malpresentation
المرحلة الرابعةنسائية
د.شيماء
العدد11
15\2\2018
تسلسل 1
Malpresentation
• Definitions• Presentation:- The lowest part of the fetus that present to the lower uterine segment & the cervix.
• About95%of fetuses at term present by the vertex in labour;so is called normal presentation
• Malpresentation:-When the presentation is other than vertex,like breech face brow&shoulder.
Breech presentation
When the buttocks of the fetus enters the pelvis before the head, the presentation is breech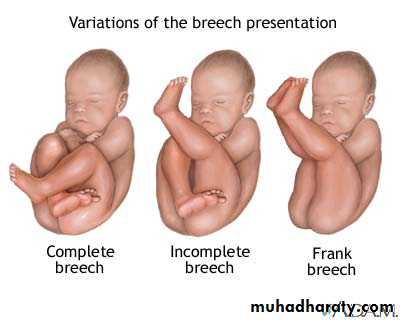
Frank breech : the lower extremities are flexed at the hip joint and extended at the knees
Complete breech : one or both knees are flexedIncomplete breech : one or both hips are not flexed
Footling breech : is an incomplete breech with one or both feet below the breech
Diagnosis of beech presentation:
History :-subcostal discomfort
-feeling the baby kick in the lower abdomen
Abdominal Examination :
-hard round ballotable head is found at the fundus and the softer breech at the lower part of the uterus.
-fetal heart sound heard above the
umbilicus.
Vaginal examination
For diagnosis after rupture of membranes additional informations obtained :In case of flexed breech afoot may present ,with extended breech the rounded buttocks resemble fetal head but the hardness of bone&sutures are abscent,anus& sacrum are identified.Antenatal management of breechpresentation
If a breech presentation is clinically suspected at or
after 36 weeks, this should be confi rmed by ultrasound scan.
The scan should document fetal biometry,
amniotic fl uid volume, the placental site and the
position of the fetal legs. The scan should also look
for any anomalies previously undetected
Predisposing factors for breech presentation
Maternal• Fibroids
• Congenital uterine abnormalities, e.g. bicornuate uterus
• Uterine surgery
Fetal/placental
• Multiple gestation
• Prematurity
• Placenta praevia
• Abnormality, e.g. anencephaly or hydrocephalus
• Fetal neuromuscular condition
• Oligohydramnios
• Polyhydramnios
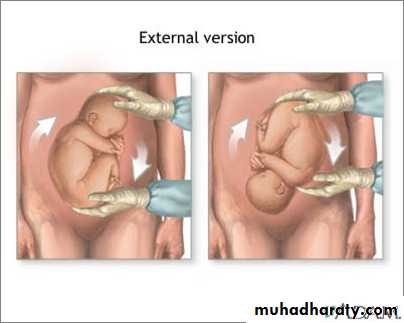
External cephalic version ECV
The procedure is performed at or after 37
completed weeks by an
experienced obstetrician at or near
delivery facilities.
a tocolytic (e.g. nifedipine).
The woman is laid fl at with a left lateral tilt
emptied her bladder and is comfortable.
With ultrasound guidance.
A fetal heart rate trace must be performed before and after the procedure and it
anti-D if the woman is Rhesus-negative
In this maneuver , the breech is elevated from the pelvis and one hand is used to manipulate this upward in the direction of a forward role, while
the other hand applies gentle pressure to fl ex the fetal head and bring it down to the maternal pelvis If the procedure fails, or becomes
diffi cult, it is abandoned.
Contraindications to ECV
• Fetal abnormality (e.g. hydrocephalus)• Placenta praevia
• Oligohydramnios or polyhydramnios
• History of antepartum haemorrhage
• Previous Caesarean or myomectomy scar on the uterus
• Multiple gestation
• Pre-eclampsia or hypertension
• Plan to deliver by Caesarean section anyway
Risks of ECV
• Placental abruption
• Premature rupture of the membranes
• Cord accident
• Transplacental haemorrhage (remember anti-D
administration to Rhesus-negative women)
• Fetal bradycardia
Mode of delivery
If ECV fails, or is contraindicated, and Caesarean section is not indicated for other reasons, then womenshould be counselled
1)regarding elective Caesarean section and
2) planned vaginally delivery.
