Neonatal care

Neonatal care 18
The transition from intrauterineto extrauterine lifeThe vast majority of babies achieve a remarkably smooth transition from intrauterine to extrauterine life, making their first respiratory efforts within 10 seconds of birth. Fetal lungs are filled with ‘lung liquid’, a fl uid that is important for normal lung development and growth. During labour, the production of lung liquid ceases and reabsorption begins. Lung liquid is squeezed out of the thorax during vaginal delivery.
The last vestiges of lung liquid are then absorbed by the lymphatics and the pulmonary capillaries.
At the same time as the lungs are fi lled with air, the blood supply to them increases dramatically. Pulmonary blood flow islow in fetal life because a high resistance is actively maintained in the pulmonary capillaries. Immediately after birth, the pulmonary vascular resistance starts to fall.
prostaglandins and
nitric oxide, and by the presence of
oxygenated blood in the pulmonary capillaries themselves.
The transition from intrauterineto extrauterine life
NeonateAn infant from the time of birth to
one month of age
Newborn
A baby in the first few hours of its life,
also known as newly born infant
Important terms
How to manage the newborn1 assessment
2 resuscitation
3 examination
4 feeding
Assessment and simple resuscitation at birth
Most infants born at term and without specific indicators of high risk during pregnancy do not need resuscitation.Using the APGAR scores can be helpful. whichare conventionally determined at 1 and 5 min and describe cardiorespiratory and neurological depression..
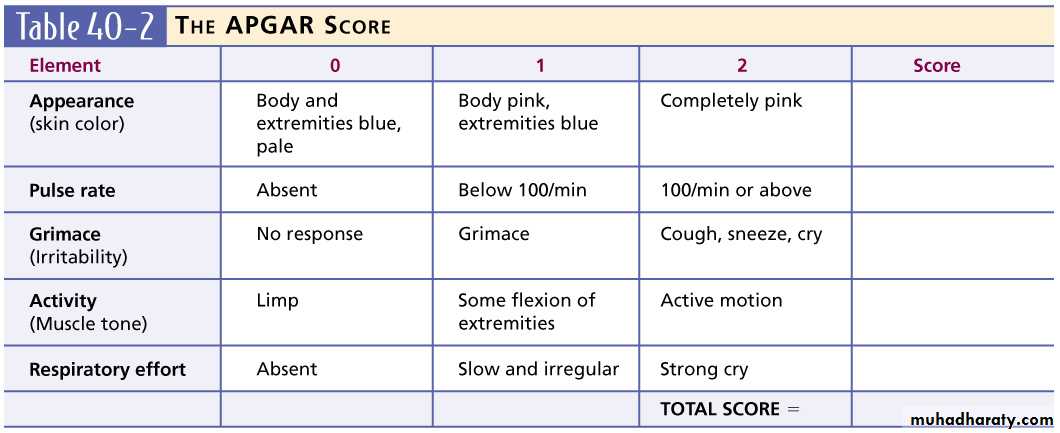
Neonatal assessment
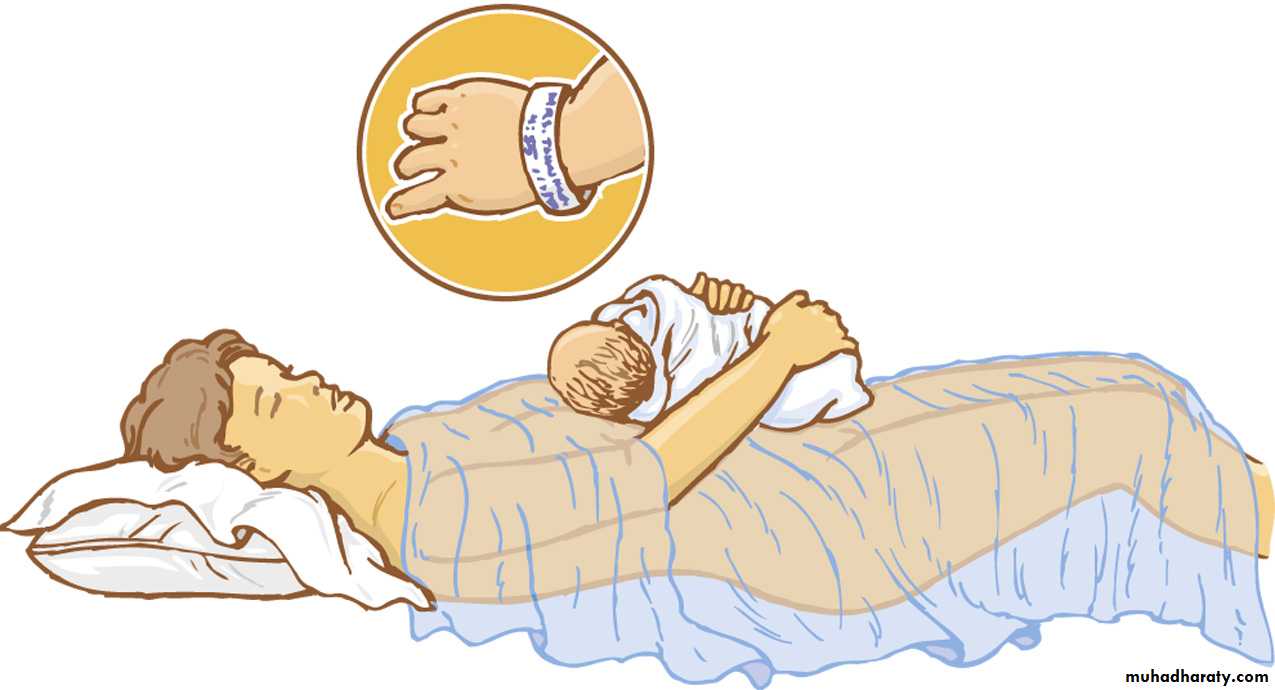
By this step the baby fall in 3 categories:-1-pink, breathing,more than 100 bpm,good tone &movement :-dry wrap with warm towel leave the baby with his mother no need for suction to avoid vagal bradycardia &cooling
2-
not breathing regularly heart rate more than 100 bpm ,centrally cyanosed :- dry ,rubbing can stimulate the the breathing if no response, mask breathing 5 inflations if baby still inactive,chest compression then intubation may be needed
3-
not breathing or heart rate less than 100bpm or pale& cmpletely floppy,:- dry him quickly put in warm dry resuscitation surface ,face mask ventilation; if heart rate remain less than 60bpm ,chest compression applied if no rapid response, intubation should done;if all measures fail, mediction started.
Inverted Pyramid for Resuscitation
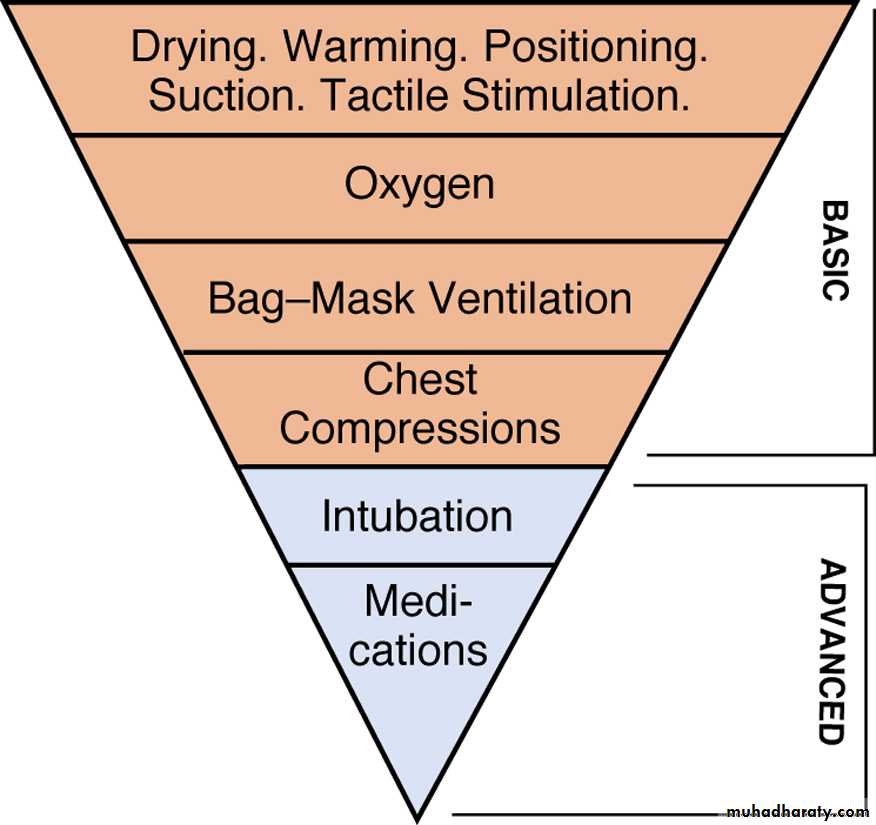
Dry the infant to prevent
loss of evaporative heat.
