Urinary tract radiology
Urinary tract disordersد- نجلاء حنون
LEC. 2
Urinary calculi
X-ray examinations :Most urinary calculi are calcified and show varying density. Many are uniformly calcifiedbut some, particularly bladder stones, may be laminated. Only pure uric acid and xanthine stones are radiolucent on plain radiography, but they can be identified at CT or ultrasound .



Small renal calculi are often round or oval; the larger ones frequently assume the shape of the pelvicaliceal system and are known as staghorn calculi .

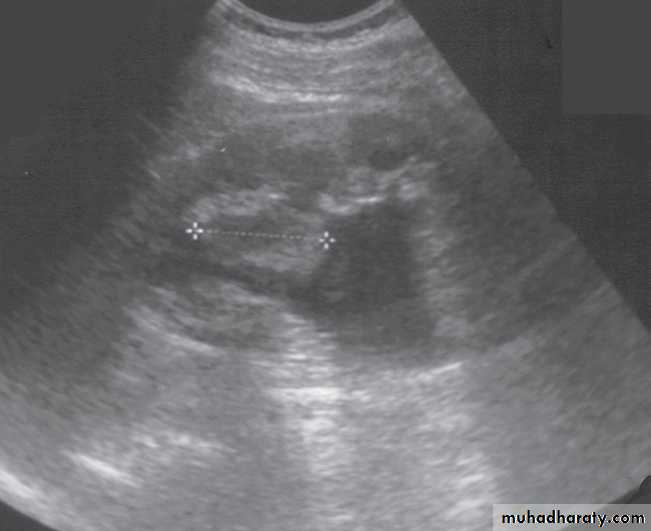
U/S :Most renal calculi of more than 5 mm in size are readily seen at ultrasound, produce intense echoes and cast acoustic shadows.

Stones in the ureters cannot be excluded on ultrasound, although stones lodged at the vesicouteric junction may be demonstrated .
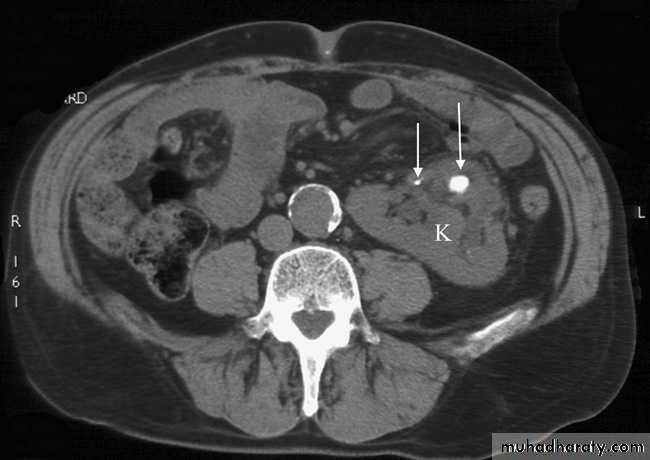
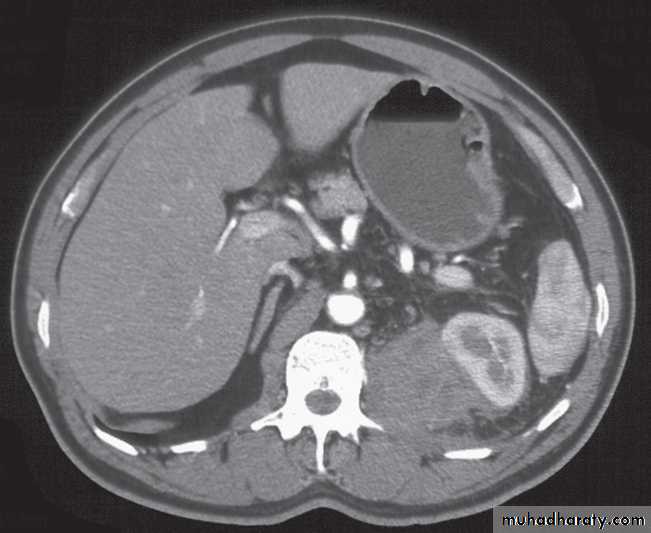
Computed tomography without intravenous contrast medium is exquisitely sensitive for the detection of calculi.
It is used in place of IVU for the detection and precise anatomical localization of stones prior to treatment in most centres


