1
Definitions
Perinatal period;
28wk-7
th
day after birth
.
Neonatal period;
1
st
28 days of life
.
Infancy;
1
st
year of life
.
PHYSICAL EXAMINATION OF THE NEWBORN INFANT
The initial examination of a newborn infant should be performed as soon as possible after
delivery to detect abnormalities and to establish a baseline for subsequent examination. Infants
should have their temperature, pulse, respiratory rate, color, type of respiration, tone, activity,
and level of consciousness checked.
Congenital anomalies may be present in 3-5 % of infants. Afterwards, a 2
nd
and more detailed
examination should be performed within 24 hr of birth.
Physical activity; which may be absent during sleep, illness, and drugs; baby may be either lying
with the extremities motionless, or vigorously crying with accompanying activity of the arms and
legs. Coarse, tremulous movements with ankle or jaw myoclonus are common in active infants,
whereas convulsive twitching usually occurs in a quiet state.
Generalized edema may occur with prematurity, hypoproteinemia secondary to severe
hemolysis, congenital nephrosis. Edema may be confined to one or more extremities of a female
as initial sign of Turner syndrome.
Skin; vasomotor instability and peripheral sluggish circulation may result in harmless cyanosis
of hands and feet acrocyanosis, skin mottling or extraordinary division of the body from the
forehead to the pubis into red and pale halves is known as harlequin color change.
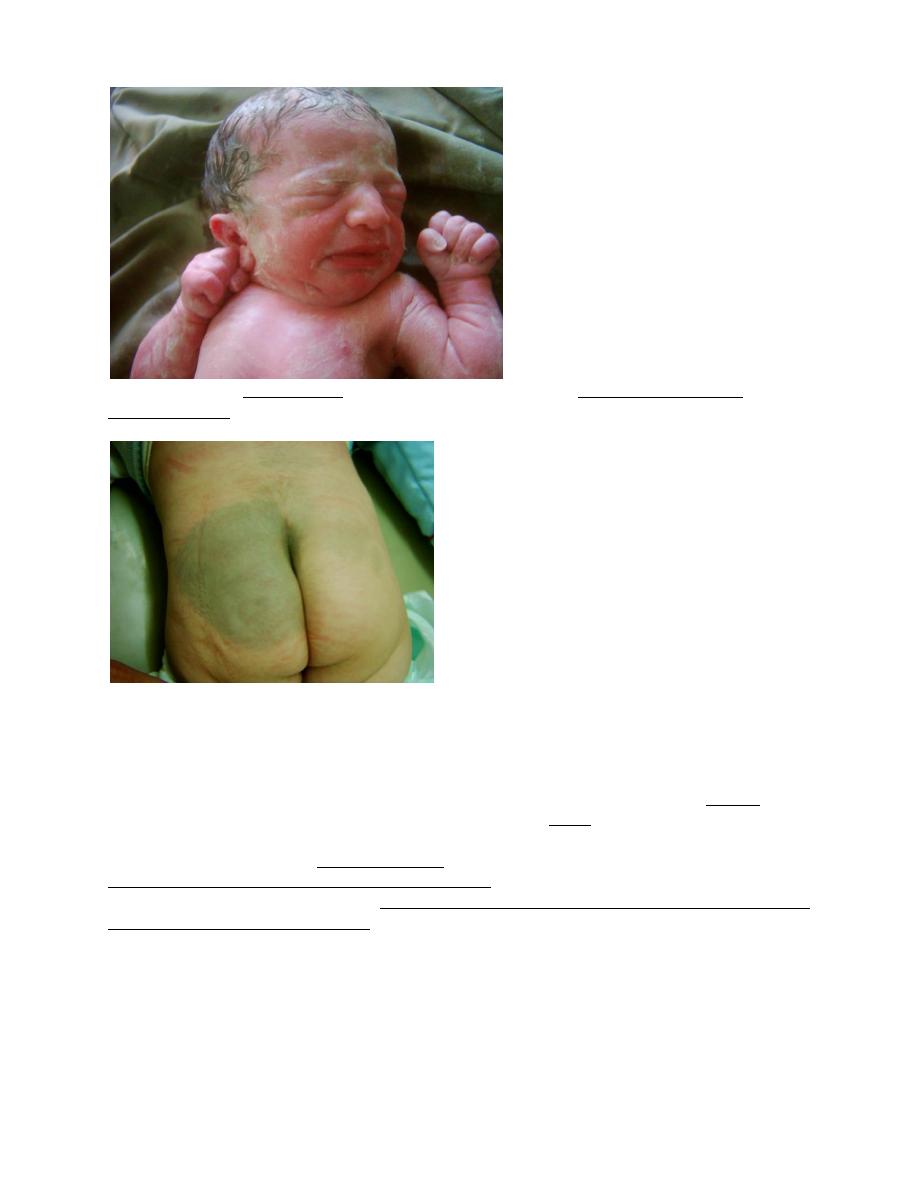
Vernix caseosa covers the skin at birth and spontaneously shed within 2-3 days.
2
Transient macular hemangiomas in neck & eyelids are common (stork bite hemangioma).
Mongolian spots are blue well demarcated areas of hyperpigmenation over buttocks and back,
are common and usually disappear within 1
st
year.
The skin of premature infants is thin and delicate and tends to be deep red, covered by lanugo
hair. Tuft of hair over spine indicates spina bifida.
Brownish-yellow skin indicates presence of meconium in the amniotic fluid as a result of intra-
partum asphyxia.
skull; All infants should have their head circumference charted. The skull may be molded due to
prolonged engagement of head. While C/S delivered head is round. The suture lines, the size and
fullness of the anterior and posterior fontanels should be determined digitally by palpation.
Premature fusion of sutures (cranial synostosis).
Persistence of, or excessively large anterior (normal, 20 ± 10 mm) and posterior fontanels may
be associated with several disorders (achondroplasia, hydrocephaly, prematurity, trisomy 21, 13,
18, and vitamin D deficiency rickets).