Healthy newborns should be allowed to begin the bonding process with the mother as soon as possible.
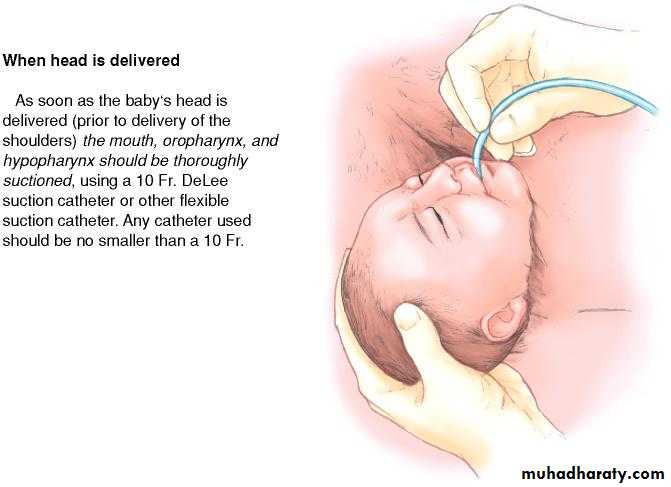
Position of newborn when first
suctioning upon delivery.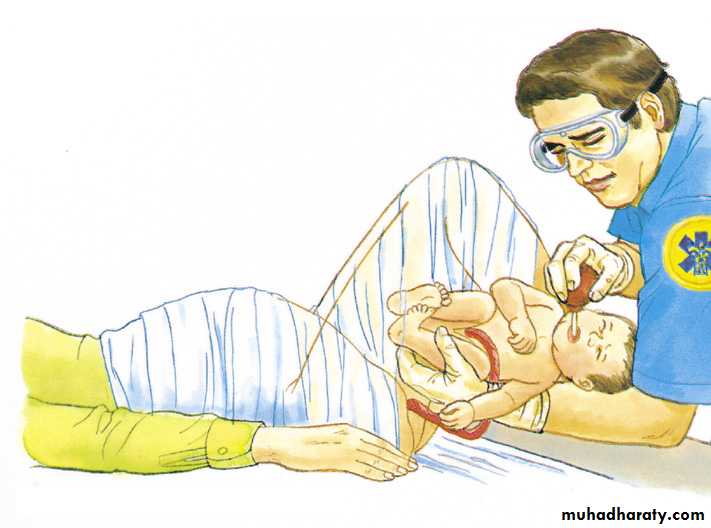
Suction the baby’s mouth first, then the nose, to avoid risk of aspiration.
Suctioning of the mouthusing flexible suction catheter.
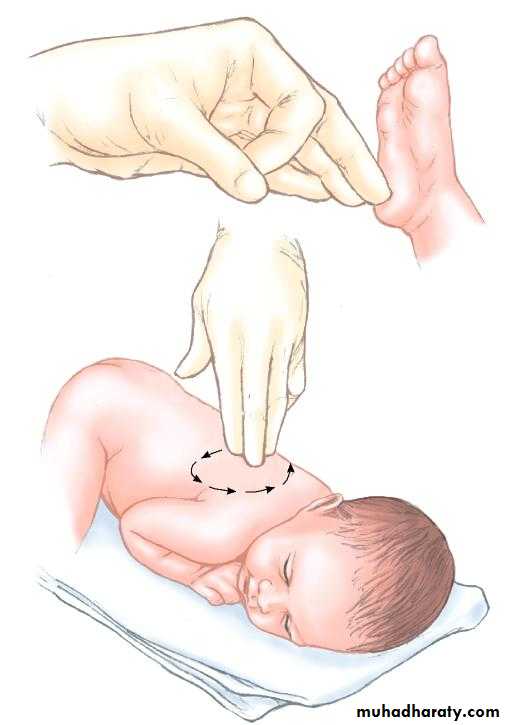
Stimulate the newborn as required
by flicking its feet or rubbingits back—DO NOT
vigorously rub a newborn baby!
