Lethargy poor feeding & absence Moro reflex are common initial signs.
In advanced cases there is irritability, increased muscle tone causing the baby to lie with an
arched back (opisthotonos), twitching, seizures, high pitched cry, bulging fontanel, coma
with the infant stiffly extended his arms with inward rotation.
Many infants who progress to these severe neurologic signs die, the survivors are usually
seriously damaged but may appear to recover & for 2-3 months manifest few
abnormalities.
Later in the 1st year of life opisthotonos, muscular rigidity, irregular movements, and
convulsions tends to recur.
In the 2nd year opisthotonos & convulsions abate, but irregular involuntary movements,
muscular rigidity or in some infants hypotonia increase gradually.
By 3 years of age the syndrome is completely developed consisting of bilateral
chorioathetosis with involuntary muscle spasm,seizures, mental deficiency, dysarthric
speech, high frequency hearing loss,squints, and defective upward movement of the eyes.

5
In mildly affected infants, the syndrome may be characterized only by mild to moderate
neuromuscular incoordination,partial deafness, or minimal brain dysfunction.
Treatment of hyperbilirubinemia:
1. Either there is no need for treatment especially if there is no hemolysis, full term baby,
healthy active & the jaundice is not deep with criteria of physiologic jaundice.
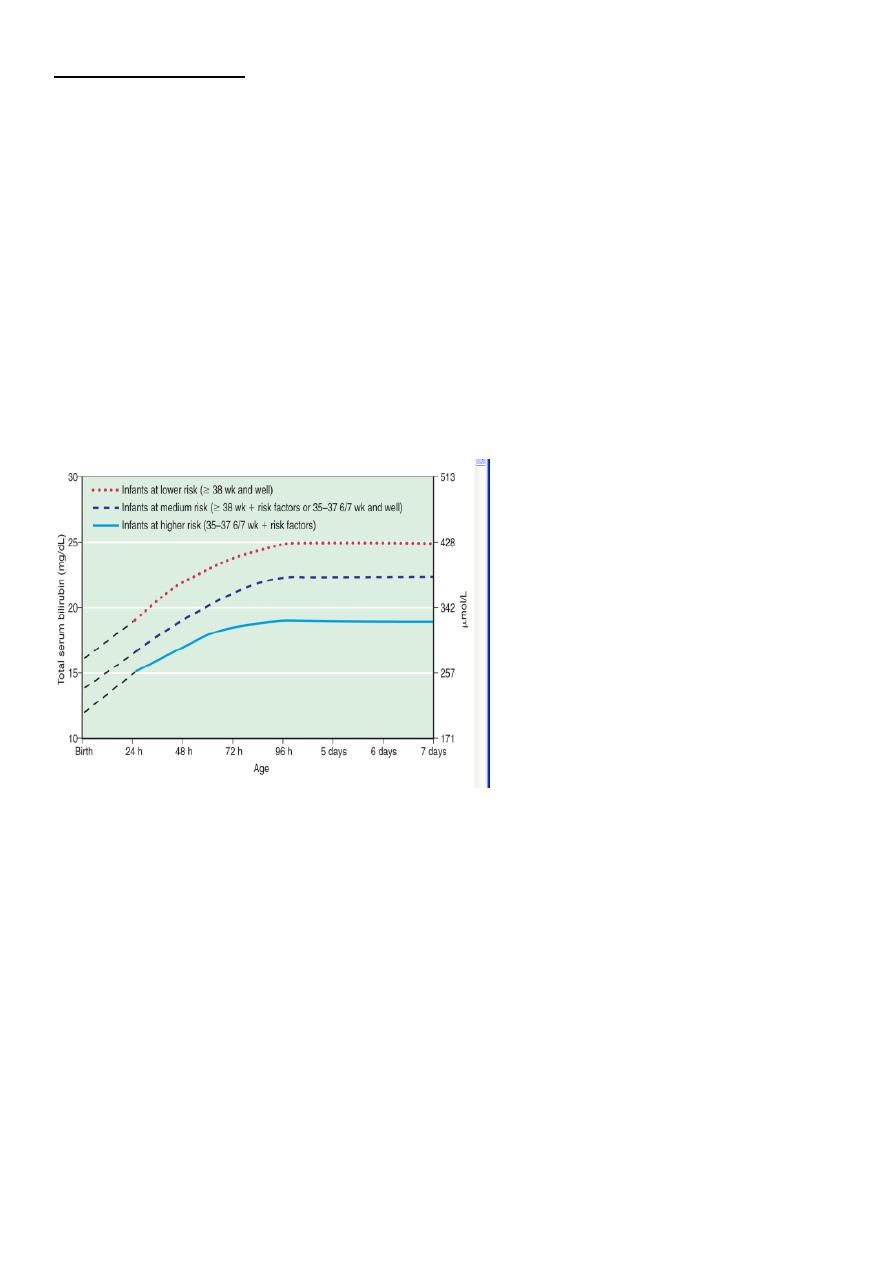
2. Phototherapy: usually started when the bilirubin level is at 50- 70% of the maximal
accepted value.
3. Exchange transfusion.
4. Intravenous immunoglobulin: for ABO and Rh incompata-bility in a dose of 0.5-1
grams/kg/dose repeated every 12 hours.
Phototherapy:-
Clinical jaundice & indirect hyperbilirubinemia reduced on exposure to a high intensity of
light in a wave length of 420-470nm. Bilirubin in the skin absorbs light energy which by
photoisomerization converts the toxic unconjugated bilirubin to a product which can be
excreted in bile without the need for conjugation, also phototherapy converts uncojugated
bilirubin to lumirubin which excreted in urine by the kidney.
Prophylactic phototherapy in VLBW infants may prevents hyperbilirubinemia & may reduce
the need for exchange transfusion.

