Infection of the Fascial spaces
1Infection of the Fascial spaces
Fascial spaces: are potential spaces, they are surrounded by muscles, loose C.T. and bone, they contain anatomical structures and they are separated by collection of pus, blood or by surgeon's finger. They are contiguous and infection spreads readily from one space to another..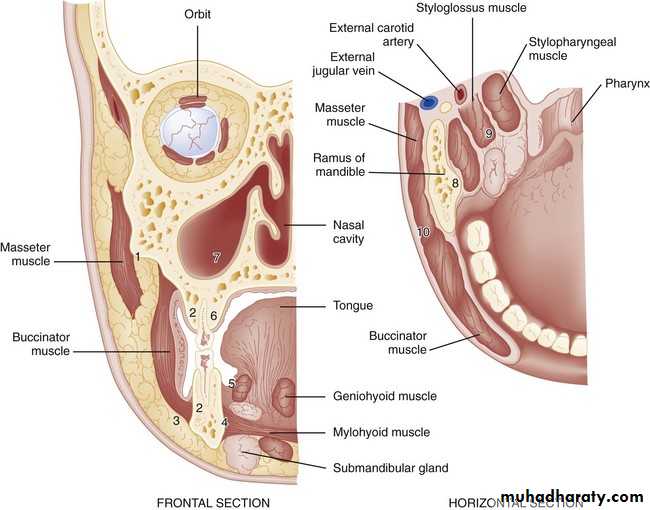
Fascial spaces are sometimes classified as primary which are directly adjacent to the origin of the odontogenic infections, and secondary; that become involved following the spread of infection to the primary spaces.

Infection of spaces in relation to the lower jaw
1. Submental space infectionAnatomic boundaries this space lies between the Mylohyoid muscle above, skin, subcutaneous tissue, Platysma muscle and deep cervical fascia below, laterally by lower border of the mandible and anterior bellies of Digastric muscle. It contains submental lymph nodes embedded in adipose tissues.
Source of infection : a direct source is from infected lower incisors and canines, lower lip, skin overlying the chin or from the tip of the tongue and the anterior part of the floor of the mouth. An indirect source of infection is from submandibular spaces. The site of the swelling is mostly extraoral including the chin and submental areas which are firmly swollen.

The site of incision and drainage is extraoral horizontal incision through the skin posterior to the crease behind the chin, providing dependent drainage and most esthetically acceptable scar. It may be drained intraorally through the Mentalis muscle via the labial vestibule, but the dependent drainage can’t be established.

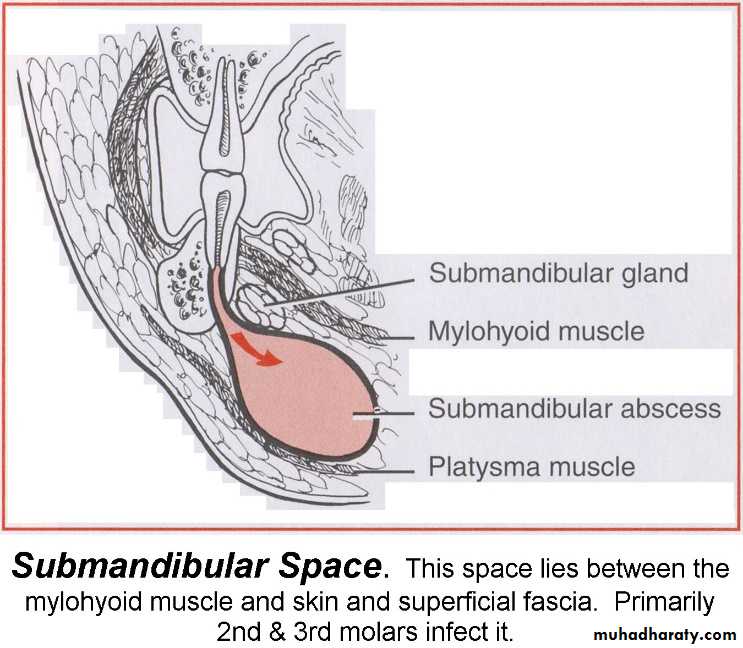
2. Submandibular space infection
Anatomic boundaries: it is bounded by Mylohyoid muscle superiorly, anterior and posterior bellies of Digastric muscle inferiorly, Mylohyoid, Hyoglossus and Styloglossus muscles medially, laterally the space is bounded by the skin, superficial fascia, Platysma, deep fascia and the lower border of the mandible.This space contains the submandibular salivary gland and lymph nodes in addition to facial artery and vein, lingual and Hypoglossal nerve as they course deep to the submandibular salivary gland.
Source of infection is from the lower molar teeth especially second and third molars, as the infection perforates the lingual cortex of the mandible below the Mylohyoid muscle attachment.