Mask uses
After the airway has been adequately cleared by suction, the mask is positioned over the nose and mouth and the bag squeezed (or gas provided) to deliversever al long inspiratory breaths followed by regular ventilation at a rate of 30–40 breaths/min. In many cases ventilating with air is as effective as using oxygen. This technique requires practice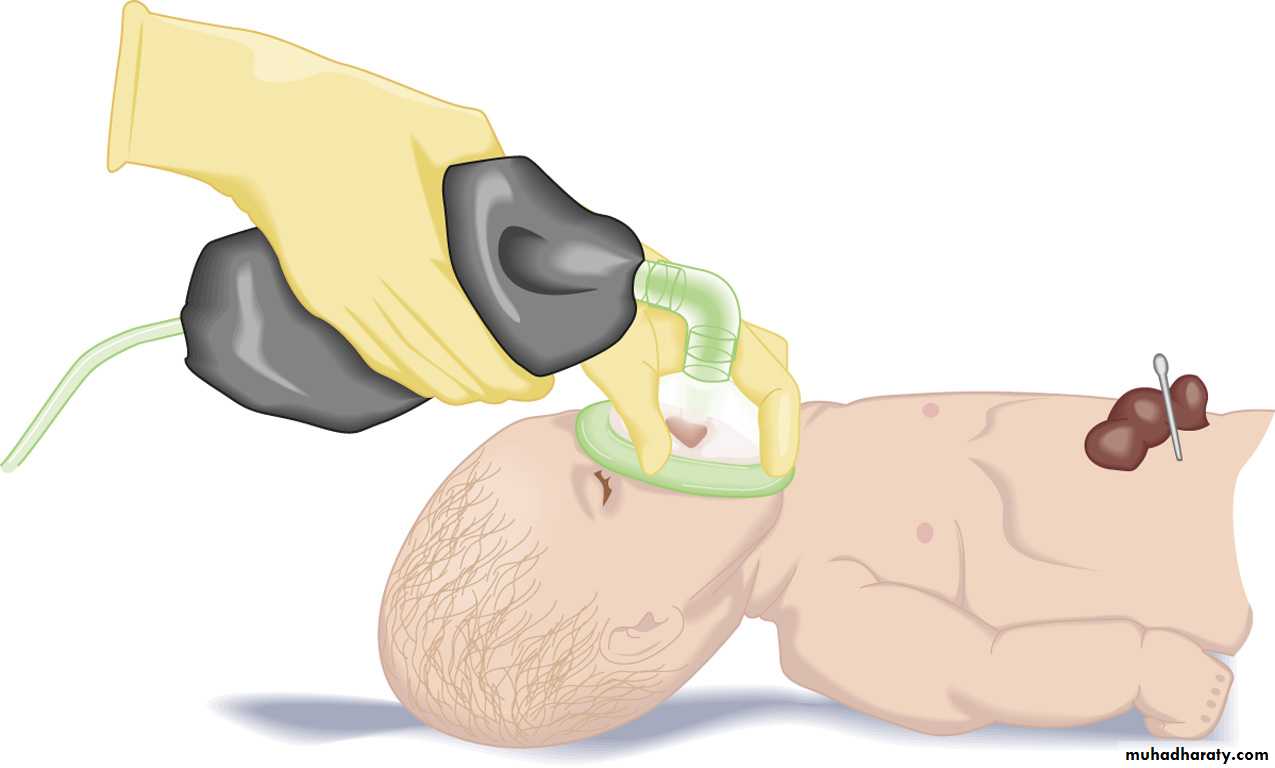
Use of a bag-valve mask
Advanced life supportIf mask ventilation fails to produce an adequate heart rate check again for evidence of upper air way obstruction and aspirate the nasal passages and nasopharynx. Meconium present in the trachea should have been aspirated under direct vision using a laryngoscope before ventilation, but this may need repeating.
If clearing of the airway and reventilation fails to produce a normal heart rate, endotracheal intubation is required.
