
1
د.سعيد
طفيليات
7
\
3
\
8102
عدد
(االوراق
9
)
م
\
3
\
موصل
lec:1+2+3
Hookworm lec 1
د
1
سعيد حميد
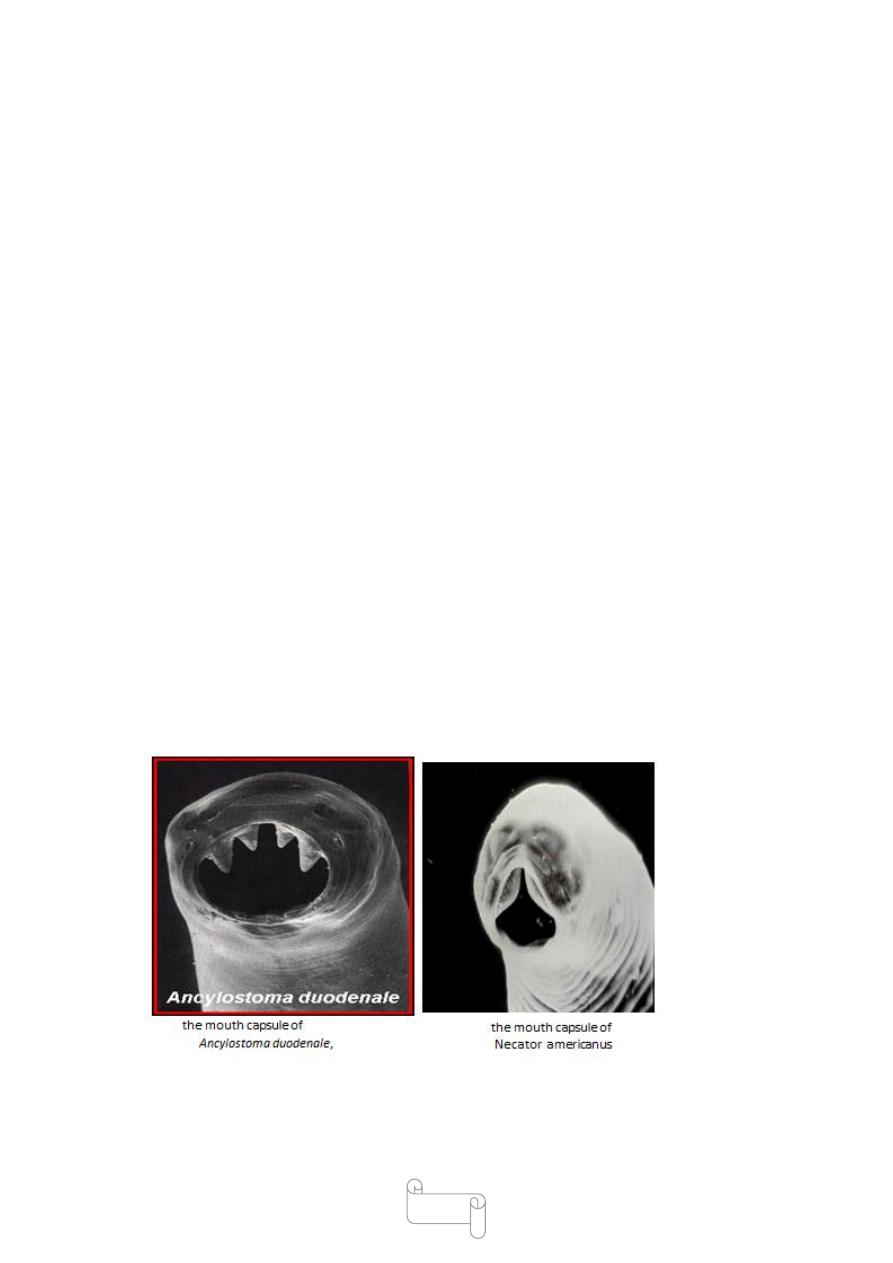
Two species of hookworms are human parasites:
1-Ancylostoma duodenale
2- Necator americanus.
Ancylostoma duodenale(Greek ankylos –hooked .stoma -mouth)
The second species Necator americanus ,called the American or
the ‘New World’ hookworm and A.duodenale the ‘OldWorld’
hookworm.
Hookworm disease is prevalent throughout the tropics and subtropics.
Even though it has been controlled in the advanced countries, it is
estimated that it still a some 900 million people, causing the loss of about
9 million litres of blood overall each day.
A. Duodenale was prevalent along the Mediterranean coast of Europe
and Africa, in northern India, China and Japan.
N. Americanus was prevalent in
Central and South America,
Central and Southern Africa,
Southern India,
2
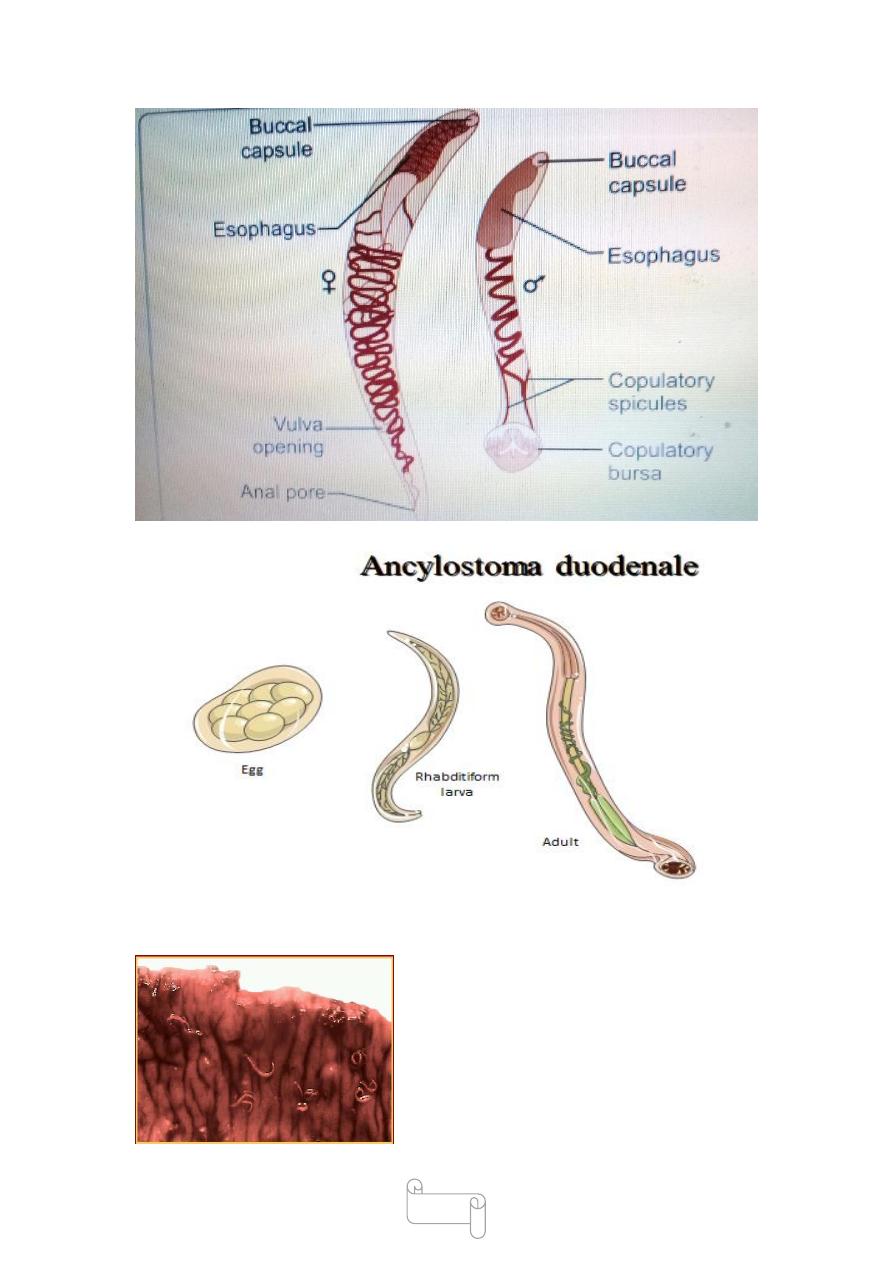
Ancylostoma duodenale
Morphology
The adult worms live in the small intestines mostly in the jejunum,
duodenum,ileum
They are pale pink or greyish white ,some time appear reddish brown
due to ingested blood .
the body is curved with the dorsal aspect concave and ventral aspect
convex,
the cervical curvature gave it the name hookworm,the mouth is not at the
tip but directed dorsally.
