د. لمى اجنة 20\2\2018
عدد الاوراق ( 5 ) م\2\موصل lec: 2EMBRYOLOGY
DIGESTIVE SYSTEM
The primitive gut is formed by partial incorporation of the endoderm into the embryo due to cephalocaudal & lateral foldings of the embryo.
The endoderm forms the epithelial lining of the digestive tract & its glands such as liver & pancreas, while the muscular & peritoneal components are derived from the local surrounding splanchnic mesoderm.
The primitive gut divided into :
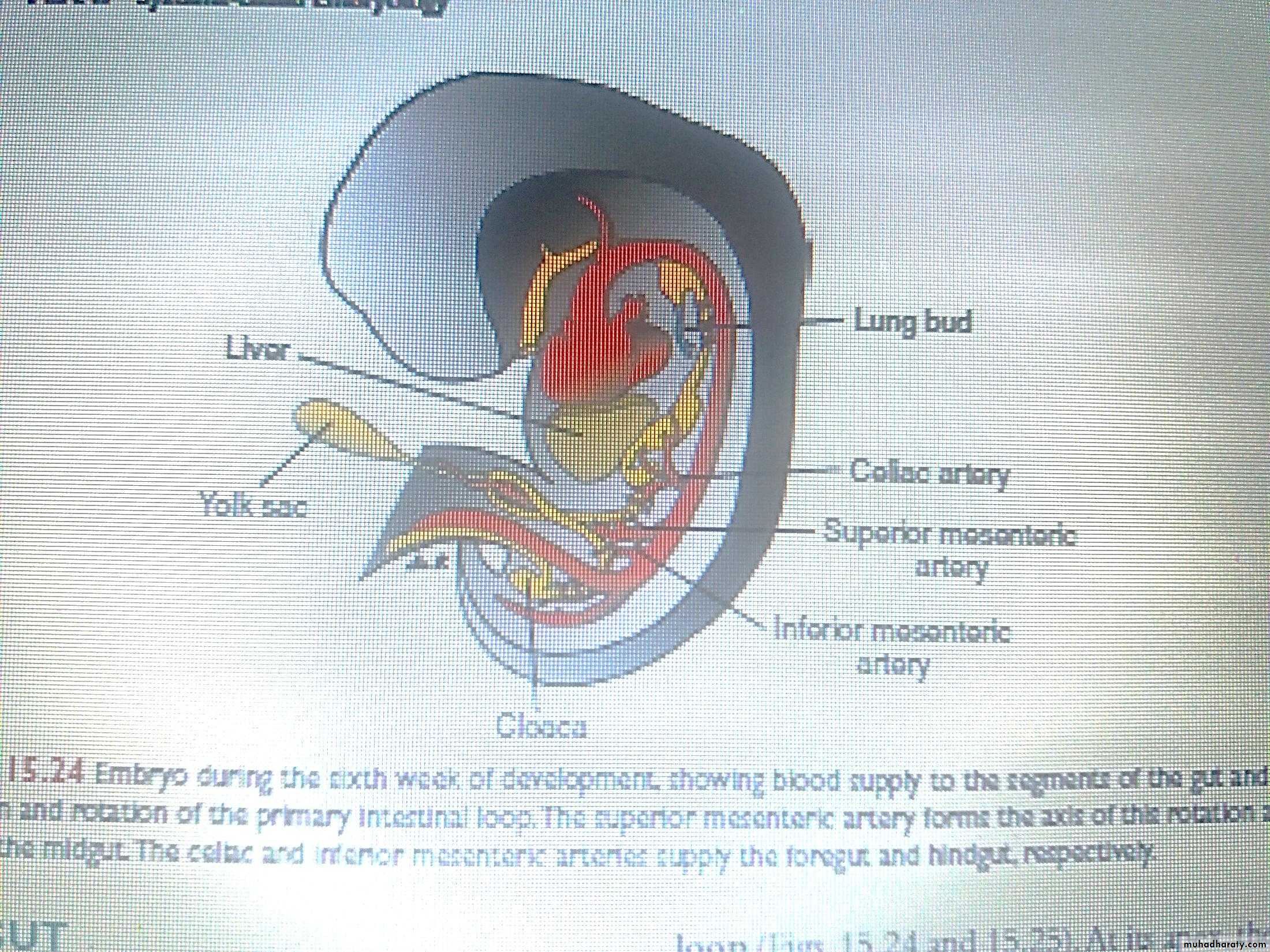
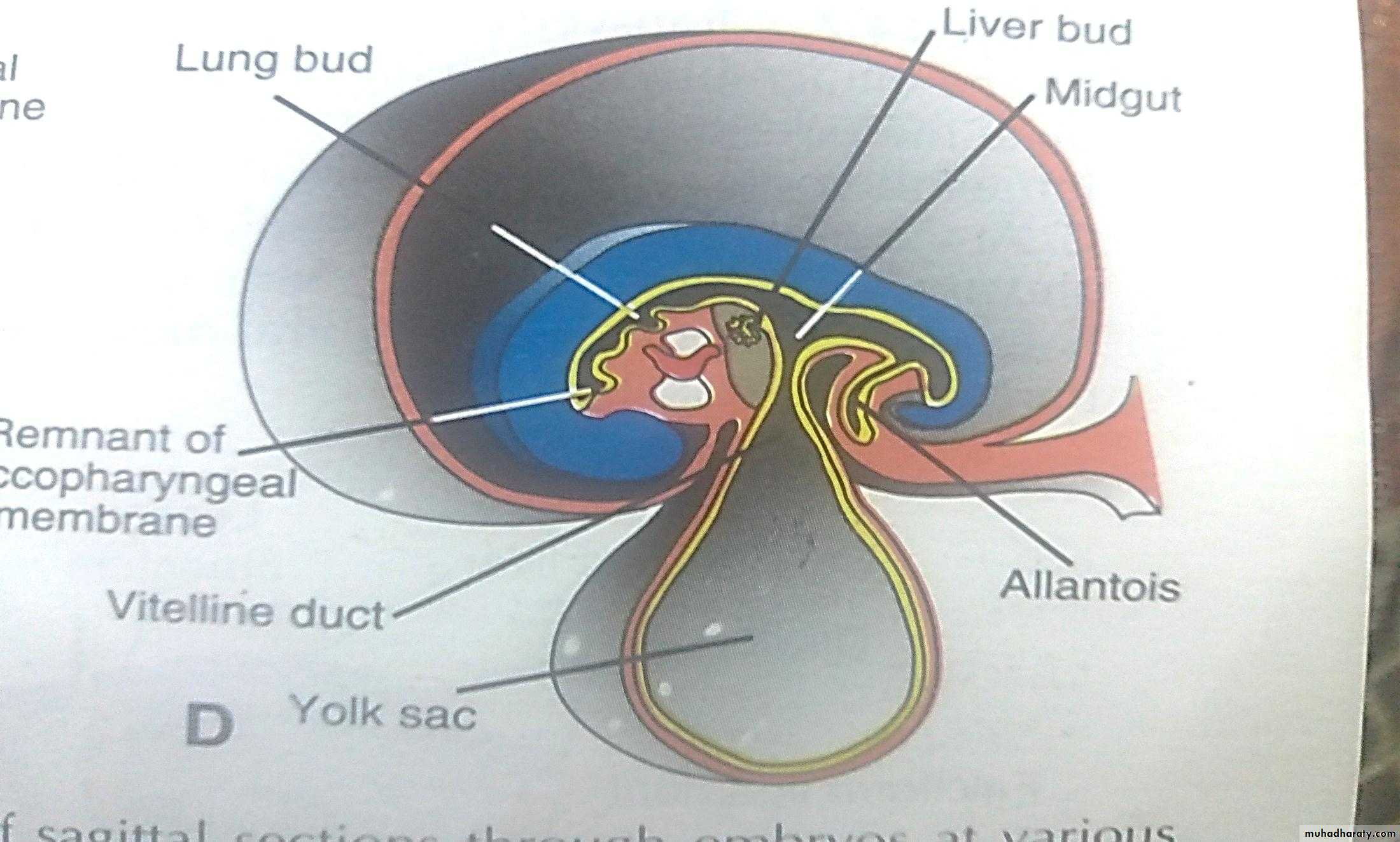
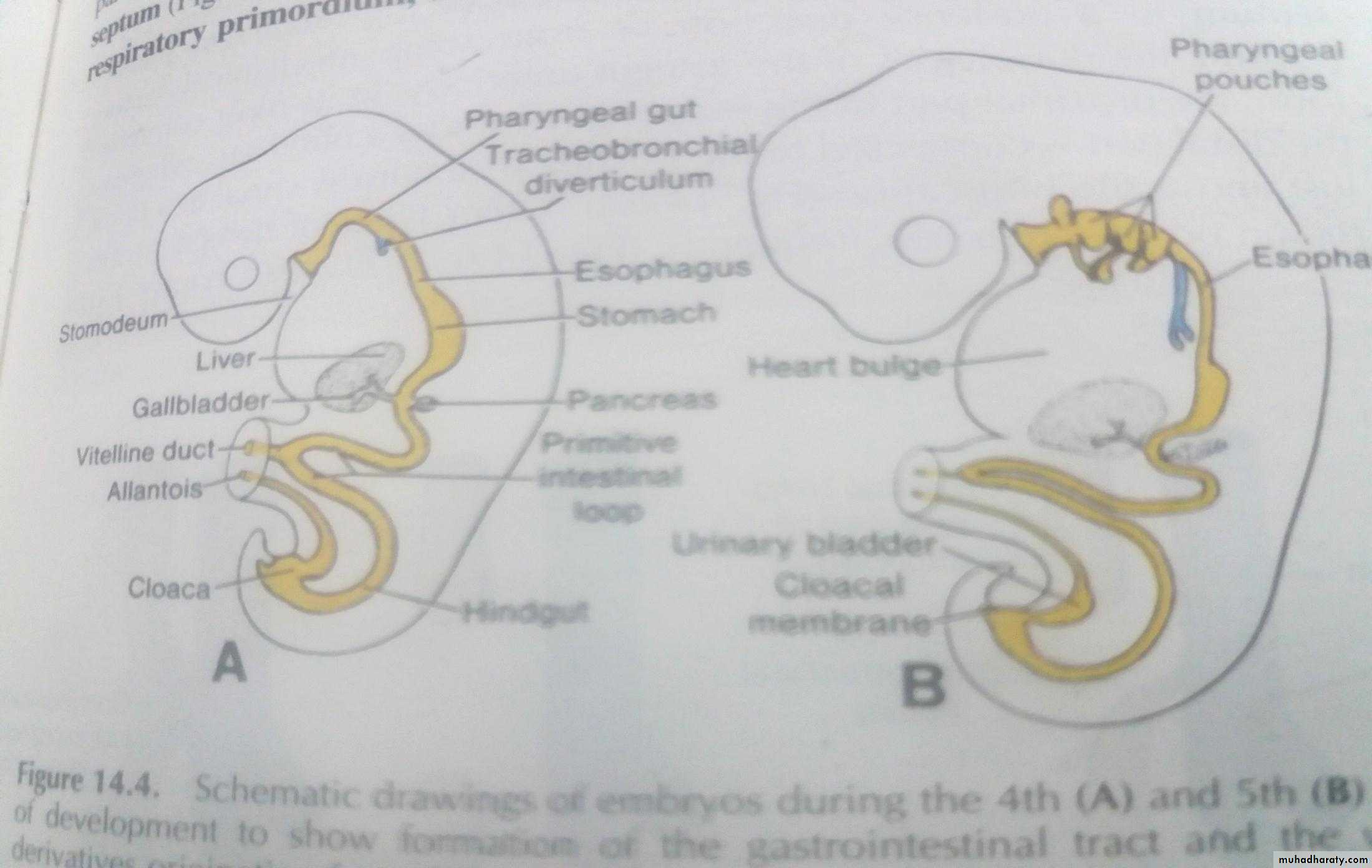
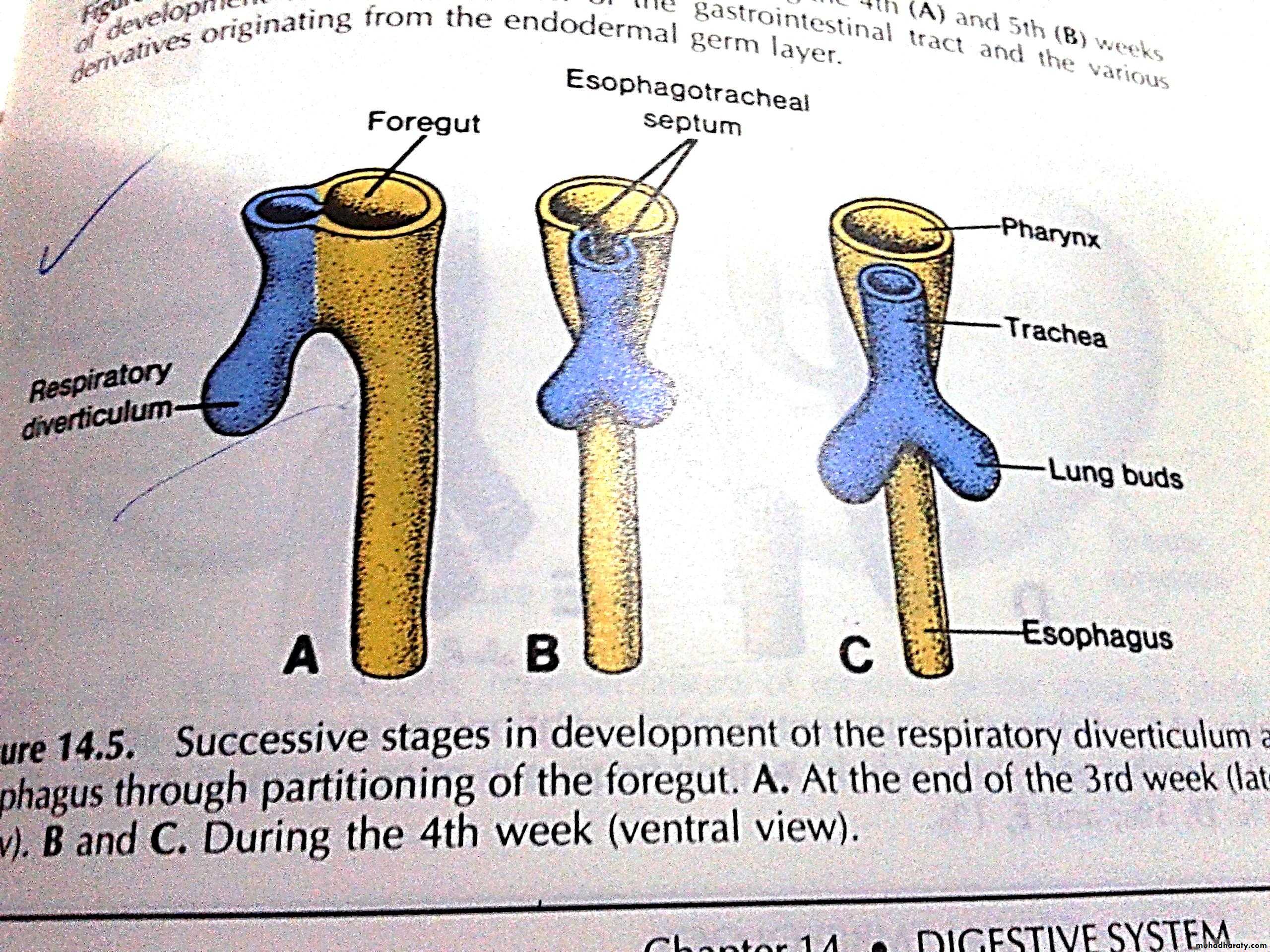
1. Pharyngeal gut : which begin from the buccopharyngeal membrane to the tracheobronchial diverticulum. 2. foregut : extends from the region caudal to the tracheobronchial diverticulum to the liver bud. 3. midgut : extends from the region caudal to the liver bud ton the junction of the right 2/3 & the left 1/3 of the transverse colon.The midgut remains temporarily connected to the yolk sac through a canal called yolk stalk or vetilline duct.