Infection can also spread from the tongue, posterior part of the floor of the mouth, upper posterior teeth, cheek, palate, the maxillary sinus and the submandibular salivary gland. Indirectly the infection may spread from infected sublingual and submental spaces. Submandibular space infections can spread posteriorly to the pharyngeal space.
Submandibular space infection presents as a firm or fluctuant erythematous swelling of the submandibular region, the swelling bulges over and obliterates the inferior border of the mandible, there may be trismus, other signs and symptoms of infection may or may not be present.
Site of incision and drainage it is extraoral incision made parallel and about 2 cm. below the inferior border of the mandible to avoid injury to the marginal mandibular branch of the facial nerve, the incision extends through the skin and subcutaneous tissue only while the space is entered bluntly to avoid structures within the space

3. Sublingual space infection
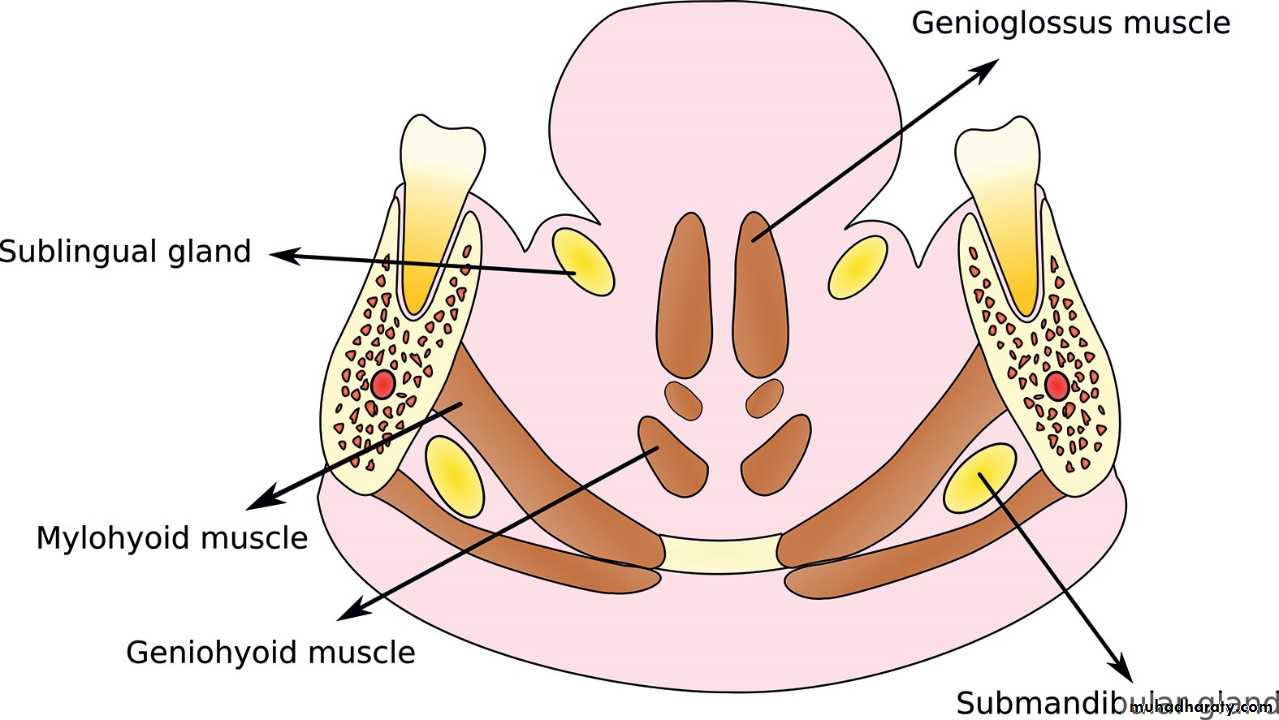
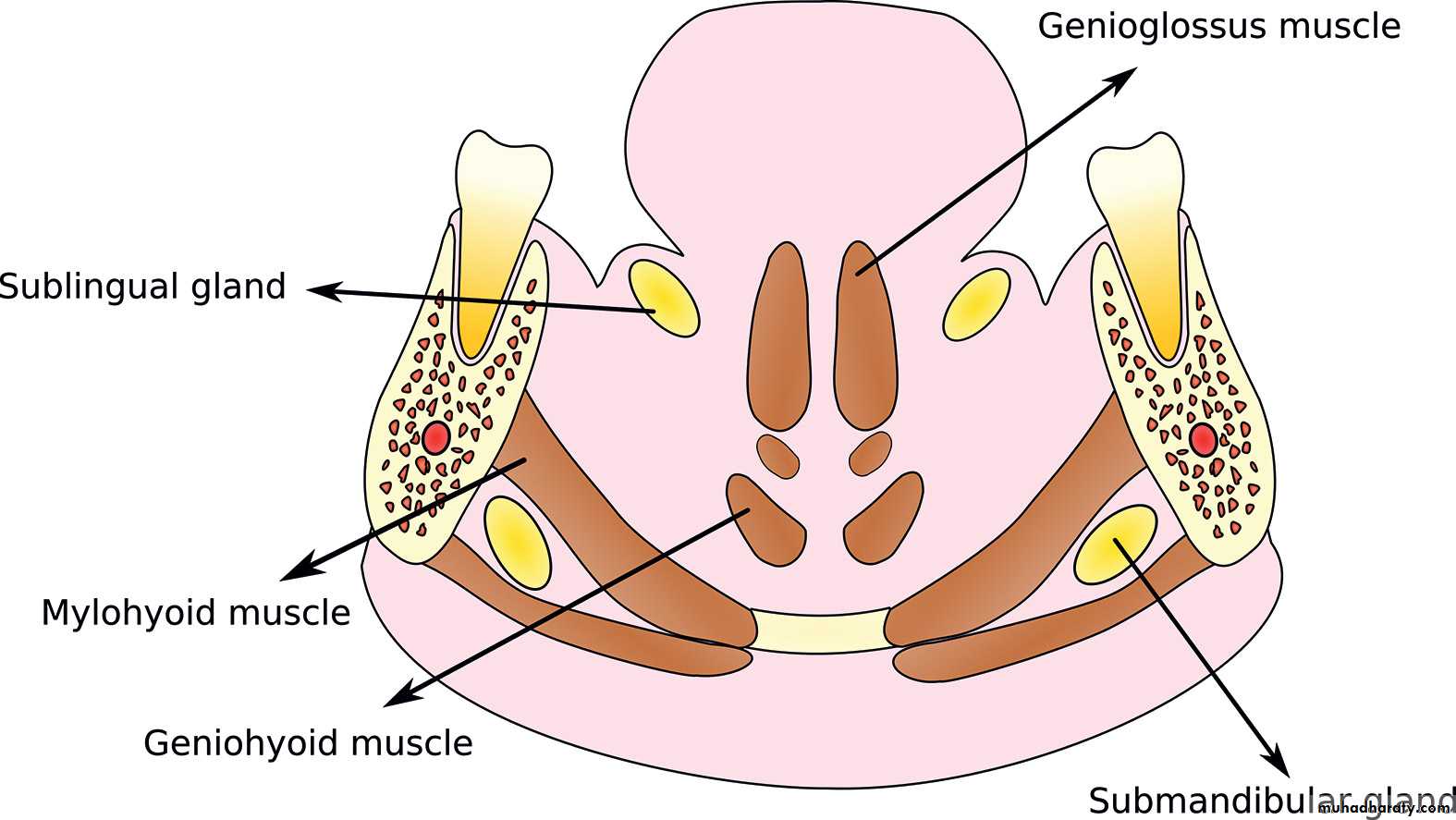
Anatomic boundaries: this is a V-shaped space, it is bounded anteriorly and laterally by the mandible, superiorly by sublingual mucosa, inferiorly by the Mylohyoid muscle and medially by Genioglossus, Geniohyoid and Styloglossus muscles.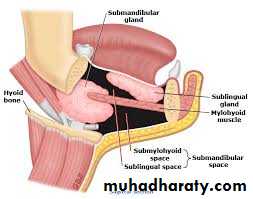
Source of infection it is usually from the premolar and less commonly from molar teeth when the infection perforates the lingual cortex of the mandible above the attachment of the Mylohyoid muscle.
Indirectly the infection may spread from submental and submandibular spaces. Infection from sublingual space may invade the submandibular and pharyngeal spaces.
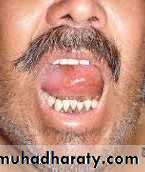
Clinically : there is erythematous swelling of the floor of the mouth that may extend through the midline since the barrier between the two sublingual spaces is weak, usually there is elevation of the tongue.