the prominent buccal capsule carries two pairs of hook-like teeth
ventrally and a dental plate with a median cleft dorsally
The antterior end is bent in the same direction of the general curvature
of the body(c shape single curve)
3
Adults in intestinal mucosa
4
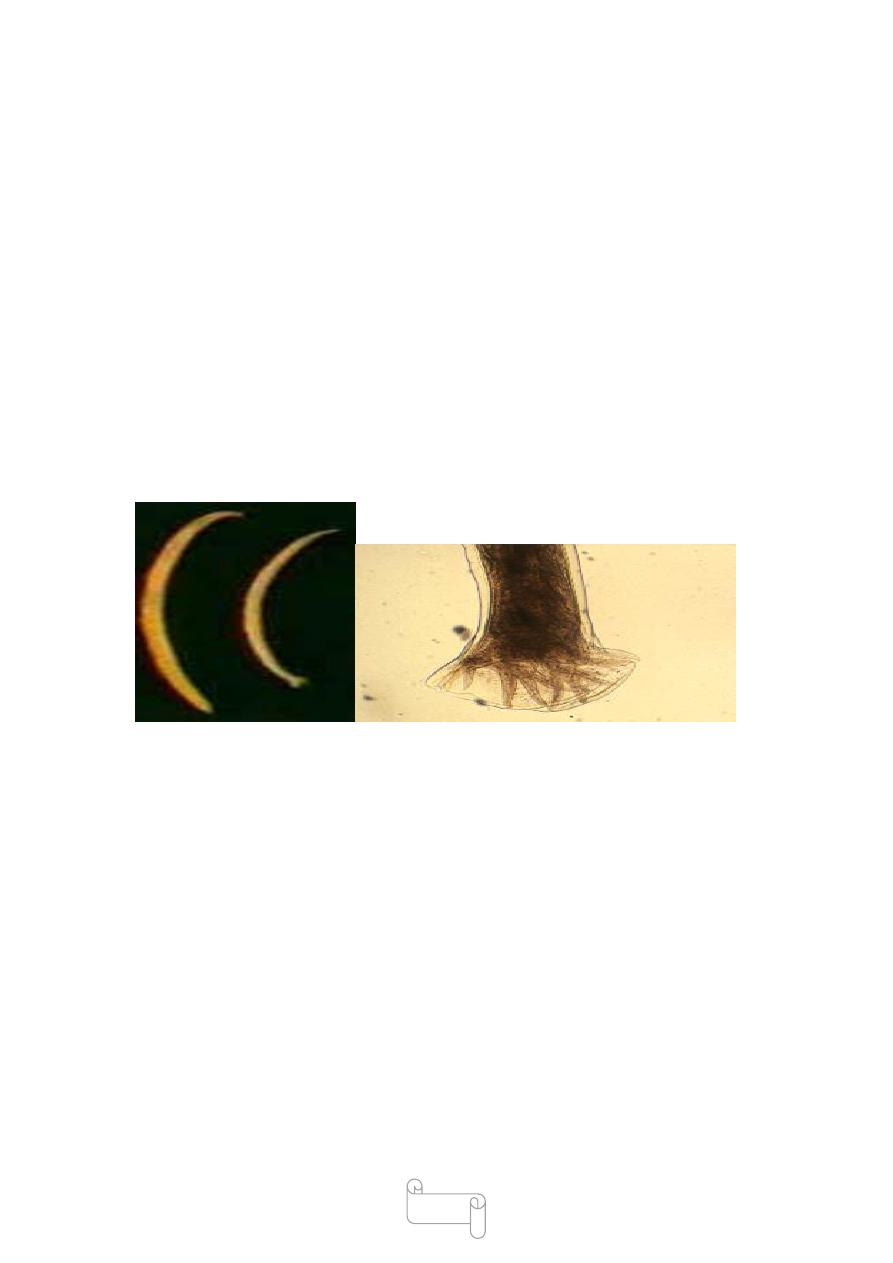
The male worm is about 8-11 mm in length 0.4mm thick. The The
posterior end of the male is expanded into a copulatory bursa supported
by fleshy rays.The pattern of the rays helps in distinguishing between
different species .
Males, smaller than females, have copulatory bursa for grasping female
.
The female is larger 10-13mm long 0.6 mm thick tapered at the posterior
end .
The anus lies ventrally near the caudal tip and the vulvar opening
at the beginning of the posterior third of the body.
Female lies around 15,000 -20,000 eggs daily and 20-50 million eggs
during its life time
Necator americanus
Morphology
The adult worms are smaller than Ancylostoma duodenale .the male 7-
9mm long 0.3 mm thick,
female 9-11mm long 0.4 mm thick.
The anterior end is bent in a direction opposite to the general curvature of
the body(s shape double curve) .
the female vulva is placed in the middle of the body,
the eggs and the life cycle are similar in both N.americanus and
A.duodenale
5
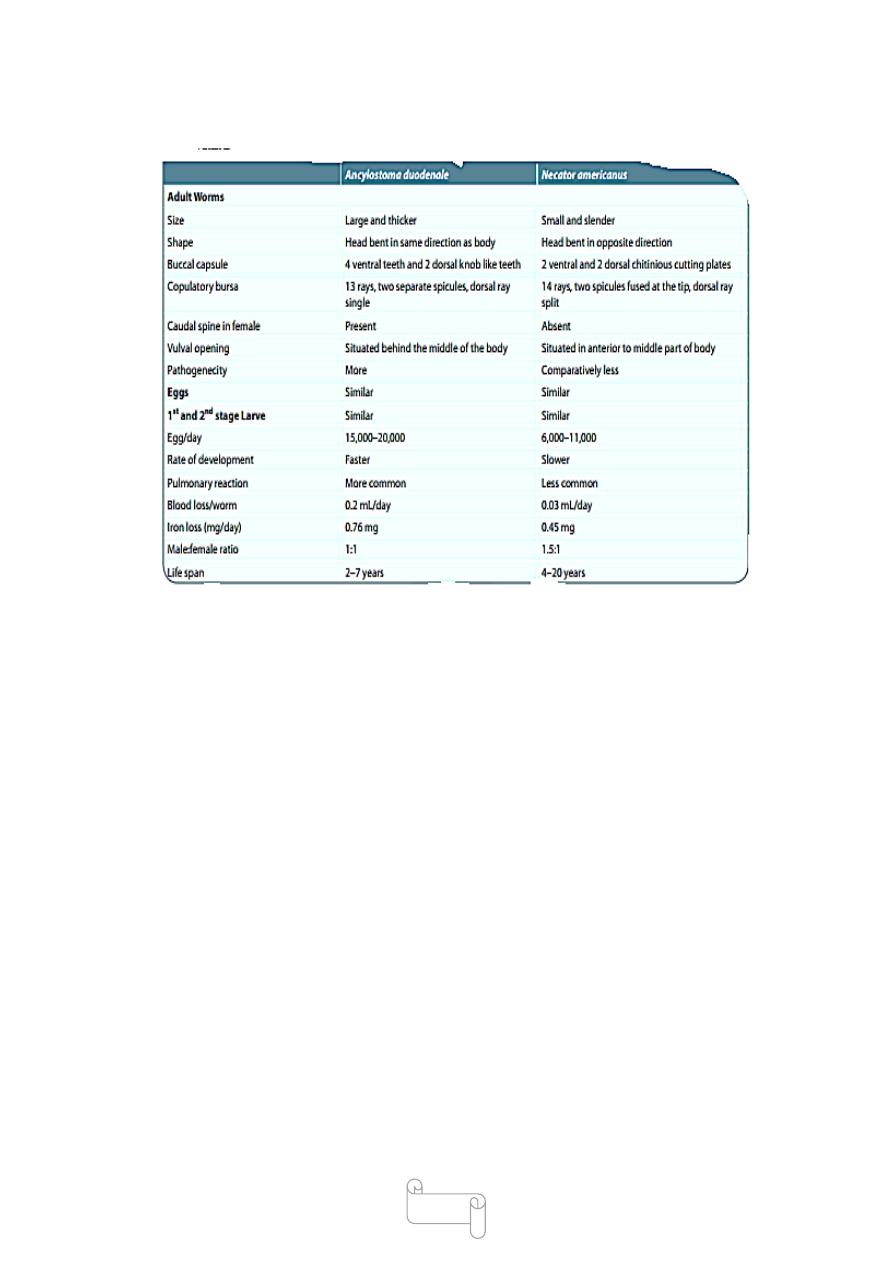
Differences between two hookworms
Adults of A. duodenale Adults of N. americanus
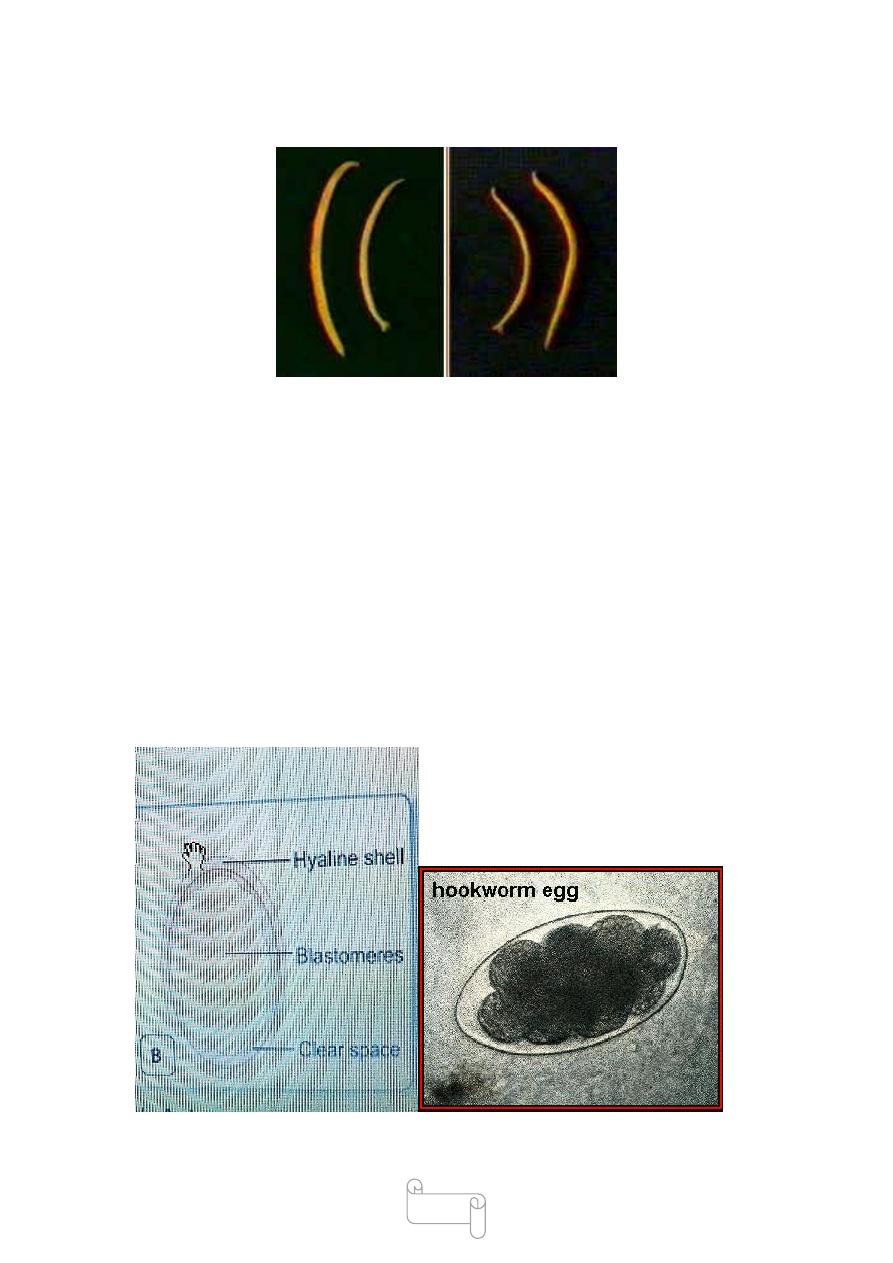
Eggs morphology
The egg is ovoid measures 60 µm by 40 µm, colourless with a thin
transparent hyaline shell membrane,
Eggs when released by the worm in the intestine ,the egg contains an
unsegmented ovum ,then developed when passed in feces ,the egg
contains a segmented ovum 4-8 blastomeres .
there is a clear space between the segmented ovum and the egg shell .the
egg float in saturated salt solution
Morphologically it is not possible to differentiate between A. duodenale
and N. americanus.