4. Hind gut: extend from the left 1/3 of the transrvese colon to the cloacal membrane.
The Fore gut:
The part of the fore gut cranial to the side of the origin of the laryngotracheal groove forms part of the oral cavity as well as the pharynx, while its part caudal to the groove develops into the following parts:Esophagus
Stomach
Upper half of duodenum
The esophagus:
The esophagus develops the fore gut just caudal to the opening of the laryngotracheal tube. It is long and narrow tube ,then proliferation of its epithelial lining leads to transient obliteration of its lumen, which is rapidly becomes re-canalized again after short time.Initially, the esophagus is short, but with descent of heart &lung, it lengthens increase rapidly.
The muscular coat, which is formed by surrounding mesenchyme, is striated in its upper 2/3 &innervated by the vagus nerve, the muscle coat is smooth in the lower 1/3 & is innervated by the splanchnic plexus.
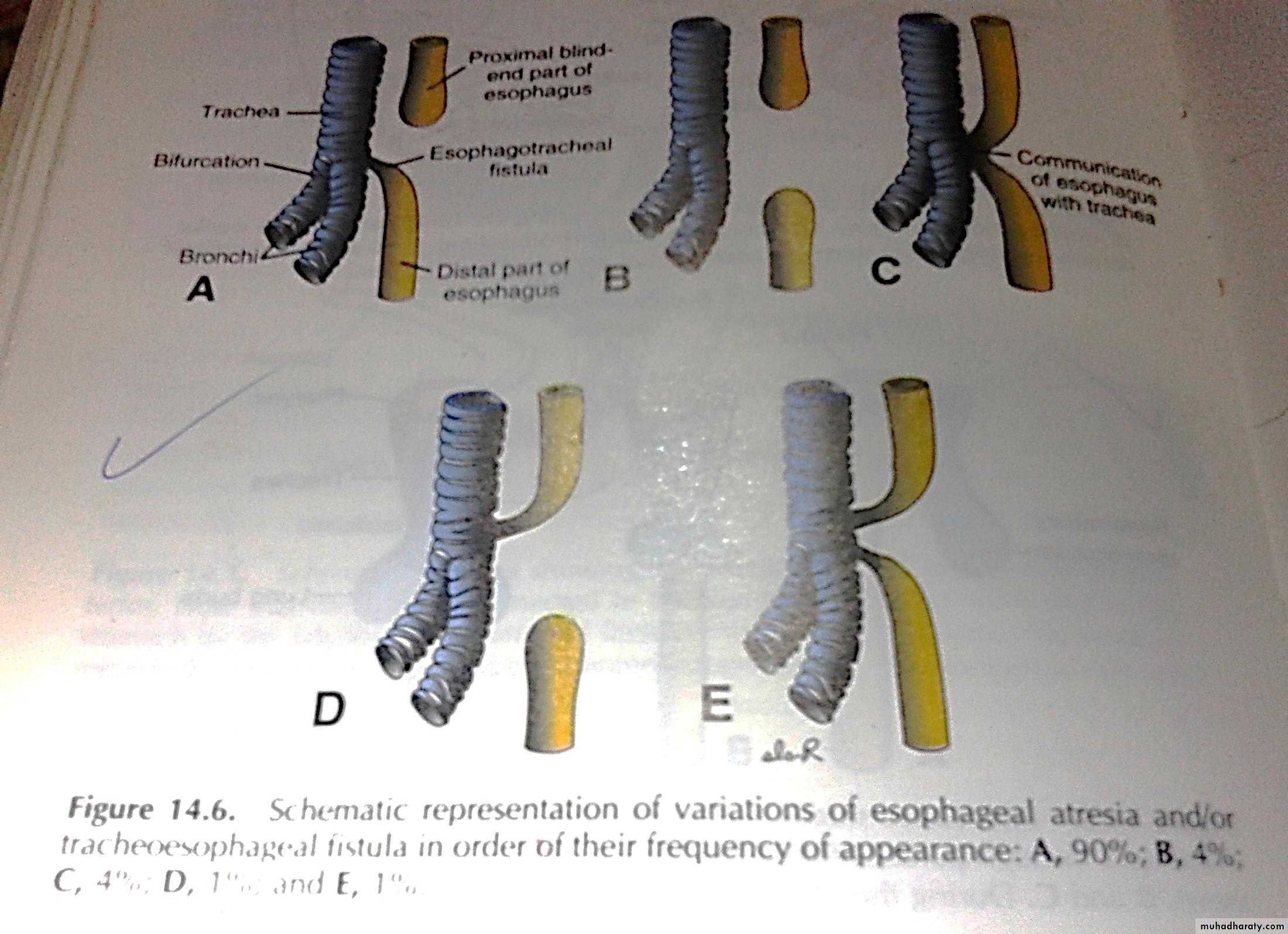
Congenital abnormality of esophagus
1-Esophageal Atresia: due to complete failure of re-canalization, usually associated with accumulation of excess fluid in aminotic sac(polyhydramnios)2-tracheo esophageal fistula (TEF): in its most common form, the proximal part of the esophagus ends as a blind sac, whereas the distal part is connected to the trachea by a narrow canal at a point just above the bifurcation . In rare cases, both the proximal &distal ends are opened in the trachea
2-Esophageal stenosis: due to incompelet re-canalization & usually occur in the lower 1/3of esophagus
3-Abnormal short esophagus: this lead to stomach is pulled up into esophageal hiatus through diaphragm result in congenital hiatus hernia
Stomach:
Its develop at the distal end of esophagus in the 4th week of development .Its position &shape is change greatly due to its rotation &due to different rates of growth of its wall.