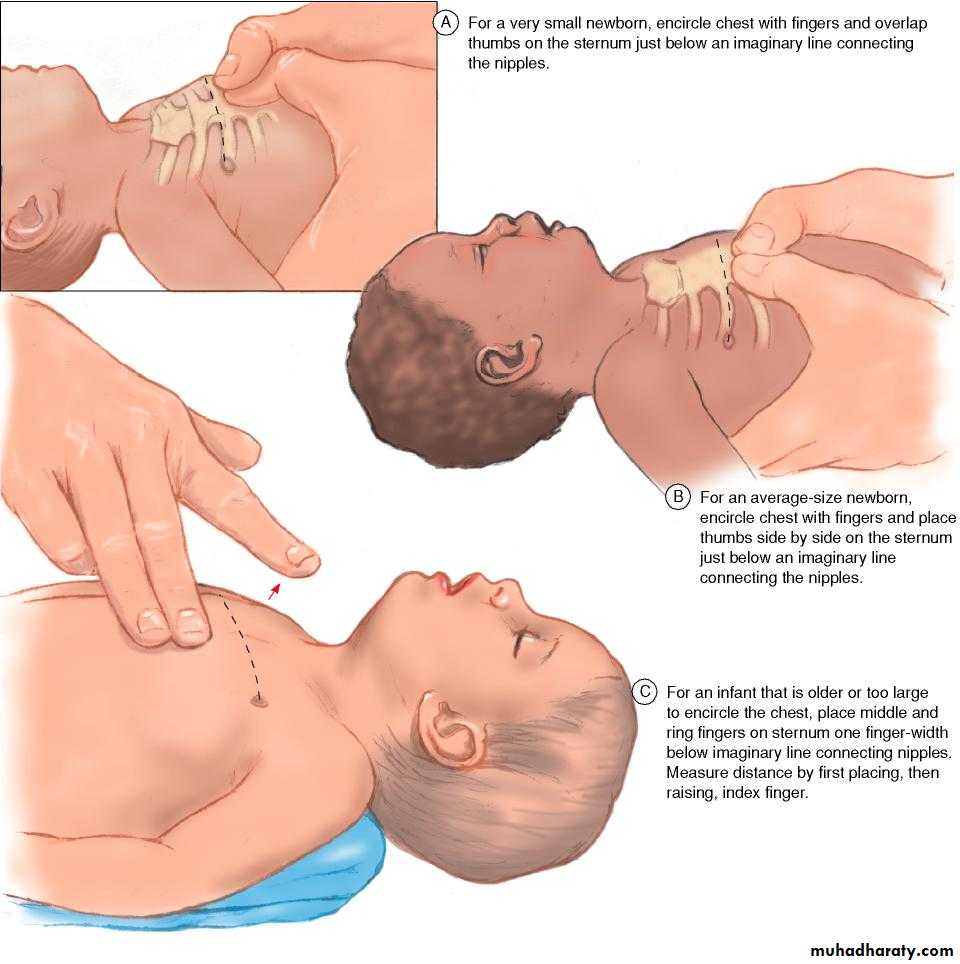
Finger positions for infant sizes
• Endotracheal intubation of a newborn should be carried out in the following situations:• Tracheal suctioning is required.
• Prolonged ventilation will be required.