6
differentiating Features of Two Species of Hookworm
Helminths requiring no intermediate host
• Ancylostoma duodenale
• Necator americanus
• Ascaris lumbricoides
• Trichuris trichiura
• Enterobius vermicularis
• Hymenolepis nana
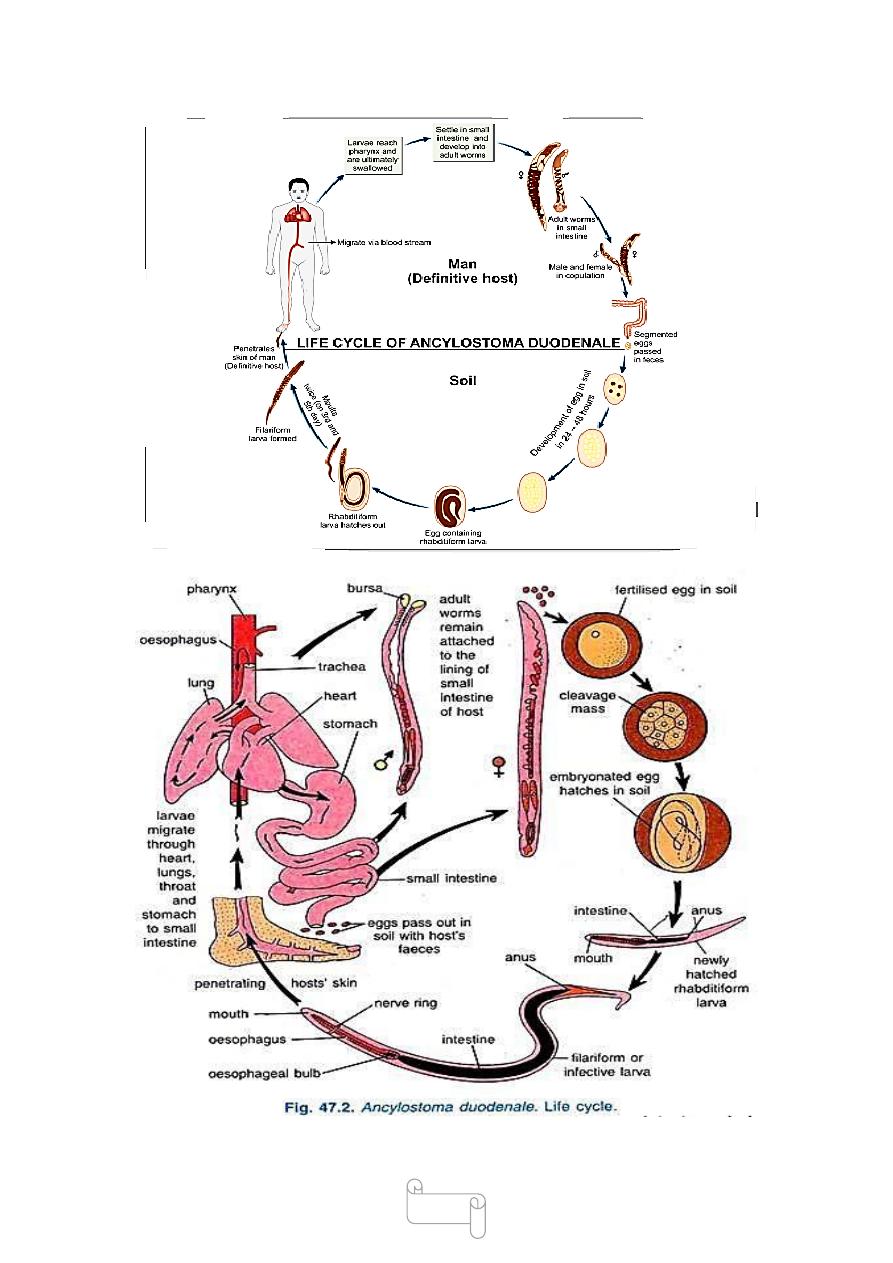
Life cycle
Natural host: Humans.
Life cycle is completed in a single host .
the male and female in small intestine ,eggs freshly passed in feces are
not infective for humans .

7
in the sandy soil and ,moist ,warm environment embryo develops inside
the eggs in about 2days the egg hatches into rhabditiform larval 250 µm
long .
rhabditiform larval feeds on bacteria and other material in soil ,grows in
size and moults twice on 3
rd
and 5
th
days after hatching to become
filariform larva 500-600 µm long (not feeding,infective stage ) ,they can
live in the soil for about 5 weeks ,waiting for their hosts.
direct sunlight ,drying ,salt water can kill the larvae .
filariform larva penetrate the skin,subcutaneous tissue(between the
toes,dorsum of the foot ,skin of the hands).
the larva enter the circulation to right heart –lung - pharynx –During
migration or on reaching the esophagus, they
undergo third moulting.
Inside the intestine under go a 4
th
moulting ,develop the buccal capsule
and grow into adult worm
the life cycle takes 6 weeks from time of infection to become adult worm
Rarely oral route infection by ingestion filariform larva enter circulation
or larva may be swallowed and develop into adult worm in the small
intestine without a tissue phase .
Transmammary and transplacental transmission reported for
Ancylostome duodenale,but not for Necator americanus
8
9
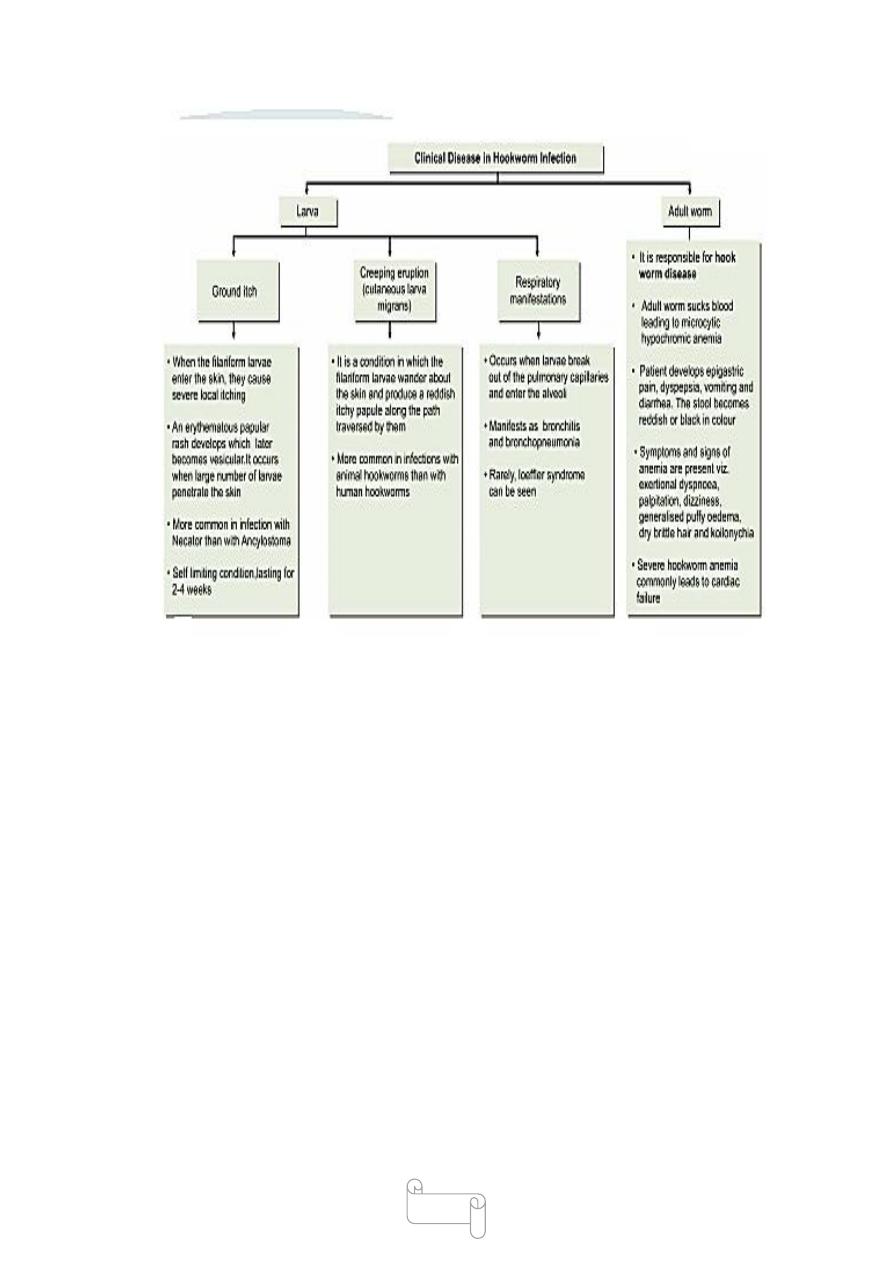
Causes of anemia in Hookworm infection
• Blood sucking by the parasite for their food
• Chronic hemorrhages from the punctured sites from jejunal mucosa
.def cient absorption of vit B12 and folic acid
• Depression of hemopoitic system by defcient intake
of proteins
• Average blood loss by the host per worm per day is
0.03 mL with N. americans and 0.2 mL with A. duodenale
10
Treatment
1- effective drug is albendazole (400 mg singledose)
or mebendazole (500 mg single dose ).
Pyrantel pamoate (10 mg/kg × 3 days) is also effective and can be used in
pregnancy.
2- if the patient suffers from anemia oral iron is effective.
Antihelminthic drugs should not be used before correcting the anemia.
3- High protein diet should be given
Prevention
Prevention of soil pollution with feces and proper disposal of night soil .
Use of footwear to prevents entry of larva through the skin of the foot.
Gloves give similar protection to the hands of farm workers.
Treatment of patients and carriers.
There are other species of ancylostoma infect animals like
species which infect

11
cats and dogs,
A.ceylanicum infects cats,Some time infected man
Trichostrongylus species infects sheep and goats can also cause human
infections.the life cycle is similar to that of hookworms
lec 2
د
0
سعيد حميد
Trichuris trichiura
Disease called Trichuriasis,whipworm infection
-Adult worm lives in large intestine
-Natural host: Man is the only host.
