Mechanism of normal labor
Definition of labor
The process by which regular painful contractions bring about progressive dilatation of the cervix &descend of the presenting part leading to expulsion of the fetus &the placenta from the mother.It is interplay between
.the power (uterine contraction)
.the passages (birth canal)
.the passenger (fetus)
Symptoms&signs of the onset of labour
Painful uterine contractionsThe show
Rupture of membranes
Shortening&dilatation of cervix
THE STAGES OF LABOUR
Labour is divided into three stages:FIRST STAGE,or stage of dilatation from onset of true labour until the cervix is fully dilated.
SECOND STAGE ,or stage of expulsion of fetus,from full dilatation of the cervix to delivery of fetus or fetuses.
THIRD STAGE ,from delivery of fetus until the placenta&membranes are delivered.
The onset of labour
Defined as regular contraction bringing cervical changes . The show(blood stained plug of mucus passed from the cervix) or rupture membranes does not defined the onset of labour
The uterus contract irregularly&painlessly throughout pregnancy[Braxton hicks contractions]
Rupture of the membranes
The membranes may rupture at any time during labour&usually occurs towards the end of first stage of labour. Early rupture of membranes is more likely to occur if the presenting part not engaged or there is malpresentation.First stage of labor
Describes the time from the diagnosis of labor to full dilatation of cervix(10cm)Divided into LATENT PHASE :IS the time between the onset to cervical dilatation of 3-4 usually last 3-8hr
ACTIVE PHASE :between the end of latent phase to the 10cm usually 2-6hr
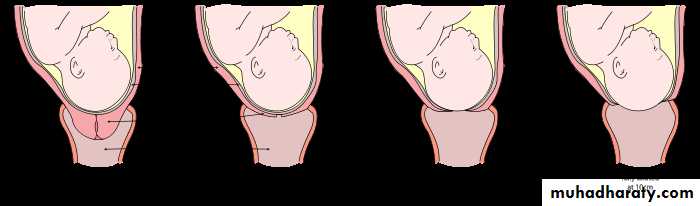
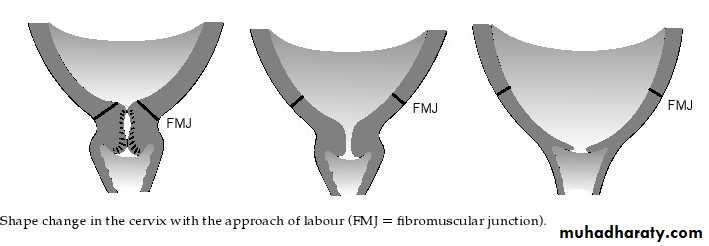
Effacement:is the process by which the cervix shortens in length as it becomes included into lower segment may start weeks before labor
FIRST STAGE OF LABOUR
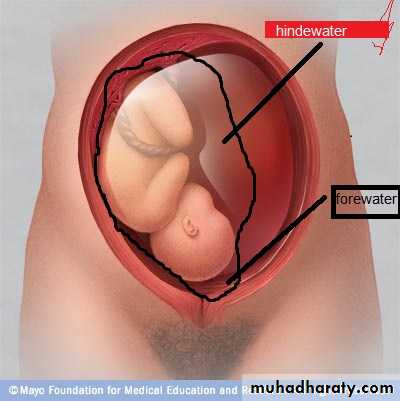
The uterine contraction&dilatation of internal os cause separation of chorion from decidua closest to it thus a small back of membranes is formed into the internal os,the head then comes down separates liquor amnii which is above it from that in the back called respectively the hind&fore waters.When membranes ruptured the fetal axis pressure comes into play ;the upper pole of fetus is pressed on by the fundus of the uterus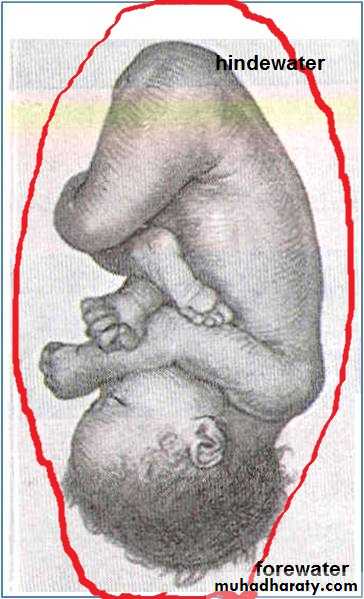
Normal first stage should not exceed 12 hours in a primegravida &8 hours in multipara.
The character of pain is the same as spasmodic dysmenorrhoea caused by ischaemia of uterine muscles from compression of blood vessels in the wall of the uterusTHE SECOND STAGE OF LABOUR
The presenting part is pushed down onto the pelvic floor,pelvic floor resistance has to be overcome by uterine contractions ,aided by the action of the voluntary muscles of the abdominal wall&diaphragm.
As contraction comes on patient takes a deep breath then bears down with all the force of her abdominal muscles ,during height of pain there may be expiratory groans.
2nd stage
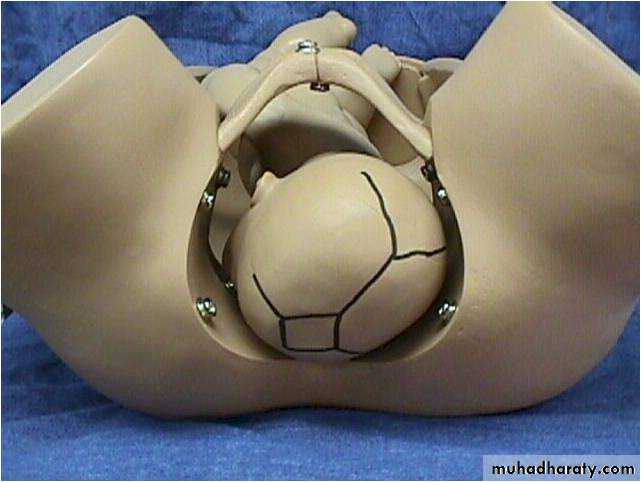
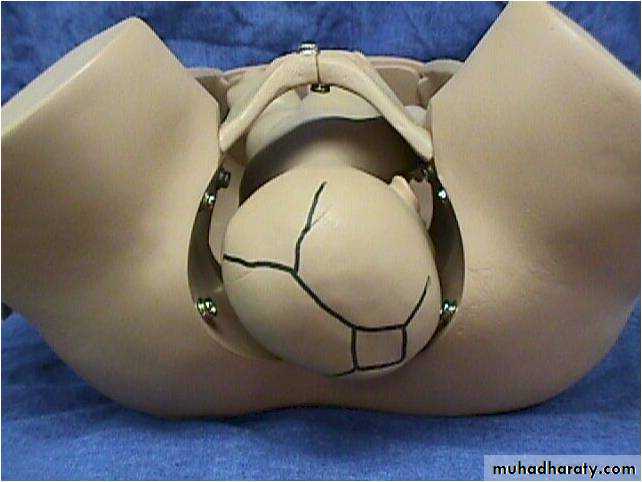
With each contraction the presenting part is forced down to pelvic floor , during intervals between contraction at first slipped back. After this ,with contraction &expulsive effort make the head slowly moves down in a forward direction,when the widest diameter of the head distends the vulva it is said to be crowned.Then the head passed through vulva followed by the body in next contractionThe third stage of labour
As the cavity of the uterus becomes smaller after delivery the placenta is shorn off the spongy layer of decidua basalis,further uterine contractions expel the placenta from the upper segment into the lower segment& vaginal vault this is called separation of placenta (5-10)when a cleavage plane develop whithin the decidua basalisThe placenta is expelled from vagina followed by membranes &any retroplacental blood clot.
THE MECHANISM OF LABOUR
This is referred to series of changes in position&attitude which the fetus undergoes during its passage through the birth canal.Lie
The relation of the long axis of the fetus to the uterus,this may be longitudinal,oblique or transverse.