Its appear as fusiform dilatation of the foregut which is attached ventrally by ventral mesogastrium &dorsally by dorsal mesogastrium.
(
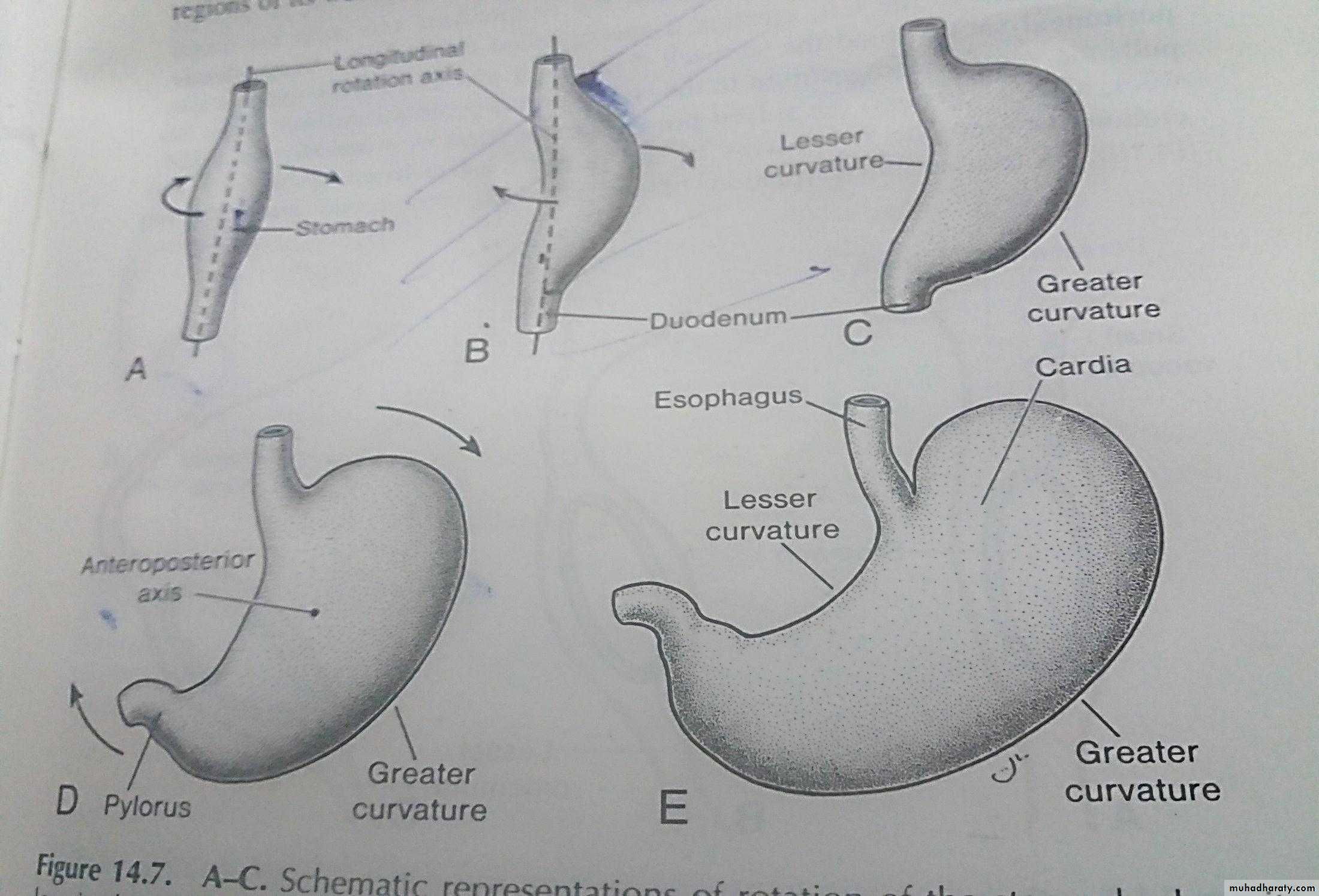
:The position change due to rotation in 2 axis
1-Longitudinal Axis 2-Anterioposterior Axis.
1-Longitudinal Axis:
Around its longitudinal axis the stomach rotates 90 degree clockwise, causing its lefts side to face anteriorly &its right side become posteriorly & for this reason the left vagus nerve now innervates the ant. Wall &the right vagus nerve innervate the post. Wall .
