Urology

Saturday 7/11/2015
HydronephrosisHydronephrosis: is an aseptic dilatation of the renal collecting system caused by obstruction to the outflow of urine. Hydroureter is defined as a dilatation of the ureter. The presence of hydronephrosis &/or hydroureter can be physiologic or pathologic.
Hydronephrosis/hydroureter caused by obstruction anywhere in the urinary tract may be acute or chronic, unilateral or bilateral.
Hydronephrosis or hydroureter is a normal finding in pregnant women. The renal pelvis and caliceal systems may be dilated as a result of progesterone effects and mechanical compression of the ureters at the pelvic brim. Dilatation of the ureters and renal pelvis is more prominent on the right side than the left side.
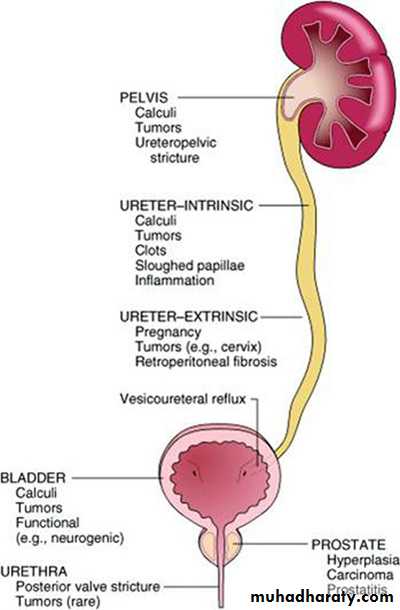
Unilateral hydronephrosis:
Affects only one side. Causes may be inside or outside the urinary tract.Causes:
Extramural compression
Tumor from adjacent structures, e.g. carcinoma of the cervix, prostate, rectum, colon or caecum.
Idiopathic retroperitoneal fibrosis
Retrocaval ureter
Intramural obstruction
Congenital stenosis, eg. pelviureteric junction obstruction (PUJO).
Ureterocele and congenital small ureteric orifice
Inflammatory stricture of the ureter.
Neoplasm of the ureter or bladder.
Intraluminal obstruction
Calculus (stone) in the renal pelvis or ureter
Sloughed papilla.
Bilateral Hydronephrosis:
Bilateral hydronephrosis is usually the result of urethral obstruction, but the lesions described above may occur on both sides.
Congenital:
posterior urethral valves
urethral atresia.
Acquired:
benign prostatic enlargement or carcinoma of the prostate
postoperative bladder neck scarring
urethral stricture
phimosis.
Other Causes of Hydronephrosis:
Infection.Vesicoureteric Reflux.
Residual (after surgery)
Pregnancy
There is calyceal dilatation and the renal parenchyma is destroyed by pressure atrophy. A kidney destroyed by longstanding hydronephrosis is a thin-walled, lobulated, fluid-filled sac.
Pathophysiology:
Clinical Presentation:
History:Unilateral Hydronephrosis:
Mild pain or dull aching in the loin, often with a sensation of dragging heaviness made worse by excessive fluid intake. The kidney may be palpable.
Attacks of acute renal colic may occur with no palpable swelling.
Intermittent hydronephrosis (Dietl’s crisis). A swelling in the loin is associated with acute renal pain. Some hours later the pain is relieved and the swelling disappears when a large volume of urine is passed.
Antenatal detection in the fetus by ultrasound scan.
Bilateral Hydronephrosis:
From lower urinary obstruction: Symptoms of bladder outflow obstruction.From bilateral upper urinary tract obstruction: This is rare compared with unilateral lesions.
From pregnancy: This physiological condition is associated with an increased liability to infection and there is a possibility of abdominal pain during pregnancy.
A history of hematuria may be due to a stone or malignancy anywhere in the urinary tract. Hydronephrosis may develop silently, without symptoms, as the result of advanced pelvic malignancy or severe urinary retention from bladder outlet obstruction.
Examination:
Kidney may be palpable in severe hydronephrosis.Bladder may be distended in lower urinary tract obstruction.
There may be features of uremia in obstructive cases.
In children .. especially newborn:
Palpable kidney: eg. Congenital hydronephrosis.
Palpable bladder: eg. Posterior urethral valve.
Distended abdomen: eg. Prune-belly Syndrome.
Investigations:
Laboratory Studies:
Urinalysis: to assess for infection. Hematuria may indicate stone or tumor.
