
Growth and Development of
Cranio – Mandibular Structures

Growth
• According to KROGMAN , growth is an
“Increase in size, change in proportion and
progressive complexity”
• According to MOYER`S “Quantitative aspect of
biologic development per unit time”

THEORIES OF GROWTH CONTROL
THEORIES OF GROWTH CONTROL
• It is a truism that growth is strongly influenced
by genetic factors, but it also can be
significantly affected by the environment, in
the form of nutritional status, degree of
physical activity, health or illness, and a
number of similar factors.

Exactly what determines the growth of the jaws, however,
remains unclear and continues to be the subject of
intensive research.
Three major theories in recent years have attempted to
explain the determinants of craniofacial growth:
(1) bone, like other tissues, is the primary determinant of
its own growth;
(2) cartilage is the primary determinant of skeletal
growth, while bone responds secondarily and passively;
(3) the soft tissue matrix in which the skeletal elements are
embedded is the primary determinant of growth, and both
bone and cartilage are secondary followers.

• The major difference in the theories is the
location at which genetic control is expressed.
• The first theory implies that genetic control is
expressed directly at the level of the bone,
and therefore its locus should be the
periosteum

• The second, or cartilage, theory suggests that
genetic control is expressed in the cartilage,
while bone responds passively to being
displaced. This indirect genetic control is
called epigenetic.

• The third theory assumes that genetic control
is mediated to a large extent outside the
skeletal system and that growth of both bone
and cartilage is controlled epigenetically,
occurring only in response to a signal from
other tissues.

Sutural Dominance Theory (Sicher)
Sutural Dominance Theory (Sicher)
• Sicher introduced that sutures were causing
most of growth
• Primary event in sutural growth connective
tissue proliferation between the two bones.
• This creates the space for oppositional growth
at the borders of the two bones.

• The connective tissue in sutures of both the
nasomaxilary complex and vault produced
forces which separated the bones.
• The theory held sutures, cartilage and
periosteum all responsible for facial growth
and assumed all were under tight intrinsic
genetic control.

• Shortcomings of Sutural theory It is clear now
that sutures are not primary determinants of
growth. Two evidences in support are:
1)Sutures & periosteal tissues lack innate
growth potential,proved by transplanting a
suture
2)Growth at sutures responds to outside
influences,as compression and tension.

• For eg. If cranial or facial bones are pulled
apart at sutures, new bone fills in and if suture
is compressed the growth will be impeded.
Sutures are thus areas that react-not primary
determinants. Thus sutures are growth sites,
not growth centres.

• Growth Center: Those areas of craniofacial
skeleton that have: tissue seperating
capabiltiesand innate growth potential not
influenced by external factors
e.g.Synchondrosis and nasal septal cartilage.

• Growth Site: Locations at which active skeletal
growth occur but as a secondary
,compensatory effect lacking direct genetic
influence effected by external influences. e.g.
sutures and periosteum.

