Interpretation of IVU finding
Dr Mohammed baderFIBMS,DMRD ,MBChB
1. loss of renal outline on the plain film
it is not necessarily associated with non visualized kidny after IVU1. technical (poor radiography or overlaying by faces or masses
2 absence kidney 1:1000 of live birth ,increase incidence of external abnormalities (VSD,meningocele ,skeletal and anal abnormalities ,) the normal kidney may reach a twice of normal size
3.displaced (ectopic kidney ,presacral ,crossed ectopia ,intrathorasic )
4perinephrichaematoma
5.perinephric abscess
6.tumour
7.post neprectomy
calcification
destrophic due to diseases1.1 infection11. a. TB nodular or curvilinear amorphous
1.1.b hydatid (curvilenear )m
1.1 .c. abcess
1.2 carcineoma
1.3 aneurysm
2.nephrocalcinosis
paranchymal calcification associated with diffuse renal lesion or metabolic abnormality may be madularry or cortical , the medullary causes are (hyperthroisim , renal tubular acidosis , and medullary spong kidney (variable portion of a kidney contain neumerous small medullary cysts contain small calculie gaivi9ng a (bunch of grapes ) appearance of big kidney with multiple cysts
cortical nephrocalcinosis
1.acute cortical necrosis
2.chroncglomerulonephritis
3.chronictransplant rejection


renal calculie
opaque stones calcium phospahte or oxalate ,calcium oxalate are more adiopaque than phospate orctriple stonesnon opaque (uricacid ,xantyhin , and matrix (mucoprotien )
poorly opaque cystine (in cystinurea )
non visualized kidney in excretion urography
1.absent , postnephrectomy
2.ectopic
3.chronicobstructive uropathy
5.tumours
6.renal artery occlusion
7.renal vein occlusion
8.multicystickidneys


small kidney
unilateral small kidneyin all these cases chronic unilateral disease is associated with compensatory hypertrophy of contralateral kidney
1. due to post obstruction atrophy(with dilated collecting system)
2. Ischemia due to renal artery stenosis
3. radiation nephritis (2300 rad )
4. end result renal infarction (renal artery vein thrombosis or renal artery embolism )
5. in congenital hypoplasia
bilateral small kidney
generalized arteriosclorosis
Chronic glumerlunephritis
Chronic papillary necrosis
arterial hypotension
bilateral causes of unilateral kidney
large kidney
1.compensatory hypertrophy2.obstructed kidney
3.pyonephrosis
4.duplexkidney '
5.tumour
6.crossed fused ectopia
7.multicystic k
8.acutepyelonephritis
9. truma
10 renal v thrombosis
11.acutearterial infarction
12.adult polycysticdisease
nephrogram
Persistent nephrogram1.acute tubular necrosis
2.renal failure
3.acute obstruction
4.acute hypoetension
5.acute pyelonephritis
rim nephrogram
1. sever hydronephrosis
2.arteril injury
Striated nephrogram
1.acute u obstruction'
2polycystickid
3.acute pyelonephritis
localized bulge ofrenal outline
renal cysttumors
dromerdy hum
promenant septum of bertin
hilar lip hyperplasia '
duplex kidney
dilatation of single calyx

radiolucent defect in the renal pelvis
1.extrensic with smaooth margins1.cyst
2.vascualar impresion
3.renal sinus lipomatosis
2.in the lumen
1.blood clot
2.lucent calculus
3.slughed papila
4.air
3.from the lumen
tumourspolyuretritis cystica
sequamous metaplasia
dilated ureter
obstruction within the lumen
1.calculus
2.blood clot
3.slughed papilla
within the wall
1.tumours
2.TB
3.schistosomiais
4.post surgical trauma'
5.uretrocele
6.megaureter
outside the wall
retroperitoneal fibrosis
ca
retocaval ureter
non obstructive like (VUR)
filingdefect in the bladder wall or lumen
1.prostate2.neoplasim
3.blood clot
4.instrument
5.calculus
6.uretrocele
7.schistosomiasis
8.endometriosis