Complete blood cell count may reveal leukocytosis.
Blood chemistry:
BUN and creatinine may be elevated in renal impairment.
Hyperkalemia.
Imaging Studies:
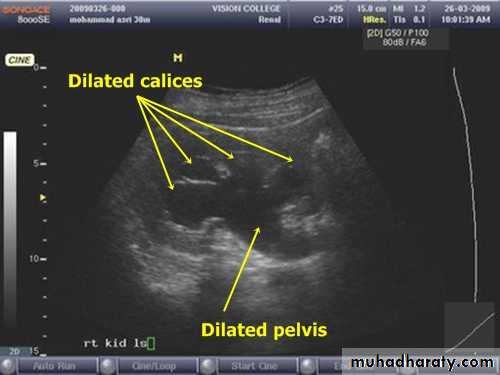
Early diagnosis of urinary tract obstruction is important because most cases can be corrected and a delay in therapy can lead to irreversible renal damage.Ultrasound Scan (USS): Simple and non-invasive. In most cases it can diagnose hydronephrosis and may detect its cause.
Plain abdominal film (KUB): may detect stone.
Intravenous urography (IVU): reveals hydronephrosis and its level and may also show the underlying cause. It requires good preparation and the injection of a contrast material which may cause allergy.
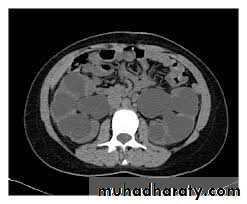
Computed Tomography (CT) scan: highly sensitive in diagnosing hydronephrosis and its cause.
Other less commonly used investigations may be required depending on the clinical situation..
Antegrade and retrograde contrast studies.
Micturating Cystourethrography (MCUG): for detecting reflux and posterior urethral valves.
Pressure studies (Whitaker study).
Magnetic resonance Imaging and Urography: MRI & MRU.
USS Showing hydronephrosis
CT scan Showing bilateral hydronephrosis
IVU Showing unilateral (left) hydronephrosis - PUJO

IVU Showing unilateral (right) hydroureteronephrosis
Management:Conservation of renal tissue is the aim; nephrectomy should be considered only when the renal parenchyma has been largely destroyed. Mild cases should be followed by serial ultrasound scans and operated upon if dilatation is increasing.
Indications of Treatment:
Bouts of renal pain
Increasing hydronephrosis
Evidence of parenchymal damage and infection.
Medical Care:
The role of medical treatment of hydronephrosis and hydroureter in adult is limited to pain control and treatment or prevention of infection. Most conditions require either minimally invasive or open surgical treatment.
Surgical Care:
The specific treatment depends on the underlying cause. Management should be urgent in cases where infection is present or there is potential for loss of renal function, eg. in solitary kidney. Severe symptoms may also mandate rapid action such as intractable pain or persistent nausea and vomiting.Options of Surgical Management:
Urethral catheter placement.
Endoscopic intervention: Cystoscopy or ureteroscopy with stent insertion.
Temporary urinary diversion: eg. percutaneous nephrostomy.
Definitive management of the causative factor.
Complications:
Post-obstructive diuresis: refers to polyuria that occurs after relief of obstruction. It is more common in patients with chronic obstruction. Post-obstructive diuresis is usually clinically significant only in patients whose obstruction involves both kidneys or a unilateral obstruction of a solitary functioning kidney. Management involves avoiding severe volume depletion, hypokalemia, hyponatremia, hypernatremia, and hypomagnesemia.
Irreversible renal damage which may mandate nephrectomy.
Pyonephrosis
Pyonephrosis is an infected hydronephrosis where pus accumulates within the renal pelvis and calyces. It is associated with damage to the parenchyma, resulting in loss of renal function. The causes are essentially those of hydronephrosis, where infection has supervened (e.g. ureteric obstruction by stone, PUJ obstruction).Presentation: Patients with pyonephrosis are usually very unwell, with a high fever, flank pain, and tenderness.
Risk Factors: Stone disease, previous urinary tract infection, or surgery.
Investigations:
KUB: may show air n the pelvicalyceal system.
USS: may show debris in the dilated collecting system.
CT scan.
Treatment: Intravenous fluid and antibiotics, with urgent percutaneous drainage (nephrostomy) or ureterc drainage via endoscope.