Scott’s Hypothesis
Scott’s Hypothesis
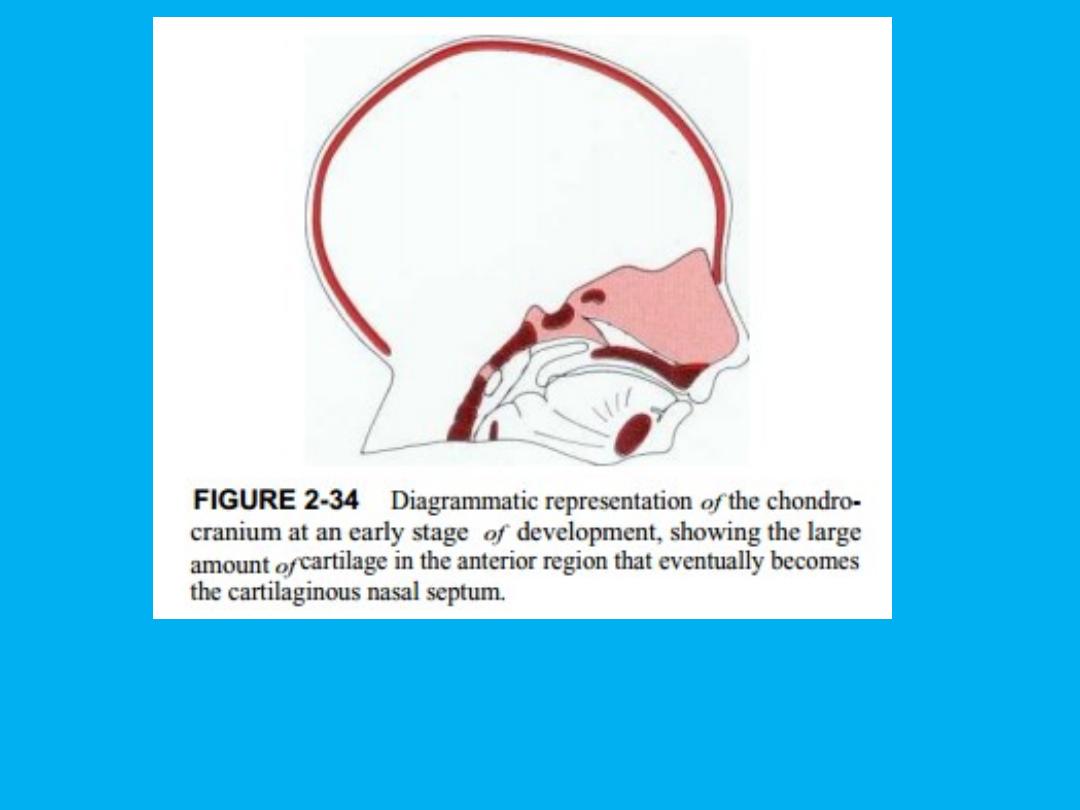
• Held that cartilaginous portions of head, nasal
capsule, mandible and cranial base dominate
facial growth.
• Specifically emphasized how the cartilage of
nasal septum paced the growth of maxilla.
• Sutural growth came in response to growth of
other str. including cartilaginous structures
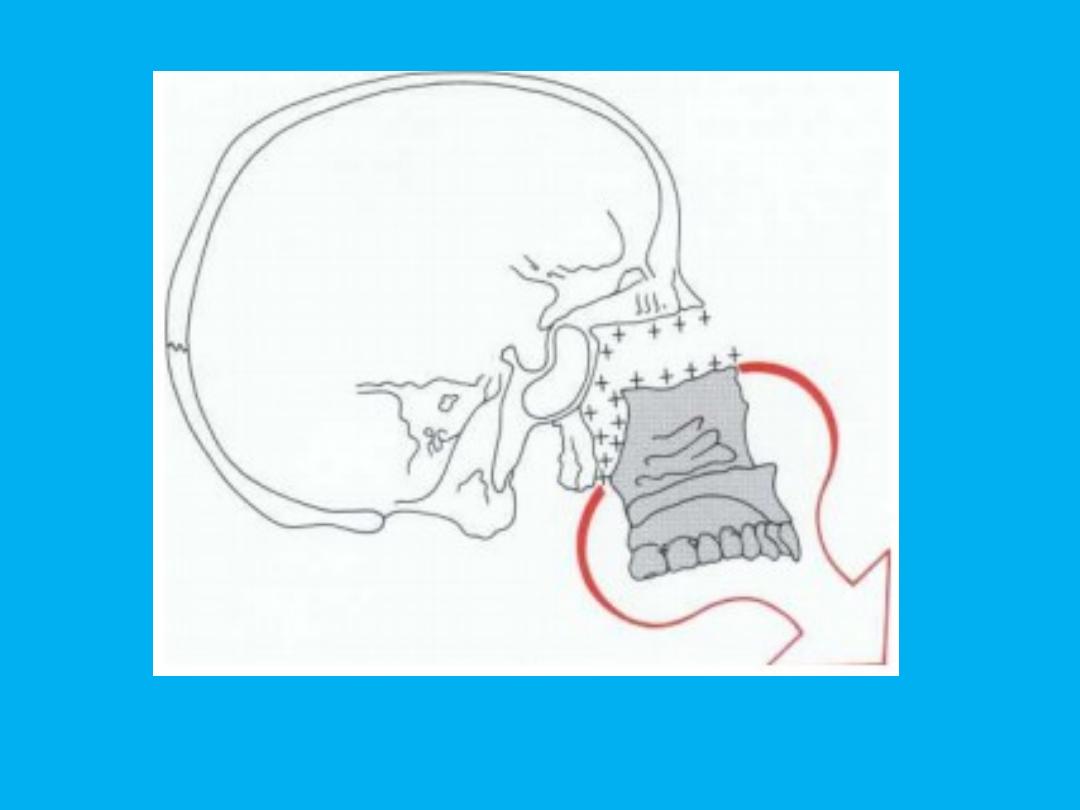
Growth at nasal septum causes downward & forward translation of maxilla

• Growth of maxilla on basis of Scott’s theory
nasomaxillary complex grows as unit that
cartilaginous nasal septum serves as a
pacemaker for maxillary growth
• cartilage growth leads to forward and
downward translation of maxilla. sutures
which serve as reactive areas respond by new
bone formation leading to growth.

Experiments to verify Scott’s
Experiments to verify Scott’s
• theory Two kinds of experiments carried out
to test the theory:
1. Transplantation experiments
2. Removal of cartilage.
In transplantation experiments not all skeletal
cartilage act same when transplanted

• Epiphyseal plate of long bone continued to
grow in new location. Spheno-occipital
synchondrosis also grows when transplanted,
but not as well. Nasal septal cartilage found to
grow nearly as well as others. No growth
found when mandibular condyle transplanted.