During this rotation the original post. Wall (now to the left)grows faster than the ant. Wall (now to the right ) &this result in the formation of the greater curvature in the left side &lesser curvature in the right side
2-Anterioposterior axis
Around its anterioposterior axis , the caudal or pyloric region of the stomach moves upward &to the right& the the cardial or cephalic region moves downward & to the left.
The liver will develop in the ventral mesogastrium ., thus dividing the ventral mesogastrium into:
Lesser omentum between the lesser curvature of stomach & porta hepatis of liver.
Falciform lig. & coronary lig. Connect the liver to the inner surface of ant. Abd. Wall &diaphagram, respectively.
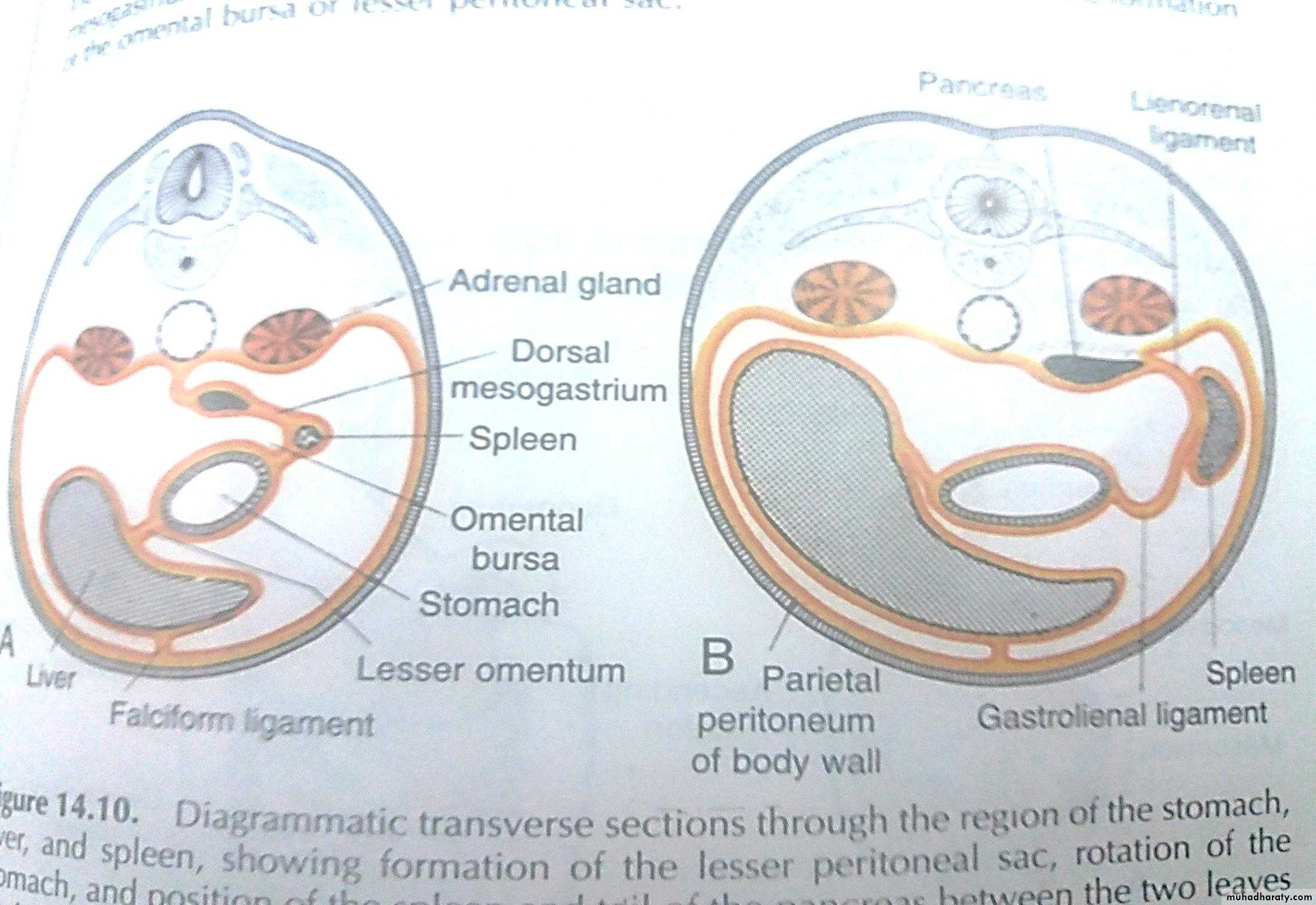
The spleen will develop in the dorsal mesogastrium, thus dividing the dorsal mesogastrium into:
Gastrolienal lig. Lie anterior to the spleen that connect the stomach to the spleen .
Lienorenal lig. Lie posterior to the spleen That connect the spleen to the kidney.
Also due to this rotation the ventral mesogastrium move to the right &dorsal mesogastrium move to the left side.
The pulling of the dorsal mesogastrium to the left will lead to the formation of a pouch behind the stomach called omental bursa.or Lesser sac which become connected with greater peritoneal cavity by epiploic foramen(foramen of winslow)
:Congenital abnormalities of stomach
1- Congenital hypertrophic pyloric stenosis: it’s the most common abonormalities, in which there is narrowing of the pyloric lumen due to hyperatrophy of the muscle of the walls of the stomach in the pyloric region, causing severe vomiting in infants.2-Pyloric atresia.
