RAISED INTRACRANIAL PRESSURE
for 5
th
class: medical college: Al Mustansiriyah University
by
Dr Mohamed Al Tamimi
INTRACRANIAL DYNAMICS
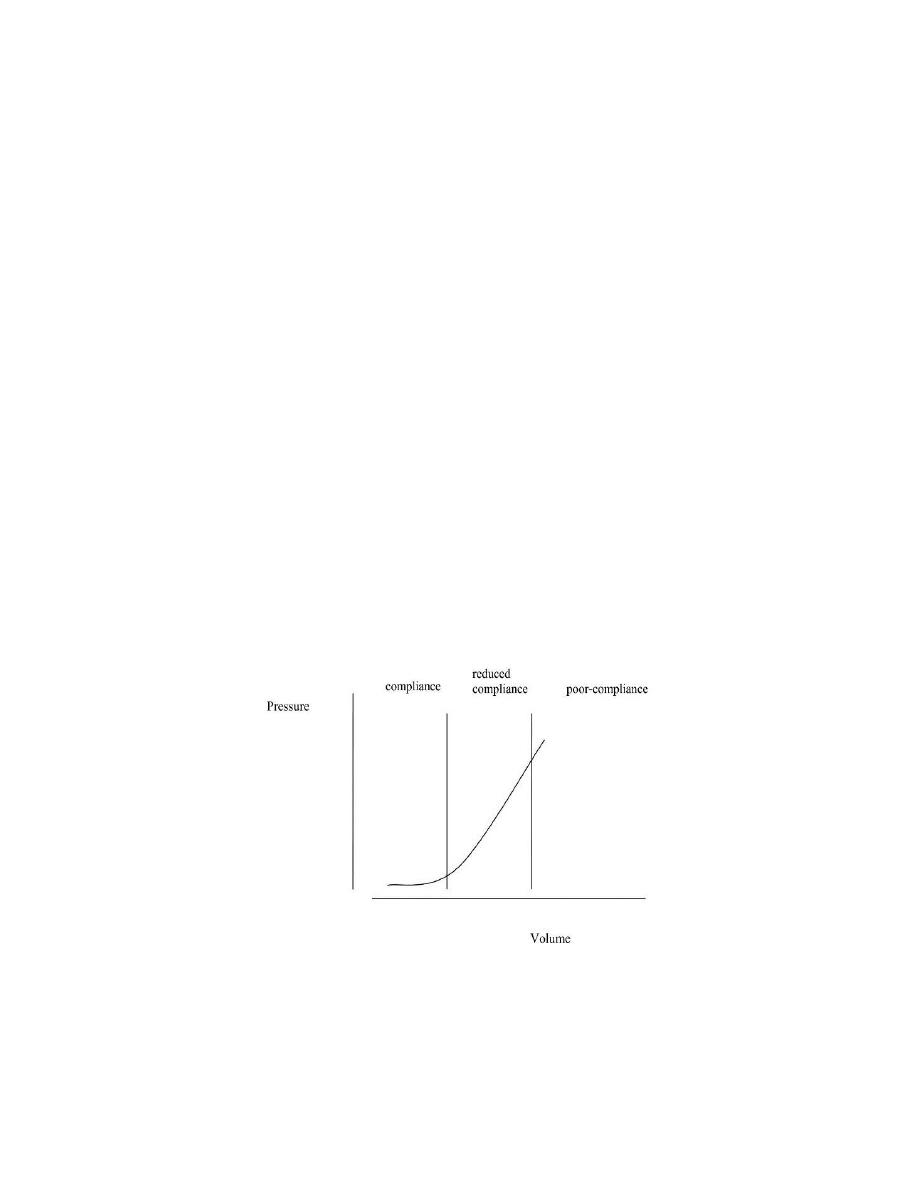
Intracranial Pressure/Volume Relationship
1. intracranial volume is constant
• Vbrain + Vblood + Vcsf + Vlesion = Vskull = constant
(Monro-Kellie hypothesis)
2. as lesion expands, ICP does not rise initially
• CSF, blood, some brain water displaced out of the head
• brain tissue may shift into compartments under less pressure
(herniation)
3. ICP then rises exponentially
4. normal ICP ~ 6-15 mm Hg (80-180 mm H2O) and varies with patient
position
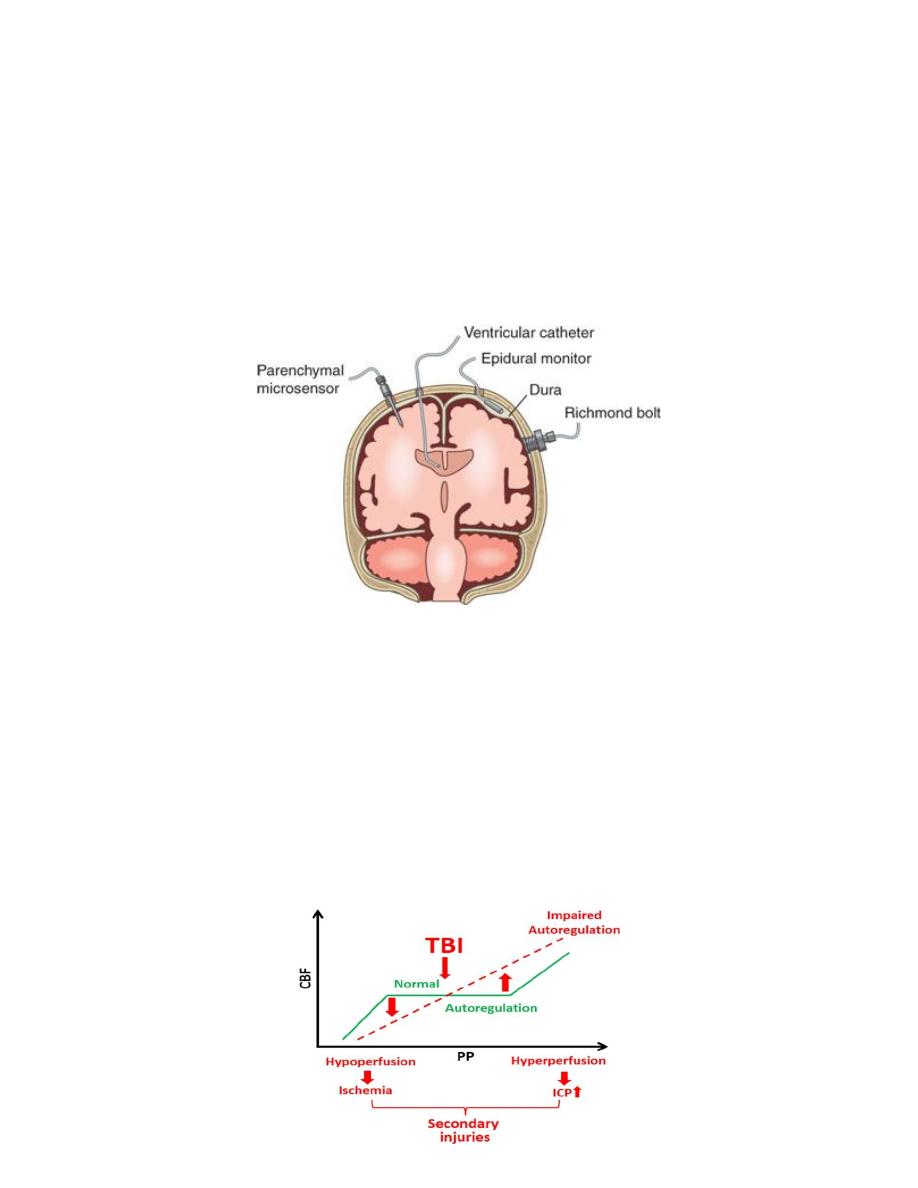
ICP Measurement
1. lumbar puncture (contraindicated with known/suspected intracranial mass
lesion)
2. ventricular catheter (also permits therapeutic drainage of CSF to decrease
ICP)
3. intraparenchymal monitor
4. subdural/subarachnoid monitor (Richmond bolt)
Cerebral Blood Flow (CBF)
*CBF depends on cerebral perfusion pressure (CPP) and cerebral vascular
resistance (CVR)
* CPP = MAP (mean arterial pressure) – ICP (intracranial pressure)