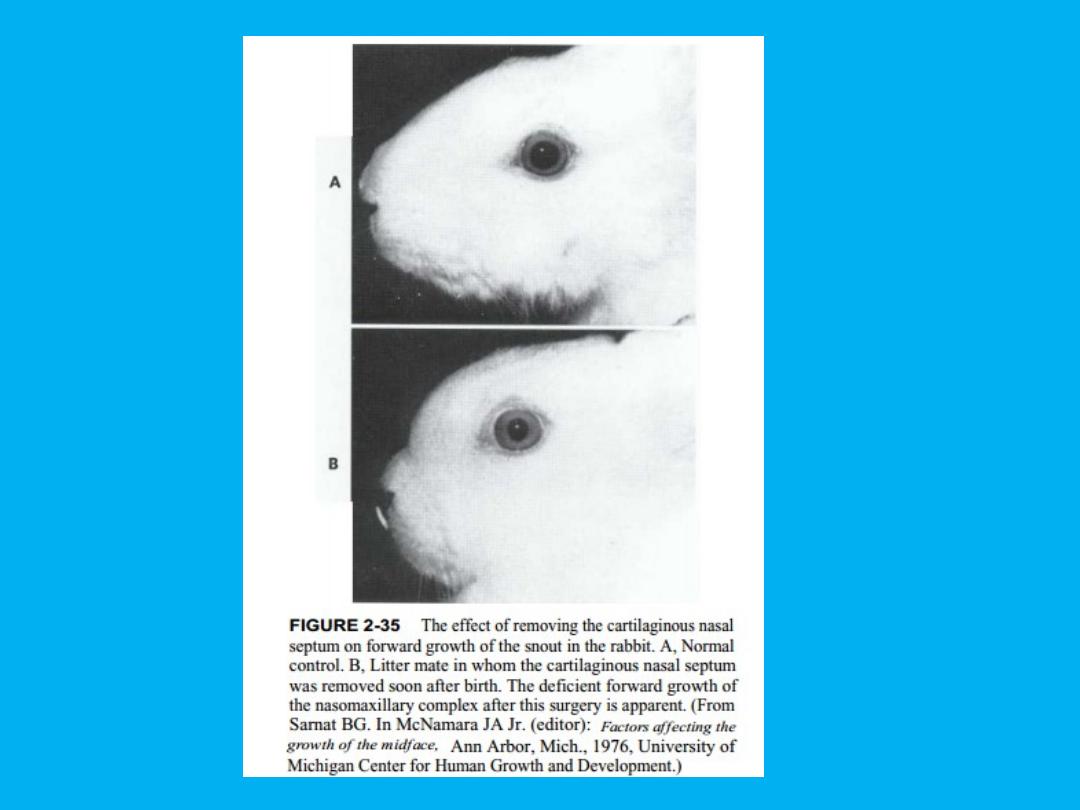
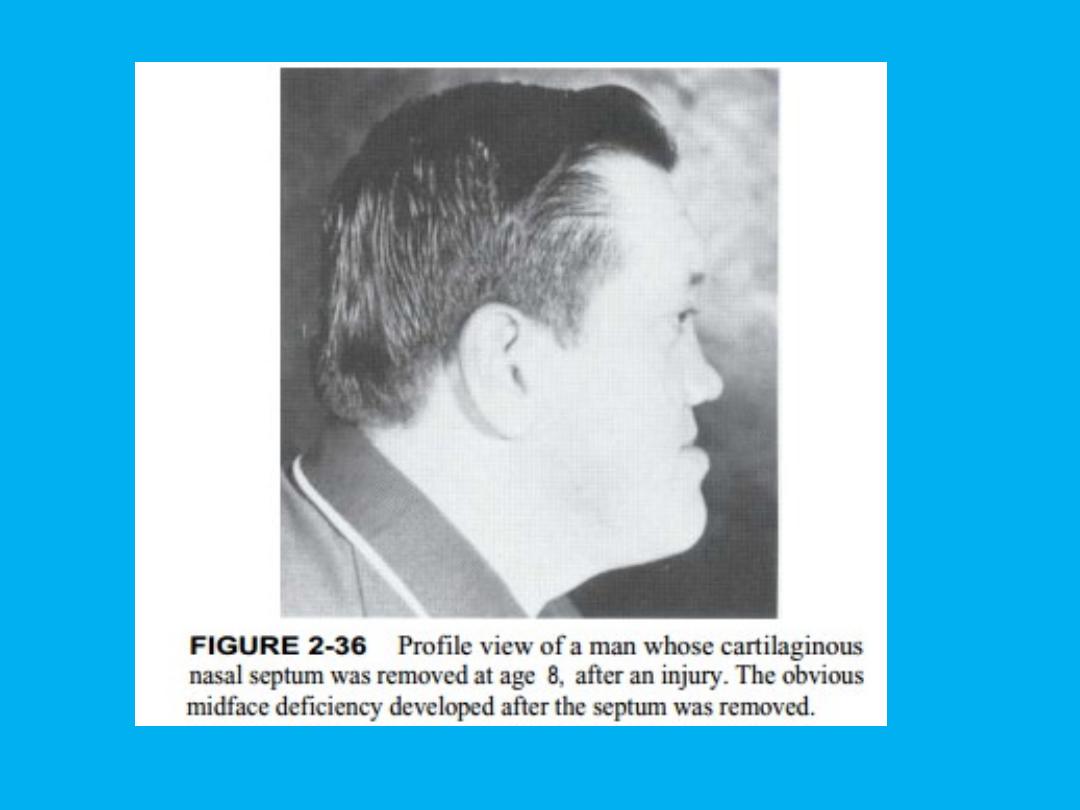
• In cartilage removal experiments, Extirpating a
young rabbits septum causes a considerable
deficit in growth of midface.
• Gilhuus- Moe and Lund demonstrated that
after fracture of condyle in a child there was
an excellent chance that it would regenerate
to app. Its original size

Shortcomings of Scott’s Theory
Shortcomings of Scott’s Theory
• Transplantation experiments have revealed
that condyle has no innate growth potential.
• It is a growth site and not a growth center
• Influenced by local factors
• growth at condyle is entirely reactive

