Impaction
Principles of management of impacted teeth
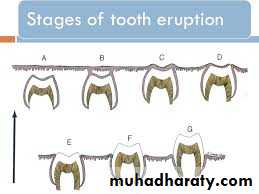
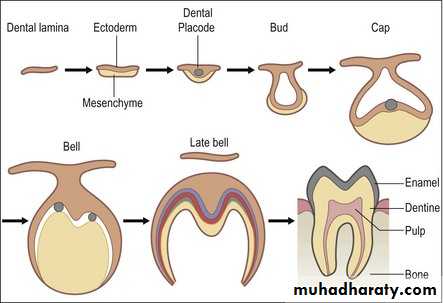
Tooth eruption :is defined as the movement of a tooth from its site of development within the alveolar bone to its functional position in the oral cavity.Root elongation, alveolar bone remodeling and periodontal ligament formation can explain tooth eruption. tooth eruption can be arbitrarily divided into the following six stages:
Stages of Tooth eruption
1. Pre-eruptive stage.2. Alveolar bone stage.
3. Mucosal stage.
4. Pre-occlusal stage.
5. Occlusal stage.
6. Maturation stage.
The normal eruption of the tooth can be interfered at any of the stages from one to four and an impaction will result.
An impacted tooth: is the one that fails to erupt into proper functional position in' the dental arch within the expected time.
Another definition set forth by Andreasen et al. 1997 is that:
impaction: is a cessation of the eruption of a tooth caused by a clinically or radiographically detectable physical barrier in the eruption path or by an ectopic position of the tooth.
It occurs where there is prevention of complete eruption due to:
• Lack of space in the dental arch (main cause).• Obstruction by another tooth.
• Development in abnormal position.
• Dense overlying bone.
• Thick fibrous tissue.
• Odontogenic tumors.
The mandibular third molar is the most commonly impacted tooth in the mouth followed by maxillary third molar, maxillary canine, mandibular canine, mandibular second premolar, maxillary second premolar and second molars.
Many theories have been proposed to explain the etiology of impaction; it seems that the discrepancy between teeth size and jaw size is probably the result of a combination of genetic and environmental factors. The inheritance of large teeth in small jaws is aggravated by the lack of maximal jaw growth and reduced arch length due to the consumption of refined softened diet which requires minimal chewing. Another factor is retarded maturation of third molars. These factors particularly affect third molars and canines, also sufficient space for the eruption of mandibular second premolar maybe lost because of the premature extraction of the overlying deciduous second molar allowing for the permanent first molar to drift forwards.
Some systemic factors that may influence impaction of permanent teeth include: Hereditary syndromes like Cleidocranial dysostosis, endocrine deficiencies (hypothyroidism and hypopituitarism), Down syndrome, irradiation and cleft lip and palate.
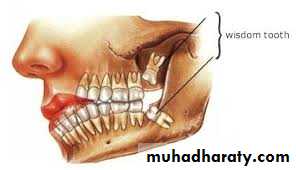
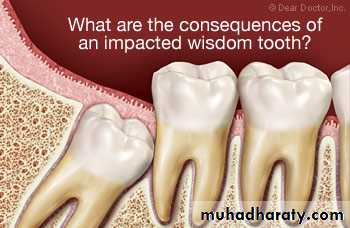
• Impacted lower third molars
Impacted lower third molarsThird molars are the last teeth to erupt in the human dentition, and are popularly known as Wisdom teeth. The surgical removal of impacted third molars is the most common oral surgical procedure performed.
The mandibular third molar tooth germ is usually visible radiographically by age 9 years, and cusp mineralization is completed approximately two years later. Crown formation is usually complete by the age 14 years, by the age of 16 years the roots are approximately 50% formed and they are completely formed with open apex by age 18 years.
The eruption of lower third molar is complete at the average age of 20 years but it can occur up to age 25 years. The prevalence rate of lower third molar impaction varies from one population to another ranging from 9.5% to 50%.