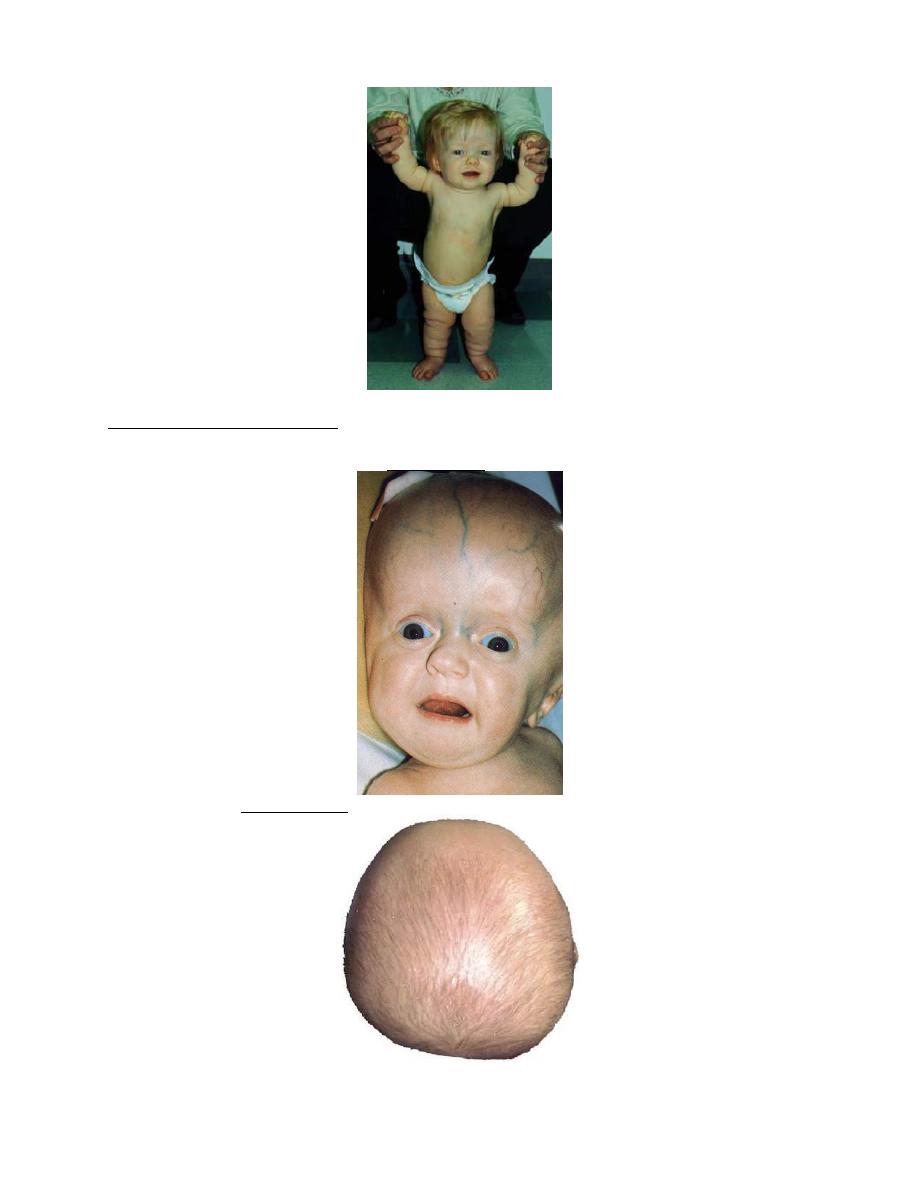
3
Persistently small fontanels suggest microcephaly, craniosynostosis, or congenital
hyperthyroidism. Transillumination of an abnormal skull in a dark room, followed by ultrasound
or computed tomography will rule out hydrocephaly.
Asymmetric skull (plagiocephaly) may be due to in utero positioning forces on the skull.
4
Face; look for dysmorphic features, such as epicanthal folds, widely or narrowly spaced eyes,
microphthalmia, asymmetry, and low-set ears, which are often associated with congenital
syndromes. The face may be asymmetric as a result of 7
th
nerve palsy.
Eyes; The eyes often open spontaneously if the infant is held up and tipped gently forward and
backward.
The conjunctiva; Conjunctival and retinal hemorrhages are common with vacuum-assisted
deliveries, usually benign and usually resolve by 2 wks.
A cornea larger than 1 cm in diameter in term infant suggests congenital glaucoma.
The iris; The presence of bilateral red reflexes suggests the absence of cataract. Leukokoria
(white pupillary reflex) suggests cataract or tumor(retinoblastoma).
Ears; Unilateral or bilateral pre-auricular skin tags may occur frequently.
Nose; The nose may be slightly obstructed by mucus accumulated in the narrow nostrils. The
nares should be symmetric and patent. Anatomic obstruction of the nasal passages is secondary
to unilateral or bilateral choanal atresia results in respiratory distress.
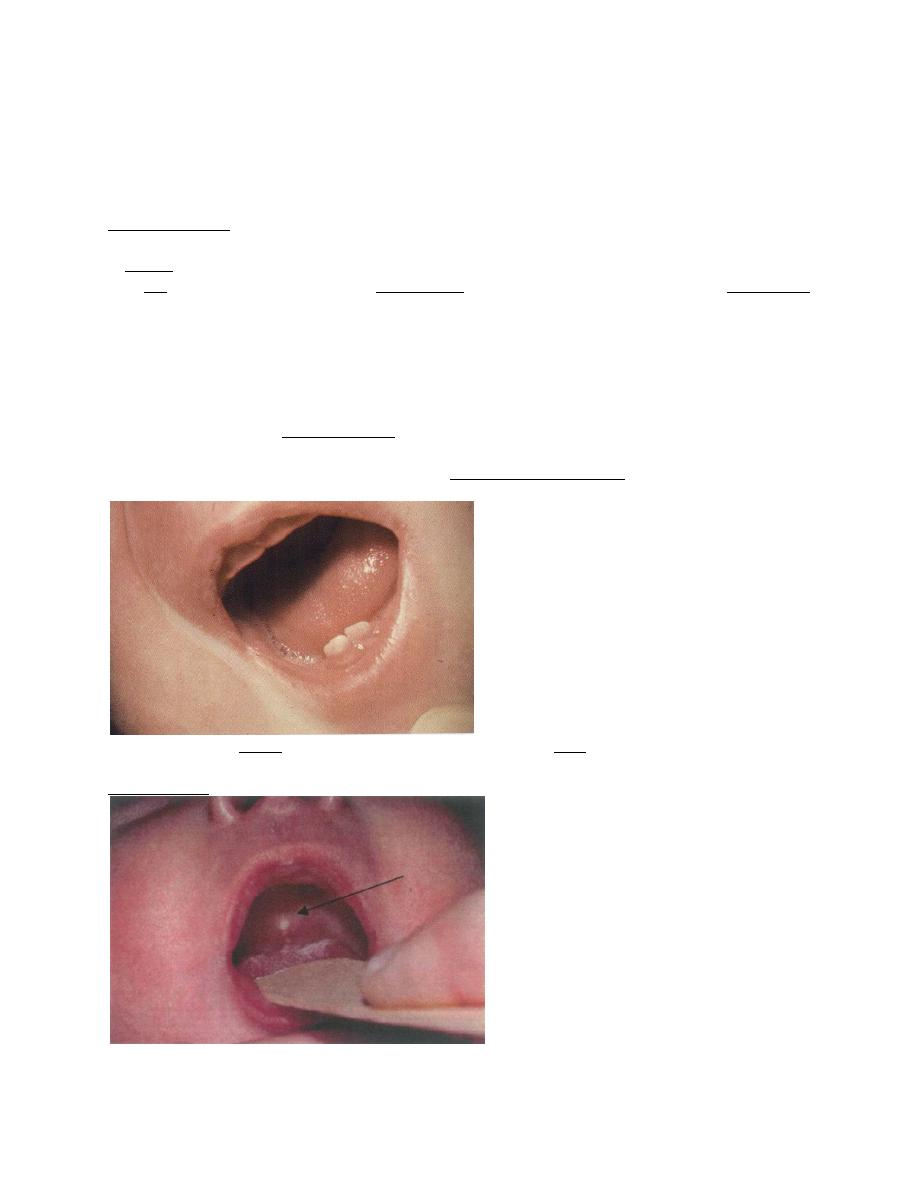
Mouth; A normal mouth may rarely have natal or neonatal teeth which shed before the
deciduous ones erupt.