Site of incision and drainage: intraorally by an incision through the mucosa only parallel to Wharton's duct and lingual cortex in anteroposterior direction and away from the sublingual fold.
This space may be drained extraorally through submandibular and submental incisions through the Mylohyoid muscle if the infection of these latter spaces is also evident.

Ludwig's Angina
is a massive firm cellulitis affecting simultaneously the subrnandibular submental and sublingual spaces bilaterally. It is a very serious condition that require prompt treatment.

Causes :
• Dental infections in 90% of the cases.• Submandibular salivary gland infections.
• Mandibulr fractures.
• Soft tissue lacerations and wounds of the floor of the mouth.
The term angina is related to the sensation of suffocation. If untreated this condition is almost fatal mainly due to posterior extension of the infection into the epiglottis causing epiglotic edema and respiratory obstruction.
Signs and Symptoms:
There is a firm extensive bilateral submandibular swelling, intraorally there is swelling of the floor of the mouth that raises the tongue which may protrude from the mouth in extreme cases. The patient is toxic, feverish and there is dyspnea and difficulty in swallowing.Treatment
• Securing the airway, endotracheal intubation is very difficult in this situation, tracheostomy may be needed, but it is also difficult to perform due to the massive neck edema.• General anesthesia should be avoided.
• Early surgical drainage under local anesthesia of all the infected spaces bilaterally .
• Intravenous antibiotic using a combination of Penicillin and Metronidazole
• Some disciplines advocate high dose of antibiotics without surgery until fluctuation develops.