Indications for removal of impacted lower third molars
1. Infection; including pericoronitis, cellulitis, abscess and osteomyelitis.2. Unrestorable dental caries, non-treatable pulpal and/or periapical pathology.
3. Periodontal disease of the adjacent tooth.
4. Interference with orthodontic treatment
5. Facilitation of restorative treatment including provision of prosthesis.
6. Internal/ External resorption of the impacted tooth or adjacent teeth.
7. Pain directly related to a third molar, pain associated with TMJ or masticatory musculature should be excluded.
8. Tooth in the line of bone fracture or impeding trauma management.
9. Fracture of tooth.
10. Teeth associated with cysts or tumors.
11. Teeth impeding orthographic surgery or reconstructive jaw surgery.
12. Satisfactory tooth for use as donor for transplantation.
13. Prophylactic removal in the presence of specific medical and surgical conditions, including; before organ transplantation, chemotherapy or radiotherapy.
Classification of impacted lower third molars
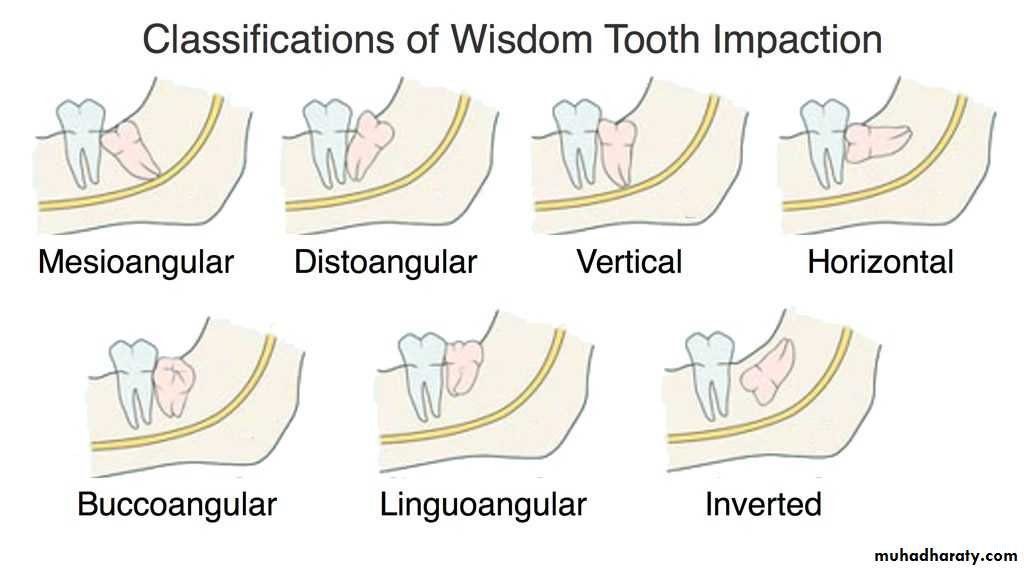
several methods. of classification of impacted lower third molars have described in the literature.The most common classification is according to Winter (1926), Archer (1975) and Kruger (1984) which is based on the relationship of the impacted tooth to the long axis of the second molar, so the impacted teeth are either;
• Vertical , 6. linguoangular 7. and inverted
• horizontal
• Mesioangular
• Distoangular
• buccoangular.
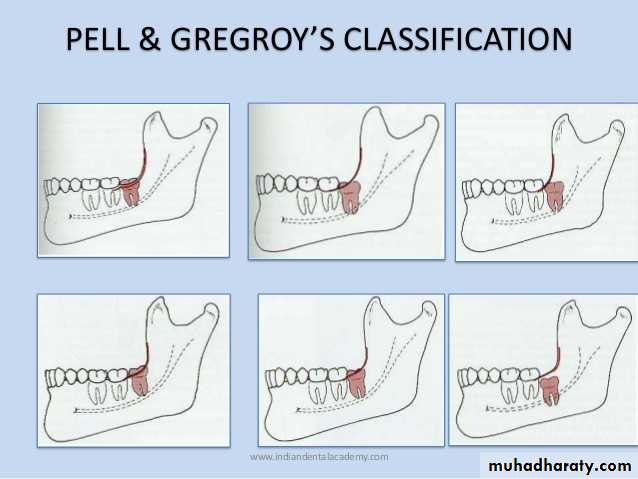
Another classification system to assess the depth of impaction was proposed by Pell and Gregory, they classified the depth of impaction into two categories; the first category is as follows:
Position A: the highest portion of the impacted tooth is on the same level or above the occlusal plane of the second molar.