6
The therapeutic effect depends on:-
1. The light energy emitted on in the effective wavelengths.
2. The distance between the lights & the infants.
3. The amount of skin exposed.
4. The rate of hemolysis if present.
5. Rate of metabolism & excretion of bilirubin.
Conventional phototherapy is applied continuously & the infant should be turned
frequently for max skin exposure.
Serum bilirubin & PCV should be measured every 4-8 hrs in infants with hemolysis or when
bilirubin level near the toxic range,others particularly older infants may be monitored every
12-24 hrs.
Monitoring should continue for at least 24 hrs after cessation of phototherapy in infants
with hemolytic disease that unexpected rise of bilirubin sometimes occur & require further
treatment.
Skin color cannot be relied on for evaluation of the effectiveness of phototherapy that the
skin of babies exposed to light may appear without jaundice in the presence of marked
hyperbilirubinemia.
The infants eyes should be closed & adequately covered to prevent exposure to light. Body
temp also should be monitored.
Complications of phototherapy:
1. loose stool.
2. Erythematous macular rashes.
3. Overheating.
4. Dehydration.
5. Bronze baby syndrome when there is direct hyperbilirubinemia.
6. Eye injury and nasal obstruction.
Phtotherapy is contraindicated in cases of porphyria.
7
Exchange transfusion:-
It is used to remove bilirubin from the circulation when phototherapy fails, is especially
used for infants with increased it bilirubin production from immune mediated hemolysis
because the circulating antibodies and the sensitized RBCs are also removed.
Exchange transfusion will:-
- Clear excess bilirubin.
- Correct the anemia without causing circulatory overload.
- Removes maternal antibodies.
- Removes sensitized RBCs.
Technique: a double volume exchange transfusion removes approximately twice the infant
circulating blood volume 170ml/kg body wt blood volume of the (infant is approximately
80-90 ml/kg body wt) replacing it with crossed-matched whole blood.The procedure
involves placement of a central catheter and removing & placing blood in a volume that is
approximately 10% or less of the infant blood volume.
Most of the bilirubin is extravascular, as a result exchange transfusion removes
approximately 25% of the total body bilirubin, after the procedure serum bilirubin falls to
approximately 1/2 of the pre exchange value, then increase to approximately 2/3 of that
level as the extravascular & vascular bilirubin reequilibirate. A double volume exchange
trnsfusion replace approximately 85% of the infants red blood cells.

8
Risks:
The risks of exchange transfusion are either to the use of blood products or from the
procedure itself,these includes:-
- blood born infection.
- thrombocytopenia.
- metabolic acidosis.
- volume overload.
- coagulopathy.
- graft versus host disease.
- necrotizing enterocolitis.
- portal vein thrombosis.
- electrolytes disturbance.
- hypoglycemia, hypocalcemia.
- cardiac arrhythmias.
- sudden death.
Direct hyperbilirubinemia:
When the direct bilirubin level is more than 2mg /dl then the problem is termed as direct
hyperbilirubinemia.
Common causes:-
- biliary atresia.
- idiopathic neonatal hepatitis.
Less common causes as:-
cystic fibrosis, galactosemia, Wilson disease, tyrosinemia, fructosemia, alpha 1 antitrypsin
deficiency, TORCH infection, choledochal cyst, total parenteral nutrition.