Peripheral Neuropathy :
describes disorders of peripheral nerves, including the dorsal or ventral nerve roots; dorsal root ganglia; brachial or lumbosacral plexus; cranial nerves (except I and II); and other sensory, motor, autonomic,or mixed nerves.Classification Of Peripheral Neuropathy:
1- mononeuropathy:a- focal :due to compression ex. Carpal tunnel syndrome or ischemia ex.diabetic mononeuropathy.
b- multiplex ex. Diabetes ,diphtheria, connective tissue disease ,etc…
2- poly neuropathy :
a-demyelination : the lesion is in the myelin sheath ex. Gullian Barri syndrome and CIDP.
b- axonal : the lesion is in the nerve axon ex. Diabetic polyneuropathy and alcoholic neuropathy .
Causes Of Neuropathy :
1- immune :GBS,CIDP ,MMN .2- metabolic : hypothyroidism, achromegaly,diabetes ,porphyria.
3- connective tissue disease :SLE,RA,polyarteritis nodosa.
4- compressive :Carpel tunnel syndrome, trauma .
5- nutritional : B12 , Vit. E and Cupper deficiency.
6- paraneoplastic neuropathy .
7- toxins and drugs :alcohol ,cisplatin ,mercury ,amiodarone .
8- infectious :lyme, diphtheria ,CMV ,EBV .
9- hereditary : Charcot Marie Tooth syndrome .
Clinical features
Motor nerve involvement produces features of a lower motor neuron lesion. Symptom s and signs of sensory nerve involvement depend on the type of sensory nerve involved. Autonomic fibers involvement may cause postural hypotension due to disruption of vasomotor control, or disturbance of sweating, cardiac rhythm , and gastrointestinal, bladder and sexual functions .
Investigations
Investigations required in a patient with peripheral neuropathy reflect wide spectrum of causes. Neurophysiological tests , and sometimes nerve biopsy , will help determine whether the pathology is primarily affecting the nerve ax on (axonal neuropathy), the myelin sheath (demyelinating neuropathy) or the blood vessels .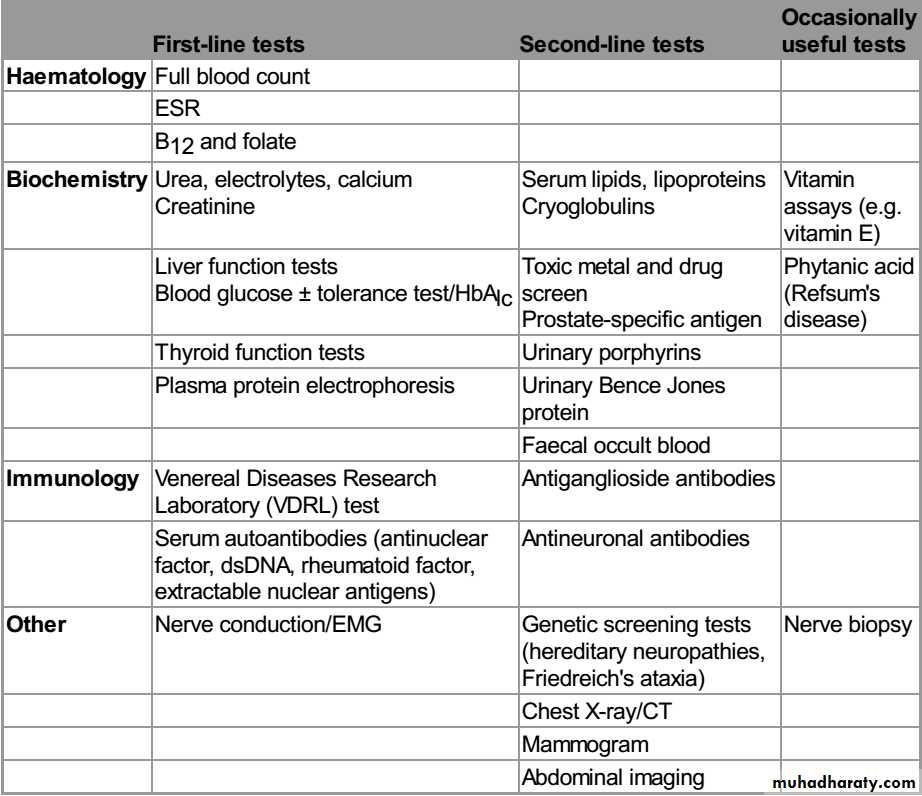
Entrapment neuropathy
Focal compression or entrapment is the usual cause of a mononeuropathy. However , some patients present with what initially appears to be a single nerve lesion and then go on to develop multiple nerve lesions. This is termed mononeuritis multiplex . In this situation pressure damages the myelin sheath, and neurophysiology studies show slowing of conduction over the relevant site ..Certain conditions increase the propensity to develop entrapment.These include acromegaly , hypothyroidism , pregnancy , any pre-existing mild generalized axonal neuropathy such as diabetes. Unless axonal loss has occurred, entrapment neuropathies will recover , provided the pressure on the nerve is relieved, either by avoiding precipitating activities or limb positions, or by surgical decompression. Cranial nerves may also be the target of entrapment neuropathy .