* cerebral auto regulation maintains constant CBF by compensating
forchanges in CPP, unless
• high ICP such that CPP < 40 mm Hg
• MAP > 160 mm Hg or MAP < 60 mm Hg
• brain injury: i.e. subarachnoid hemorrhage (SAH), severe trauma
Other factors may increase ICP by increasing intracranial blood volume
• pCO2
• CO2 is a powerful vasodilator
• CNS pathology ––> respiratory compromise ––>increased pCO2 ––>
increased
cerebral
vasodilatation––>
raised
ICP,
therefore
ventilate/hyperventilate ––> decreased pCO2––> vasoconstrict ––>
decreased ICP
• pO2 (< 60): decreased pO2 ––> vasodilate ––>raised ICP, therefore
prevent hypoxia
• decreased venous drainage
1. intracranial venous sinuses drain directly into superior vena cava
2.lying down, bending over, Valsalva all increase ICP
3. standing, raising head of bed both decrease ICP
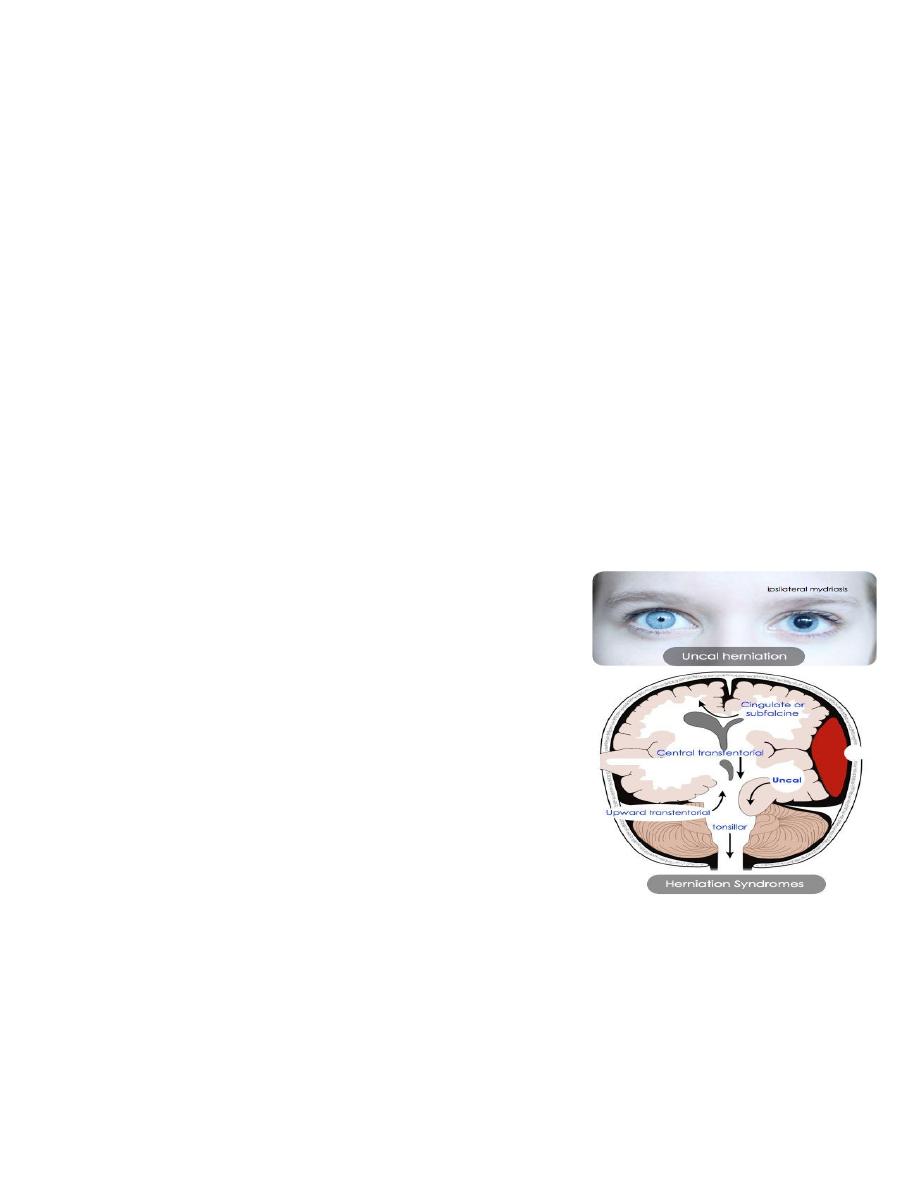
HERNIATION SYNDROMES
Subfalcine (Cingulate) Herniation
* definition: cingulate gyrus herniates under falx
* cause: supratentorial lateral lesion
* presentation
• pathological/radiological observation
• warns of impending transtentorial herniation
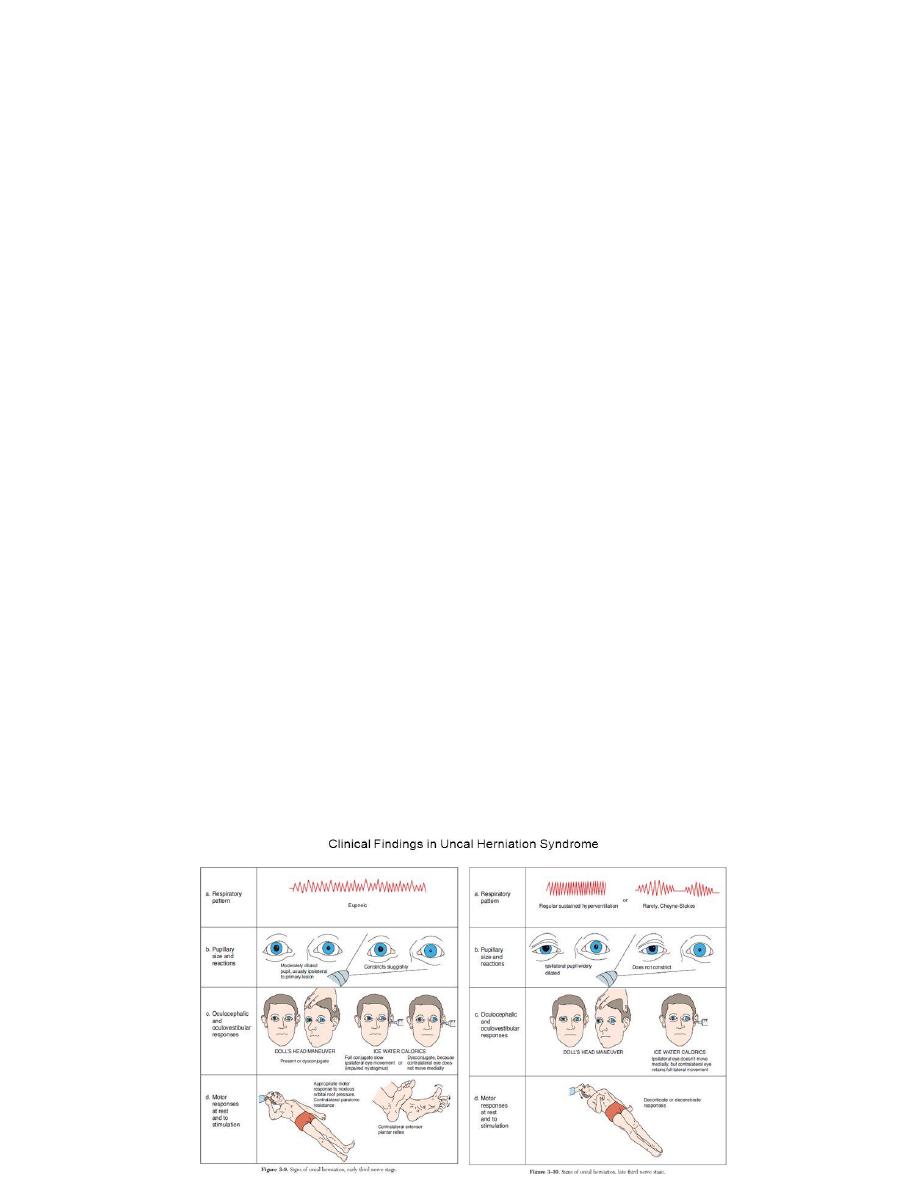