-No intermediate host-
the name come (Greek trichos-hair, oura-tail)
Epidemiology
It is worldwide in distribution, but is much more
common in the tropics.
The infection is widespread in tropical Africa, South America, and South-
east Asia .
children are more frequently infected than adults
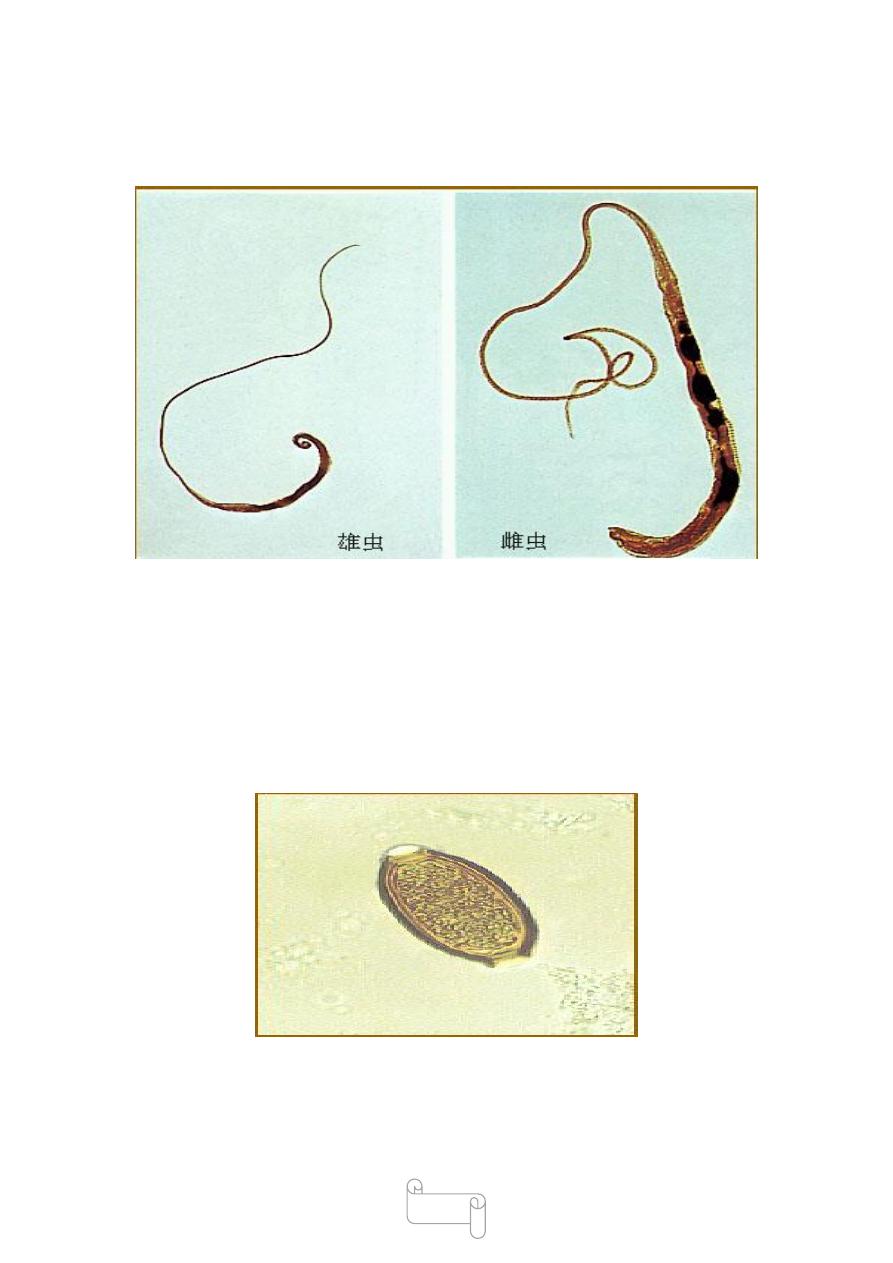
Morphology
The adult worm is flesh colour ,the shape it resembles a whip, with the
anterior 3/5 is thin and thread-like .
the posterior 2/5 is thick and fleshy appearing like the handle of a whip .
the anterior portion which contains the capillary oesophagus embedded
in the mucosa .
posterior part contains the intestines and reproductive organs
The male 30-45mm long , posterior end coiled ventrally .
The female 40-50mm long ,the posterior end straight ,blunt and rounded
Humans are the only natural host for Trichuris trichiura But similar
worms are found in pigs and monkeys
12
Adults of T. trichiura
Egg: it is barrel or spindle in shape,about 50µm long 20µm width . It is
brownish in colour and has a translucent clear polar plug at each ends.
The content of the egg is an undeveloped cell,
the egg floats in saturated salt solution
The fertilized female lays about 5,000 eggs per day
Helminths whose eggs float in saturated salt solution

13
• Enterobius vermicularis
• Ancylostoma duodenale
• Necator americanus
• Ascaris lumbricoides
• Trichuris trichiura
Nematodes present in large intestine
• Enterobius vermicularis
• Trichuris trichiura
Life Cycle
Humans are the only natural host for T. trichiura, but
morphologically similar worms are found to infect pigs
and some monkeys .
No intermediate host is required.
Infective form: Embryonated eggs contaning Rhabditiform larva.
When freshly passed, the egg contains an unsegmented ovum. At this
stage, it is not infective for humans.
The fertilized female lays about 5,000 eggs per day .
.Adult female worm lives in large intestine ,female lays eggs which are
discharged in feces.
The egg undergoes development in soil, optimally under warm, moist,
shady conditions.
when the infective rhabditiform larva develops within the egg in 3–4
weeks. At lower temperatures, this may be delayed for 3 months or more .
These embryonated eggs are infective stage to man.
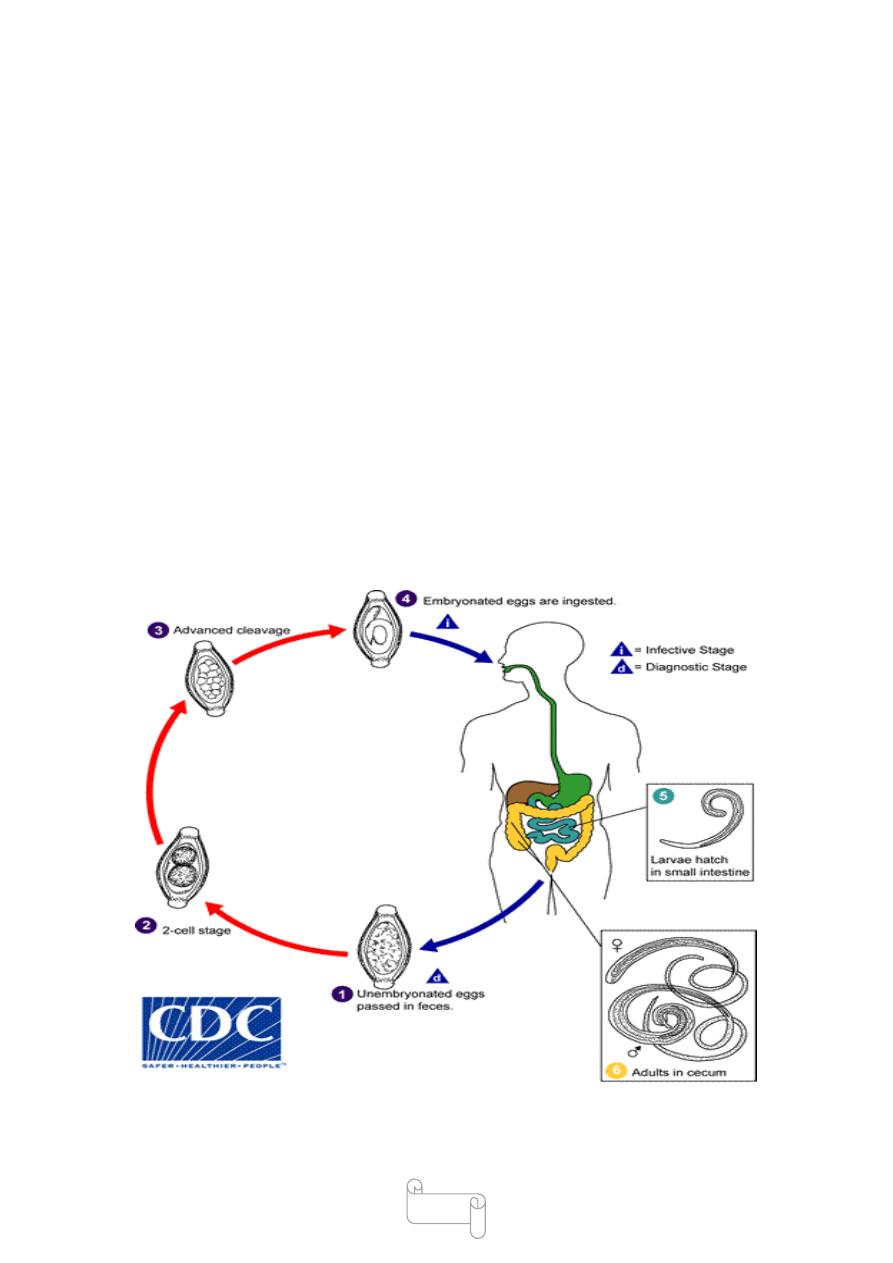
14
Infection occurs in humans when the mature embryonated eggs
containing the infective larvae are swallowed in contaminated food or
water.
The eggs hatch in the small intestine and the larva penetrate and develop
in the intestinal villi with in 3-7days, and then return to lumen and
migrate to the area of the cecum.
In about 2–3 months they become mature adults and
lie embedded in the cecal wall, with the thread-like
anterior portion piercing the mucosa and the thick posterior end
projecting out.
The gravid adult female lays eggs, eggs start appearing in feces usually
about 3 months after infection which are discharged in feces and the
cycle is repeated .
Life span is usualy 4-6 years

15
Clinicl feature
Slight infections - are usually asymptomatic .