Prerequisites for vaginal breech delivery
Feto-maternal:The presentation should be either extended (hips flexed, knees extended) or
flexed (hips flexed, knees flexed but feet not below the fetal buttocks).
There should be no evidence of feto-pelvic disproportion with a pelvis clinically thought to be adequate and an
estimated fetal weight of 3500 g (ultrasound or clinical measurement).
no evidence of hyperextension of the fetal head, and
fetal abnormalities that would preclude safe vaginal delivery (e.g. severe hydrocephalus) should be excluded.
Technique
Delivery of the buttocks
In most circumstances, full dilatation and descentof the breech will have occurred naturally. When
the buttocks become visible and begin to distend the
perineum, preparations for the delivery are made.
The buttocks will lie in the anterior–posterior diameter.
Once the anterior buttock is delivered and the anus is seen over the fourchette (and no sooner than this), an episiotomy can be cut.
.
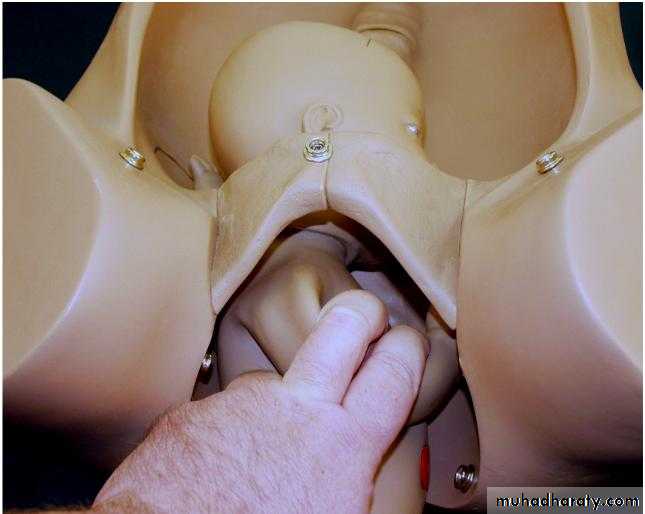
Delivery of the legs and lower body
If the legs are flexed, they will deliver pontaneously.If extended, they may need to be delivered using
Pinard’s manoeuvre. This entails using a finger to
flex the leg at the knee and then extend at the hip,
first anteriorly then posteriorly. With contractions
and maternal effort, the lower body will be delivered.
Usually a loop of cord is drawn down to ensure that
it is not too short.
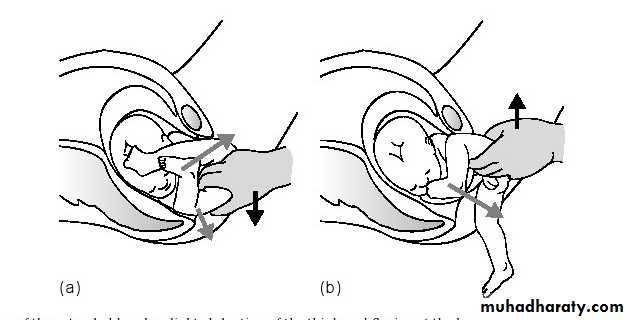