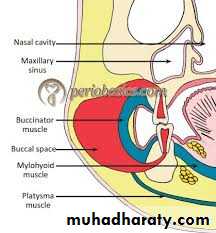
4.buccal space infection
Anatomic boundaries : bounded by the Buccinator muscle and buccopharyngeal fascia medially, skin of the cheek laterally, labial musculature anteriorly, zygomatic arch superiorly, the inferior border of the mandible inferiorly and the pterygomandibular raphe posteriorly.It contains the buccal pad of fat, facial artery and the parotid duct.
Source of infection: of this space can be related to both jaws. The relationship of the origin of the Buccinator muscle from the alveolar bone and the apices of the upper and lower premolars and molars determines the direction of the spread of infection from these teeth. If the infection exits the alveolar bone above the attachment of the muscle in the upper alveolus or below the attachment in the lower alveolus, the infection spreads to the buccal space. Otherwise the infection spreads intraorally into the vestibule where it can be drained easily.

Usually the swelling appears in the cheek, the inferior border of the mandible can still be palpated.
Site of incision and drainage intraorally by a horizontal incision in the buccal mucosa below the parotid duct, the incision should be through the mucosa only, the space should be entered bluntly using an artery or sinus forceps through the Buccinator muscle to avoid damage to the facial artery and nerve.
The incision can be placed extraorally if the pus points cutaneously.
5.Masticator spaces infection
These are well differentiated spaces but they each other as well as with the buccal ,submandibular and pharyngeal spaces. They are:• Masseteric space.
• Pterygomandibular space.
• Temporal space.
• Masseteric space infection (also called submasseteric space)
Anatomic boundaries: this space lies between the outer surface of the ascending ramus of the mandible medially, the Masseter muscle laterally and the parotid gland posteriorly.
Source of infection: usually from molar teeth especially lower third molars, it can also occur after fracture of the angle of the mandible or it can also spread from buccal space.
The swelling is moderate in size over the ascending ramus and the angle of the mandible region. This infection is characterized by a marked trismus. Chronic abscess can run a protracted course and can spread to the muscle itself or it can cause osteomyelitis of the ramus of the mandible.

Site of incision and drainage
extraorally below and behind the angle of the mandible, the incision is carried through the skin and the subcutaneous tissue then by blunt dissection through the Platysma muscle and the deep fascia, after incising the attachment of the muscle at the angle the periosteal elevator is inserted beneath the muscle and in close contact with the outer surface of the ramus of the mandible to drain all the pus.
Intraorally drainage can be carried out through an incision along the anterior border of the ramus of the mandible, but in this case the drainage can be insufficient as it is not in a dependent point, also intraoral drainage may prove to be very difficult due to the presence of trismus
• Pterygomandibular space infection
Anatomic boundaries: it is bounded medially by the Medial Pterygoid muscle, laterally by the medial surface of the ramus of the mandible, Lateral Pterygoid muscle superiorly, parotid gland posteriorly and the pterygomandibular raphe and the Superior Constrictor muscle of the pharynx anteriorly.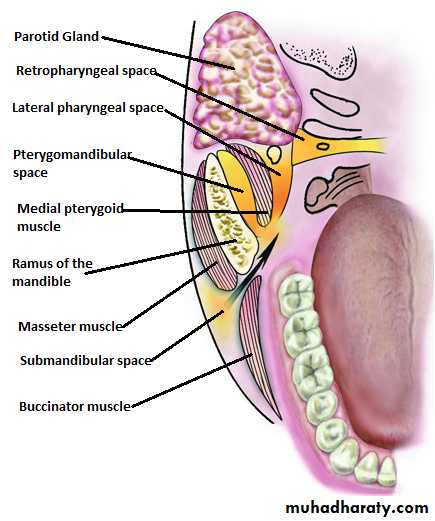
Source of infection: usually from molar teeth especially lower third molars, it can also result after inferior dental nerve block with contaminated needle or solution. Infection can spread from submandibular, sublingual and infraternporal spaces. Swelling is minimal near the angle of the mandible or sometimes there is no swelling at all, but there is a marked trismus.
Site of incision and drainage:
extraorally, the same as that described in the masseteric space infections but directed to the inner surface of the ramus.Intraorally can be drained through an incision made just medial to the pterygomandibular raphe and dissecting along the inner surface of the ramus., but the presence of trismus can prevent efficient drainage.