Urinary tract obstruction
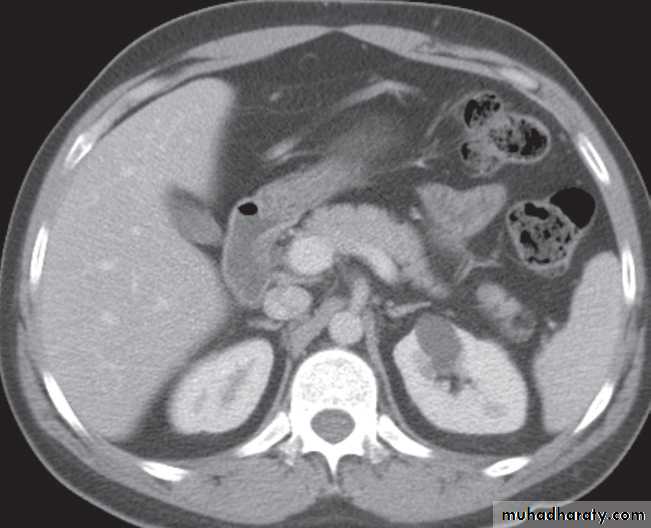
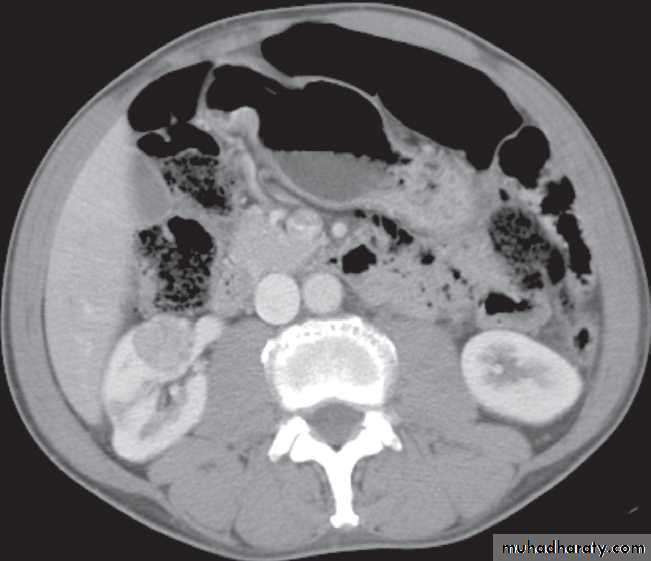
The principal feature of obstruction is dilatation of the pelvicaliceal system and ureter. collecting system is dilated down to the level of the obstructing pathology and demonstrating this level is a prime objective of imaging .
Ultrasound and urographic examination play major roles when evaluating urinary tract obstruction, and CT urography has overtaken IVU for the investigation of obstruction .
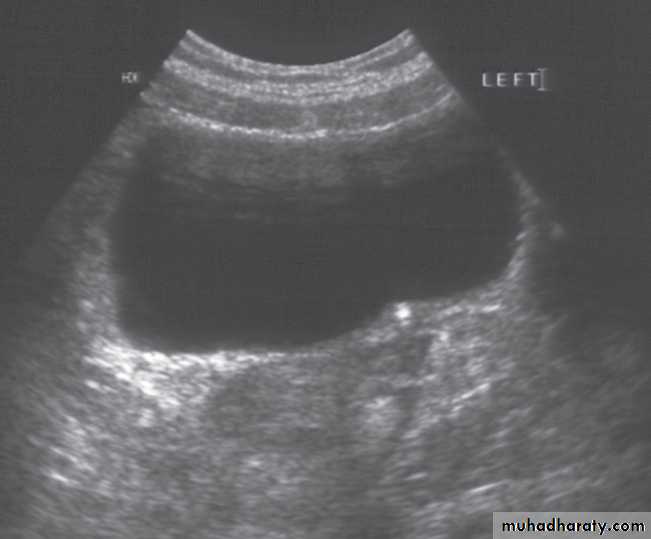
Ultrasound Dilatation of the pelvicaliceal system ( hydronephrosis ) is demonstrated sonographically as a multiloculate fluid collection in the central echo complex, caused by pooling of urine within the distended pelvis and calices .