•
•

• .'" '
• I• ! 1\
• 11
• A
• B
• ii
• F
• c
• D
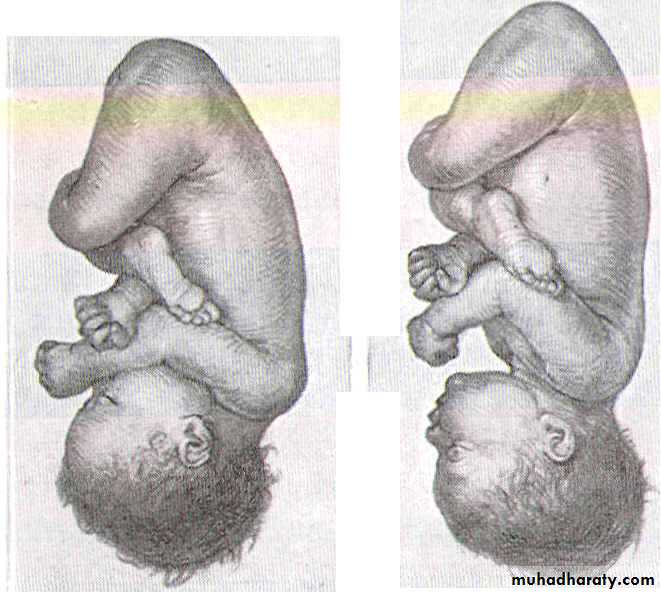
• Longitudinal lie. Cephalic presentation. Differences in attitude of fetal body,
• Note changes in fetal attitude in relation to fetal vertex as the fetal head becomes less flexed.
(A) vertex
(B) sinciput
(C) brow
(D) face
Prsentation
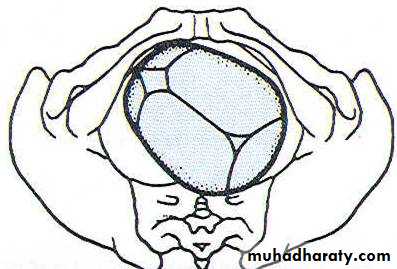
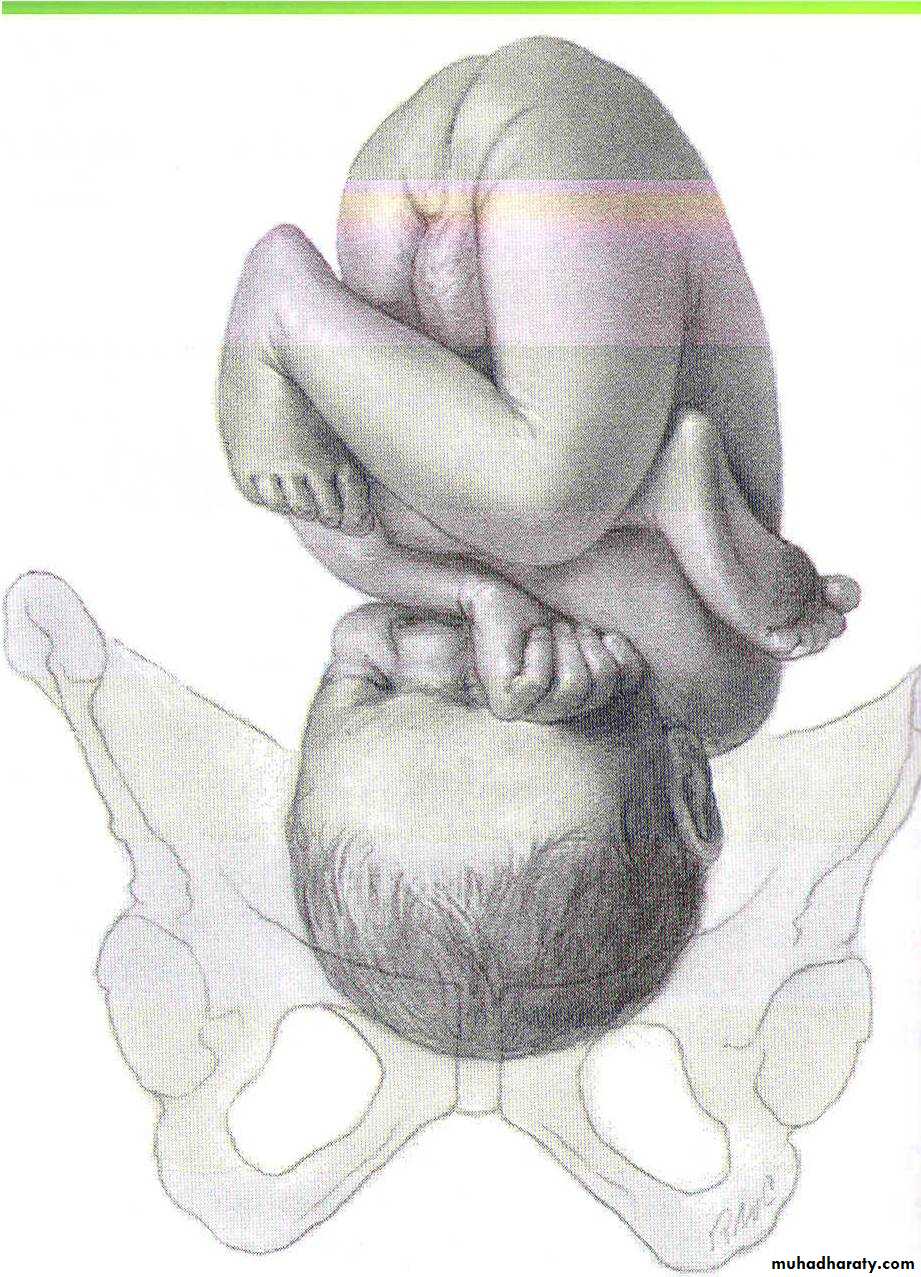
The lowest pole of the fetus that presents to the lower uterine segment & the cervix or defind as that part of the fetus in or over the pelvic brim in relation to the cervix.If the head occupies the lower segment the presentation is cephalic,if is flexed on the spine vertex presents.