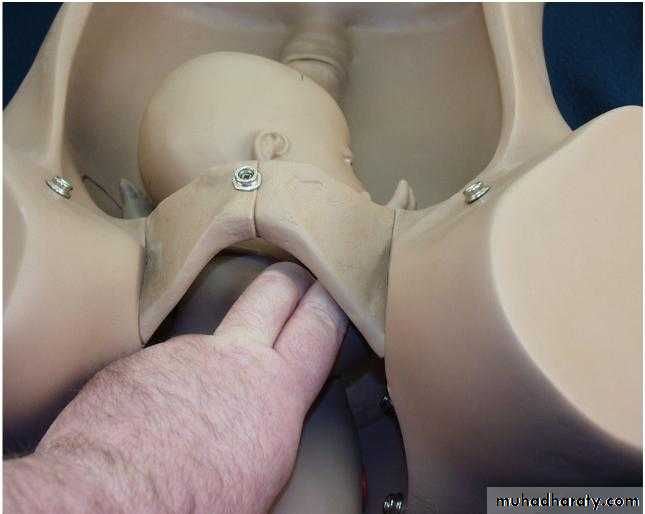
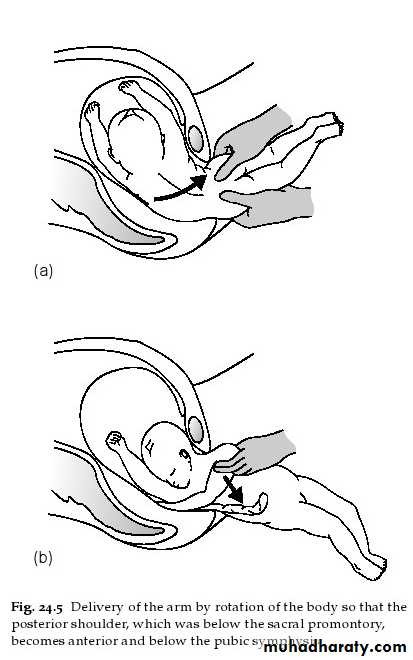
Delivery of the shoulders
The baby will be lying with the shoulders in the transverse diameter of the pelvic mid-cavity. As theanterior shoulder rotates into the anterior–posterior
diameter, the spine or the scapula will become visible.
At this point, a finger gently placed above the shoulder
will help to deliver the arm. As the posterior arm/shoulder reaches the pelvic floor, it too will rotate anteriorly (in the opposite direction). Once the
spine becomes visible, delivery of the second arm
will follow. This can be imagined as a ‘rocking boat’with one side moving upwards and then the other.
Loveset’s manoeuvre essentially copies these natural
Movements