• A diaphragmatic hernia is suspected.
Positioning the newborn
to open the airway.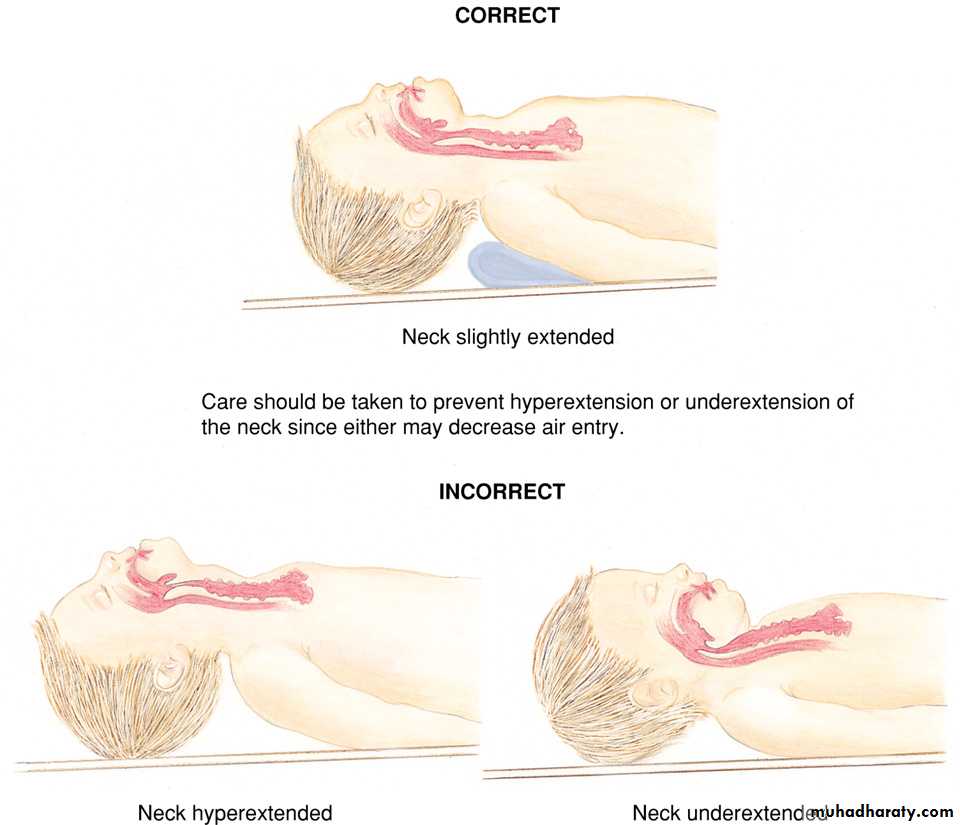
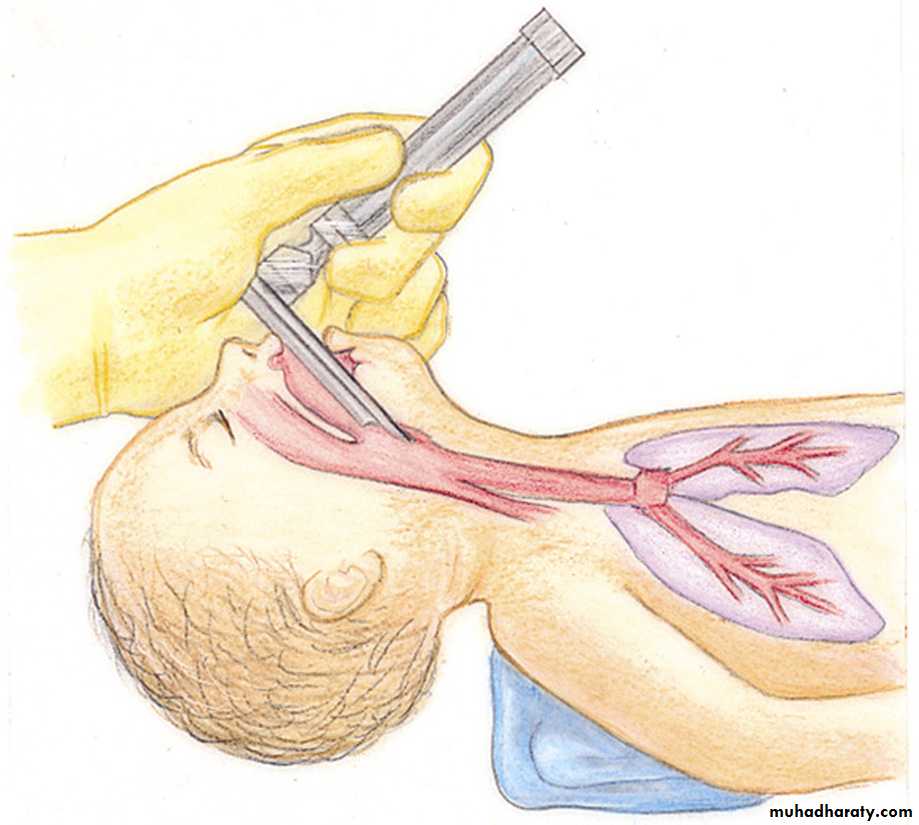
Insert the larynogscope.
Suction any meconium present.