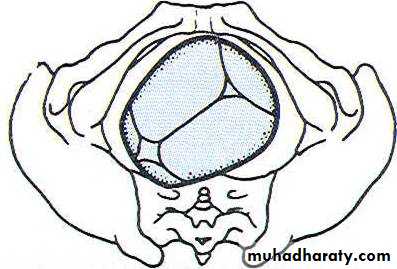
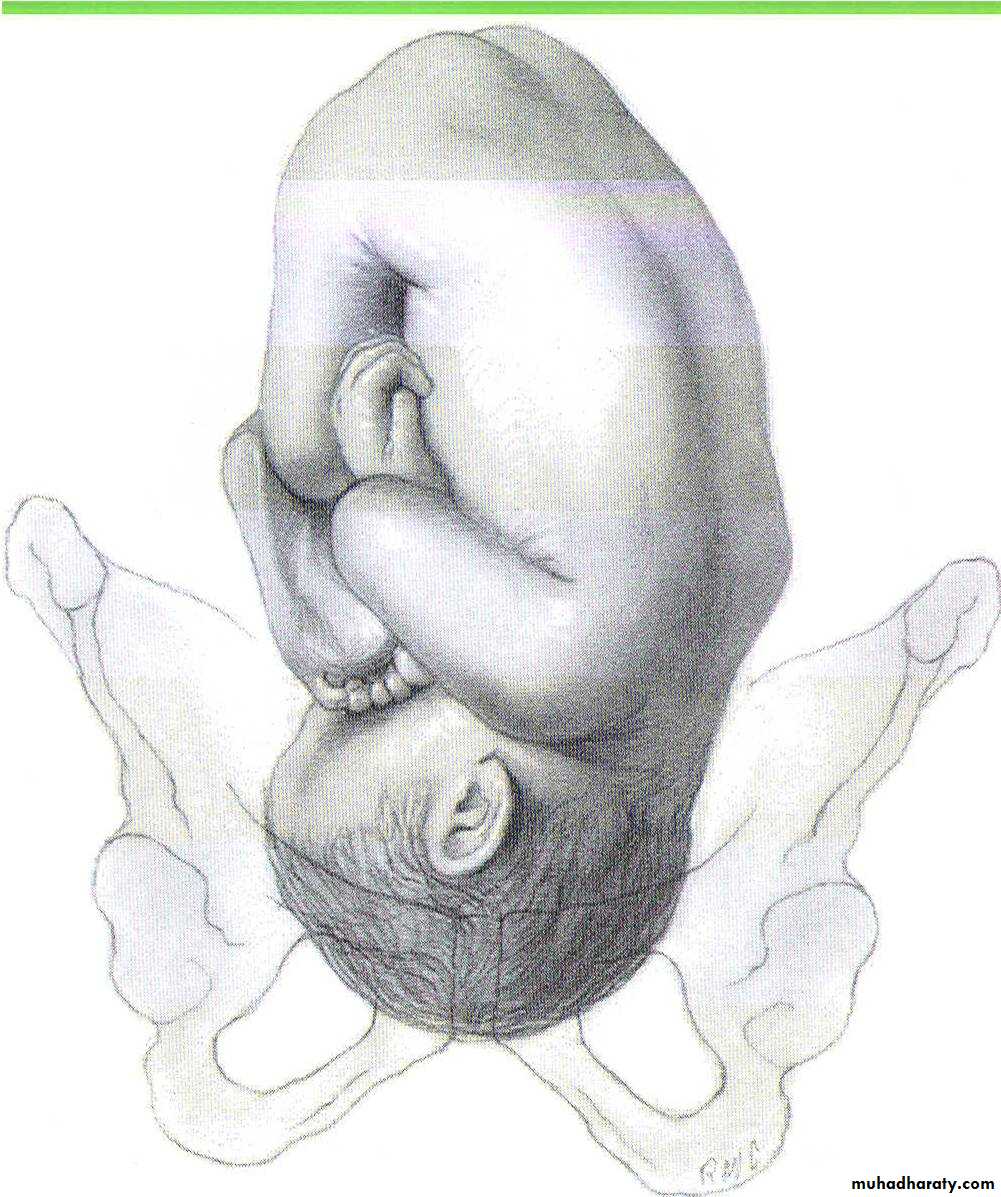
If the head is fully extended this causes face presentation,&if is partly extended cause brow prsentation.
If the breech occupies lower segment termed
breech presentation.If the fetus lies obliquely caused shoulder presentation.
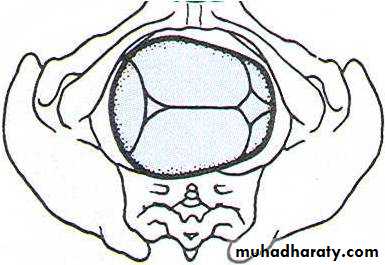
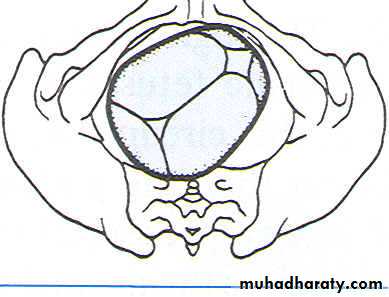
CEPHALIC PRESENTATION
Head is flexed sharply vertex / occiput presentation
Head is extended sharply face presentation
Partially flexed bregma presenting (sinciput presentation)
Partially extended brow presentation
Position
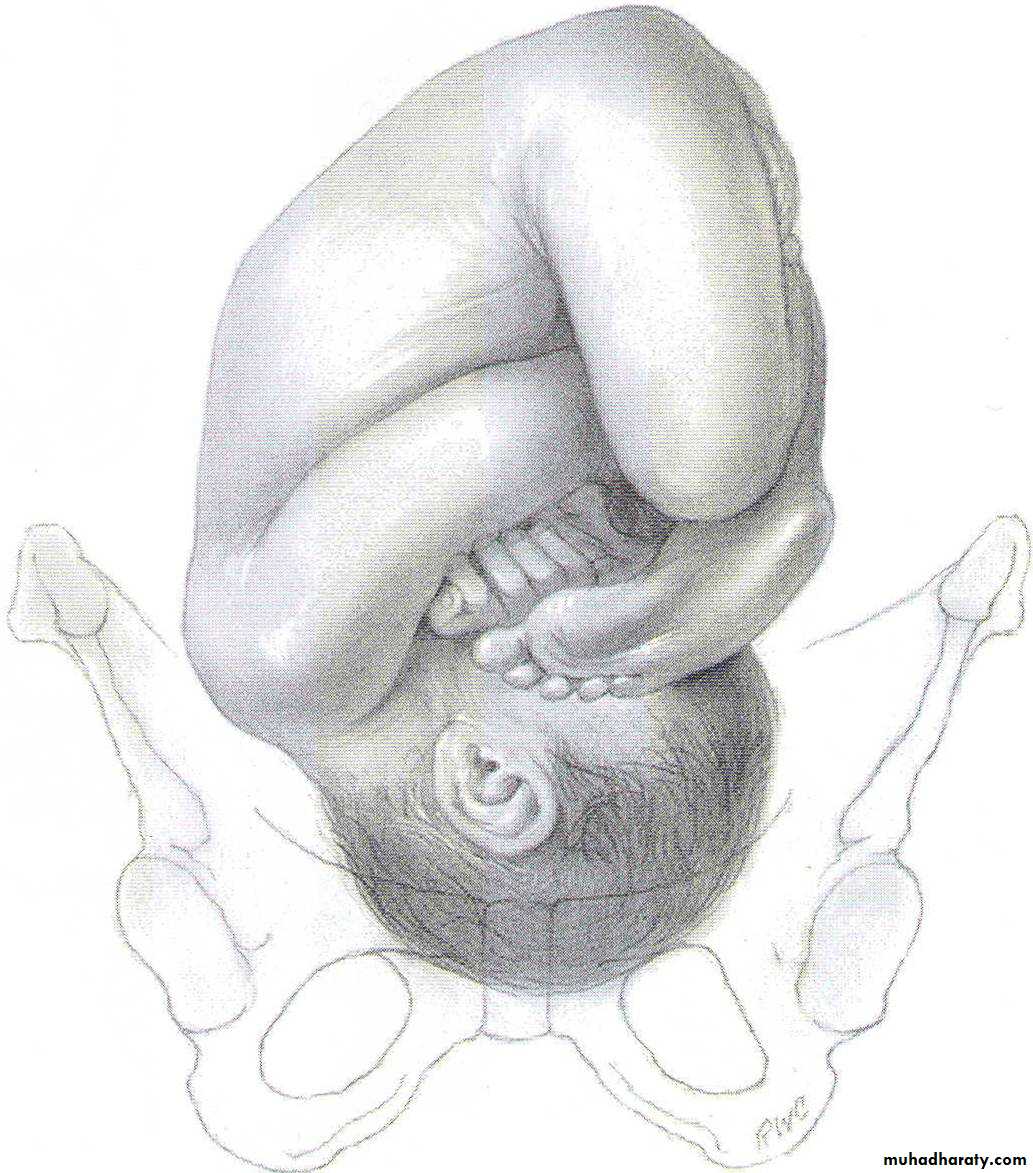
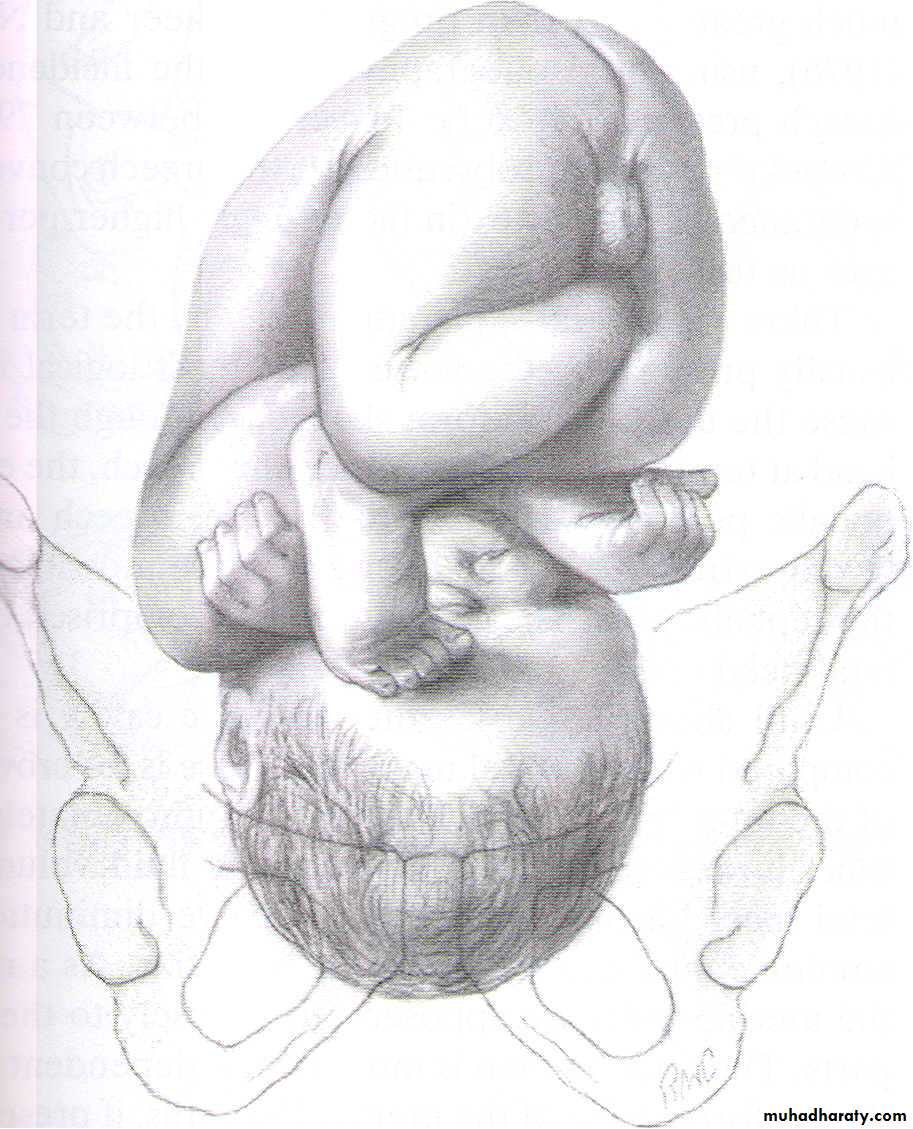
The relationship between selected part of the presenting part of the fetus[the denominator] to fixed points of maternal pelvis .With vertex presentation the denominator is the occiput,with face presentation it is the chin[mentum]&with breech presentation it is the sacrum.For each prsentation many positions are described .In vertex presentation;the occiput either anterior or posterior or left&right occipitoanterior (LOA&ROA) left&right occipitoposterior (LOP&ROP).