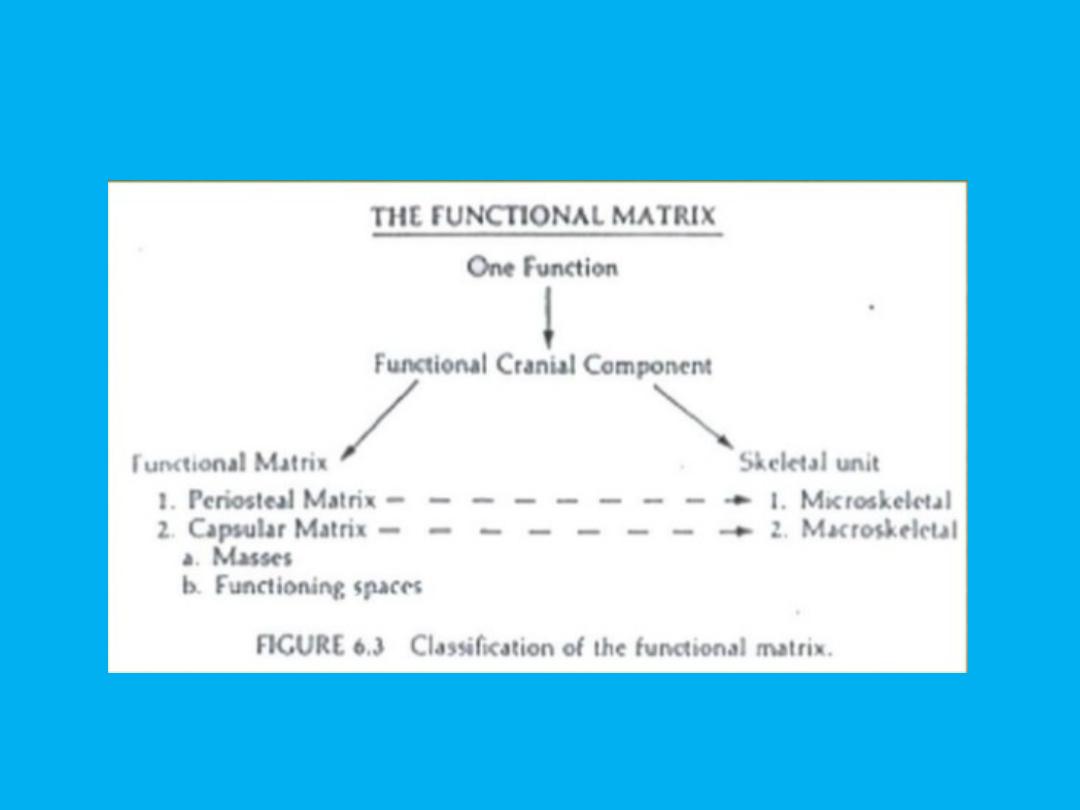
FUNCTIONAL MATRIX HYPOTHESIS (Melvin
Moss)
FUNCTIONAL MATRIX HYPOTHESIS (Melvin
Moss)
• In this conceptual view, the soft tissues grow, and
both bone and cartilage react.
• The growth of the cranium illustrates this view of
skeletal growth very well. There can be little
question that the growth of the cranial vault is a
direct response to the growth of the brain. Pressure
exerted by the growing brain separates the cranial
bones at the sutures, and new bone passively fills in
at these sites so that the brain case fits the brain.

• Another excellent example is the relationship
between the size of the eye and the size of the
orbit. An enlarged eye or small eye will cause
a corresponding change in the size of the
orbital cavity. In this instance, the eye is the
functional matrix.
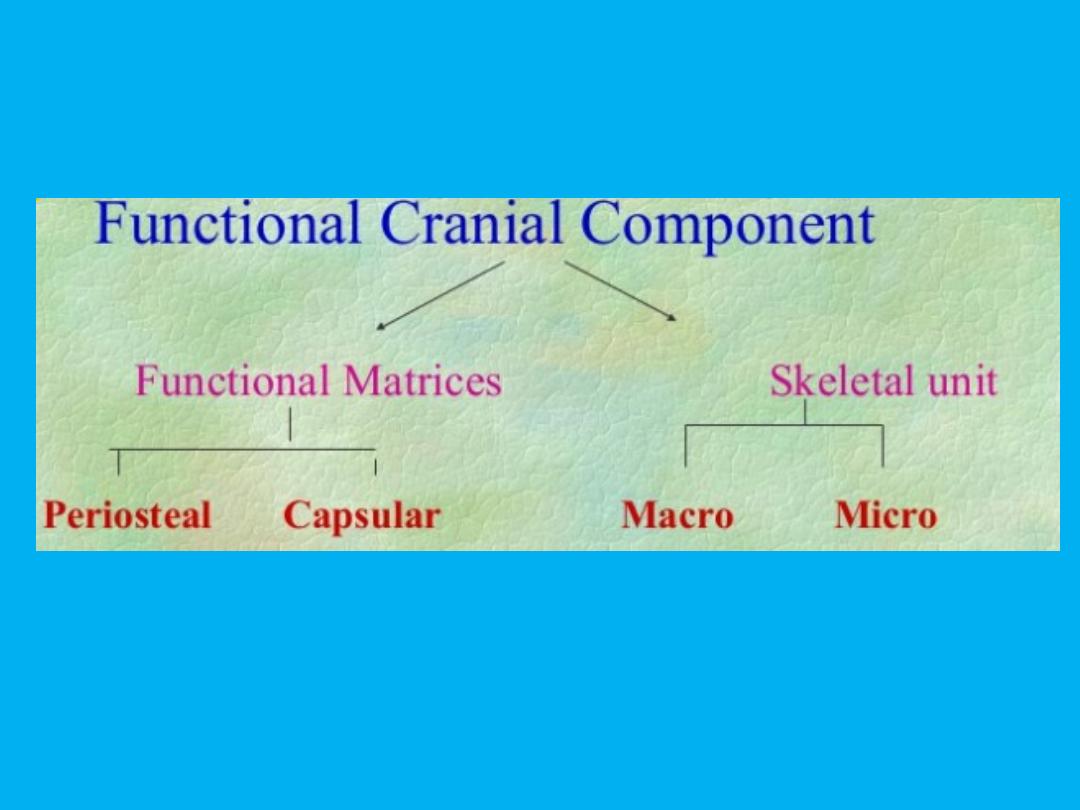