An infant born in the presence of thin meconium may not require treatment, but those born through thick meconium should be intubated immediately.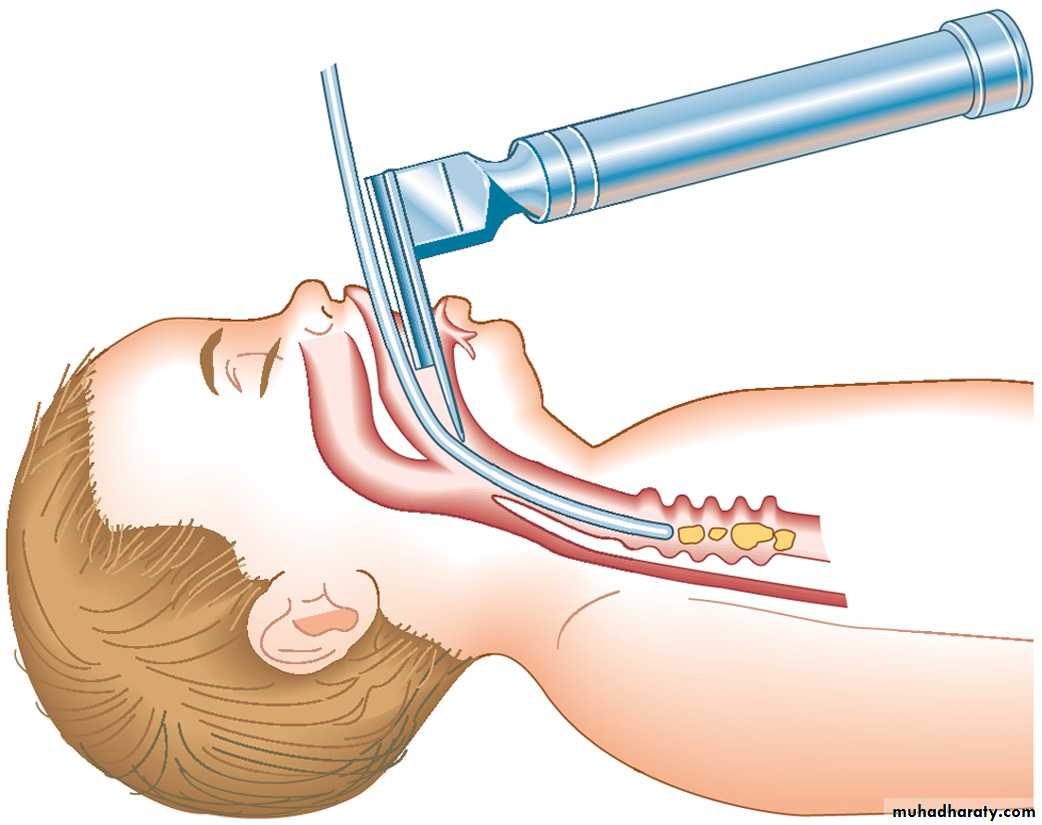
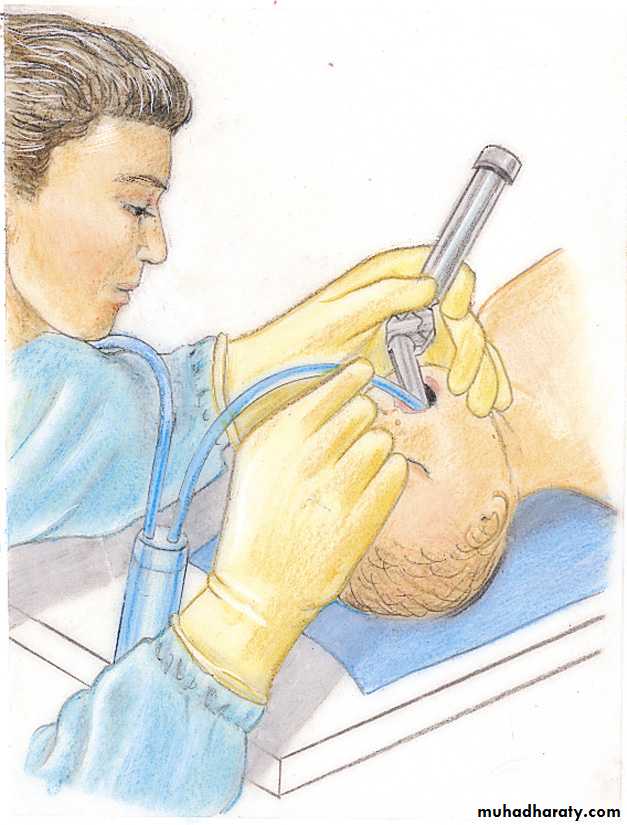
Intubating the infant
Oxygen• If central cyanosis is present, administer supplemental oxygen.