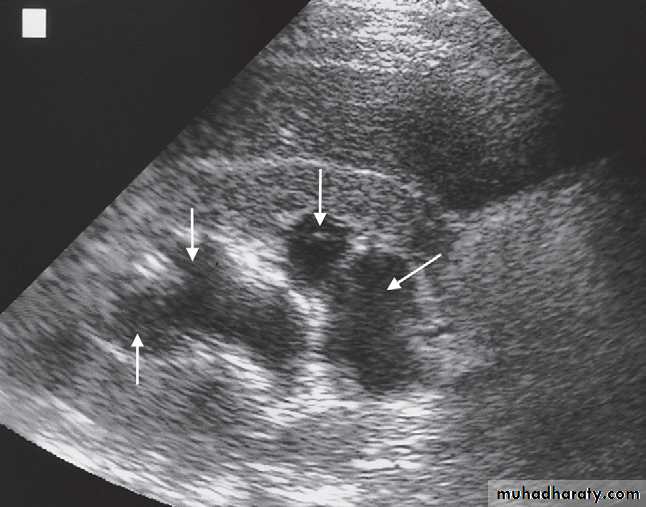
Major DDX are multiple renal cysts. With prolonged obstruction, thinning of the cortex due to atrophy will be seen.
Some causes of obstruction are identifiable (e.g. carcinoma of the bladder or a stone at the vesicoureteric junction), it is often not possible to determine the cause of urinary tract obstruction at ultrasound examination.
Intravenous urogram:
mainly replaced by CT scan & CT urography in patients with suspected acute obstruction, which is usually caused by a calculus.-In Plain films may demonstrate the calculus responsible for the obstruction .
-Following injection of intravenous contrast medium, a film of the renal tract is taken at approximately 15 minutes. If the urogram is normal, with contrast seen in normal, undistended ureters bilaterally,then this effectively rules out ureteric colic as the cause of acute pain.
-If one of the ureters is obstructed, then adense nephrogram will be seen and opacification of the pelvicaliceal system and ureter on the obstructed side takes much longer. Delayed films are, therefore, essential part of any IVU.


Computed tomography
Computed tomography is now widely used to evaluate urinary tract obstruction .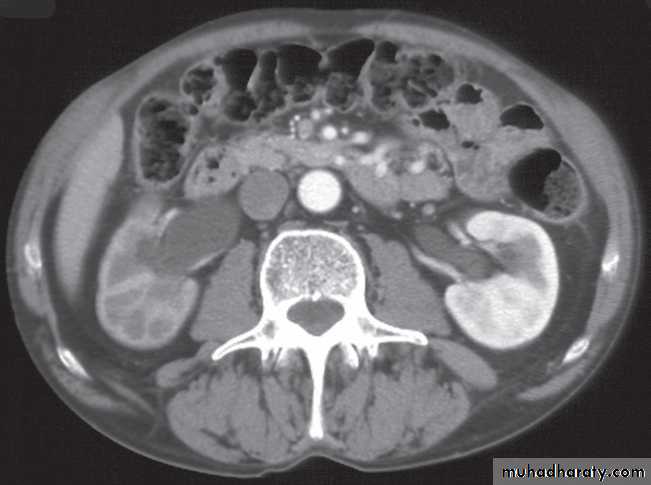