• Temporal space infection
Anatomic boundaries: the Temporalis muscle divides this space into two spaces:• Superficial temporal space; between the muscle and temporal fascia.
• Deep temporal space; between the muscle and the temporal bone.
The temporal space is contiguous with the pterygomandibular and masseteric spaces.

Source of infection: upper and lower molars, or by extension from the other masticator spaces.
The swelling is behind the lateral orbital rim and above the zygomatic arch, it is almost always associated with trismus.
Site of incision and drainage:
extraoral: through an incision superior and parallel to the zygomatic arch between the lateral orbital rim and the hair line.Intraorally: this space can also be drained through an incision along the anterior border of the ascending ramus with the artery forceps directed upwards on the outer aspect of the ramus, but the presence of trismus makes this approach difficult.

6.Lateral pharyngeal space infection (also termed parapharyngeal space)
Anatomic boundaries: this space extends from the base of skull to the hyoid bone, it is conical in shape, the lateral boundaries include the medial surface of the Medial Pterygoid muscle, the medial wall is the Superior Constrictor muscle, Styloglossus muscle, Stylopharyngeus muscle and the Middle Constrictor muscle of the pharynx. Posteriorly by the parotid gland and anteriorly by pterygomandibular raphe.This space can be divided into two compartments; anterior and posterior, the latter contains the carotid sheath.
Source of infection : Spread of infection from upper and lower molar teeth, most commonly from lower third molar infections by the way of submandibular, sublingual and pterygomandibular spaces.
A non-odontogenic infection can spread to this space like tonsillar infections.

Infections of this space are serious, the patient exhibits pain, fever, chills, medial bulge of the lateral pharyngeal wall, extraoral swelling below the angle of the mandible and trismus. It may lead to respiratory obstruction, septic thrombosis of the internal jugular vein and carotid artery hemorrhage.

Site of incision and drainage:
intraoral incision medial to the pterygomandibular raphe with the dissection medial to the Medial Pterygoid muscle.Extraoral incision at the level of the hyoid bone anterior to the Sternocleidomastoid muscle (SCM) and the dissection continued superiorly and medially between the submandibular gland and the posterior belly of Digastric muscle. Through and through drainage can also be applied.
7. Retropharyngeal space infection
Anatomic boundaries: extend from the base of the skull to the upper mediastinum (C6-T1), it is bounded anteriorly by posterior wall of the pharynx and posteriorly by the Alar fascia.Source of infection: upper and lower molar teeth by lateral pharyngeal space by the way of pterygomandibular, submandibular, sublingual spaces. It can also result from nasal and pharyngeal infections.
The swelling causes bulge of the posterior pharyngeal wall, there is dysphagia, dyspnea, and fever. Lateral neck radiograph may reveal widening of the retropharyngeal space.
Site of incision and drainage :
extraorally :by an incision anterior to the SCM below the hyoid bone, SCM and the carotid sheath are retracted laterally. and blunt dissection is carried out deeply to enter the space. Some authors advocated intraoral drainage by an incision along the posterior pharyngeal wall in extreme Trendelenburg position and suction. Most anesthesiologists prefer tracheostomy to secure the airway.
8. Peritonsillar abscess or Quinsy
Anatomical boundaries: it is localized between the C.T. bed of the facial tonsil and the Superior Constrictor muscle of the pharynx.

Source of infection: it arises from tonsillitis, but it is occasionally a complication of pericoronitis of the lower third molar.
It causes swelling of the anterior pillar of the fauces and a bulge of the soft palate of the affected side which may reach the midline and push the uvula. Also there is acute pain, dysphagia, the voice becomes muffled, odynophagia, drooling and anorexia.
Site of incision and drainage:
the incision is placed in the point of maximum fluctuation, this can be done under local anesthesia, if general anesthesia is used the anesthetist should be experienced and good suction be available to prevent aspiration and the patient should be in head down position.