Attitude
Refers to the relation of different parts of the fetus to one another.Normally the head ‘back&limbsof fetus are flexed,in some abnormal presentation head or limbs may be extended.
• s
• A
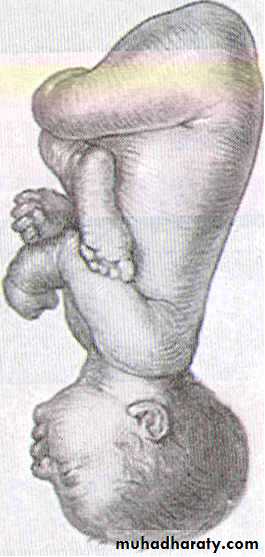
• Longitudinal lie. Vertex presentationA. Right occiput posterior (ROP)
Right occiput transverse (ROT)
• ~
• 'tJ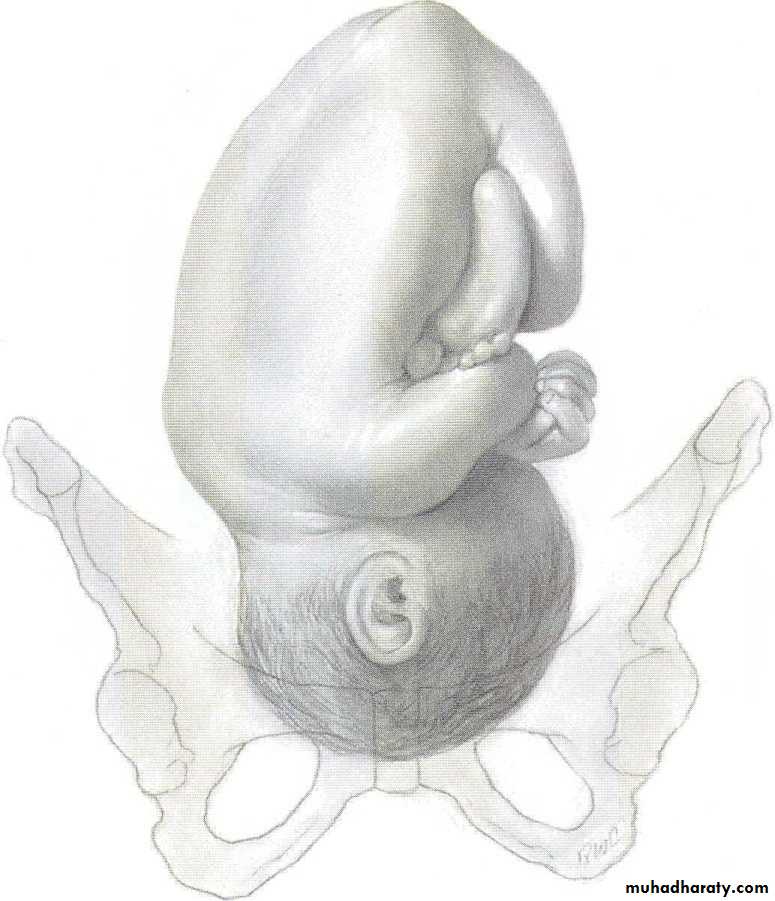
• a ill
• (1 bJ 3~• Sf a!
• w Cc
• ht p(
• fit tb fe
• w
• c
• al ta tb oj

Cardinal movements of labour
EngagementDescend
- Flexion
Internal rotation
- Extention
- Restitution
- External rotation
- Delivery of shoulder & fetal body
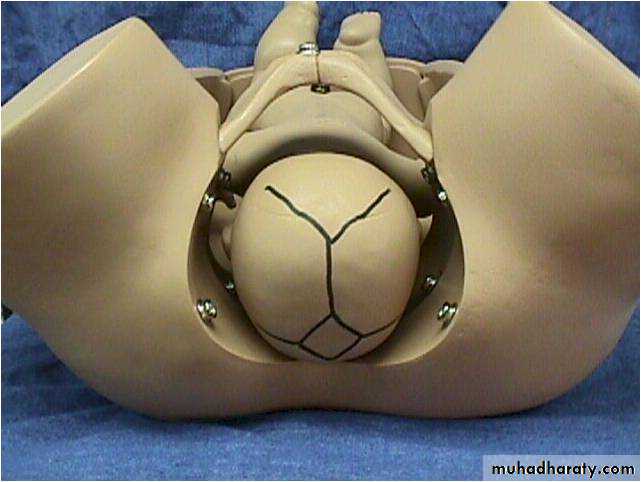
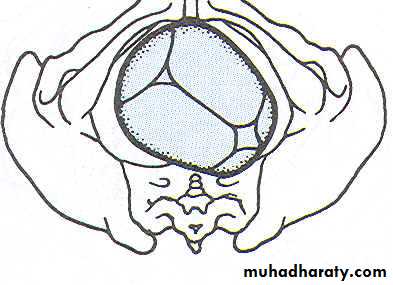
Engagement
The head normally enters the pelvis in the transverse position ,engagement is occurred when the widest part of the presenting part has passed through the inlet.It occur in vast majority of nulliparous women prior to labour,but not in multipara.If more than two-fifths of the fetal head is palpable abdominally then the head is not said to be engaged.