In acute obstruction, non-contrast enhanced CT sensitively demonstrates calculi and the unopacified, dilated collecting system can frequently be traced down to the point of obstruction .
Non-contrast CT is often used in acute ureteric colic, as an alternative to IVU, in patients with an allergy to intravenous contrast medium.
Causes of obstruction to the ureters and pelvicaliceal systems
Causes within the lumen of the urinary tract
1.Calculi are by far the commonest cause of obstruction of the urinary tract.2. A sloughed papilla in papillary necrosis is a rare cause of ureteric obstruction.

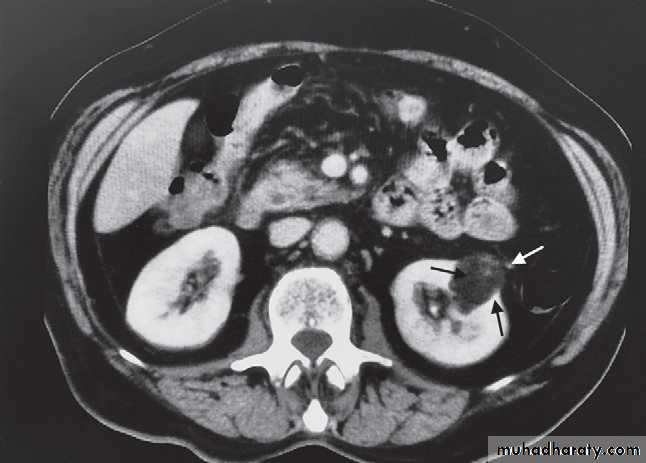
3. Blood clot within the collecting system needs to be differentiated from other causes such as stones or a tumour .
Causes arising in the wall of the collecting system
-A transitional cell carcinoma (TCC) within the ureter or the bladder in the region of the vesicoureteric junction may cause obstruction (a TCC in the pelvicaliceal system rarely causes obstruction).

-Carcinoma of the bladder causing ureteric obstruction can usually be identified on IVU, ultrasound, CT or MRI, though cystoscopy is the best method of establishing the diagnosis.
-Infective strictures of the collecting systems are mostly due to tuberculosis or schistosomiasis. In the case of tuberculosis there is usually other imaging evidence to suggestthe diagnosis .


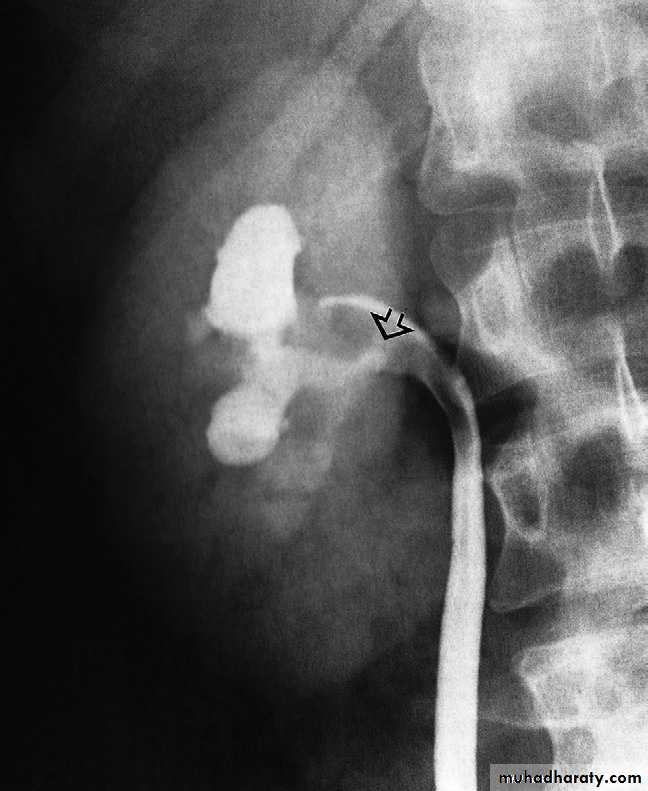
-Congenital intrinsic pelviureteric junction obstruction(PUJ obstruction ):The diagnosis depends on identifying dilatation of the renal pelvis and calices, with an abrupt change in calibre at the PUJ with normal ureter .

