Medication and Acute Kidney Injury
By:Dr. Wael Thanoon Younis
C.A.B.M.,Mosul college of medicine.
Why do we need to consider medication in AKI
Prescribing medication is a common interventionComplacent - medicines are dangerous
Between 5 and 20 % of all AKI cases occur as a direct result of medication
We need to consider medication because:
Wide range of drugs which can cause/contribute to AKIKidneys are responsible for the metabolism of two drugs:- vitamin D and insulin
Kidneys are responsible for the excretion of many water soluble drugs and their metabolites
Why do we need to consider medication in AKI?
On admission, a thorough review of medication is required to:Identify drugs which have potentially caused/contributed to AKI
Avoid inappropriate combinations of medications which may exacerbate AKI
Ensure all doses of medications prescribed continue to be correct and clinically appropriate
Common medications which can contribute to, or are affected by, AKI:
Several options when reviewing medication in AKI:
Stop
Withhold
Amend
Continue
First we need to know which medications to pay attention to
Common medications which can contribute to, or are affected by, AKI
Consider Acute Nephrotoxic Drug ActionContrast media
ACE InhibitorsNSAID’S
Diuretics
ARB’s
Contrast media
Contrast induced nephropathyCan occur in any patient with intra venous or intra-arterial contrast
Known renal dysfunction or CrCl = <60mls/min, consider non-contrast imaging
Oral N-acetylcysteine – antioxidant. Neutralises free radicals
IV sodium bicarbonate can also be used
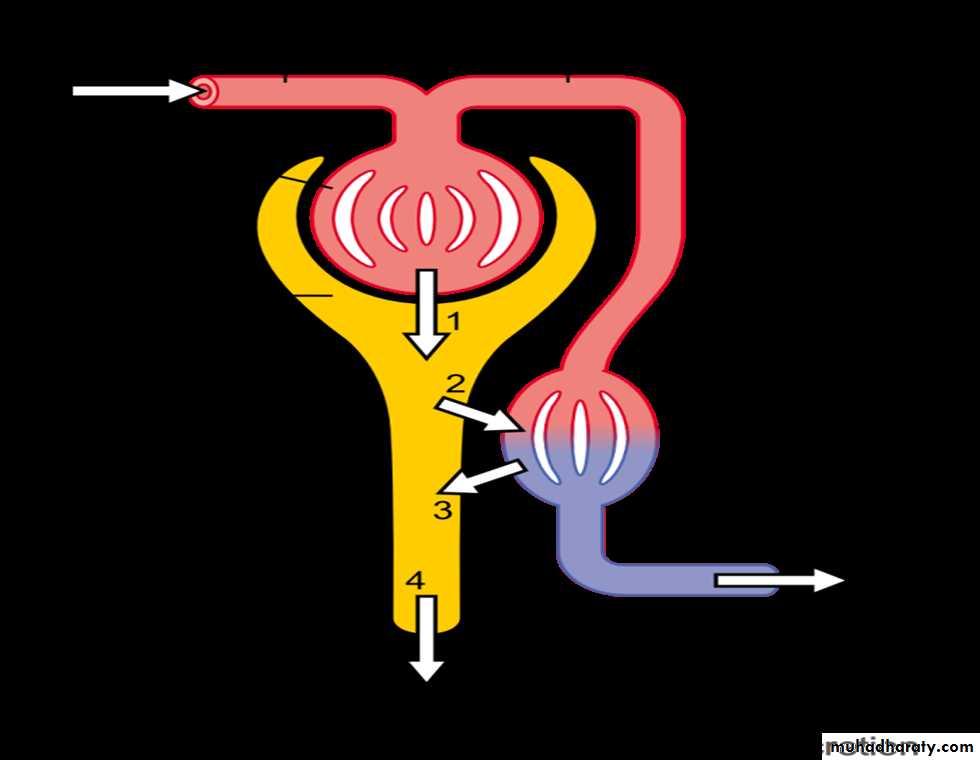
ACE Inhibitors
Used to treat hypertension, heart failure, nephropathy
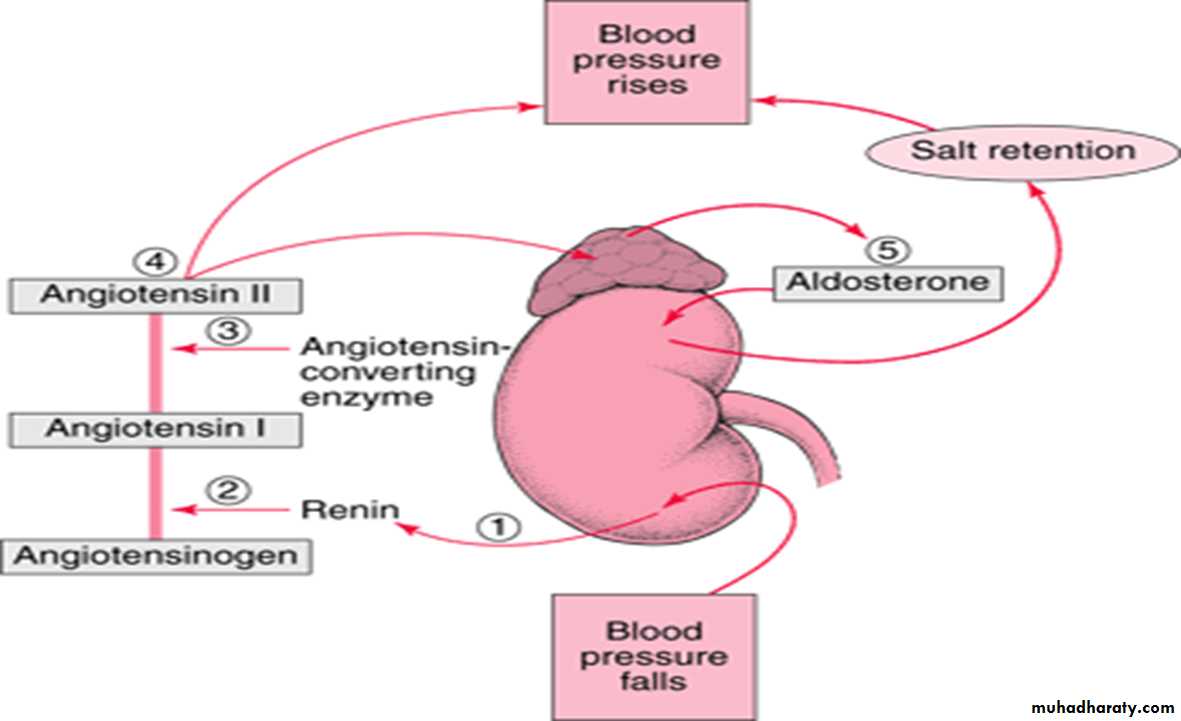
Work on the RAAS system
Inhibit conversion of angiotensin I to angiotensin II
Dilate efferent arterioles
Reduced renal perfusion and GFR
Hyperkalaemia – potassium retention due to reduction of aldosterone
NSAIDS
Analgesic, antipyretic and anti-inflammatoryNon-selective COX inhibitors
Acetic acids – diclofenac, indomethacin
Proprionic acids – ibuprofen, naproxen
Salicylates - aspirin
Enolic acid derivatives – meloxicam
Anthranilic acid derivatives – mefenamic acid
Two other groups which we never see
Selective COX II inhibitors - celecoxib
Inhibit cyclooxygenase
Impair prostaglandin synthesis
Prostaglandins usually mediate renal blood flow
Reduced prostaglandin synthesis = Reduced renal perfusion