The soft and hard palate should be inspected and palpated for cleft.
On the hard palate on either side may be temporary accumulations of epithelial cells called
Epstein pearls.
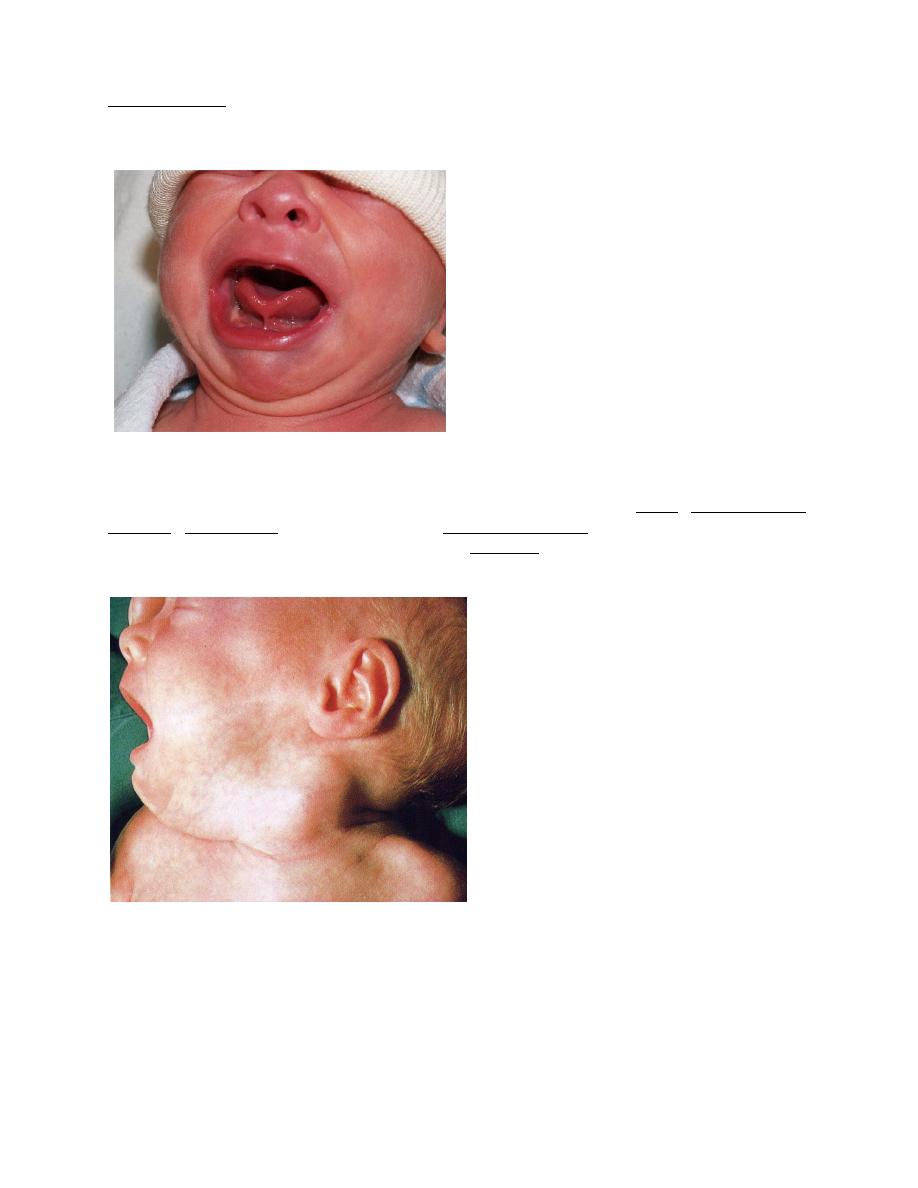
5
Retention cysts of similar appearance may also be seen on the gums. Both disappear
spontaneously, usually within a few weeks of birth.
The frenulum may be short, but rarely is shortness (tongue-tied) a reason for cutting it, unless
there are problems with feedings (frenotomy).
The cheeks have a fullness on both the buccal and the external aspects as a result of the
accumulation of fat making up the sucking pads.