3-Duplication of stomach.
4-Pancreatic tissue may develop in side the submucosa of the pyloric antrum due to invasion of the stomach by pancreatic bud.
5-Prepyloric septum.
DUODENUM:
Its formed by the terminal part of the foregut &cephalic part of the midgut directly distal to the origin of liver bud.
Due to the rotation of the stomach, it take the shape of –C- loop, rotate to the right.
This rotation , together with the rapid growth of the head of pancreas, causes the doudenum to swing from its initial midline position to the left side of abdominal cavity .
The duo. & head of pancreas are pressed against the post. Abd. Wall &the dorsal mesoduodenum fuses with adjacent peritoneum ,then both layers are disappear & both of them come to lie retroperitonealy
The dorsal mesoduodenum disappear entirely except at the pylorus of stomach where a small portion of duodenum (duodenal cap) remains intraperitonealy..
Since the foegut is supplied by celiac artery & the midgut is supplied by the superior mesenteric artery so, the duodenum is supplied by branches of both arteries.
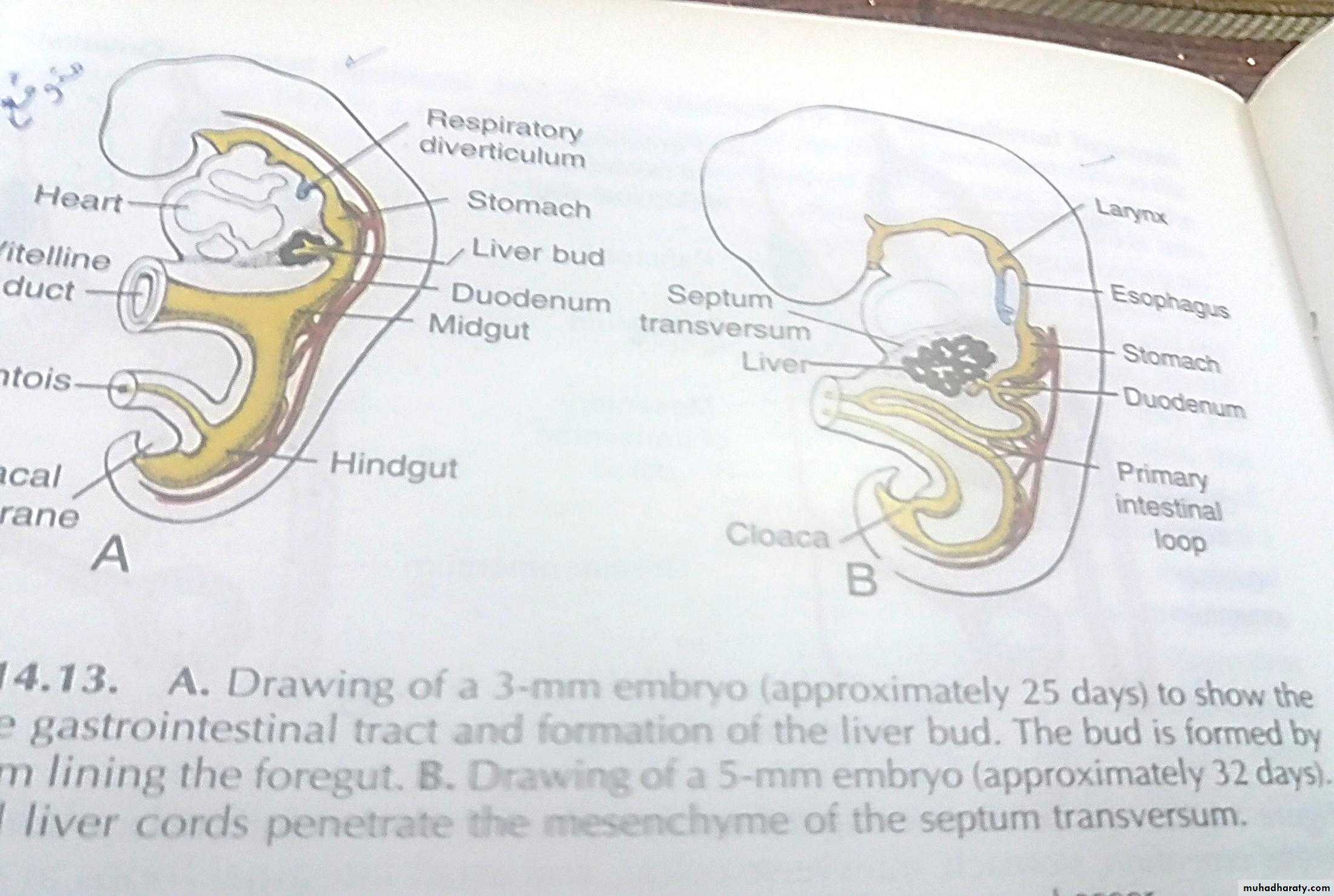
Liver and gallbladder:
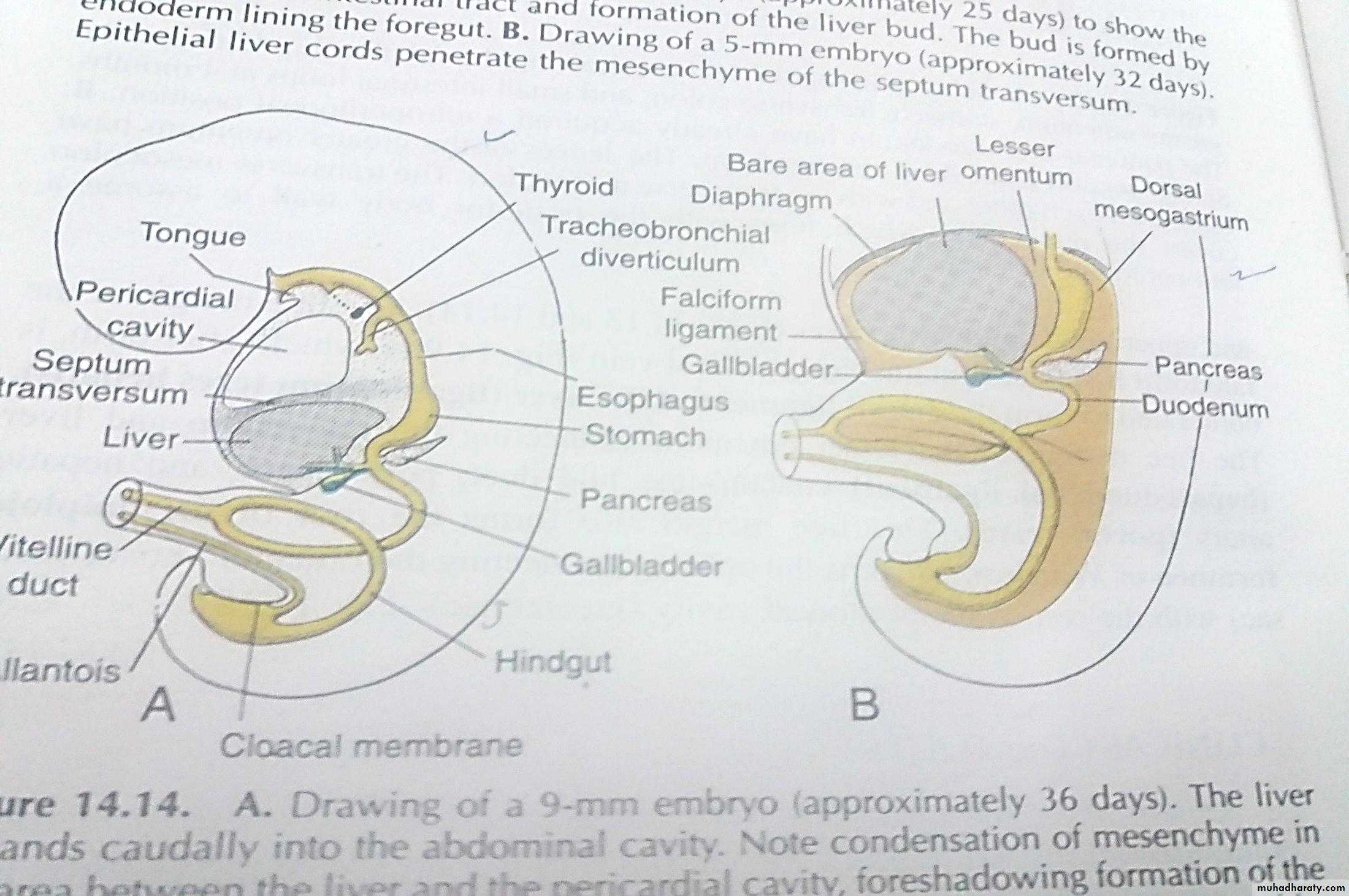
During the 3rd-4th wk of development , the liver is formed as an outgrowth from the endodermal lining of the distal part of the foregut.This outgrowth is called Liver bud (hepatic diverticulum).
Its consist of proliferating cell strands which penetrate the septum transversum,which is mesodermal plate between the pericardial cavity &yolk sac stalk.
i.e septum transversum, will form the diaphragm in future.