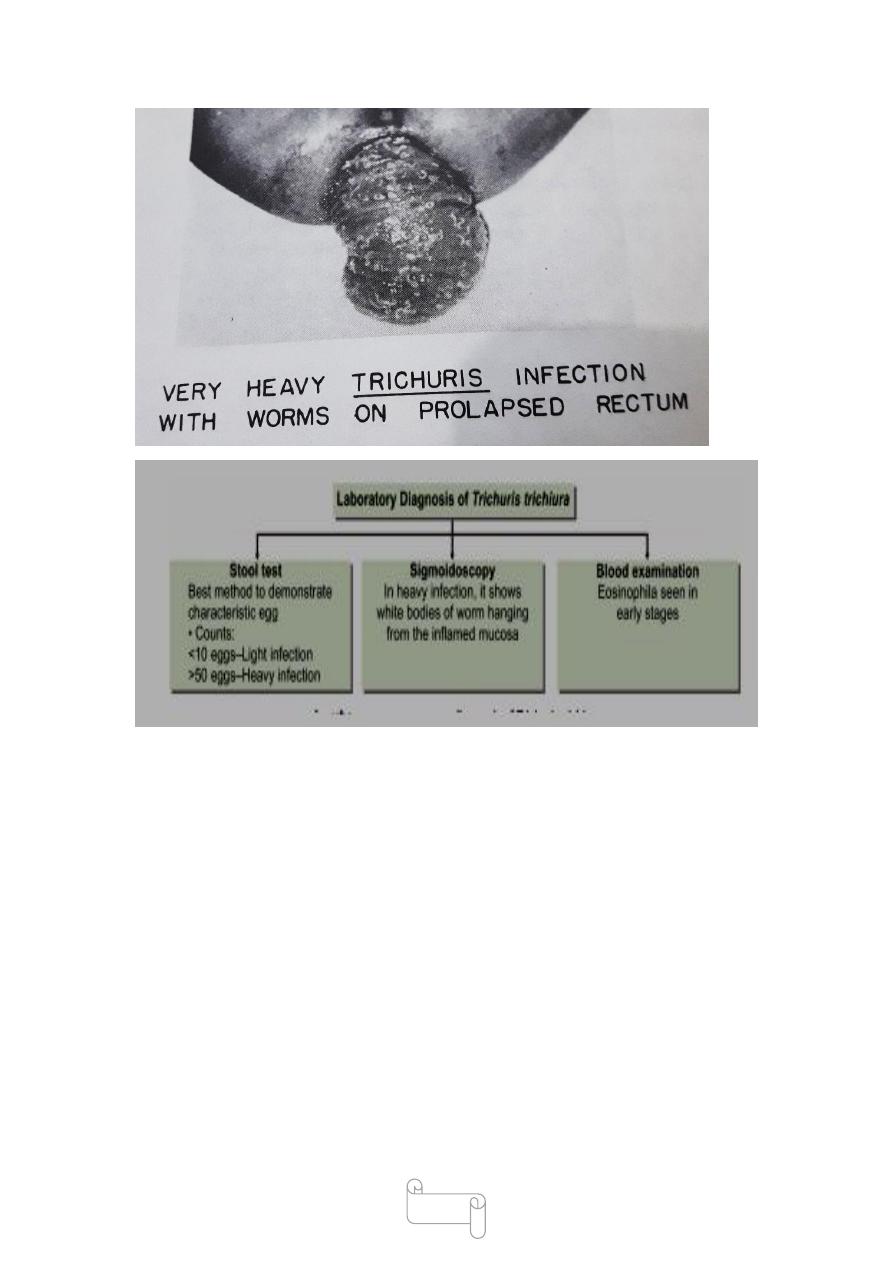
In the Heavy infections lead to mechanical effects or allergic reaction.
The worms lie threaded into the cecal mucosa and even though it is not a
blood feeder, oozing of blood may at the sites of attachment.
The blood loss is about 0.005 mL per worm per day.
Over a period of time, this may lead to anemia and malnutrition.
It has been suggested that mechanical blockage of the appendical lumen
by masses of whipworms may cause acute appendicitis
worms in children may cause a chronic dysentery,abdominal pain and
tenderness
increased peristalsis and rectal prolapse especially in children .
worms in children may cause a chronic dysentery,abdominal pain and
tenderness
increased peristalsis and rectal prolapse especially in children
In heavy infection, sigmoidoscopy
may show white bodies of worm hanging from the inflamed
mucosa called coconut cake rectum
16
Treatment:
Mebendazole (100 mg 12 hourly for 3–5 days) or
Albendazole (single dose of 400 mg) are effective with cure rates of 70–
90%.
Prophylaxis
Proper disposal of feces.
Avoiding consumption of unwashed fruits and vegetables.
Treatment of infected persons.
Trichinell aspiralis lec 3
د
1
سعيد حميد

17
disease called trichinosis, trichinelliasis
The name Trichinella derived from the minute size of
the adult
the smallest nematodes infecting humans
The major source of human infection was shown to be
the consumption of inadequately cooked pork
Trichinosis is recognized as an important public health
problem in Europe and America, but is much less
common in the tropics and oriental countries
Subspecies
(a) Trichinella spiralis spiralis- seen in temperate regions,
Acquired from domestic pigs, source of majority of
infections in U.S.A.
(b) Trichinella spiralis nativa seen in arctic regions, acquired
by eating undercooked bear and walrus meat.
(c) Trichinella spiralis nelsoniis acquired form wild pigs in southern
Europe and Africa.
Morphology
Adult worm white in colour females are 3.5 mm long by 0.06mm thick.
males measure 1.5 mm long by 0.04 mm,
the antreior half of the body is thin and pointed.

18
the posterior port of the male has a pair of pear –shaped clasping
papillae;
The female worm is viviparous and discharge larva instead of eggs.
The life span of the adult worm is very short.
The male worm dies soon after fertilizing the female and the female dies
after 4 weeks to 4 months (16 weeks).

19
د. سعيد طفيليات
00
\
3
\
8102
( عدد االوراق
7
) م
\
3
\
موصل
LEC:4
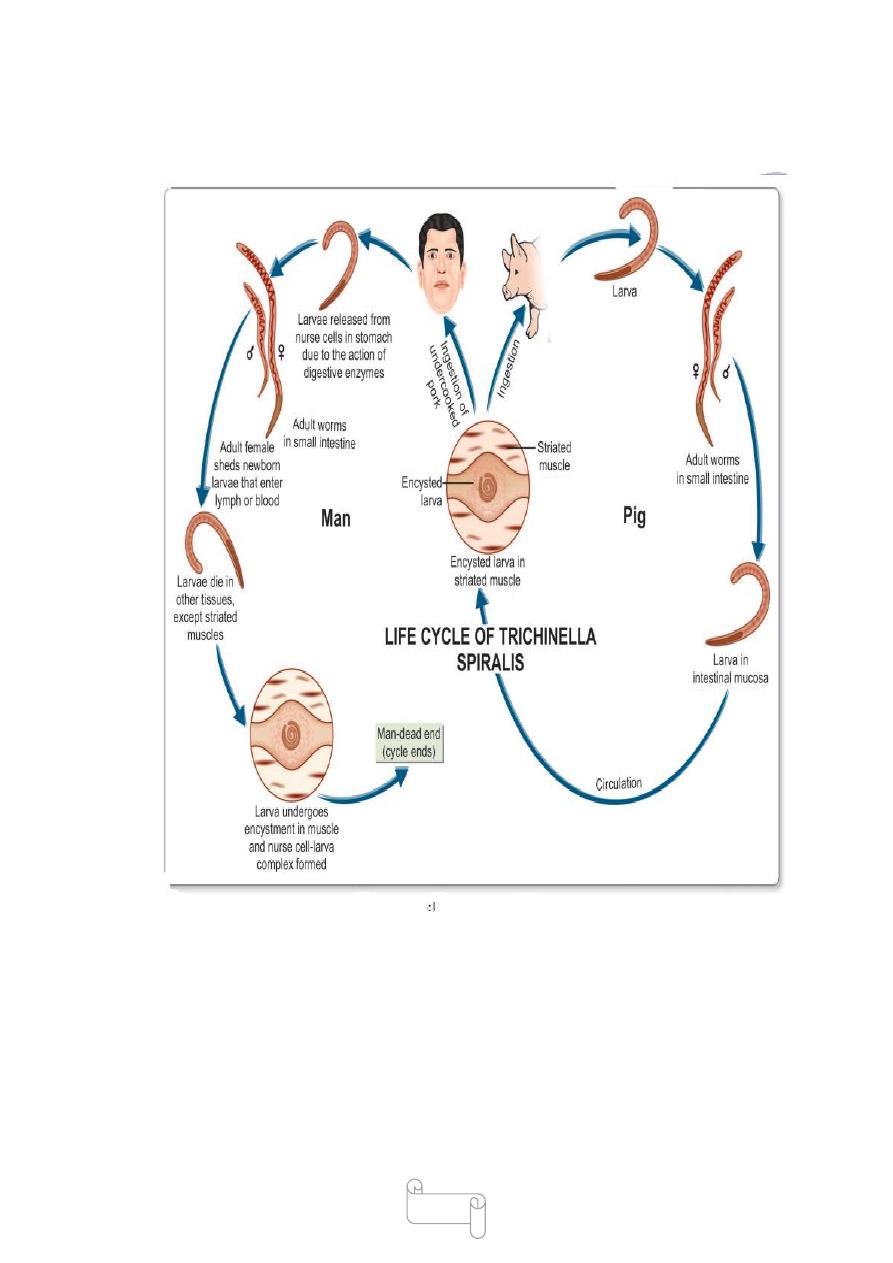
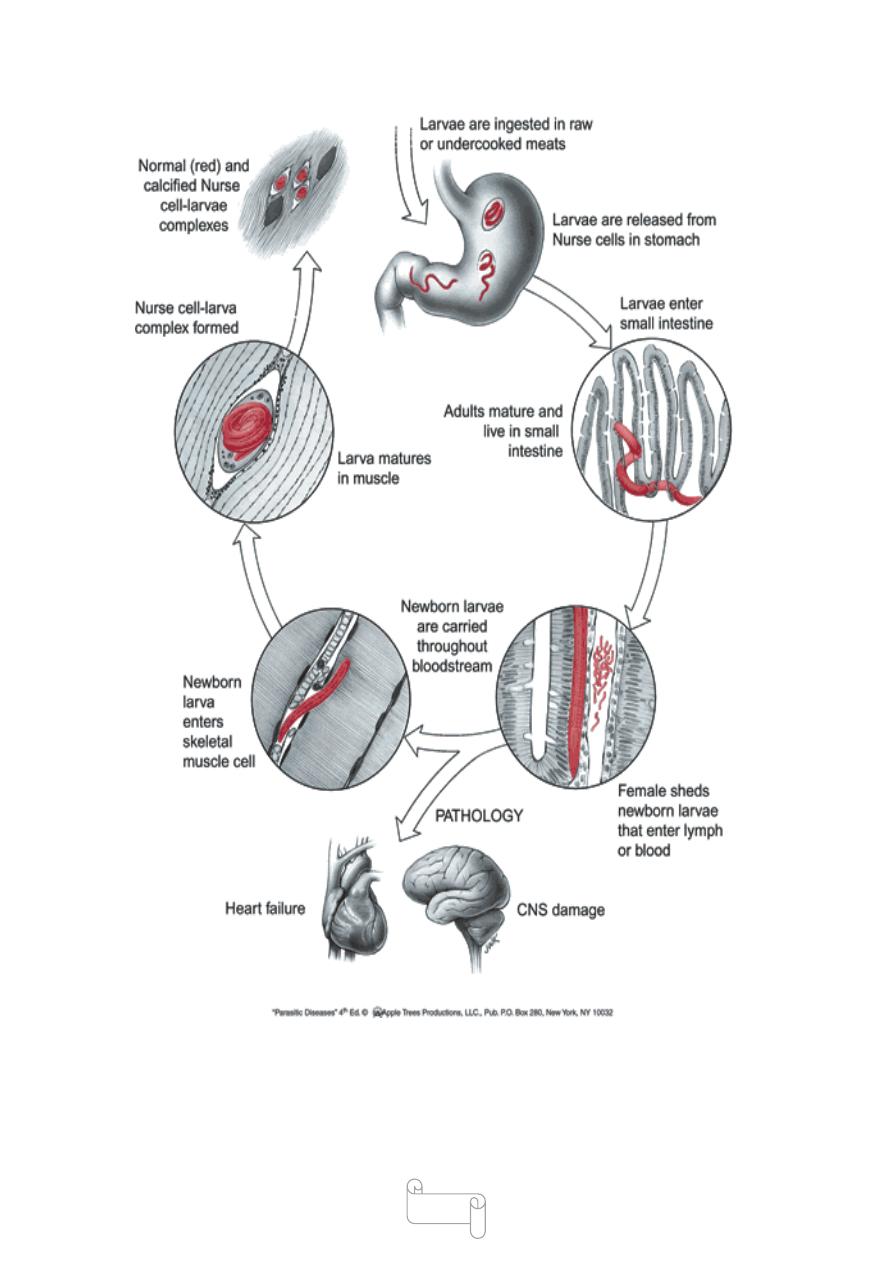
life cycle
Natural host: Pig . Alternate host: Man.