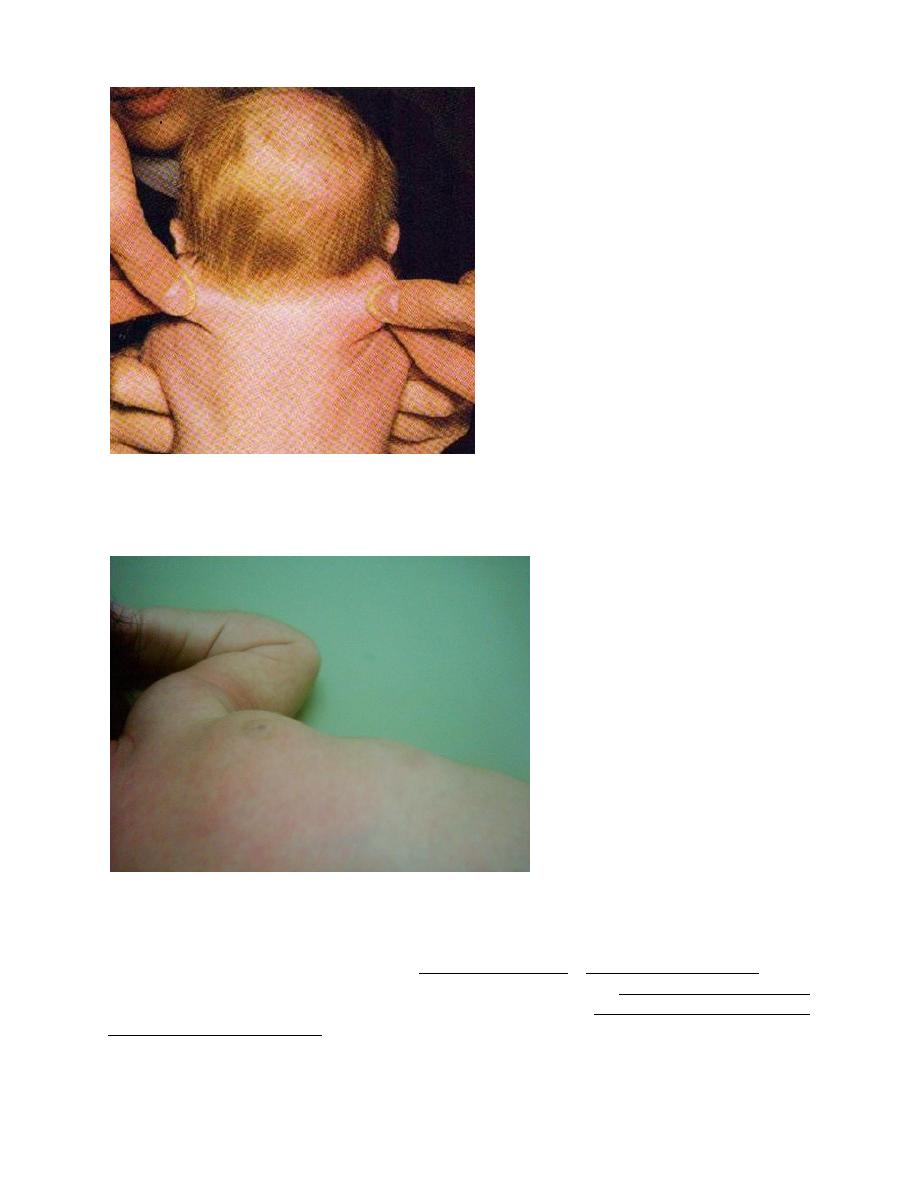
Neck; the neck appears relatively short. Abnormalities may include goiter, cystic hygroma,
teratoma, hemangioma, and lesions of the sternocleidomastoid muscle that are presumably
traumatic, a muscle hematoma followed by later torticollis (that causes the head to turn toward
and the face to turn away from the affected side), plagiocephaly, facial asymmetry, and
hemihypoplasia if untreated.
Redundant skin or webbing in a female infant suggests intrauterine lymphedema and Turner
syndrome.
6
Both clavicles should be palpated for fractures.
Chest; Breast hypertrophy is common, and milk may be present (but should not be expressed).
Asymmetry, erythema, induration, and tenderness should suggest mastitis or a breast abscess.
Widely spaced nipples with a shield-shaped chest suggests Turner syndrome.
Lungs; The respiratory rate should be counted for a full minute with the infant in the resting
state. The rate for normal term infants is 30-40/min; in premature infants the rate is higher and
fluctuates more widely. A rate consistently over 60/min during periods of regular breathing
usually indicates pulmonary, cardiac, or metabolic disease (acidosis).
Premature infants may have irregular periodic respiration (Cheyne-Stokes rhythm). The
breathing of newborn infants is mainly diaphragmatic. A weak cry or grunting during expiration
signifies potentially serious cardiopulmonary disease or sepsis. Flaring of the alae nasi and
intercostal muscles retraction are common signs of pulmonary pathology. Normally, the breath
sounds are broncho-vesicular.
7
Heart; The location of the heart (levocardia or dextrocardia) should be determined. Transitory
murmurs usually represent a closing ductus arteriosus. Although congenital heart disease may
not initially produce the murmur that will appear later. The pulse may vary normally from
90/min in relaxed sleep to 180/min during activity (usually 110-140 beat/minute at rest). Pulses
should be palpated in the upper and lower extremities to detect coarctation of the aorta.
Abdomen; The liver is usually palpable (2 cm). The tip of the spleen may be felt. The GIT is
gasless at birth. Gas should normally be present in the rectum on roentgenogram by 24 hr of age.
Unusual masses should be investigated immediately by ultrasonography.
Cystic masses include: hydronephrosis, multicystic-dysplastic kidneys, adrenal hemorrhage,
intestinal duplication, ovarian, omental, or pancreatic cysts.
Solid masses include neuroblastoma, congenital nephroma, hepatoblastoma, and teratoma.
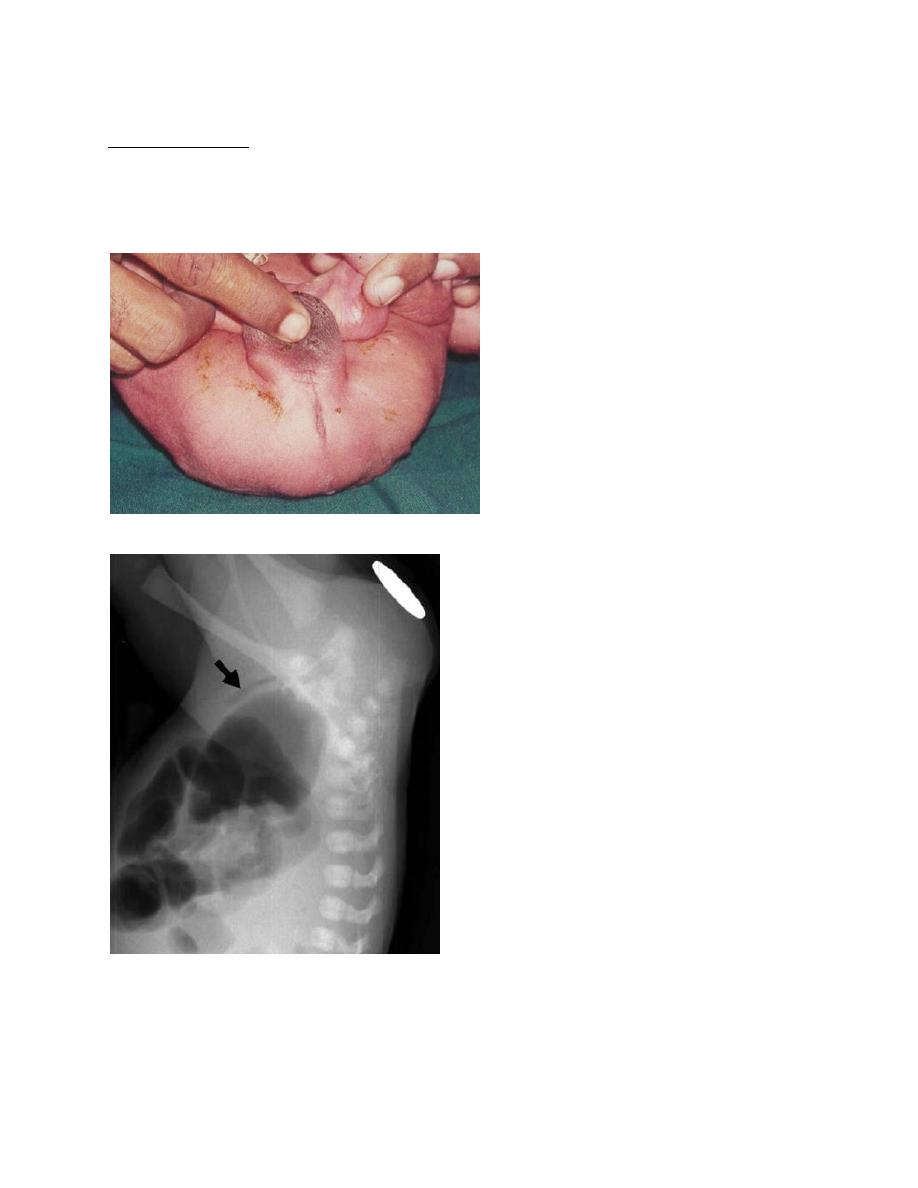
Abdominal distention at birth or shortly afterward suggests either obstruction or perforation of
the gastrointestinal tract, often as a result of meconium ileus; later distention suggests lower
bowel obstruction, sepsis, or peritonitis.