• FUNCTIONAL MATRIX : all soft tissues and
spaces that perform a given function
• SKELETAL UNIT: bony structures that support
the functional matrix and are necessary for
that function

FUNCTIONAL MATRICES
FUNCTIONAL MATRICES
1- Periosteal Matrix
Relates the matrix to those tissues that influence the bone
directly through the periosteum Muscles Blood vessels and
nerves lying in grooves or entering or exiting through
foramina Affects a microskeletal unit, the influence is usually
limited to a part of one bone.
All responses of skeletal units
to periosteal matrices brought about by complementary and
inter related processes of osseous depositon and
resorption .They act by bringing transformation of the related
skeletal units
e.g. Temporalis – coronoid process
Tooth - alveolar bone

2- Capsular Matrix
• Included in this matrix are those masses and spaces
that are surrounded by capsules. Neural mass with
scalp and dura. Orbital mass with supporting tissues
of the eyes. Capsules tend to influence
macroskeletal units which means portions of several
bones are simultaneously affected Inner surface of
calvarium. This sharing of reaction by several
adjacent bones constitutes a macroskeletal unit.

• Expansion of the brain i.e closed capsular matrix
volume is primary event in expansion of the capsule.
The volumetric increase causes compensatory
expansion of surrounding capsule which is brought
about by mitotic activity.
• Later the calvarial functional cranial component as a
whole are passively and secondarily translated .Such
translations occur without necessity of involving the
processes of selective periosteal apposition and
resorption

• Moss theorizes that the major determinant of growth of
the maxilla and mandible is the enlargement of the nasal
and oral cavities, which grow in response to functional
needs. The theory does not make it clear how functional
needs are transmitted to the tissues around the mouth
and nose, but it does predict that the cartilages of the
nasal septum and mandibular condyles are not important
determinants of growth and that their loss would have
little effect on growth if proper function could be
obtained. From the view of this theory, however, absence
of normal function would have wide-ranging effects.

• We have already noted that in 75% to 80% of
human children who suffer a condylar
fracture, the resulting loss of the condyle does
not impede mandibular growth. The condyle
regenerates very nicely. What about the 20%
to 25% of children in whom a growth deficit
occurs after condylar fracture?19 Could some
interference with function be the reason for
the growth deficiency?

Mechanism Of Bone Growth
Mechanism Of Bone Growth
Mechanisms Of Bone Growth are:
- Remodeling
-Cortical drift
-Displacement

REMODELING
REMODELING
• BONE DEPOSITION & RESORPTION:
• Bone changes in shape & size by two basic
mechanisms,bone deposition & bone resorption. The bone
deposition & resorption together is called “ BONE
REMODELING”.The changes that bone deposition &
resorption can produce are:
• Change in size
• Change in shape
• Change in proportion
• Change in relationship of the bone with adjacent structures.