The liver cords give rise to the parenchyma of the liver & the lining of the biliary system, while the hemopoietic, kupffer & connective tissue cells are derived from the mesoderm of septum transversum.
The liver grows rapidly & due to this rapid growth liver begins to protrude into the abdominal cavity.
The mesoderm of septum transversum between the the liver & the ventral abdominal wall becomes stretched & very thin , thus forming a thin membrane , known as the falciform ligament.
The mesoderm of septum between the liver & the foregut(duodenum &stomach) becomes stretched &membranous forming the lesser omentum.
While hepatic cell strands continue their proliferation & penetration in the septum transversum, the connection between the liver& the foregut (duodenum) narrows leading to the formation of the bile duct which give rise to the gall bladder & cystic duct.
With further development of the proliferating hepatic cell strands intermingle with vitelline &umbilical veins forming the hepatic sinusoids.
The mesoderm that surrounds the liver will differentiate into visceral peritoneum except on its cranial area where the bare area is formed.
Functions of the liver:The main functions are:
Hemopoietic function: which means the formation of WBC,RBC.Formation of the bile by the hepatic cells from the 12th wk of development.
Storage of glycogen.
Congenital abnormalities:
Atersia of the bile duct ( or the gall bladder).Dplication of the bile duct (or the gall bladder).
Diverticulum of the gall bladder.
Stenosis of the bile duct.