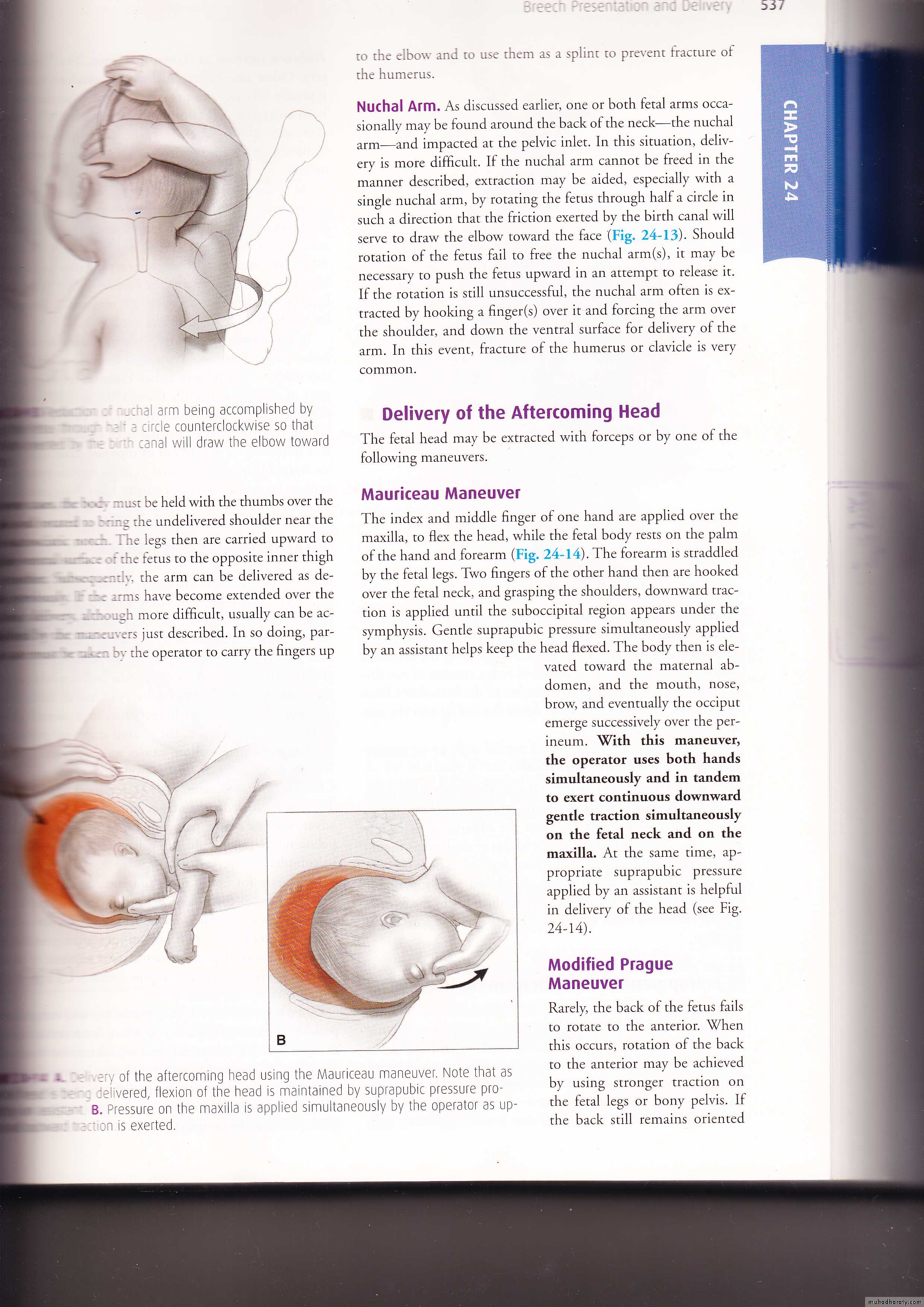
Delivery of the head
The head is delivered using the Mauriceau–Smellie–Veit manoeuvre: the baby lies on the obstetrician’s arm with downward traction being levelled on the head via a finger in the mouth and one on each maxilla
Delivery occurs with first downward and then upward movement (as with instrumental deliveries). If this manoeuvre proves diffi cult, forceps need to be applied.
An assistant holds the baby’s body aloft while the forceps are applied in the usual manner

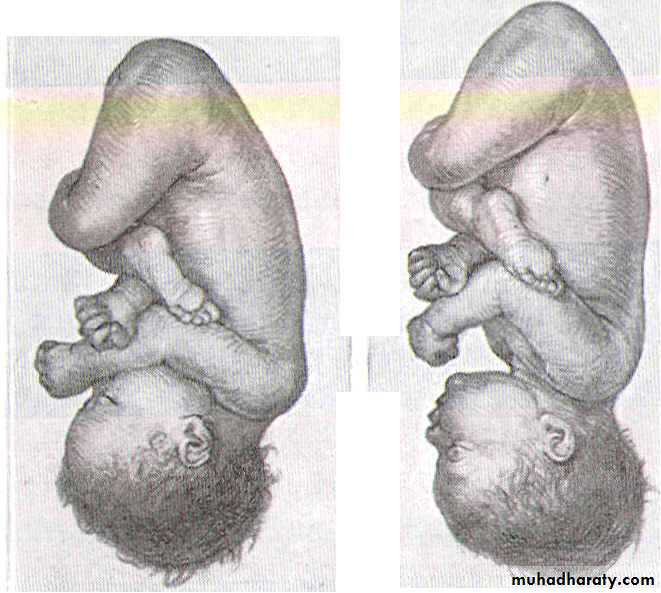
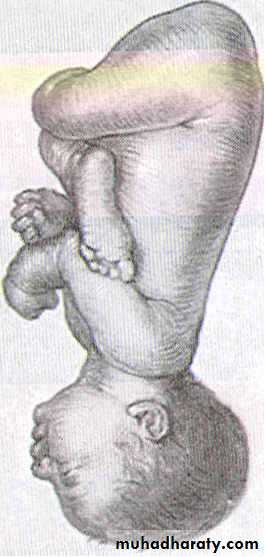
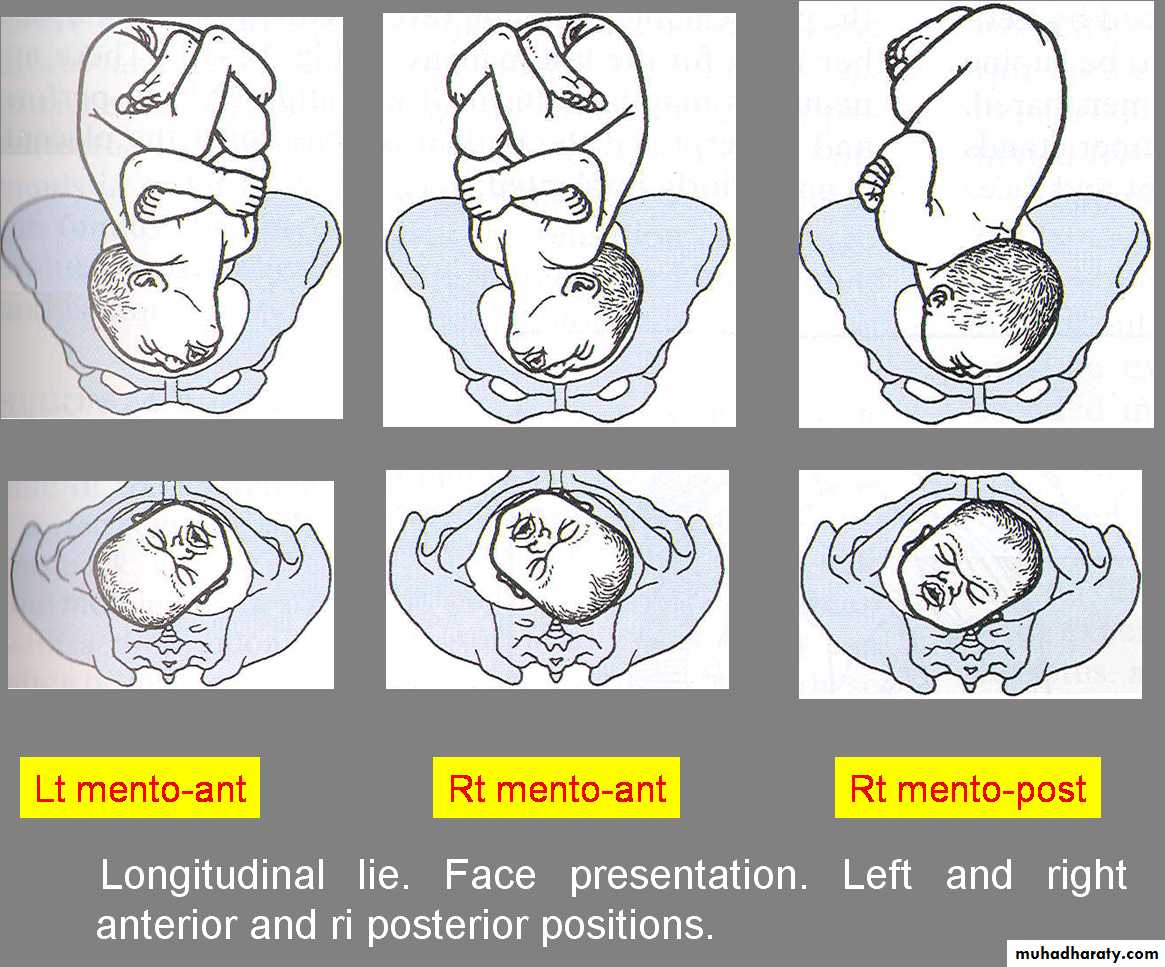
Face presentation
• Incidence 1/500.• Aetiology
• 1-the head is normal &extended which continue even after labour for few days.