Descent
During the first stage &first phase of the second stage of labour descent of the fetus is secondary to uterine action .In the second phase of the second stage of labour descent of fetus is helped by voluntary use of abdominal musculature.
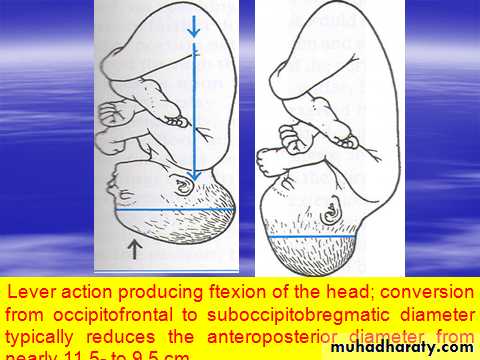
Flexion
The fetal head may not always be completely flexed when it enters the pelvis.As the head descends into the narrower midcavity,flexion should occur.This is probably as a passive movement in part due to the surrounding structures.
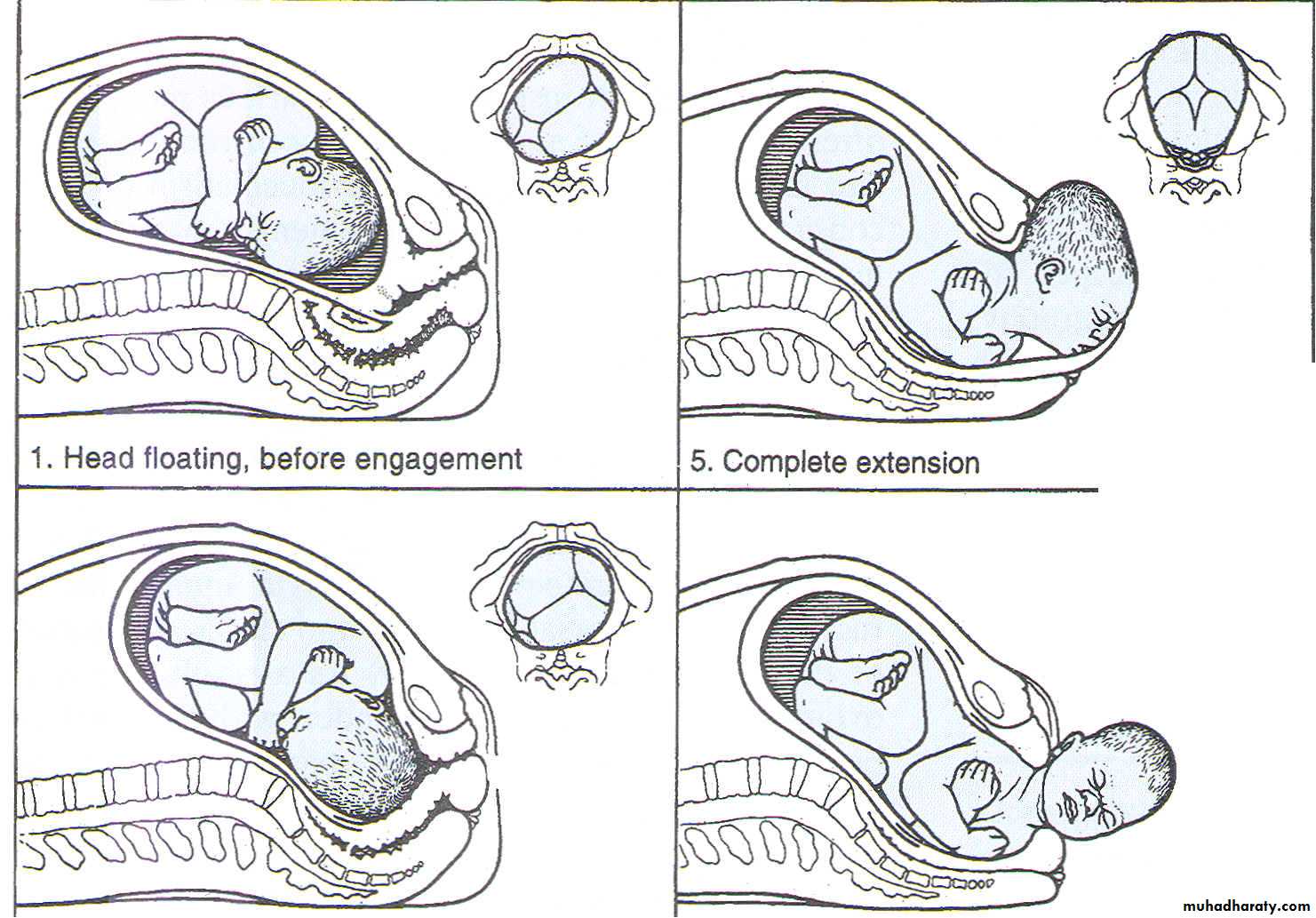
Internal rotation
This occurs because with a well- flexed head the occiput is leading &meets the sloping gutter of the levator ani muscles,which by their shape direct it anteriorly ;the occiput rotate forward from the LOA or LOT position to lie under subpubic arch,with the sagittal suture in the anteroposterior diameter of the pelvic outlet.Extension
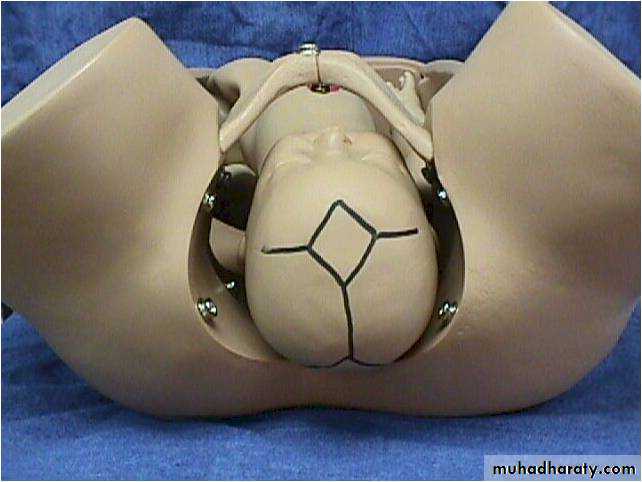
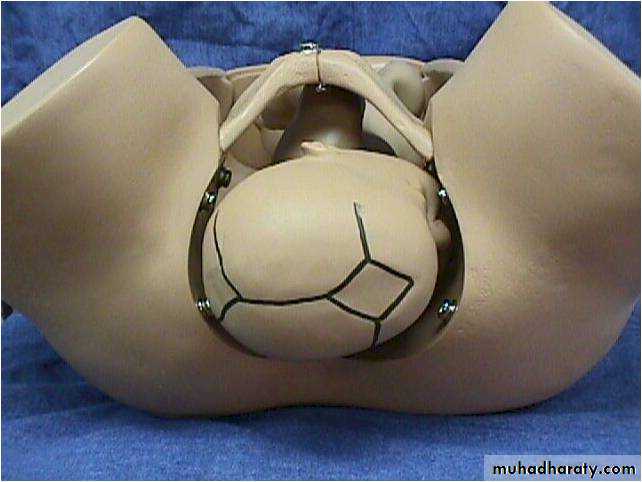
The well flexed head now extends with the occiput escaping from underneath the the symphysis pubis&starting to distend the vulva,this is known as crowning of head.The head extends further &the occiput underneath the symphysis pubisalmost acts as a fulcrum point as the bregma,face&chin appear in succession over the posterior vaginal opening &perineal body.