Carpel Tunnel syndrome :
The median nerve pass below the flexor retinaculum in the wrist; so any condition that cause thickening of this structure or the structures near it will cause pressure on the median nerve.
Causes :
1- Diabetes Mellitus .
2- Pregnancy.
3- alcoholism.
4- mechanical so more common in housewives and heavy workers .
5- hypothyroidism .
6- Rheumatoid arthritis .
7- sarcoidosis .
8- amyloidosis .
9- acromegaly.
Clinical features :
Pain and parasthesia on palmer aspect of the hand and fingers(lateral 3and a half fingers) ,this occur mainly in the dominant side ,sometimes awake the patient from sleep.; this is followed by weakness in the medial nerve innervated muscles .
An important sign what is called index pointing sign which occur during flexion of the fingers ,there will be only flexion of 4th and 5th fingers with extension of the index and 3rd finger due to weakness of the 1st and 2nd flexor digitorum profondus muscles (median nerve innervated ) .
Investigation :
Usually the diagnosis is clinical but there is some indications for sending the patient for investigations :1-bilateral CTS.
2- positive family history .
3- non dominant side .
4- no respond to treatment .
5- atrophy of the hand .
The investigation include :
1- nerve conductive study and EMG: confirm the diagnosis and important also in the prognosis (demyelinating or axonal type ) .
2-FBS and Hb A1c.
3-Rheumatoid factor ,ESR & CRP .
4- Thyroid function test .
5- CXR for sarcoidosis .
6- finally nerve biopsy for cryptogenic type .
Treatment :
1- fixation of the hand during sleep .2- NSAIDs
3- Antidepressant :Tricyclic , duloxetine .
4- anticonvulsants : carbamazepine , gabapentine &pregabaline .
5- steroid injection locally .
6- surgery is indicated in :
a- sever symptoms not respond to treatment .
b- impending atrophy of the muscles .
c- axonal type .
Idiopathic facial nerve palsy : Bell's palsy :
Is a common condition affecting all age groups and both sexes .the lesion is within the facial canal due to reactivation of the Herpes simplex virus type 1 .the symptoms develop subacutely within hours with pain around the ear preceding the unilateral facial weakness .the patient describe the face as numb but there is no objective sensory loss except for taste .Hyper acusis can occur if stapedius muscle is involved with also diminished salivation and tear .Examination show only LMN facial palsy .
NO need for investigations just if we suspect immunocompromization (FBS &RFT) .prednisolone 40- 60 mg /day for 7-10 days should be taken in the 1st 3 days of the disease .artificial tears to protect the eye from secondary infections .the eye should be taped shut during sleep .
Poor prognosis occur if :
1- complete paralysis .2- alder age .
3- axonal type .
Recurrence can occur and this indicate for investigations.
Sometimes aberrant regeneration occur during recovery period leading to tearing during salivation "crocodile tears " or eye blinking during smiling .