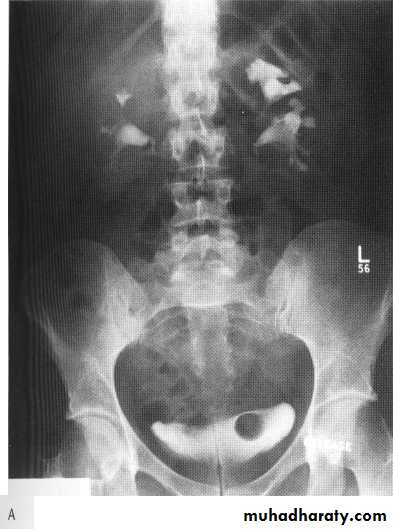
Obstructive uropathy
Causes 1.intralumenal .congenital like PUJ obstruction ,megaureter, Ureterocele (ectopic and orthotopic)Acquired : stones
Tumors (urothelial tumors )
Blood clots or sloughed papilla
2. extralumenal :abdomial or pelvic tumours
Stricture
Retroperitoneal fibrosis
Bladder outlet obstruction or bladder masses
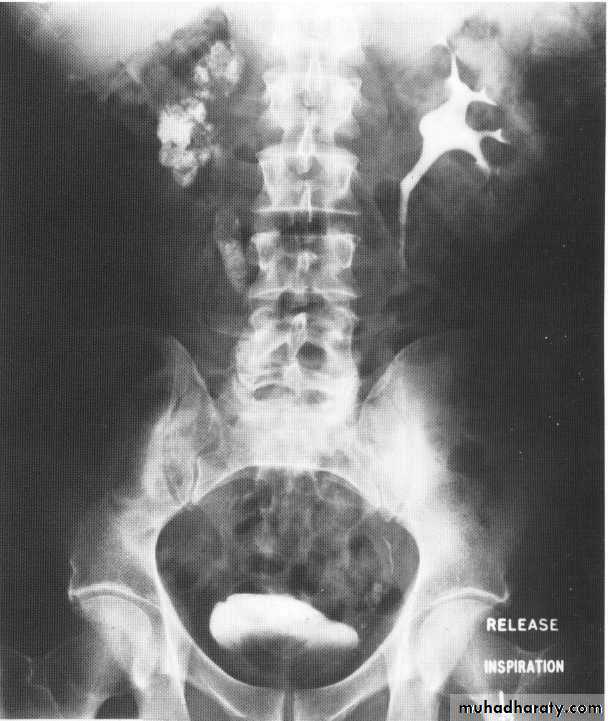
Ivu FINDING OF ACUTE OBSTRUCTION
Increasingly dense ‘obstructive’ nephrogramModest kidney enlargement (50% of patients)
Delayed caliceal opacification
PCS and uretric dilation (g.1 mild PCS dilation ,g.2 moderate PCS dilation (blunting calyces),g.3 sever dilatation within thinning of parenchyma .
Spontaneous pyelosinus extravasations (up to 24% of patients
Large kidney(partial obstruction)
Small kidney (complete obstruction)
Nephrogram density:
Normal or decreased (may increase with acute-on-chronic obstruction)
Parenchymal thickness:
Reduced
‘Crescents’, ‘soap-bubbles’, ‘rims’, or ‘shells’
Pyelogram:
Hydronephrosis
‘Negative pyelogram’ on nephrogram phase
Ureter:
Dilatation and tortuosity (low obstructions)
Mucosal striations



VUR
Vesicoureteric reflux results from congenital or acquired incompetence of the valve-like ureterovesical junction mechanismgrades
I-Reflux into the ureter alone; or part of ureter
• II-Reflux into the ureter and pelvis;
• III-Reflux into ureter and pelvis with mild dilatation;
• IV-Reflux into ureter and pelvis with moderate dilatation and
preservation of the papillae;
• V-Reflux into ureter and pelvis with obliteration of the
papillae;
Reflux nephropathy is usually assymetrical or unilateral.
Theclassical IVU appearances are of cortical scarring over clubbedcalyces. This is most frequently seen at the renal poles, especiallythe upper pole .
Dilated PCS and ureter without obstruction
reflux and is always more obvious on voiding cystourethrography