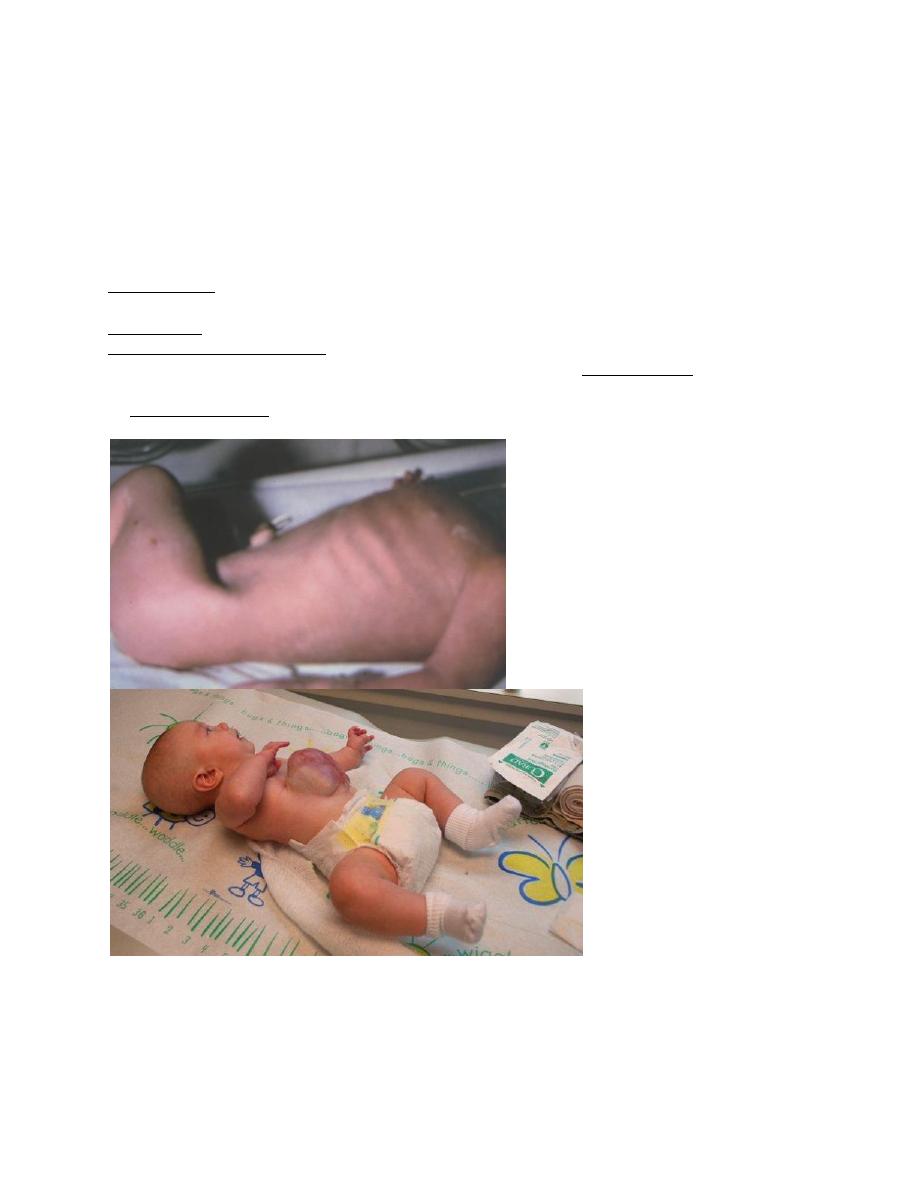
A scaphoid abdomen in a newborn suggests diaphragmatic hernia. Abdominal wall defects
produce an omphalocele.
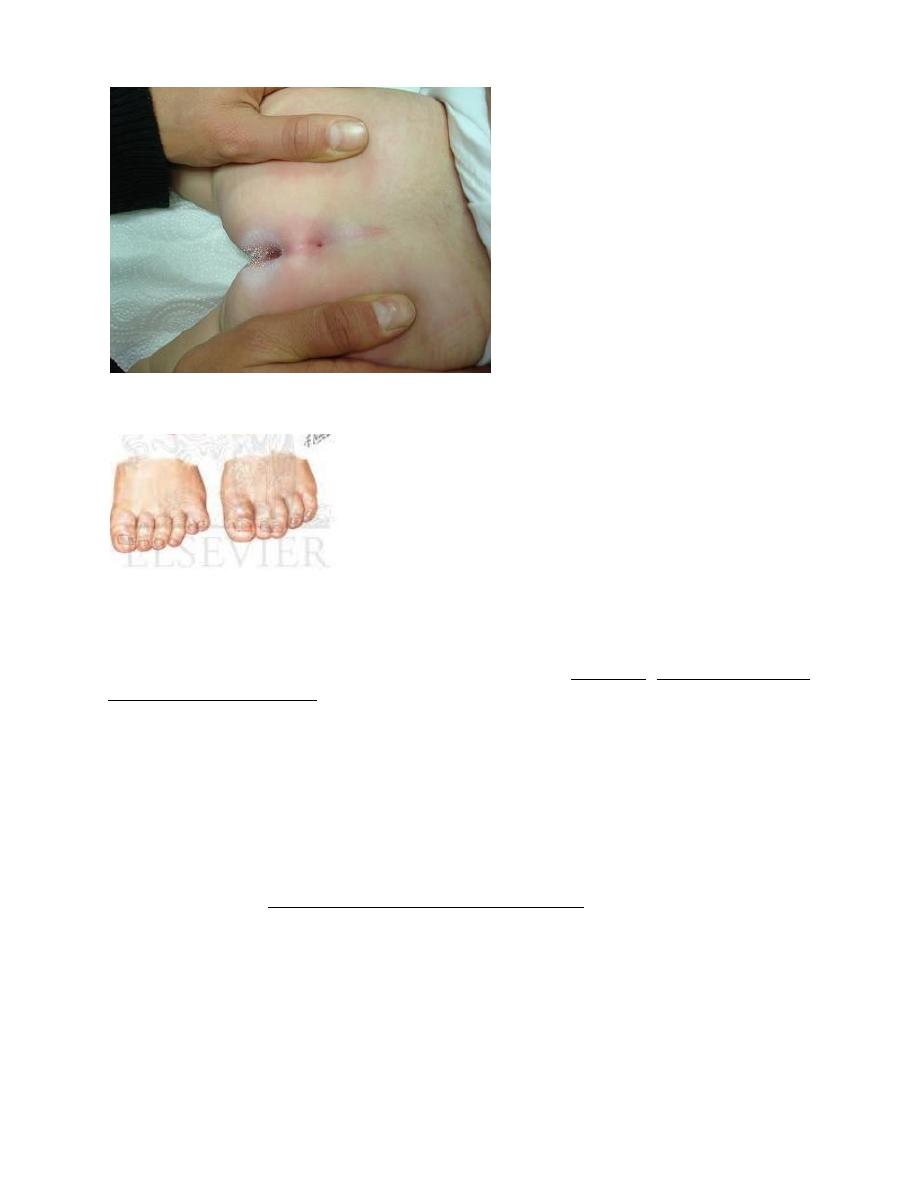
Omphalitis is an acute inflammation of the periumbilical tissue that may extend to the abdominal
wall, peritoneum, umbilical vessels, liver, and may result in later portal hypertension.