Extrinsic causes of obstruction
-Tumours. Carcinoma of the cervix, ovary and rectosigmoidcolon and malignant lymph node enlargement are frequent
causes of ureteric obstruction. CT is the ideal method of diagnosis because it shows the tumour mass as well as the level of obstruction.
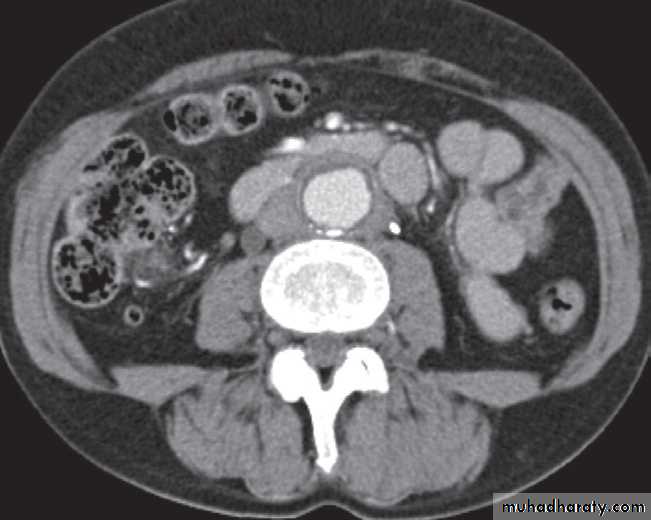
-Retroperitoneal fibrosis. In most cases, no cause can be found for this benign fibrotic condition, which encases the ureters and causes obstruction. When first seen, only one side may be obstructed but, eventually, the condition becomes bilateral.
The obstruction is usually at the L4/5 level. Fibrosis may extend superiorly to surround the kidneys and inferiorly to involve the pelvic side walls. CT has become the diagnostic method of choice.


Renal parenchymal masses
Solitary masses arising within the renal parenchyma are either malignant tumours or simple cysts .In adults, amalignant tumour is almost certain to be a renal cell carcinoma, whereas in young children it is usually Wilms’tumour.
Multiple renal masses include:
• Multiple simple cysts.
• Polycystic disease.
• Malignant lymphoma.
• Metastases.
•Inflammatory masses.
Ultrasound
Renal masses are usually first detected at ultrasound examination.Ultrasound can establish whether a mass is a simple cyst and can, therefore, be ignored, or whether the lesion is solid and, therefore, is likely to be a renal carcinoma.( further evaluation with CT is indicated ) .
-A mass with mixed cystic and solid features falls into the indeterminate category and could be a renal tumour, a renal abscess, or possibly a complex benign cyst or other benign condition ( also further evalution with CT scan is indicated )