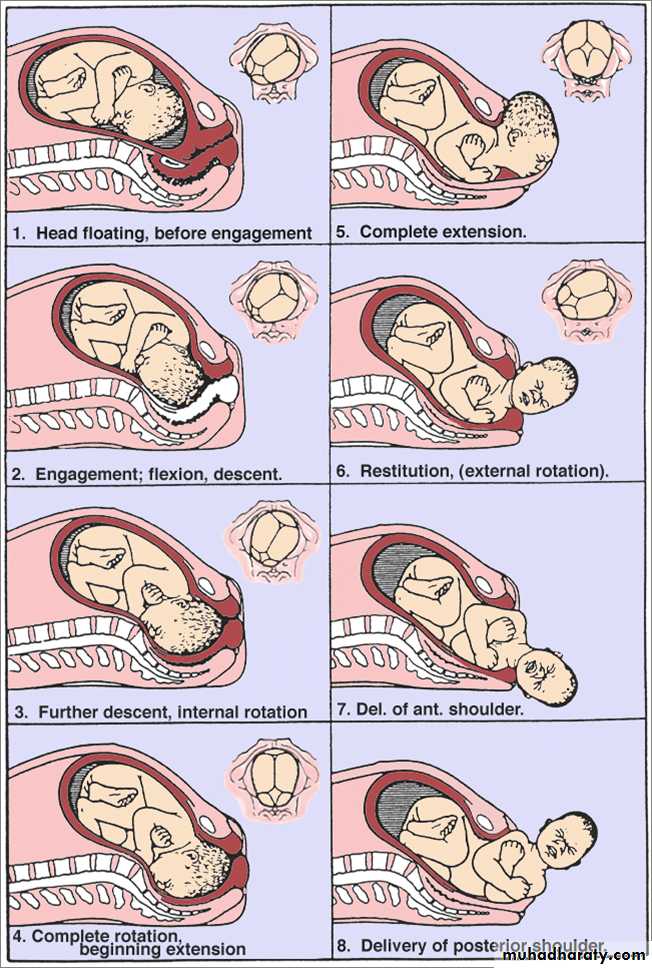
Restitution
When the head is delivering,the occiput is directly anterior .As soon as it escapes from the vulva,the head aligns itself with the shoulders,which have entered the pelvis in the oblique position.The slight rotetion of the occiput through one-eighth of a circle is called restitution.External rotation
In order to be delivered,the shoulders have to rotate into direct anterior-posterior plane.When this occurs,the occiput rotate through a further one-eighth of a circle to the transverse position.
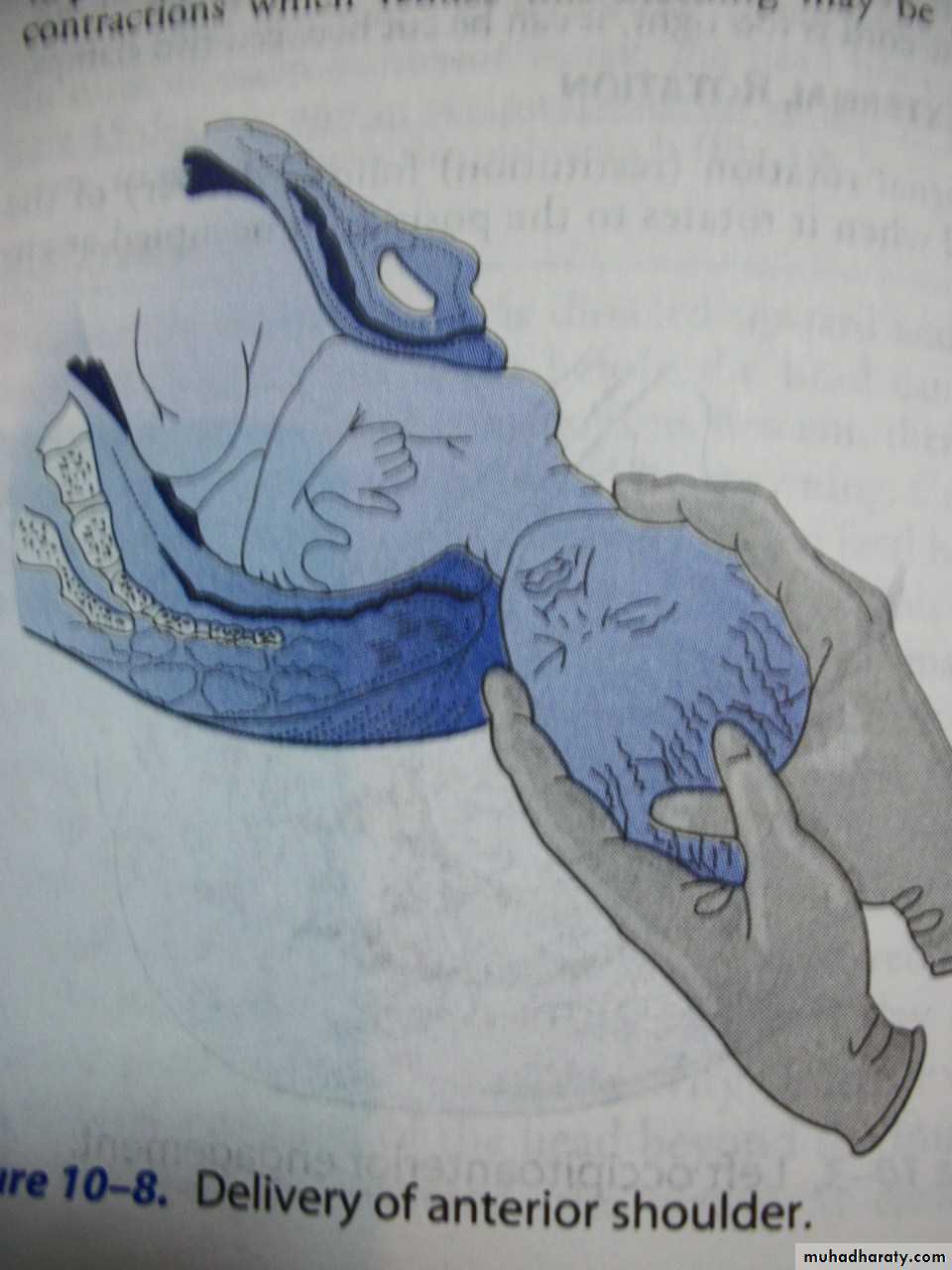
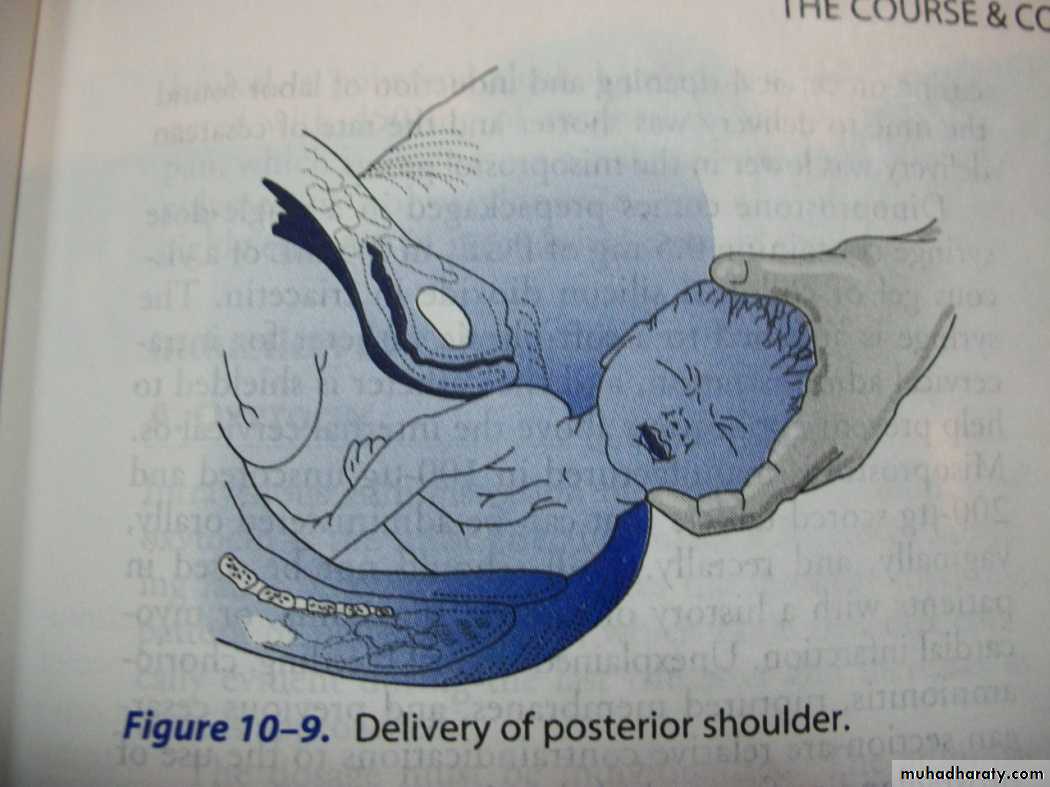
Delivary of the Shoulder&bod y
When restitution &external rotation have occurred ,the shoulders will be in the anterior-posterior position.The anterior shoulder is under the symphysis pubis &delivers first &the posterior shoulder delivers subsequently.The body then easily delivered .