• If possible, oxygen should be warmed and humidified.
Ventilation
• Begin positive-pressure ventilation if any of the following is present:
•
• Heart rate less than 100 beats per minute
• Apnea
• Persistent central cyanosis

Medications & Fluids
On occasion, medications may be necessary and should beavailable:
1. Epinephrine 1:10 000; 0.1–0.3 ml/kg intravenous (IV) or
via endotracheal tube (ET) given rapidly.
2. Volume expanders (whole blood, normal saline, 5%
albumin-saline, Ringer’s lactate); 10 ml/kg IV over 5 minutes.
3. Sodium bicarbonate 0.5 mEq/ml; 2 mEq/kg IV given
over at least 2 minutes.
4. Naloxone hydrochloride 0.4 mg/ml; 0.1 mg/kg ET or IV
given rapidly.
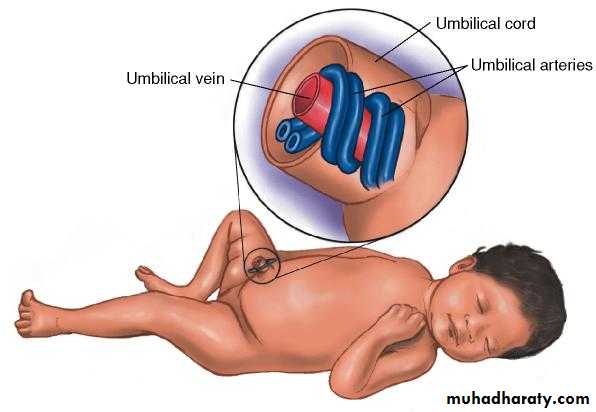
The umbilical cord
ExaminationTo establish that the baby does not have a majorabnor mality such as spina bifida and the full examination at a latertime.
Ideally it should take place 24–48 h after birth
A history should be taken including maternal obstetric and family historyto identify problems in the baby that will require further management or follow up.
abnormalities of posture and asymmetry of facial or limb movements.
Evidence of jaundice, polycythaemia,anaemia or rashes is noted and anal atresia excluded.examining along the midline and then passing to the limbs. Starting with the head, the facial features should be noted and thought given to dysmorphic syndromes.
The palate needs to be examined visually to exclude a clef palate or bifid uvula which signifies a sub-mucus cleft.
The eyes must be examined by ophthalmoscopy to exclude cataracts.
Eye movements may not be fully coordinated in the first week of life
Specific Neonatal Situations
• Apnoea Usually due to hypoxia or hypothermia; other causes include:• Narcotic or CNS depressants
• Weakness of respiratory muscles
• Septicemia
• Metabolic disorders
• CNS disorders
• Seizures…may indicate serious illness.
• Fever…uncommon and may also indicate serious underlying illness.
• Hypothermia…may indicate sepsis.
• Hypoglycemia…
• Vomiting/diarrhea
Premature Infants
• Are at a greater risk of respiratory depression, head injury, changes in blood pressure, intraventricular hemorrhage

Babies born preterm may fail to clear lung liquid or produce surfactant so that
pulmonary compliance remains low and the high negative intrathoracic pressures required for lung inflation during the first breath persist.These infants develop respiratory distress and may require ventilation and surfactant replacement.
Infant feeding
Milk production (lactogenesis)Two similar, but independent, mechanisms are involved in the establishment of lactation the first mechanism causes the release of prolactin which acts upon the glandular cells of the breast to stimulate milk secretion and the second induces the release of oxytocin which acts upon the myoepithelial cells of the breast to induce the milk ejection reflex
Human breast milk is a complex bioactive fluid that alters in composition over time.
Colostrum has a greater concentration of protein and minerals and also contains antibodies,humoral factors, growth factors and interleukins.Breastfeeding contraindicated
Cytotoxics, ergotamine, immunosuppressants, lithium,phenindione, chloramphenicol, tetracyclinesdrugs to be used with caution during breastfeeding
Antiarrhythmic Amiodarone
Antibiotic Metronidazole
Anticonvulsant
Antidepressant Doxepin, selective serotonin re-uptake inhibitors (SSRI)
Antihypertensive Betablockers
Anxiolytic Benzodiazepines,
Radioisotopes
Thank you
for your attention