8
The umbilical cord should have two arteries and one vein. A single umbilical artery suggests an
occult renal anomaly.
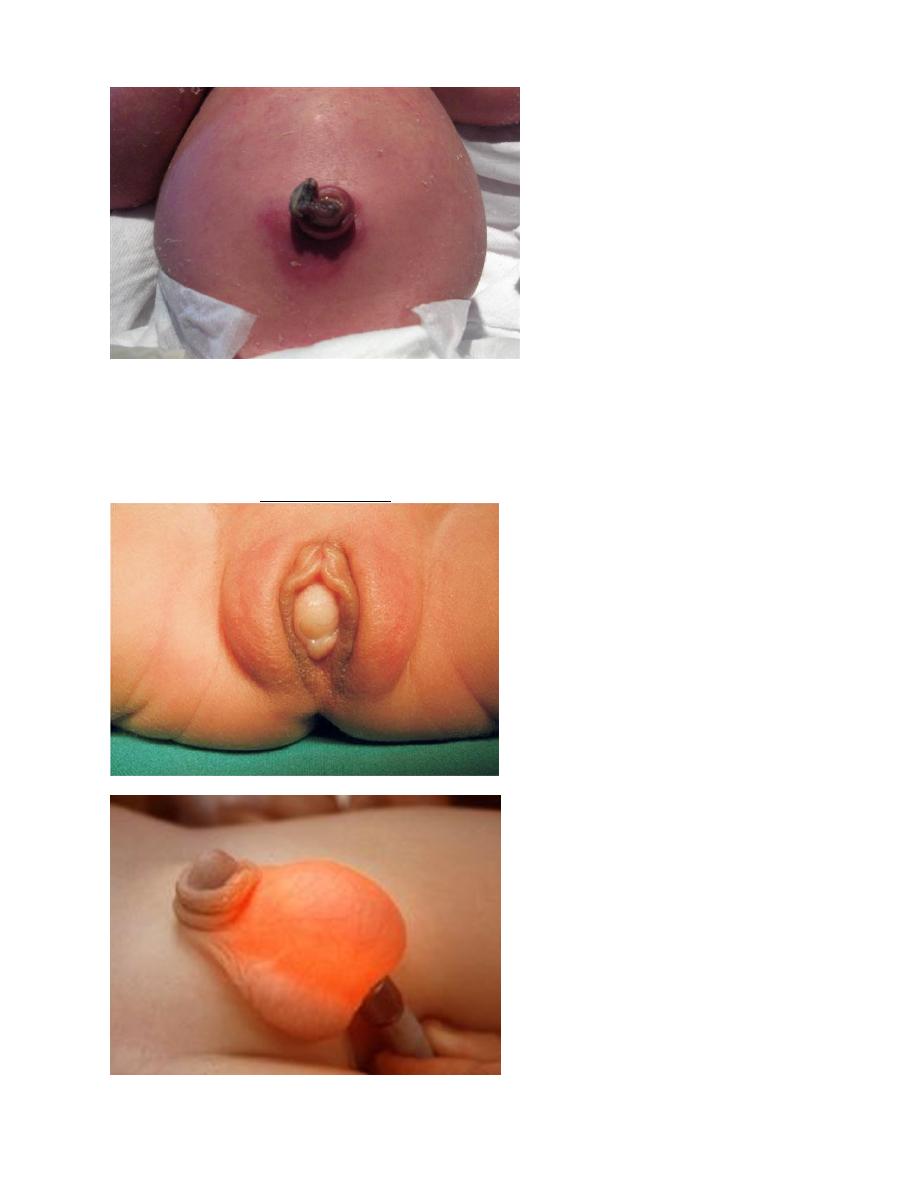
Genitals; Transplacentally acquired maternal hormones may produce enlargement and secretion
of the breasts in both sexes and prominence of the female genitals, often with considerable
nonpurulent discharge. These transitory manifestations require observation only. An imperforate
hymen may result in hydrometrocolpos.
Hydrocele, is distinguished from a hernia by palpation and trans-illumination.
9
Black male infants usually have dark pigmentation of the scrotum before the rest of the skin
assumes its permanent color. The prepuce of a newborn infant is normally tight and adherent. In
severe hypospadias, should suspect abnormal sex chromosomes or a masculinized female with
an enlarged clitoris because of adrenogenital syndrome. Urine is usually passed during or
immediately after birth; 95% of infants void within 24 hr.
Anus; 99% of term infants and 95% of premature infants pass meconium within 48 hr of birth.
Imperforate anus is not always visible and may require insertion of rectal tube(thermometer).
Roentgenographic study is required. Passage of meconium does not rule out an imperforate anus
if a rectal-vaginal fistula is present.
The dimple in the sacro-coccygeal midline may be mistaken for a sinus.