Tend to promote sodium retention and subsequent fluid retention therefore increasing blood pressure.
NSAID’s cause constriction HERE.
DiureticsThree main classes of diuretic
Loop diuretics
• Act on the ascending links of the loop of Henle
• Inhibit reuptake of sodium
• Less water uptake therefore increased urine production
• Reduced circulating volume
• Reduced renal perfusion
Potassium sparing diuretics
• Act on the distal convoluted tubule• Competitive antagonists which inhibit sodium/potassium exchange
• Inhibits reuptake of sodium therefore increasing water excretion.
• Reduces excretion of potassium - Hyperkalaemia
Thiazide diuretics
• Act on distal convoluted tubule
• Inhibit reuptake of sodium therefore increasing water excretion
• Causes volume depletion and hypoperfusion
Angiotensin Receptor Blockers:
Antagonise the action of angiotensin II by blocking the angiotensin II AT1-receptor.
Reduces production and secretion of aldosterone
Hyperkalaemia – potassium retention due to reduction of aldosterone
Other ‘problem’ drugs:
AnalgesicsOpiates –. Reduce dose of standard release preps. Risk of accumulation.
Fentanyl – minimal renal excretion
Antibiotics
Aminoglycosides – gentamicin – AVOID
Glycopeptides – vancomycin - AVOID
Antiepileptics
Consider reducing dose and/or monitoring levels
Anticholinergics
Can cause urinary retentionAntihistamines
Antipsychotics
Antispasmodic
Reduce dose
Digoxin
Accumulates – monitor level and consider reducing dose
Lipid lowering agents
Statins
Fibrates
increased risk of rhabdomyolysis
Lithium
Accumulation
Can cause chronic interstitial nephropathy
Proton pump inhibitors PPIs.
‘Sick Day Rules’
Many health care professionals provide advice to such patients that certain drugs should be temporarily discontinued during acute intercurrent illnesses, particularly where there is disturbed fluid balance. This advice is commonly described as ‘sick day rules’ or to take a ‘drug holiday’..
There are three main reasons for providing such advice:
1. Non-steroidal anti-inflammatory drugs impair renal autoregulation by inhibiting prostaglandin-mediated vasodilatation of the afferent arteriole and may increase the risk of AKI.2. Drugs that lower blood pressure, or cause volume contraction, might increase the risk of AKI by reducing glomerular perfusion.
3. Drugs might accumulate as a result of reduced kidney function in AKI, increasing the risks of adverse effects.