Angiomyolipomas .are a fairly frequent incidental finding at ultrasound, appearing as small echogenic masses. CT or MRI may be used to confirm the diagnosis .
Solid masses may be irregular in outline and contain calcifications.
Intravenous urography
The initial diagnosis of a renal mass is now rarely madeon IVU as ultrasound and CT are the usual primary modalities.Computed tomography
CT may be used to
- Differentiate cysts from tumours.
- Diagnose angiomyolipomas
- To stage renal carcinoma.
Renal masses may be characterized on MRI, but this is usually reserved for solving specific problems.
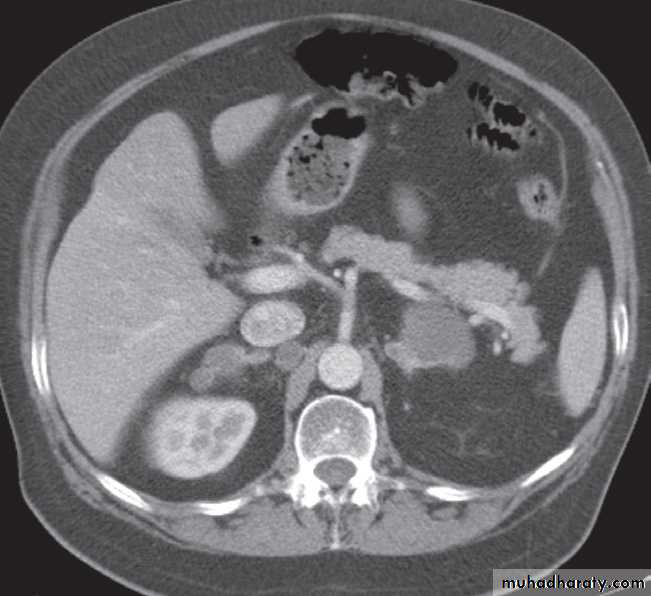
At CT:
-A typical simple renal cyst is a spherical mass with an imperceptible wall . The interior of the cyst is homogeneous with attenuation values similar to water.
-Angiomyolipomas are usually incidental findings. They are benign tumours, which rarely cause problems, although, on occasion, they cause significant retroperitoneal haemorrhage.
At CT their fat content allows a confident diagnosis (Fig. 8.32b, c).

-Renal cell carcinomas are approximately spherical and often lobulated .With density similar to renal parenchyma or slightly less with often seen some areas of necrosis & calcification .
Staging of renal cell carcinoma is usually undertaken with CT, the current method of choice .

Wilms’ tumour is the likely diagnosis in a child with a renal mass. These lesions are frequently large and may contain stippled calcification

Urothelial tumours
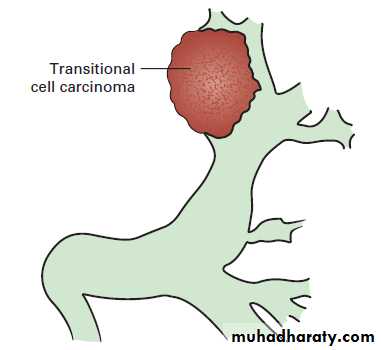
Almost all tumours that arise within the collecting systems of the kidneys are transitional cell carcinomas.Computed tomography is used for demonstrating the upper tracts (pelvicalicealsystem and ureters) & staging them .
In the pelvicaliceal system, TCCs are seen as lobulated or, very occasionally, as fronded filling defects projecting into the lumen .
The differential diagnosis of a filling defect in the collecting systems includes calculi and blood clot.