Position B: the highest portion of the impacted tooth is below the occlusal plane but above the cervical line of the second molar.
Position C: the highest portion of the impacted tooth is below the cervical line of the second molar.
The second category related the impacted third molar to the ascending ramus of the mandible as follows:
Class I: none of the crown is in the ramus of the mandible.
Class II: less than half of the crown is in the ramus.
Class III: more than half of the crown is in the ramus.
Killey and Kay classified the state of eruption of impacted third molars into:
• Erupted.
• Partially erupted.
• Unerupted.
Clinical examination
After taking a thorough medical and dental history, with a special consideration to the age, since this factor may significantly influence the management of impacted third molars, studies have shown that the complications of surgery increase with increased age.The clinical examination starts with a general assessment of the size and the build of the patients, patient's attitude is important as this reflects the way he/she will respond to the stress of surgery. General fitness is essential.
Intraoral examination should include:
• The mouth opening.
• Oral hygiene.
• General state of the dentition, especially the first and second molars.
• Examination of the third molar, if it is visible or not, carious, the condition of the soft tissue over the impacted tooth is noted; if there are signs of pericoronitis treatment will be required before the operation.
• The external and internal oblique ridges of the mandible are palpated, if the external oblique ridge is low, relatively vertical and posterior to the tooth, the alveolar bone will be thin, while if the ridge lies high and forward, the alveolar bone will be thick and the extraction more difficult.
• The position and the condition of the upper third molar is checked and its relationship with the lower third molar is noted.
• The related lymph nodes should be palpated to determine the extent of infection.
Radiographic examination
The radiographic examination should demonstrate:• The whole impacted tooth.
• The investing bone.
• The adjacent tooth.
• The inferior dental (alveolar) canal.
• the anterior border of the ascending ramus.


Periapical radiograph offers the highest definition and it should be used whenever possible, but the film should be positioned with care.
Orthopantomogram (OPG) is regarded as the radiograph of choice, its main advantages are; the low radiation exposure and its ability to demonstrate the entire dental arch.

Occlusal films are used in difficult cases especially in unerupted teeth in conjunction with another view at right angle, this is necessary to understand the problem in 3 dimensions.
Cone beam CT (CBCT) is relatively a new technique and it is indicated when on OPG there is a suggestion of a relationship between the roots of the impacted tooth and the inferior dental (alveolar) canal



Radiographic assessment
It aims to estimate how much work will need to be done at the operation and what technical difficulties will need to be overcome. The following features should be considered:• Angulation of the impacted tooth
• The depth of the impacted tooth, it can be assessed by Pell and Gregory classification, but other methods for depth assessment have been proposed.
• The relationship to the inferior dental canal, certain features may indicate the close proximity to the inferior dental canal; such as narrowing of the canal, loss of the continuity of the radio-opaque roof of the canal, overlapping, deflection of the canal or dilacerations of the roots.
• Crown features.
• Root morphology, e.g. fused roots, curved roots ...etc.• Bone density.
• Any associated pathology like cysts or tumors.
• The state of the second molar (root morphology, caries, restoration or resorption ...etc.)
Removal of impacted lower third molar
The choice of anesthesia depends on many factors:• The anticipated difficulty.
• Patient's anxiety.
• The number of the impacted teeth removed.
• Availability of patient-care options.