• MANAGEMENT OF NORMAL LABOUR
• Important terms
• Gravida-number of pregnancies
• Para-number of pregnancies carried to viability &delivered
• Primigravida-pregnancy for the first time
• Multigravida-pregnant more than three
• Nulliparous-never carried pregnancy to viability
• Multiparous-had two or three delivaries that were carried to viability
• Management of first stage
The key principles are as follows:Provision of continuity of care &emotional support to the mother.
Observation of the progress of labour with timely intervention if it becomes abnormal.
Monitoring of fetal wellbeing.
Adequate &appropriate pain relief consistent with the woman’s wishes.
Adequate hydration to prevent ketosis.
On admission ,
complete history must be taken.the woman’s general condition is assessed
abdominal examination including obstetric examination ,then vaginal examination
her urine is tested for protein&sugar
Much of the apprehension from which many women suffer during labour, may be removed by adequate explanation beforehand.
She should have intermittent monitoring of her condition[pulse,BP,temperature]&the fetus by CTG(cardiotocography),this is as long as labour is progressing normally .
If labour is abnormal continuous CTG monitoring,antacid adminstration to the mother,epidural&urinary catheter insertion may be required.
In normal first stage the women is encouraged to mobilize if the head is engaged &eat alight diet.If the presenting part is not engaged she is kept in bed to diminish the risk of cord prolapse when the membranes rupture.Pelvic examination is performed every four hours&progress of labour is plotted on a partogram.
If epidural analgesia is not employed pethidine 100 mg i.m. may be given .
When the head is deep in pelvis there is may be urinary retention so soft catheter may be passed .
During the first stage of labour the membranes may be intact so they are ruptured artificially[ARM:-Artificial Rupture of Membrane] .
A graphical representation of progress of labour.
This record allows visual assessment of mother pulse rate&blood pressure,srength &frequency of uterine contraction.Cervical dilatation in centimeters against the time in hours plotted against expected normal so compaired to an average curve for normal primegravidae or multigravidae as may be appropriate in any given population.
partogram
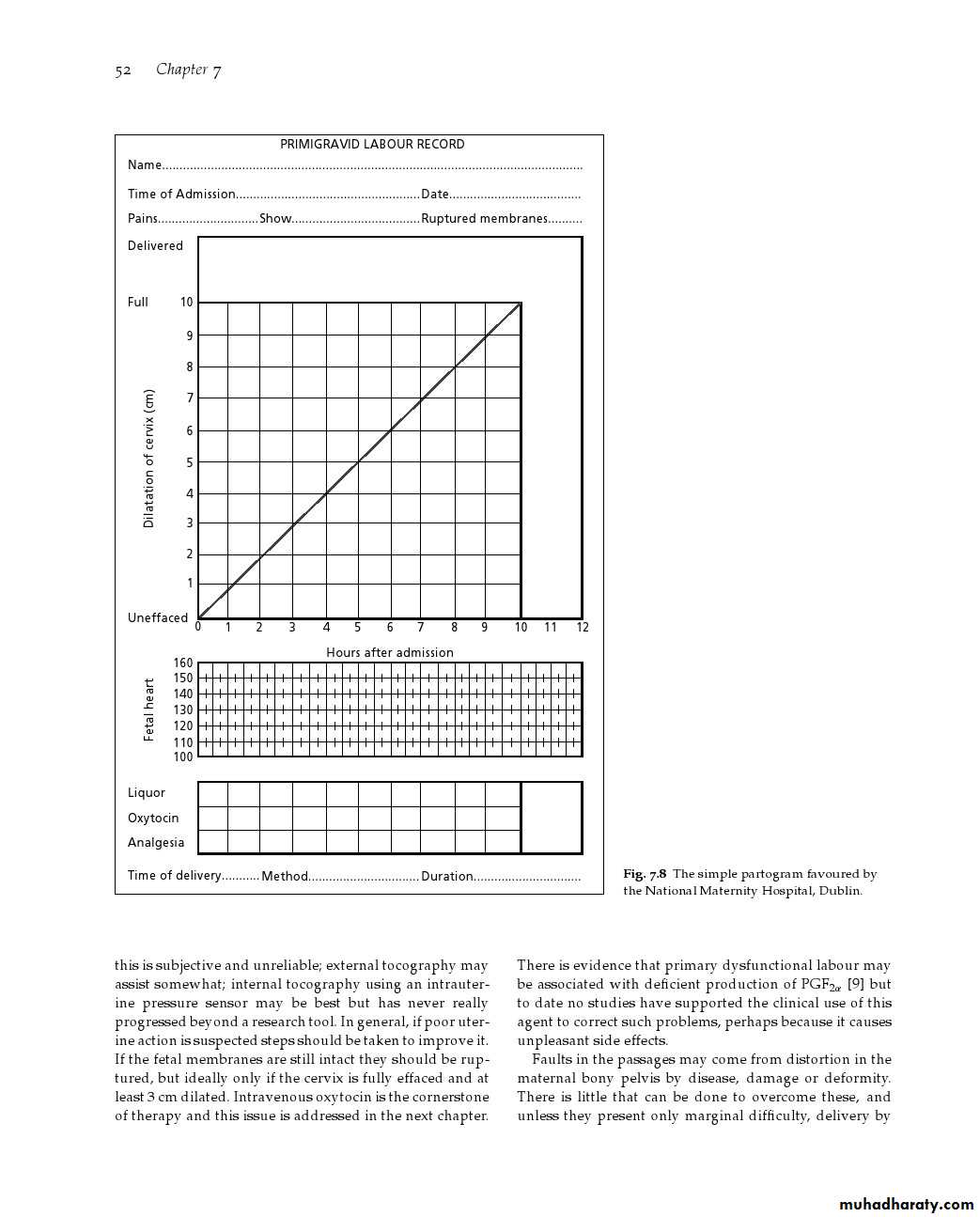
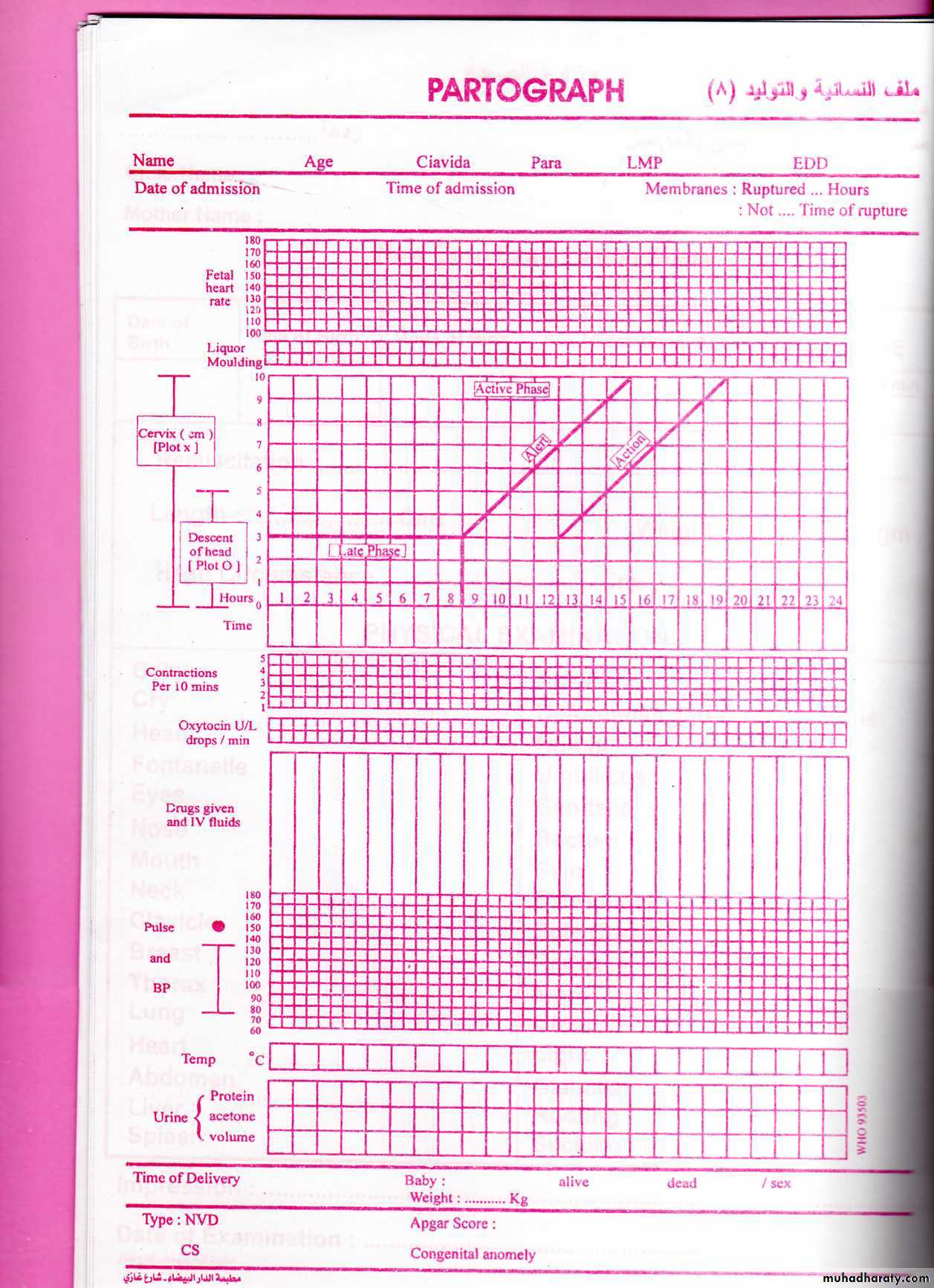
If labour is not progressing normally dilatation of the cervix become slower Or may cease &her curve will be to the right of the normal curve.So if there is delay the membranes are ruptured artificially&uterine action augmented by oxytocin infusion .
So frquency of uterine contractions ,dilatation of the cervix,descend of fetal head
The state of the fetus fetal heart,amount&colour of amniotic fluid draining also recorded in special area of the partogram.
Any drugs or fluid given to the mother also recorded as part of intervention in the first stage of labour.
• Management of second stage