Animal and man act as final and intermediate host
Infection can pass from—Pig-to-pig (facilitated by the custom of feeding
pigs with untreated household garbage, which may contain bits of pork
with infective cysts),
rat-to-rat, and pig-to-rat .
Man is the dead-end of the parasite, as the cysts in human muscles are
unlikely to be eaten by another host.
Infective form: Encysted larva found in the muscles of pigs and other
animals
Mode of infection: Man acquires infection mainly by eating raw or
undercooked pork or inadequately processed sausages or other meat
products containing the viable larvae.
When such meat is eaten without adequate cooking, the
cysts are digested by the gastric juice and viable larvae are released
(excystation) in the stomach, duodenum, and jejunum
The larvae immediately penetrate the intestinal mucosa.

20
They moult 4 times and rapidly develop into adults, either male or
female, by the second day of infection and with in 5 days, they become
sexually mature worm.
The male dies after fertilizing the female.
The fertilized females start releasing motile larvae by the sixth day of
infection
Larvae continue to be discharged during the remaining part of the
lifespan of the female worm, which ranges from 4 weeks to 4 months.
Each female gives birth to approximately 1,000 larvae. These larvae
enter the intestinal lymphatics or mesenteric venules and are transported
in circulation to different parts of the body.
They get deposited in the muscles, central nervous system ,heart and
other sites.
The larva die in most other situations, except the skeletal muscles, where
it grows.
The common muscle involved (diaphram,intercostal , cervical,tongue in
heavy infection 1000 cysts per gram of muscle
Deposition in the muscles occurs mostly during the second week of
infection.
Larval development in muscles takes place during the next 3 or 4 weeks.
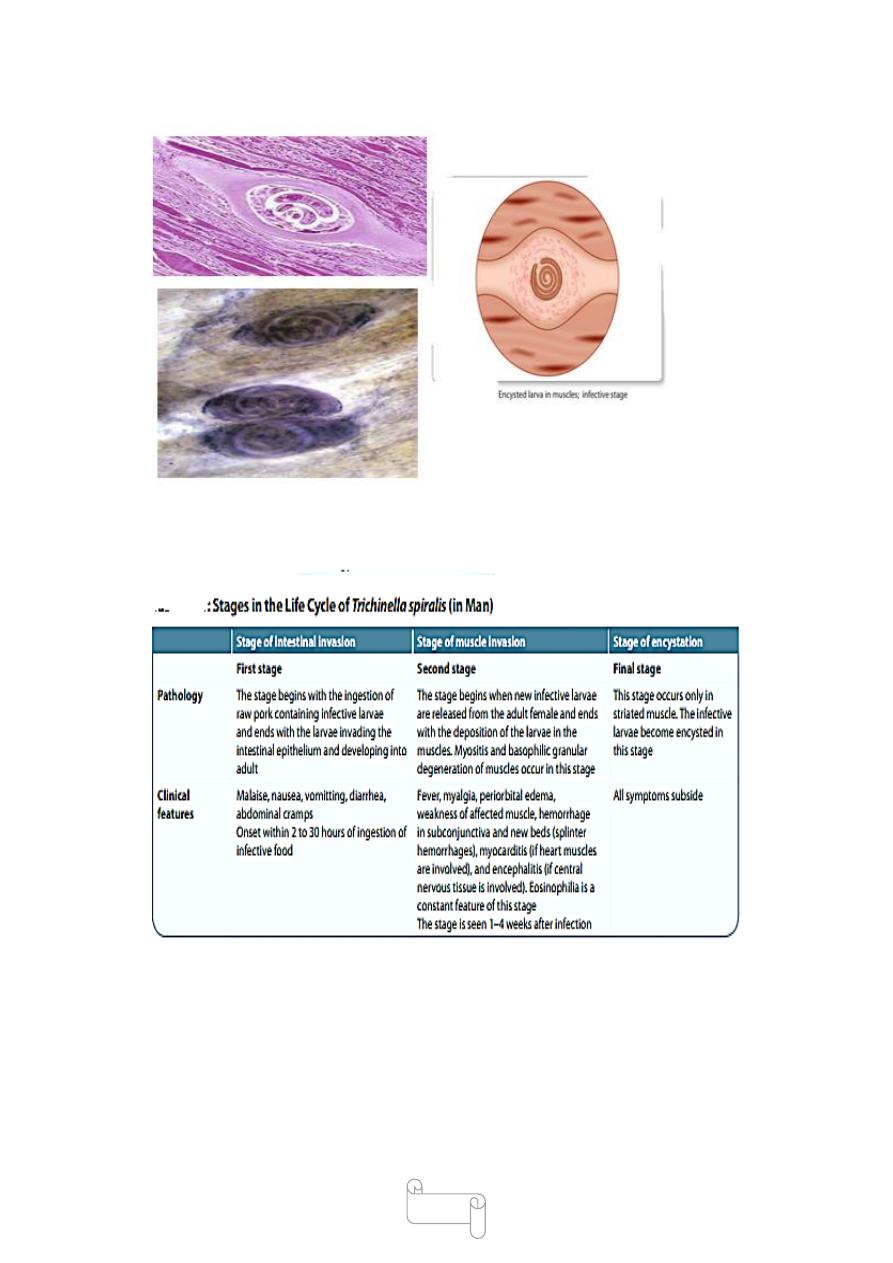
Within 20 days after entering the muscle cells, the larvae become
encysted.
Encysted larvae lie parallel to the muscles of host.
Encysted larva can survive for months to years
In man, the life cycle ends here
The larva at birth 100 µm and grow to reach 1000 µm in length The
mature encysted larva becomes simillar to adult worm but sex organ not
fully developed.
The cyst is formed by the tissue reaction around the encapsulated larvae.
the larva in the cyst is coiled
21
The larva remains infective inside the cyst for years and eventually,
most become calcified and die with in 6-months to 2years
22
23
Clinicl feature
24
Treatment
Mild cases: Supportive treatment consisting of bed rest, analgesics, and
antipyretics
Moderate cases: Albendazole 400 mg for 8 days or Mebendazole 200–
400 mg for 3 days.
Severe cases: Add glucocorticoids like prednisolone to albendazole or
mebendazole.
Mebendazole and albendazole are active against enteric stage of the
parasite,
Prophylaxis
-Proper cooking of pork and other meat likely to be infected.
-the most effective method is to stop the practice of feeding pigs with
raw garbage.
-Extermination of rats from pig farms the spread of infection .
-Smoking, salting or drying the meat does not destroy
the infective larvae.
-Prolonged freezing (20 days in a normal freezer) or (at –20°C for 3
days) decontaminates the meat.