10
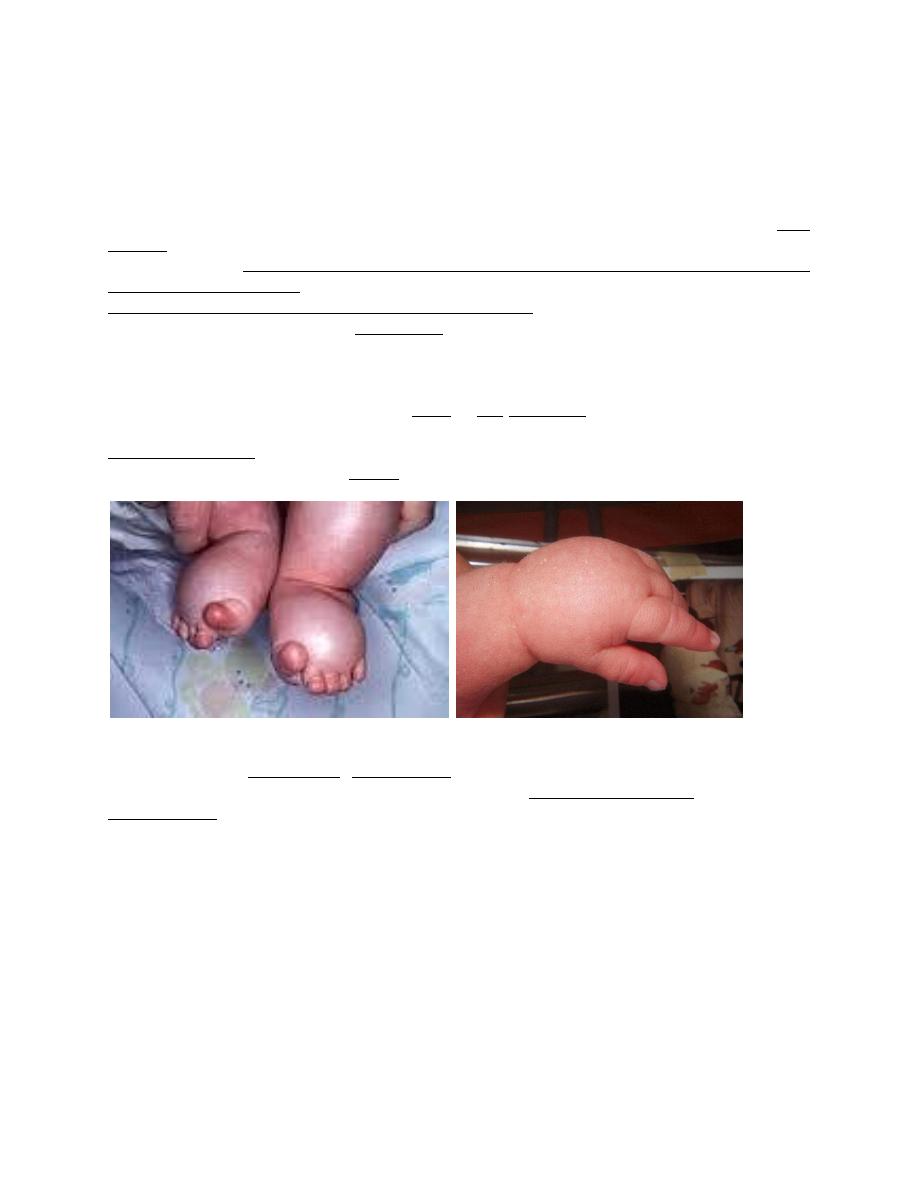
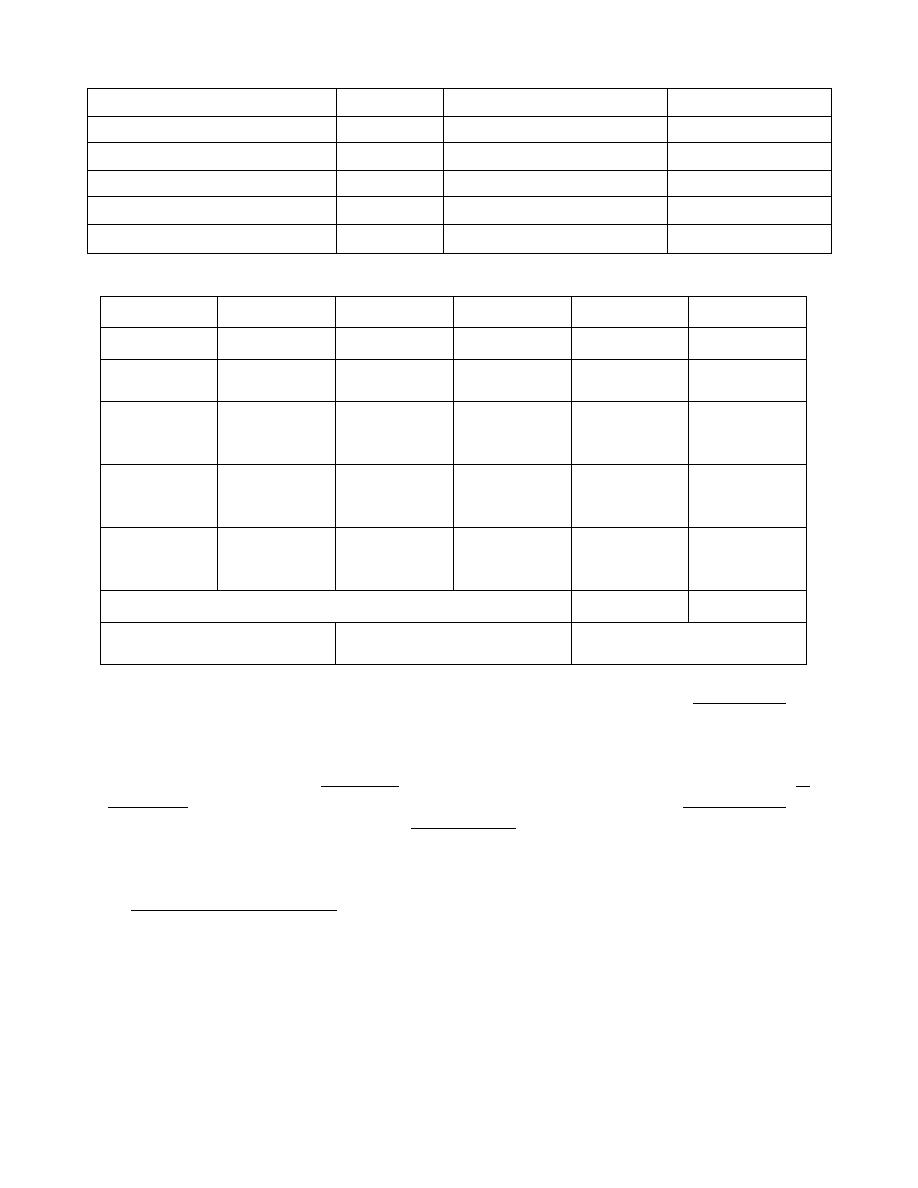
Extremities; Observing the extremities in spontaneous or stimulated activity may arouse the
suspicion of a fracture or nerve injury. The hands and feet should be examined for polydactyly,
syndactyly, and abnormal dermatoglyphic patterns such as a simian crease.
The hip joints of all infants should be examined to rule out congenital dislocation.