If labour has been normal the first sign of the second stage is an urge to push by the mother .Full dilatation of the cervix should be confirmed ,the woman will get an expulsive reflex with each contraction &will generally take a deep breath ,hold it,&strain down.If the woman is well propped up in lithotomy position with her head upright &her hands behind her knees she will be in a comfortable position to push effectively .• The process of the descent of the head can be judged by watching perineum
• the head has crowned, the woman should be discouraged from bearing down by telling her to take rapid shallow breaths.• The head is dlivered carefully by pressure through the perineum onto the forehead by means of a finger &thumb placed on each side of the anus pushing the head forward slowly before it is allowed to extend& complete its delivery &controlling the rate of escape with the other hand.
• Episiotomy An incision in perineum indicated in some cases to prevent lacerations
• 2nd stage
• Once the head is born, cheking the neck [if there is loops of umbilical cord are found]to slip the cord over the head;nasopharyngeal suction is performed• .With the next contraction there is external rotation of the head &delivery of shoulders ,to aid it the head is pulled gently downwards&forwards until the anterior shoulder appears beneath the pubis.
• The head is then lifted gradually until the posterior shoulder appears over perineum &baby is swept upwards to deliver body&legs.
•

• Management of third stage
• Separation of placenta occurs because of reduction of volume of uterus due to uterine contraction& retraction so it lies free in the lower segment of uterine cavity. The mother will become aware of its presence on the pelvic floor &by straining expel it from vagina.
• Signs of separation of placenta are:
Lengtheing of the cord protruding from the vulva.A small gush of blood from the placental bed which is normally stops quickly due to retraction of myometrial fibers.
A rising of uterine fundus to above the umbilicus ,the fundus becomes hard&globular compaired to the broad ,softer fundus prior to separation.
The placenta can be felt with a finger inserted into vagina.
• The modern management is the active management of third stage which involve a procedure called controlled cord traction [Brandt-Andrews’ method].
• This technique as follows:
• 1-Synthetic oxytocin 10 iu or syntometrin [5iu oxytocin,0.5 mg ergometrine] is given by intramuscular injection following delivery of anterior shoulder .• 2-After delivery ,the attendant should place the left hand on the uterus to identify when a contraction has occurred .During this time the vulva should be obseved for any bleeding.
The cord should be double clamped approximately 1-2minute after delivary
• 3-When a contraction is felt the left hand should be moved suprapubically &the fundus is elevated with the palm facing towards the mother.At the same time the right hand should grasp the cord &exert steady tractionso that the placenta separates &delivered gently ,care being taken to peel off all membranes ususlly with a twisting motion.
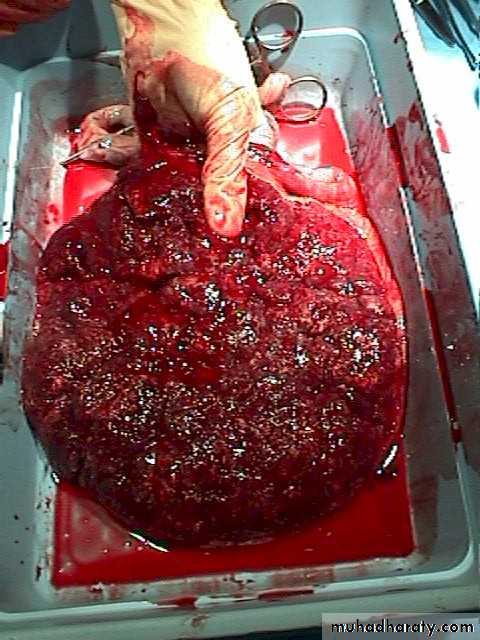
After completion of third stage the placenta should be inspected for missing cotyledons or a succenturiate lobe.If these are suspected then manual removal is arranged.
Finally the vulva is inspected for tears&lacerations.Minor tears do not require suturing,but tears extending into perineal muscles will require careful repair.
•
•