Cortical Drift
Cortical Drift
• Most bones grow by interplay of bone deposition &
resorption .A combination of bone deposition &
resorption resulting in a growth movement towards
the deposition surface is called “Cortical Drift”.
• If bone deposition & resorption on either side of a
bone are equal, the thickness of the bone remains
constant.
• If in case more bone is deposited on one side & less
bone resorbed on the opposite side The thickness of
the bone increases.
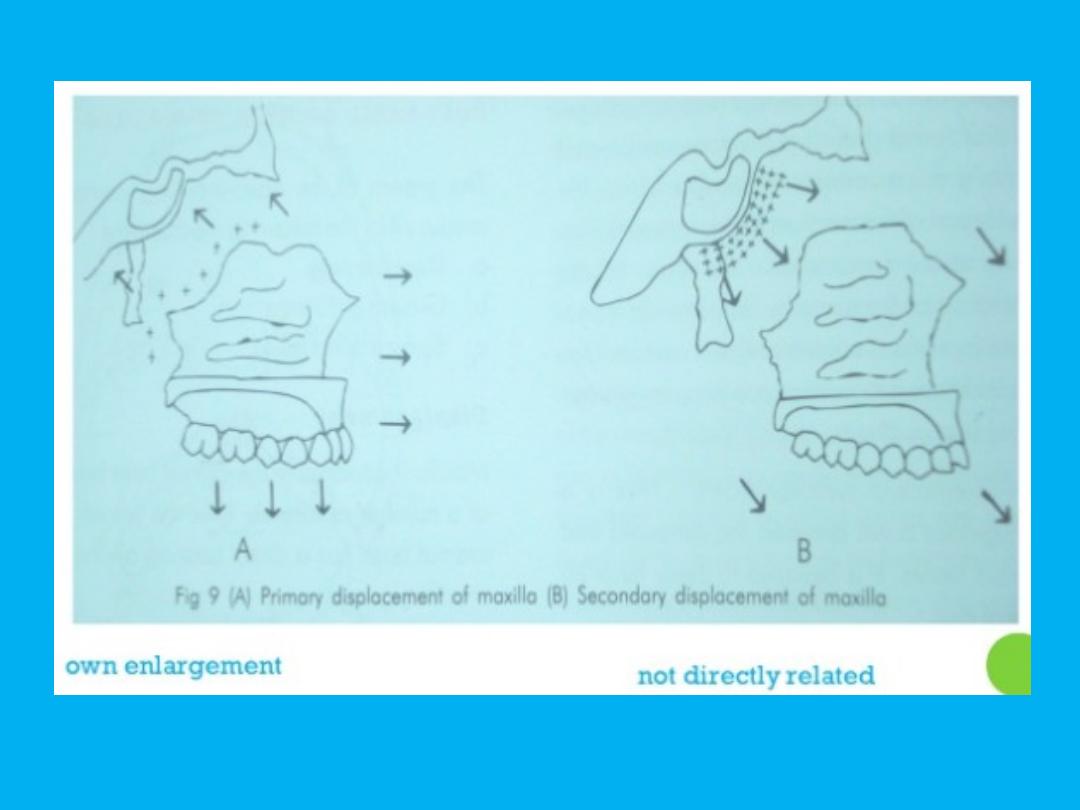
Displacement
Displacement
• Displacement: Growth which causes the mass
of a bone to be moved relative to its
neighbours. Displacement can be of two types.
• Primary displacement: If a bone gets displaced
as a result of its own growth, it is called
“Primary displacement”. e.g.. Growth of the
maxilla at the tuberosity region results in
pushing of the maxilla against the cranial base
in a forward & downward direction.
Displacement
Displacement
• Secondary displacement: If the bone gets
displaced as a result of growth &enlargement
of an adjacent bone, it is called “Secondary
displacement.”e.g.. The growth of the cranial
base causes the forward &downward
displacement of the maxilla

Characteristics of Bone Growth
Characteristics of Bone Growth
• Bone formation occurs by 2 methods of
differentiation of mesenchymal tissues.
Accordingly 2 types of bone growth is normally
seen.
• 1) Intra-membranous ossification : The
transformation of mesenchymal connective
tissue usually in membranous sheets, into
osseous tissues. E.g. Cranial vault, face (Mx &
body of Md) and the clavicles

2. Endochondral ossification: The conversion of
hyaline cartilage into bone. E.g. Cranial base,
condyle and Epiphyseal plate Proliferating
cartilage.
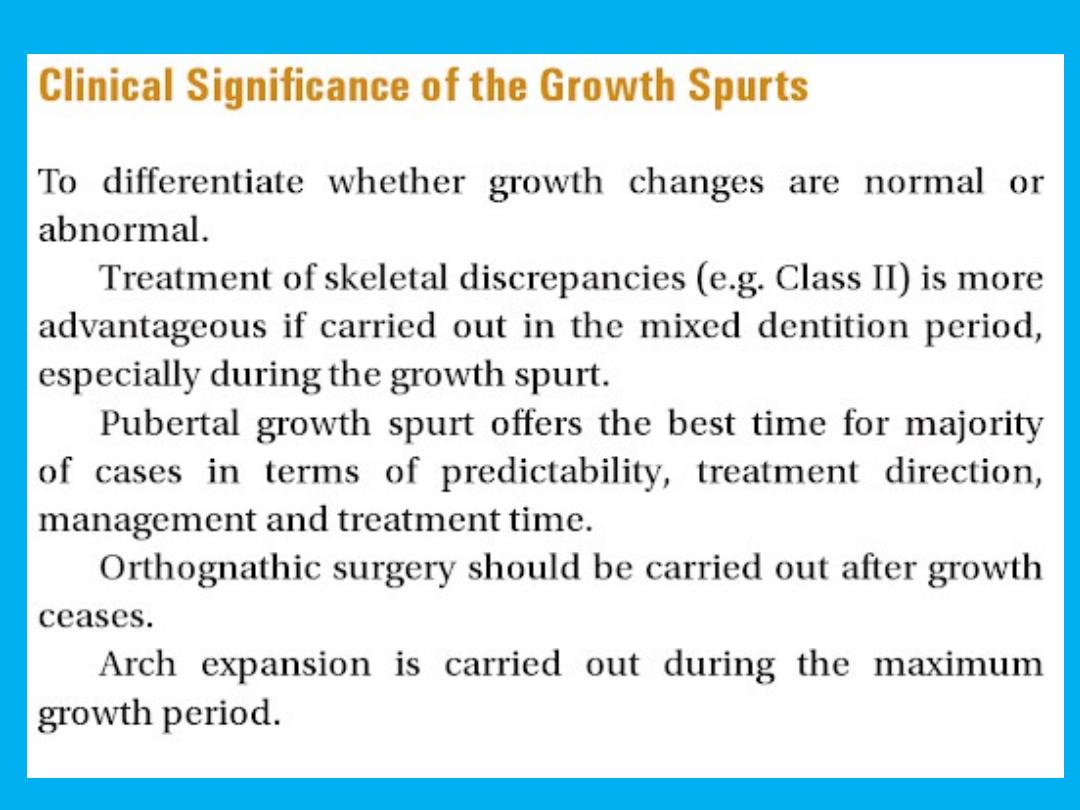
Growth Spurts
Growth Spurts
• Growth doesn’t take place uniformly at all
times. There seem periods when a sudden
acceleration of growth occurs. This sudden
increase in growth is called growth spurt.
• The physiologic alteration in hormonal
screation is believed to be the cause for such
accentuated growth. The timing of growth
spurt differs in boys and girls.