Ultrasound, TCCs can be difficult to see because they blend with the renal sinus fat, although large tumours can usually be demonstrated as a central mass within the sinus .
Ultrasound may help to differentiate between a radiolucent stone and tumour, as the calculus demonstrates acoustic shadowing.
Computed tomography urography demonstrates thickening of the wall of the ureter at the site of a urothelial tumour. The ureter is often obstructed at the level of a TCC.
Acute pyelonephritis
Acute pyelonephritis is usually due to bacterial infection from organisms that enter the urinary system via the urethra.Most patients with acute urinary tract infection do not require urgent imaging investigations. In patients presenting with signs of infection associated with pain, ultrasound and plain films may diagnose underlying stones, obstruction or abscess formation.
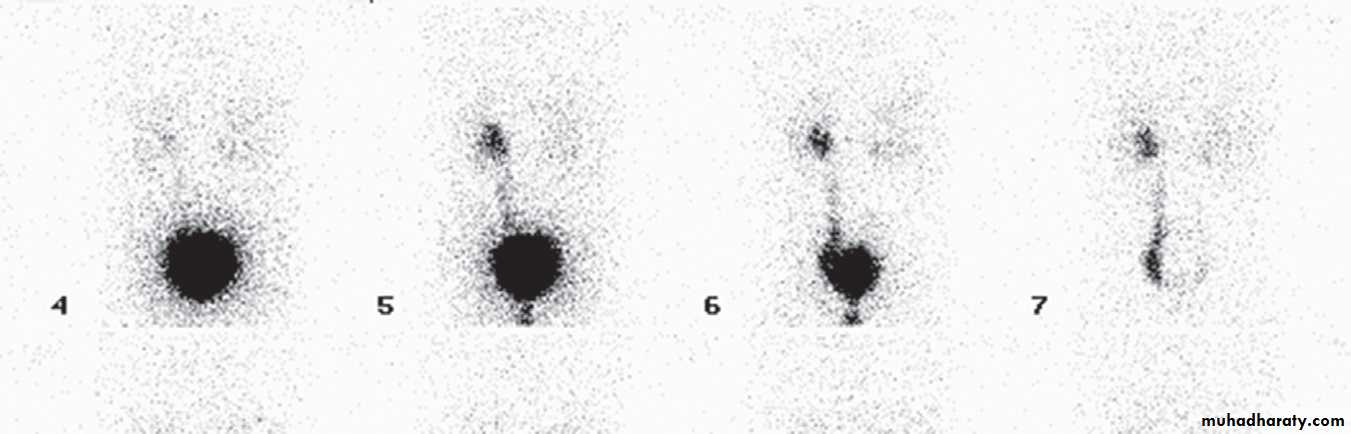
Investigation of the renal tract is indicated in all children with confirmed urinary tract infection. The aim is to identify an abnormality, such as reflux, which could lead to renal damage, if left untreated.
radionuclide scan of the kidneys to demonstrate scarring, Micturating cystography is performed in male (and in some female) children to look for vesicoureteric reflux and urethral valve.
Renal and perinephric abscesses
Ultrasound is the initial imaging investigation in most suspected renal abscesses, although in patients who are very unwell CT is often the first imaging investigation.Intrarenal abscesses may have thick walls and show both cystic and solid components recognizable at both ultrasound and CT, but may just look like a simple cyst.

Perinephric abscesses :may conform to the shape of the underlying kidney. The CT and sonographic characteristics are variable, usually showing both solid and cystic elements .

Tuberculosis
Urinary tuberculosis follows blood-borne spread of Mycobacterium tuberculosis, usually from a focus of infection in the lung. The tubercle bacilli infect the cortex of the kidneys and may cause tiny cortical granulomas, which rupture through capillaries into the renal tubules and involve other portions of the urinary and genital systems.In the early stages of the disease, the ultrasound and IVU may be normal.
There are various signs that develop in the later stages that are best seen on IVU:
• Calcification is common. Usually, there are one o more foci of irregular calcification, but in advanced cases with longstanding tuberculous pyonephrosis the majority of the kidney and hydronephrotic collecting system may be calcified, leading to a so-called autonephrectomy. Calcification implies healing but does not mean that the disease is inactive.
• The earliest change on the post contrast films is irregularity of a calix. Later, a definite contrast-filled cavity maybe seen adjacent to the calyx.
• Strictures of any portion of the pelvicaliceal system or ureter may occur, producing dilatation of one or more calices.
The multiplicity of strictures is an important diagnostic feature.
• If the bladder is involved, the wall is irregular because of inflammatory oedema; advanced disease causes fibrosis resulting in a thick-walled, small volume bladder. Multiple strictures may be seen in the urethra.
Ultrasound may demonstrate calcifications and pelvicaliceal dilatation and cavities, but the appearances are nonspecific.CT can sensitively demonstrate early calcifications, small cavities and extrarenal spread.