• 2-prematurity was associated between 25% &34% of cases & most women was multiparous.
• 3-Multiple pregnancy.
•
•

• .'" '
• I• ! 1\
• 11
• A
• B
• ii
• F
• c
• D
• Longitudinal lie. Cephalic presentation. Differences in attitude of fetal body,
• Note changes in fetal attitude in relation to fetal vertex as the fetal head becomes less flexed.
(A) vertex
(B) sinciput
(C) brow
(D) face
• 4-presence of multiple loops of the cord around the neck.
• 5-anencephaly
• 6-congenital tumours of the neck, thyroid goitres.
• 7-musculoskeletal abnormalities
• 8- uterine abnormalities such as pelvic tumours, bicornuate uterus, placenta previa &polyhydramnio
Diagnosis
Abdominal examinationWith mentoposterior position the cephalic prominence is felt on the same side as the back from which is separated by deep sulcus &it may be difficult to hear fetal heart
In mentoanterior position ,in addition ,the fetal heart is easily heard over the chest &the small parts may be felt on the same side.
Vaginal examination As the face fits less well than the vertex ,the membranes may rupture early .When the face engaged ,supra-orbital ridges ,bridge of nose &the alveolar margins within mouth are recognized. If the face is oedematous it can be mistaken for the breech.
Mechanism of labour
The chin is the denominator; mentoanterior position (77% of cases) is more common than mentoposterior.In mentoanterior position the head engages& descends with increasing extension, so that the submentobregmatic diameter of 9.5cm comes through the cervix.
mechanism of labor
When the chin reaches the pelvic floor it undergoes internal rotation through one-eighth of a circle& the submental region comes to lie under the subpubic arch.
The head is then born by flexion Restitution occur& followed by external rotation as in vertex presentation.
In mentoposterior the chin undergo internal rotation through 3 eighth of the circle and deliver as mentoanterior.
Persistant mentoposterior position or mentotransverse position occur only in 10% of face presentation ,in these cases the baby can not be delivered vaginally unless is very small or macerated because the head is already fully extended so further extension to deliver the head is impossible.
Management of labour
• The patient is kept in bed in the first stage &vaginal examination is made as soon as the membranes ruptures to exclude cord prolapse. An epidural block or infiltration of perineum with local anesthesia, episiotomy is advisable. With a mentoanterior position spontaneous delivery is to be expected• If second stage delayed,sustaine efficient uterine contraction ;forceps delivary& episiotomy can be used if needed.
With mentoposterior position time should be allowed for spontaneous rotation which usually occur in the second stage. If not occur manual rotation with epidural block or general anesthesia may be tried &its failure indicate c/s.
• Caesarian Section indicated in face presentation if:
• failure of presenting part to descend• cord prolapse in first stage
• fetal distress in first stage
• prolonged first stage
• persistent mentoposterior position
Brow presentation
Incidence 1 in 1500the head is partially extended&present to the cervix with its largest diameter mento-vertical;13 cm
BROW PRESENTATION
Incidence 1 in 2000
The head is halfe extended &present to the cervix with its largest diameter, mentovertical-13cm.
Diagnosis;-abdomially,when the head above pelvic brim& cephalic prominence is in the same side with fetal back.By vaginal examination,the forhead i palpable but is termed as brow because the orbital ridges&bridge of the nose defind.Anterior fontanell also felt.
ManagementVaginal delivary
If the head is partially extended in early labour &there is no evidence of severe disproportion a short trial of labour is permitted which may result in further extension of the head to face presentation& engagement with following normal delivery.If there is evidence of disproportion &brow is above the pelvic brim & the head fail to engage,
caesarian section is indicated