• The following are the timings of growth spurt
a. Just before the birth
b. 1 year after the birth
c. Mixed dentition growth spurt
Boys 8- 11
Girls 7-9
d. Pubertal growth spurt
Boys 14-16
Girls 11-13

• Growth modification by the means of
functional and orthodontic appliances elicit
better response during growth spurt . surgical
corrections of maxilla and mandible should be
carried out only after cessation of growth
spurt
Growth patterns
Growth patterns
• In studies of growth and development, the concept of
pattern is an important one.Pattern in growth also
represents proportionality, but in a still more complex
way, because it refers not just to a set of proportional
relationships at a point in time, but to the change in
these proportional relationships over time. In other
words, the physical arrangement of the body at any one
time is a pattern of spatially proportioned parts. But
there is a higher level pattern, the pattern of growth,
which refers to the changes in these spatial proportions
over time.

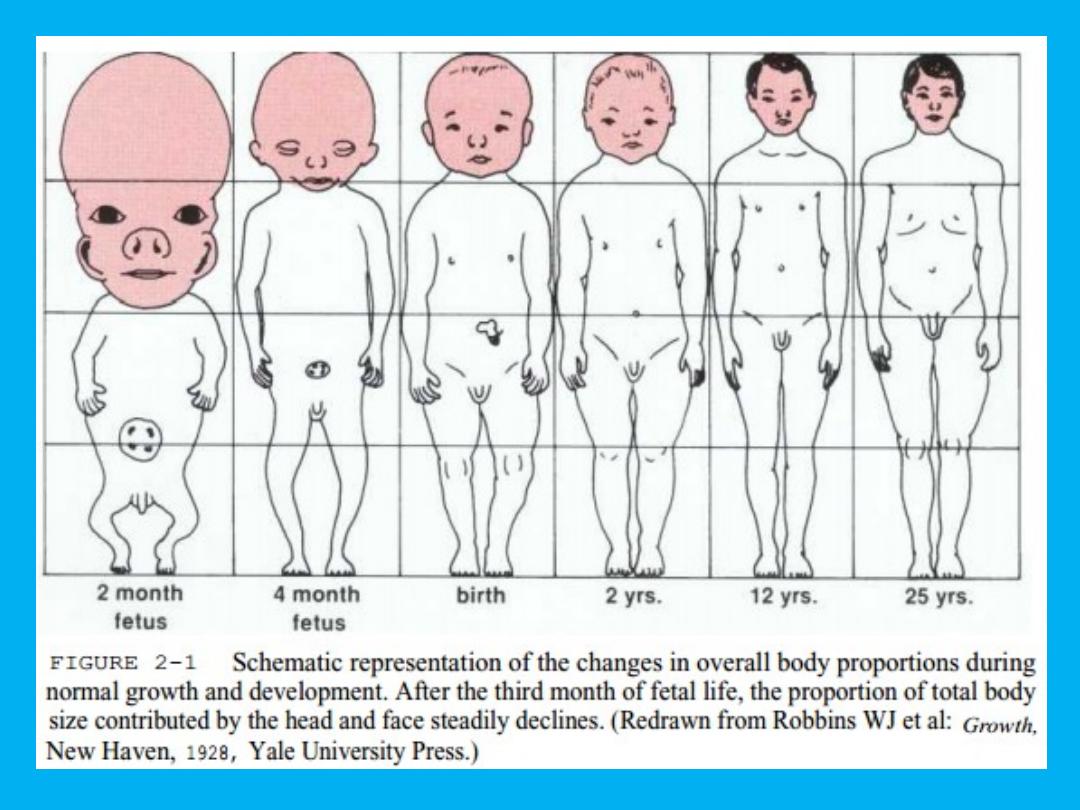
• In fetal life, at about the third month of intrauterine
development, the head takes up almost 50% of the total
body length. At this stage, the cranium is large relative to
the face and represents more than half the total head. In
contrast, the limbs are still rudimentary and the trunk is
underdeveloped. By the time of birth, the trunk and limbs
have grown faster than the head and face, so that the
proportion of the entire body devoted to the head has
decreased to about 30%. The overall pattern of growth
thereafter follows this course, with a progressive reduction
of the relative size of the head to about 12 % of the adult.