Lateral Tentorial (Uncal) Herniation
* definition: uncus of temporal lobe herniates down through tentorial notch
* cause: supratentorial lateral lesion (often rapidly expanding traumatic
hematoma)
* clinical presentation
• unilateral dilated pupil, followed by extraocular muscle (EOM) paralysis
(ipsilateral cranial nerve III compressed)

• decreased level of consciousness (LOC) (midbrain compressed)
• “Kernohan’s notch”: contralateral cerebral peduncle compressed due to
shift of brain ––> ipsilateral hemiplegia (afalse localizing sign)
Central Tentorial (Axial) Herniation
* definition: displacement of diencephalon and midbrain through tentorial
notch
* cause: supratentorial midline lesion, diffuse cerebral swelling, late uncal
herniation
* clinical presentation
• decreased LOC (midbrain compressed)
• EOM/upward gaze impairment (“sunset eyes”, pressure on superior
colliculus in midbrain compresses 3rd nerve nucleus)
• brainstem hemorrhage (Duret’s, secondary to shearing of basilar artery
perforating vessels)
• diabetes insipidus (traction on pituitary stalk and hypothalamus) - this is
an end stage sign
Tonsillar Herniation (“Coning”)
* definition: cerebellar tonsils herniate through foramen magnum
* cause: infratentorial lesion, or following central tentorial herniation
* clinical presentation
• rapidly fatal (compression of cardiovascular and respiratory centers in
medulla)
• may be precipitated by lumbar puncture (LP) in presence of space
occupying lesion (particularly in the posterior fossa)
CLINICAL FEATURES
Acute Raised ICP
1. headache
2. nausea and vomiting (N/V)
3. decreased LOC
4. Glasgow Coma Scale (GCS) best index to monitor progress and predict
outcome of acute intracranial process
5. papilledema: may take 24-48 hours to develop
6. CN palsy
• CN III: pupillary dilatation (unilateral dilated pupil signifies
herniation) (CN III compressed)
• CN VI: longest intracranial course, causative mass may be remote
from nerve root, i.e. CN VI palsy can be a false localizing sign
7. Cushing response: increased blood pressure (BP), decreased pulse
8. respiratory changes e.g. Cheyne Stokes, apneustic, ataxic
9. localizing neurologic signs may occur e.g. contralateral hemiplegia except
with Kernohan’s notch
10. paralysis of upward gaze especially in children (obstructive
hydrocephalus)
Chronic Raised ICP
1. headache
• postural: worsened by coughing, straining, bending over (Valsalva)
• morning H/A: worse on waking in the morning
2. visual changes( enlarged blind spot, long standing papilledema may
produce optic atrophy and blindness
Imaging Features
1. CT: key diagnostic investigation
• enlarged ventricles - hydrocephalus
• compressed ventricles with midline shift - mass lesion
2. skull x-rays: in chronic ICP may show
• separation of sutures in infants
• digital markings in skull vault from compression of brain matter against
bone (“copper beating”)
• thinning of dorsum sellae
MANAGEMENT
1. elevate head
• head of bed at 30-45 degrees ––> decreases intracranial venous
pressure
2. ventilate/hyperventilate( decreases pCO2, increases pO2, decreases
venous pressure
3. mannitol (20% IV solution preferred)
4. identify etiology CT, MRI
5. steroids
6. surgery
• remove mass lesion
• remove CSF by external ventricular catheter drain (if acute) or shunt
• Note: lumbar puncture contraindicated when known/suspected
intracranial mass lesion