25
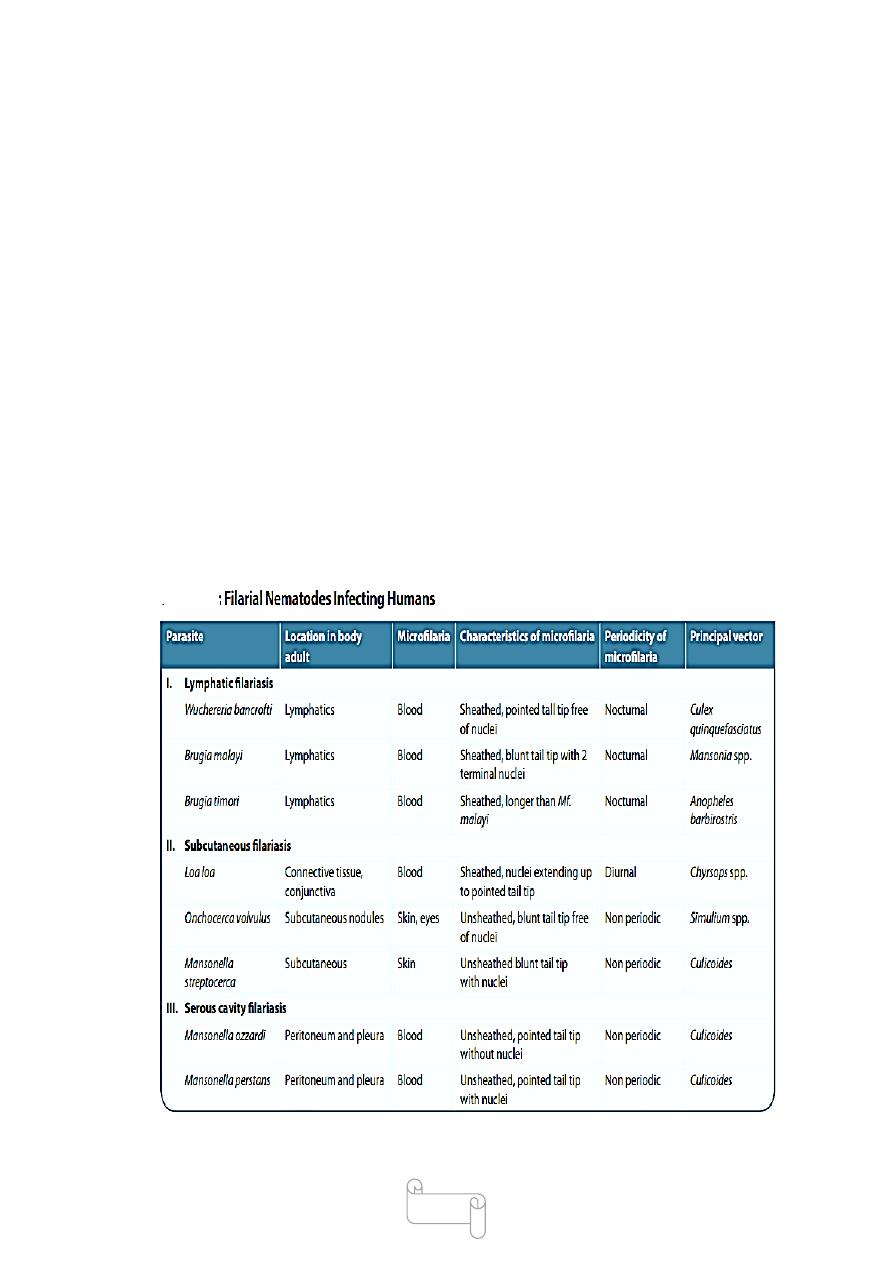
filarial nematodes
The filarial worms reside in the 1- subcutaneous tissues,
2-lymphatic system, 3- body cavities of humans
The adult worm generally measures 80–100 mm in
length and 0.25–0.30 mm in breadth.
the female worm being longer than the males.
The tail of the male worm has perianal papillae and
unequal spicules but no caudal bursa.
The female worms are viviparous and give birth to
larvae known as microfilariae.
The microfilariae released by the female worm, can be
detected in the peripheral blood or cutaneous tissues, body cavities of
humans depending on the species.
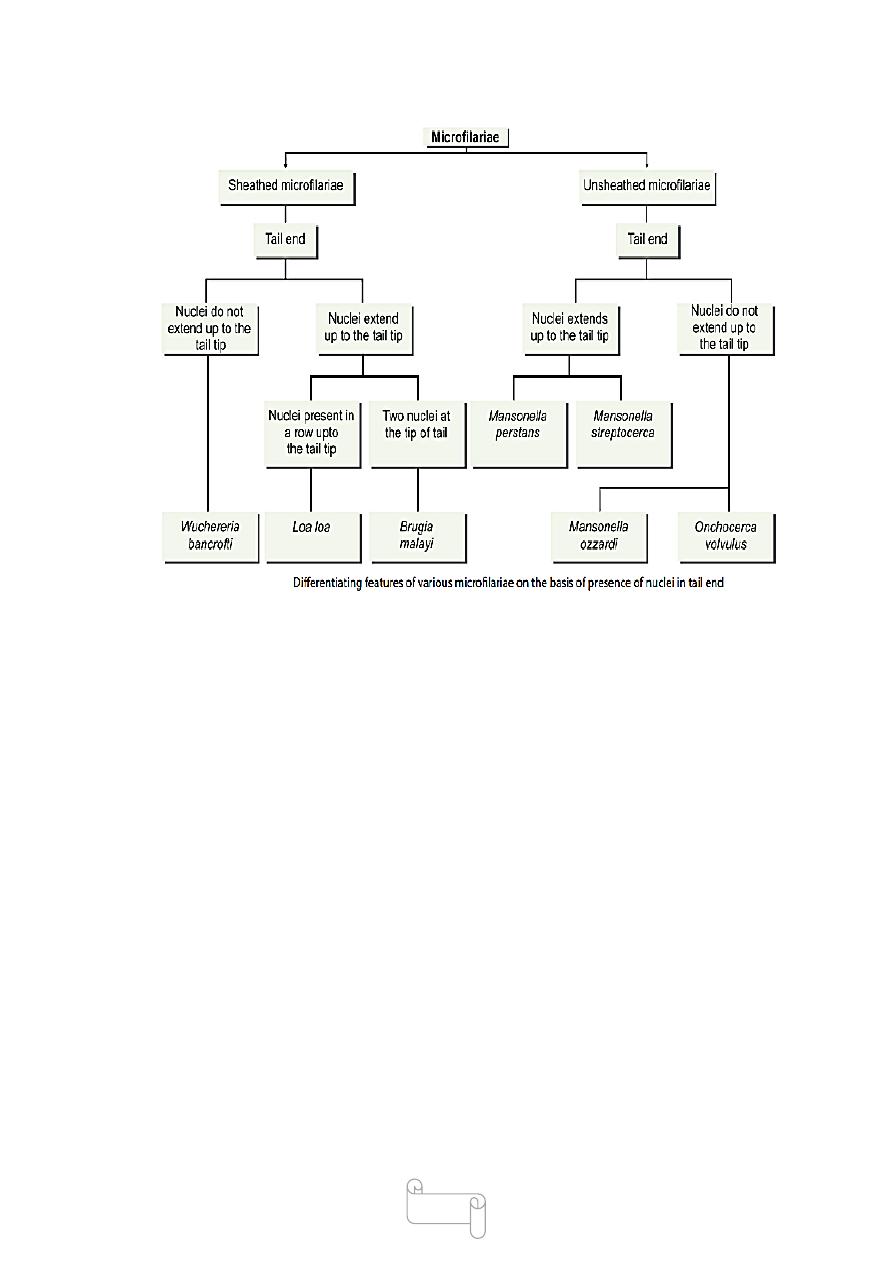
-In some species, the microfilariae retain their egg membranes which
envelop them as sheath. They are known as sheathed microfi lariae .
-In other species the egg membrane is ruptured and are known as
unsheathed microfi lariae. the microfilariae are classified on the basis of
sheath
as ‘sheathed’ or ‘unsheathed.
-Other differentiation can be done on the characteristic arrangement of
nuclei
26
Periodicity: depending on when the largest number of microfi lariae occur
in blood, filarial worms can exhibit
nocturnal, diurnal periodicity or non periodicity at all
• Nocturnal periodicity: When the largest number of
microfi lariae occur in blood at night, e.g. Wuchereria
bancrofti
• Diurnal periodicity:When the largest number of
microfi lariae occur in blood during day, e.g. Loa loa
• Nonperiodic:When the microfi lariae circulate
at constant levels during the day and night, e.g.
Onchocerca volvulus.
- The life cycle of filarial nematodes is passed in 2 hosts:
definitive host is man
intermediate host are the blood-sucking arthropods.
27
The microfilariae complete their development in the
arthropod host to produce the infective larval stages. These are
transmitted to humans by arthropod.
Adult worms live for many years .
the microfilariae survive for 3–36 months.
Eight species of filarial worms infect humans, of them six are
pathogenic—
(Wuchereria bancrofti, Brugia malayi, and B. timoricause ) lymphatic
filariasis.
Loa loa causes malabar swellings and allergic lesions.
Onchocerca volvulus causes eye lesions and dermatitis.
Mansonella streptocerca leads to skin diseases.
two of them, M. ozzardi and M. perstans are virtually nonpathogenic

28
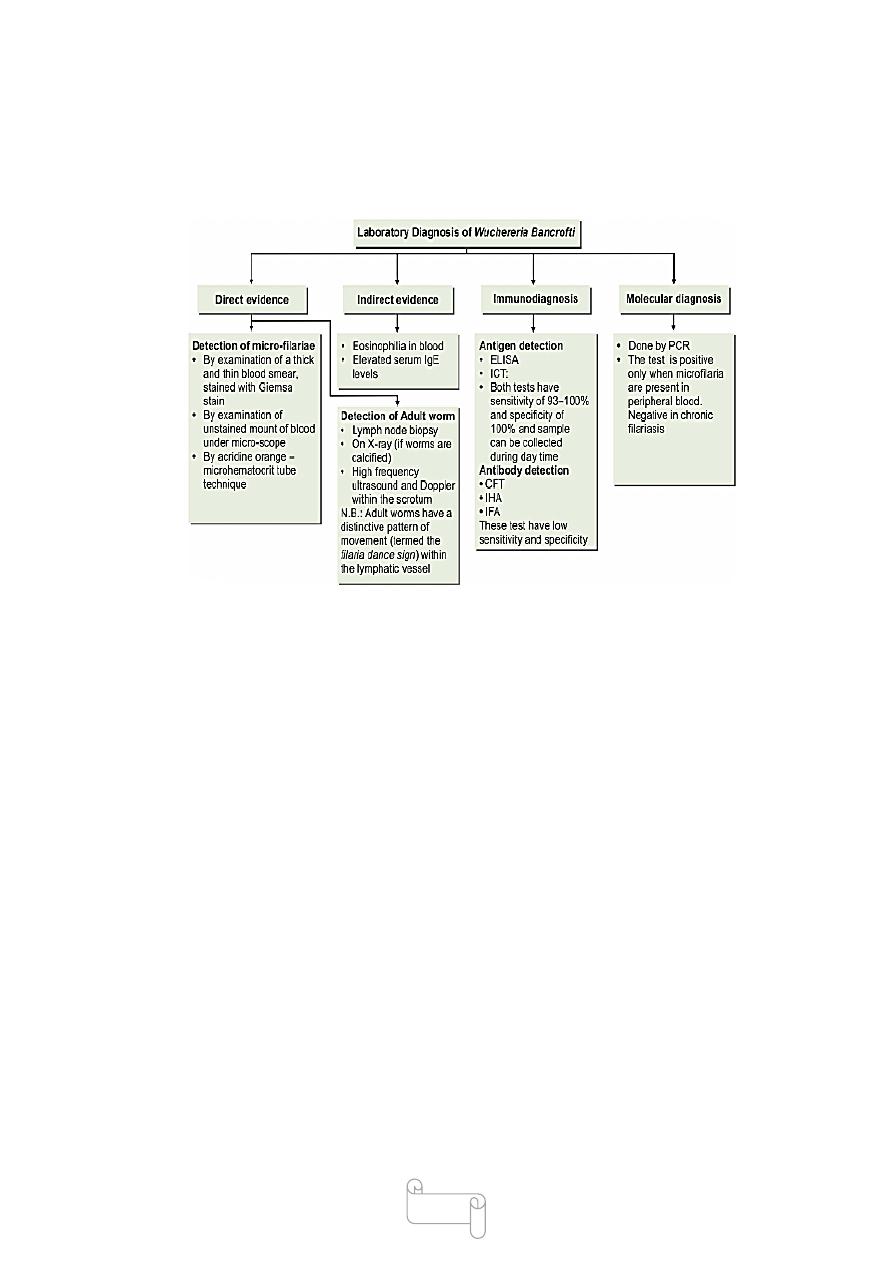
LYMPHATIC FILARIASIS
Wuchereria Bancrofti
Wuchereria bancrofti (Bancroftian filariasis,elephantiasis)
The disease is widely distributed through the tropical area of Africa,
Asia and Latin America.