Surgical extraction of impacted third molars is commonly done under L.A. other choices include L.A. with sedation and G.A.
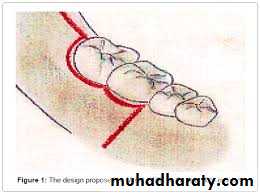
The incision design is either:
1. Envelope flap.
2. Triangular flap, which is an envelope flap with a vertical releasing incision.
The degree of soft tissue reflection depends on the type of impaction and the quantity of bone removal required. Good visual access is essential.
The lingual tissue is gently reflected and protected to avoid any damage to the lingual nerve which is anatomically close to the lingual aspect of the third molar
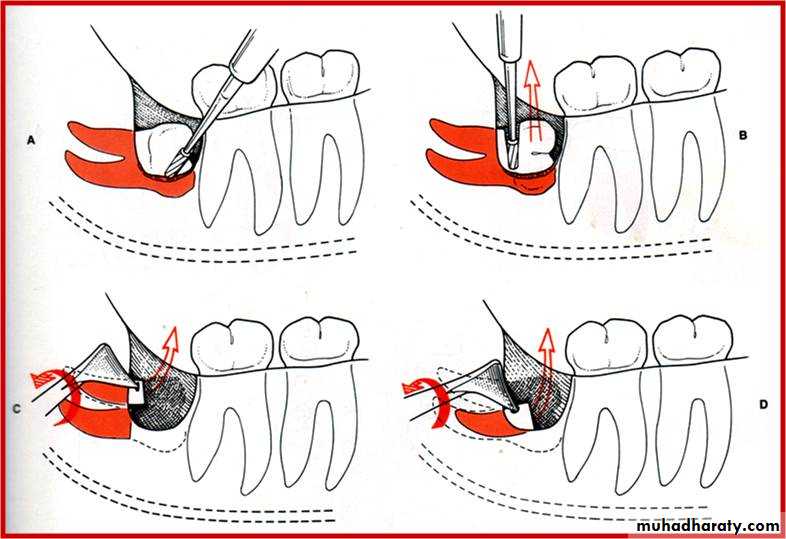
Bone removal is commonly achieved using burs and a high torque, low speed handpiece that does not blow air into the surgical field, and is carried out on the buccal, distal and mesial aspects of the tooth to facilitate the removal of the tooth and to create points of application for the elevators on the mesial and buccal aspects of the tooth

The intention is to create a deep narrow gutter around the crown of the impacted tooth (buccal guttering technique). Occasionally tooth sectioning is needed to deliver the tooth in segments, the tooth should not be sectioned completely using a bur since this may cause damage to the lingual nerve but it should be done through 3/4 the way and split the remaining tooth with a straight elevator.
Another method for bone removal using chisel and mallet is termed the lingual split technique, it involves increased incidence of lingual nerve damage and it is not convenient for patients under L.A.
Recently Erbium laser (Er) YAG was used in bone removal. The main advantage being reduced inflammatory response.
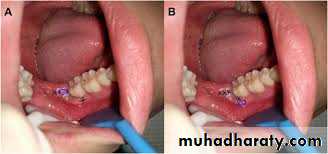
After tooth removal any debris and the remaining follicular tissue are cleaned out, sharp bone smoothed, copious irrigation of the socket and underneath the flap is carried out.
The flap is repositioned and sutured using resorbable or non-resorbabal suture, two sutures may suffice, the most important one is just distal to the second molar and the other in the centre of the posterior incision, a third suture can be placed in the buccal relieving incision.

Postoperative care include; instructing the patient to bite on a gauze pad for about one hour, not to rinse during the first 24 hours, the use of ice bag on the face for about 15 minutes on and 15 minutes off for the rest of the day. Antibiotics (e.g. Amoxicillin) and analgesics are prescribed, some clinicians use corticosteroids preoperatively or postoperatively to reduce the inflammatory response. Chlorhexidine mouth wash, twice daily, starting the next postoperative day. Sutures are removed 7 days after surgery.