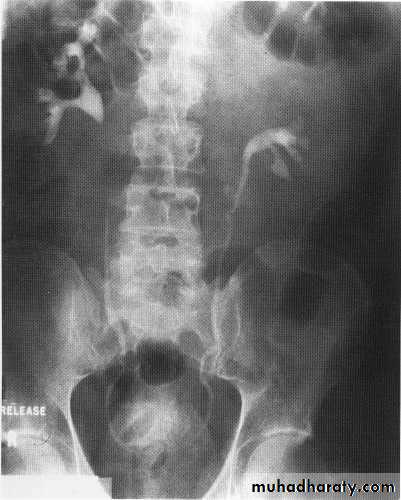
Congenital anomalies of the kidney
Duplex kidneyThese are common, being found in
1 0% of the population. The most minor form of this condition is a bifid renal pelvis, which is a normal variant. Otherwise duplication abnormalities (duplex kidneys) are characterized by two (on rare occasions more than two, up to six having been reported) ureters and renal pelvis
The duplication of the ureter may be incomplete (the ureters fusing at some point in their course and
having a common distal ureter and orifice) or complete (both ureters having separate distal orifices)
They may be associated with pelviureteric junction obstruction. The lower renal moiety drains via the ureter withthe orthotopic insertion (i.e. inserts on the trigone in the anatomically correct site) but is often associated with vesicoureteric reflux.
The ureter draining the upper moiety is inserted ectopically and it stermination is always distal to the lower moiety insertion
There is often stenosisof the ureteric orifice with a variable degree of obstruction


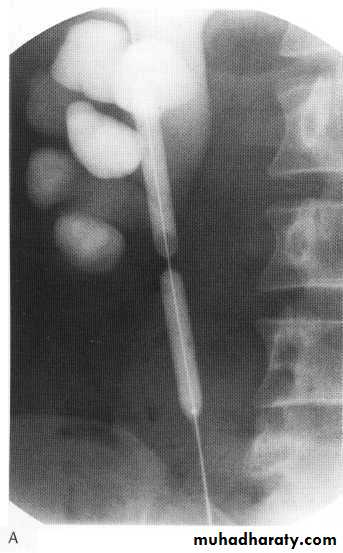
ureteroceles
These are submucosal dilatations of the intramuraldistal ureter. They often project into the bladder lumen
There is a female preponderance of approximately 4 to 1.
On IVU the ureterocele can be seen as a contrast-filled structure with a thin smooth radiolucent wall surrounded by contrast containing urine in the bladder. This has been described as a cobra's head appearance
Polycystic kidneys
I n autosomal recessive polycystic disease of the kidneys (ARPCK) the renal parenchyma is replaced by numerous tiny (1-8 mm) cystsOn IVU there is a striated nephrogram thought to be due to contrast lying in the minority of preserved functioning tubules next to dilated non-opacified diseased tubules.
Polycytic disease
In autosomal dominant polycystic disease of the kidneys(ADPCK) numerous cysts of varying size, often becomingextremely large, develop within the kidneys, gradually replacingnormal renal parenchyma and ultimately producing renal failure. It usually presents between 20 and 39 years of age
Ectopic kidney
failure of kidney to acsent to L2 levelPelvic kidney
Crossed fused ectopia
Intrathorasic kidney
horse shoe kid
This is a common renal anomaly affecting
1/400 live births, with a 2 to I male predilection. In utero contact between the metanephric tissue of the developing kidneys results in a midline connection (isthmus) between the lower poles



Pelviureteric junction obstruction
This condition has a spectrumof severity from severe antenatal hydronephrosis with global cortical loss to radiologically demonstrable hydronephrosis in theadult without apparent symptoms or loss of renal functionUp to 20%are associated with an accessory renal artery running across thePUJ, which may be visible on the IVU as a smooth indentation.
During the acute episode there are features on IVU of severe acute obstruction, which include a delayed, increasingly dense nephrogram and delayed appearance (sometimes up to 24 h or more) of contrast within the collecting system. When opacification occurs it demonstrates clubbed calyces and a dilated pelvis