Routine delivery room care
Low-risk infants may initially be placed head downward after delivery to clear the mouth,
pharynx, and nose of fluid, mucus, blood, and amniotic debris by gravity; gentle suction with a
bulb syringe or soft catheter. Wiping the palate and pharynx with gauze may lead to abrasions
and development of thrush, ulcers, and maxillary osteomyelitis. The stomachs of infants
delivered by cesarean section (C/S) may contain more fluid than those of infants delivered
vaginally. Their stomachs may need to be emptied to prevent aspiration. Most healthy infants
may be given directly to their mothers for immediate bonding and nursing.
The Apgar score; is a practical systematic assessment of newborn infants immediately after birth
to help identify those requiring resuscitation and to predict survival in the neonatal period. The 1-
min Apgar score may signal the need for immediate resuscitation, and the 5-, 10-, 15-, and 20-
min scores may indicate the probability of successfully resuscitating an infant.
The Apgar score was not designed to predict neurologic outcome. Indeed, the score is normal in
most patients in whom cerebral palsy subsequently develops. The Apgar score at 5 min and
umbilical artery blood pH both predict neonatal death. A low score may be due to a number of
factors, including drugs given to the mother during labor and immaturity.
11
Sign
0
1
2
Heart rate
Absent
Below 100
Over 100
Respiratory effort
Absent
Slow irregular
Good, crying
Muscle tone
Limp
Some flexion of extremities
Active motion
Response to catheter in nostril
No response
Grimace
Cough or sneeze
Color
Blue, pale Body pink, extremities blue Completely pink
Example of Apgar scoring
Sign
0
1
2
1 min
2 min
Heart rate Absent
Below 100
Over 100
2
2
Respiratory
effort
Absent
Slow
irregular
Good, crying
1
2
Muscle tone
Limp
Some flexion
of
extremities
Active
motion
1
2
Response to
catheter in
nostril
No response
Grimace
Cough or
sneeze
1
2
Color
Blue, pale
Body pink,
extremities
blue
Completely
pink
1
2
Total score
A/S
1
= 6
A/S
2
= 10
≥ 7 start simple stimulation
4 - 6 start Ambu bag
ventilation
<4 start endotracheal intubation,
active ventilation
Maintenance of Body Heat: Body surface of a newborn infant in relative to body weight, is
approximately three times that of an adult. Under the usual delivery room conditions (20-25°C),
an infant's skin temperature falls approximately 0.3°C/min. and deep body temperature decreases
by 0.1
o
C/min after delivery.
The heat loss occurs by 1. convection of heat energy (to the cooler surrounding air), by 2.
conduction of heat (to the colder materials on which the infant is resting), by 3. heat radiation (to
other nearby cooler solid objects), and by 4. evaporation (from moist skin and lungs).
Metabolic acidosis, hypoxemia, hypoglycemia, and increased renal excretion of water and
solutes may develop in term infants exposed to cold. These infants increase heat production by
increasing the metabolic rate and oxygen consumption by releasing norepinephrine which results
in nonshivering thermogenesis through oxidation of fat and there may be increased muscle
activity. Hypoglycemic or hypoxic infants cannot increase their oxygen consumption, so their
central temperature decreases. Therefore, to reduce heat loss, it is desirable to ensure that infants
are dried and wrapped in blankets or placed under a radiant warmer.
Kangaroo mother care with direct skin to skin contact and a hat and blanket covering the infant is
a safe alternative when incubators are unavailable.
12
Maintaining a relative humidity of 40-60% aids stabilizing body temperature, by preventing
drying of the respiratory passages.
Antiseptic skin and cord care; Skin and cord should be cleansed with warm water or non-
medicated soap solution and rinsed with water. To reduce colonization with Staphylococcus
aureus and other pathogenic bacteria, the umbilical cord may be treated daily with triple dye or
bacitracin followed by twice-daily alcohol swabbing until the cord falls off. Alternatively,
chlorhexidine washing or, on rare occasion during S. aureus epidemics, a single hexachlorophene
bath may be used. Routine or repeated total body exposure to hexachlorophene may be
neurotoxic, particularly in low-birth weight infants.
Nursery personnel should use chlorhexidine for routine hand-washing. Hand-to-elbow washing
for 2 min in the initial wash and 15-30 sec in subsequent washes is essential for staff and visitors.
Other measures;
The eyes of all infants must be protected against gonococcal infection by 1% silver nitrate drops
(the best-proven therapy). Erythromycin (0.5%) or tetracycline (1.0%) sterile ophthalmic
ointments are alternative measures that add coverage against chlamydia.
Hemorrhage in newborn can be due to factors other than vitamin K deficiency, an intramuscular
injection of 0.5-1mg of water-soluble vitamin K
1
is recommended for all infants immediately
after birth to prevent hemorrhagic disease of the newborn. Larger intravenous doses predispose
to the development of hyperbilirubinemia and kernicterus and should be avoided.
Neonatal screening is available for various genetic, metabolic, hematologic, and endocrine
diseases. Specific tests vary according to the country. Laboratory tests performed on infant heel
puncture blood samples include those for hypothyroidism, phenylketonuria, galactosemia, maple
syrup urine disease, homocystinuria, adrenal hyperplasia, hemoglobinopathy, cystic fibrosis,
tyrosinemia, and other organic acid defects.
Hearing; Hearing impairment affects speech and language development, may be severe in
2/1.000 and overall affects 5/1.000 births. Universal screening of infants is recommended to
ensure early detection of hearing loss and intervention.
Universal screening pulse oximetry detects ductal cyanotic congenital heart diseases.
Universal screening for hyperbilirubinemia by serum or transcutaneous bilirubin levels.
Universal screening for congenital hip dysplasia by Ortolani and Barlow tests. No routine
ultrasonography indicated.

13
Parent-Infant bonding; normal infant development depends bonding between mother and her
newborn infant psychologically and physiologically. This bonding reinforced by the emotional
support of a loving family. The quiet alert state of the infant provides the opportunity of eye to
eye contact which is important in stimulating the loving feelings of parents to their babies.
Successful breast-feeding; includes immediate postpartum mother-infant contact with suckling,
rooming-in, demand feeding, and support from experienced women. Nursing at least 5 min at
each breast is reasonable. Nursing episodes should then be extended according to the comfort
and desire of the mother and infant.
Drugs contraindicates breast feeding; Maternal sedatives may result in sedation of the infant.
Antimetabolites, immunosuppressants, methimazole (antithyroid), amphetamines, iodides and
radiopharmaceuticals are.
Medical contraindicates breast-feeding; in the United States include infection with HIV (in
developed countries), human T-cell leukemia virus types 1 and 2, cytomegalovirus, active
tuberculosis (until treated and not considered contagious), and hepatitis B virus (until an infant
receives hepatitis B immune globulin and vaccine).