• At birth the legs represent about one third of the
total body length, while in the adult they represent
about half. As Figure 2-1illustrates, there is more
growth of the lower limbs than the upper limbs
during postnatal life. All of these changes, which
are a part of the normal growth pattern, reflect
the "cephalocaudal gradient of growth." This
simply means that there is an axis of increased
growth extending from the head toward the feet.

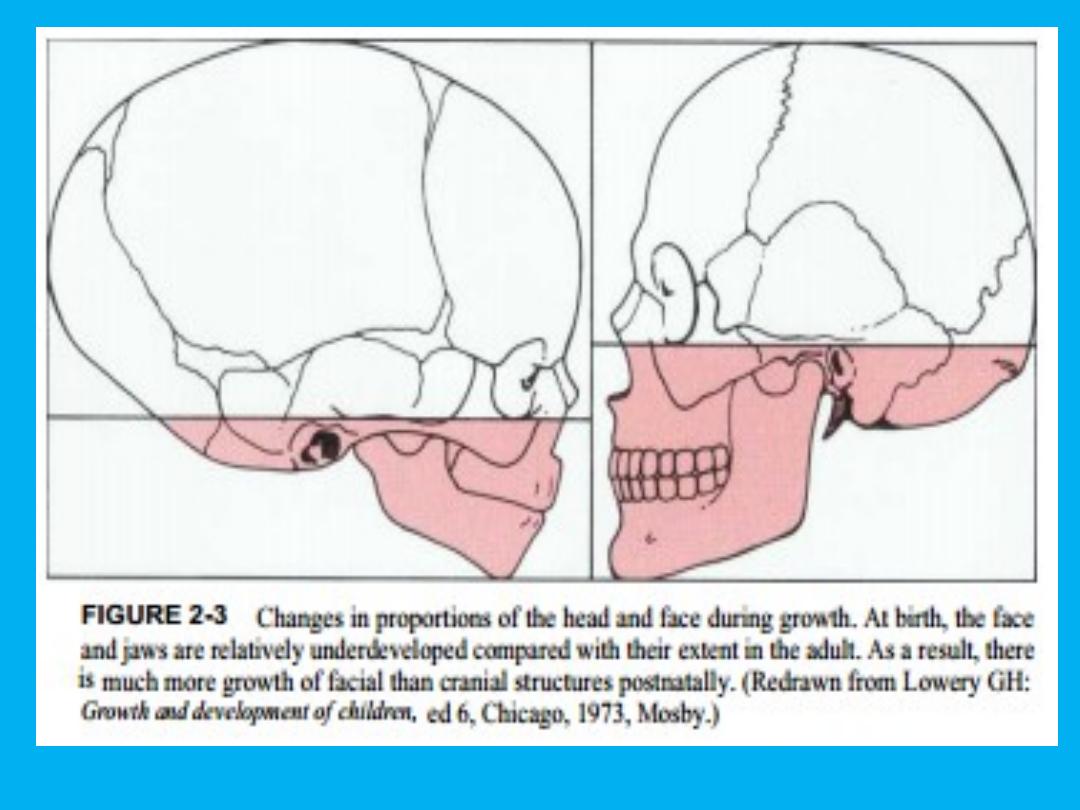
• Even within the head and face, the cephalocaudal growth
gradient strongly affects proportions and leads to changes in
proportion with growth (Figure 2-3). When the skull of a
newborn infant is compared proportionally with that of an adult,
it is easy to see that the infant has a relatively much larger
cranium and a much smaller face. This change in proportionality,
with an emphasis on growth of the face relative to the cranium,
is an important aspect of the pattern of facial growth. When the
facial growth pattern is viewed against the perspective of the
cephalocaudal gradient, it is not surprising that the mandible,
being further away from the brain, tends to grow more and later
than the maxilla, which is closer.
Growth patterns
Growth patterns
• Different tissues have different growth
patterns (curves) in terms of rate and timing,
and four main types are recognized: neural,
somatic, genital, and lymphoid. The first two
are the most relevant in terms of craniofacial
growth.

Neural grow
• this essentially that which is determined by
growth of the brain, with the calvarium
following this pattern. There is rapid growth in
the early years of life, but this slows until by
about the age of 7 years growth is almost
complete. The orbits also follow a neural
growth pattern.

Somatic growth
• Is that which is followed by most structures. It is seen in the long
bones, amongst others, and is the pattern followed by increase in
body height. Growth is fairly rapid in the early years, but slows in
the prepubertal period. The pubertal growth spurt is a time of very
rapid growth, which is followed by further slower growth.
• Traditionally, the pubertal growth spurt has been reported to occur
on average at 12 years in girls, but there is evidence that the age
of
puberty is decreasing in girls. In boys the age of puberty is later at
about 14 years.

• The maxilla and mandible follow a pattern of
growth that is intermediate between neural
and somatic growth, with the mandible
following the somatic growth curve more
closely than the maxilla, which has a more
neural growth pattern

• Thus different parts of the skull follow
different growth patterns, with much of the
growth of the face occurring later than the
growth of the cranial vault. As a result the
proportions of the face to the cranium change
during growth, and the face of the child
represents a much smaller proportion of the
skull than the face of the adult.