The largest number of cases of fi lariasis occur in India
Man is the only natural definitive host.
Intermediate host is the female mosquitoes especially anopheles and
culex species.
Morphology
The adults are whitish, translucent, thread-like worms with smooth
cuticle and tapering ends
The female is larger (70–100mm × 0.25 mm), the male (25–40mm ×
0.1 mm).
The posterior end of the female worm is straight, while that of the
male is curved vertically and contains 2spicules of unequal length.
Males and females remain coiled together usually in the abdominal
and inguinal lymphatics and in the testicular tissues
The female worm is viviparous and directly liberates sheathed
microfi lariae into lymphatics.
Adult worms live for many years, probably 10–15 years or more.
29
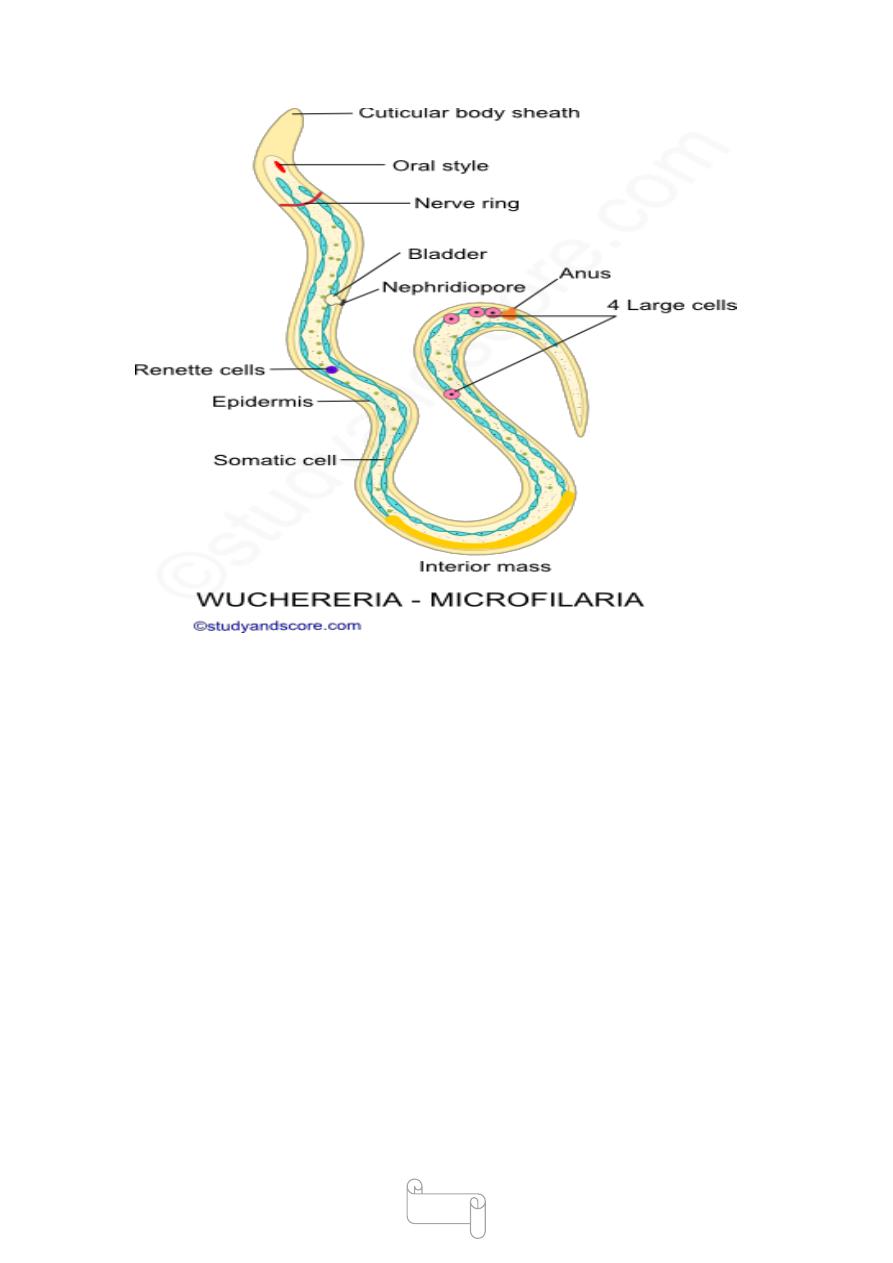
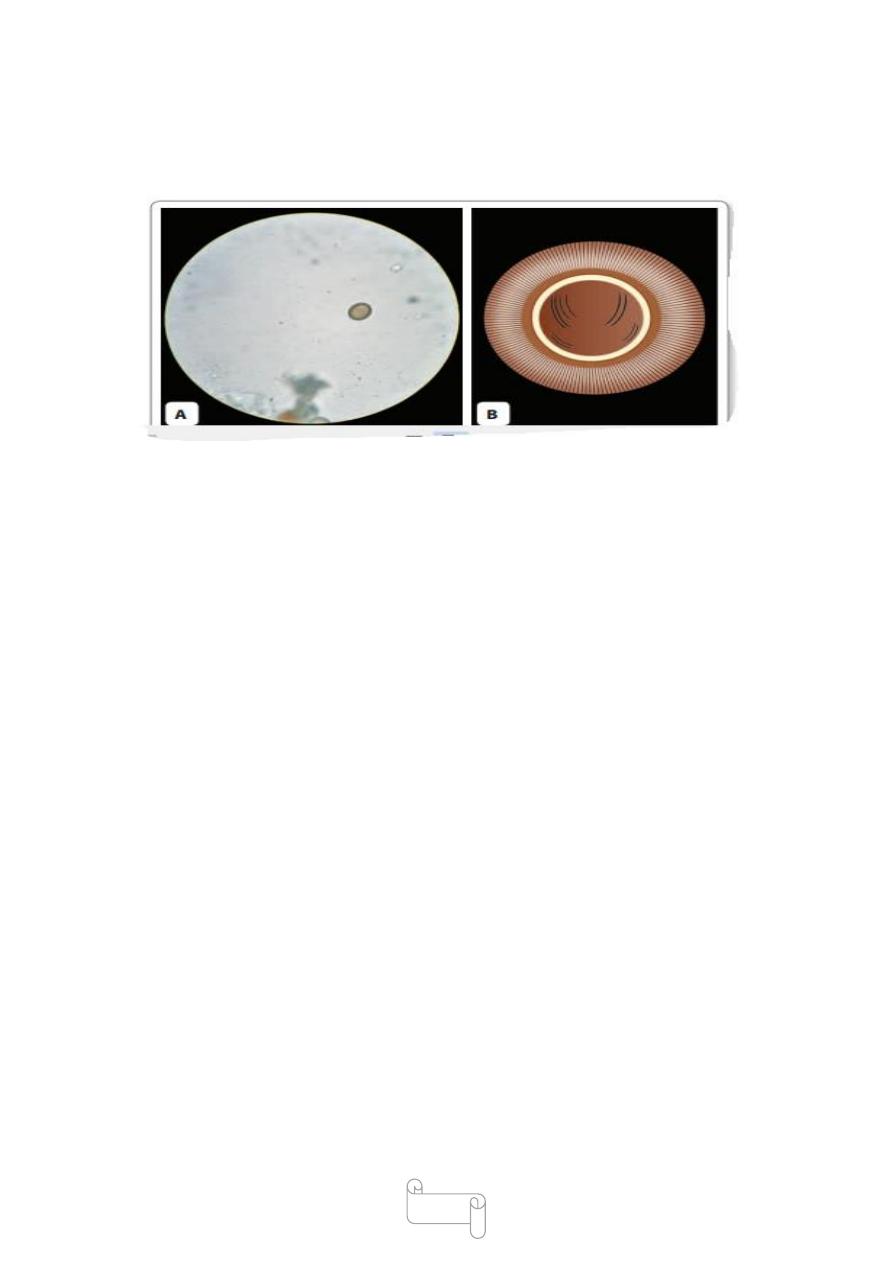
Microfi lariae
The microfi laria has a colorless, translucent body with a blunt head,
and pointed tail
It measures 250–300 µm in length and 6–10 µm in thickness. It can
move forwards and backwards within the sheath which is much
longer than the embryo.
large numbers of microfilariae in peripheral blood only at
night (between 10 pm and 4 am).
30
Microfilariae do not multiply or undergo any further development
in the human body.
If they are not taken up by a female vector mosquito, they die.
The lifespan is believed to be about 2–3 months.
It is estimated that a microfilarial density of at least 15 per
drop of blood is necessary for infecting mosquitoes.
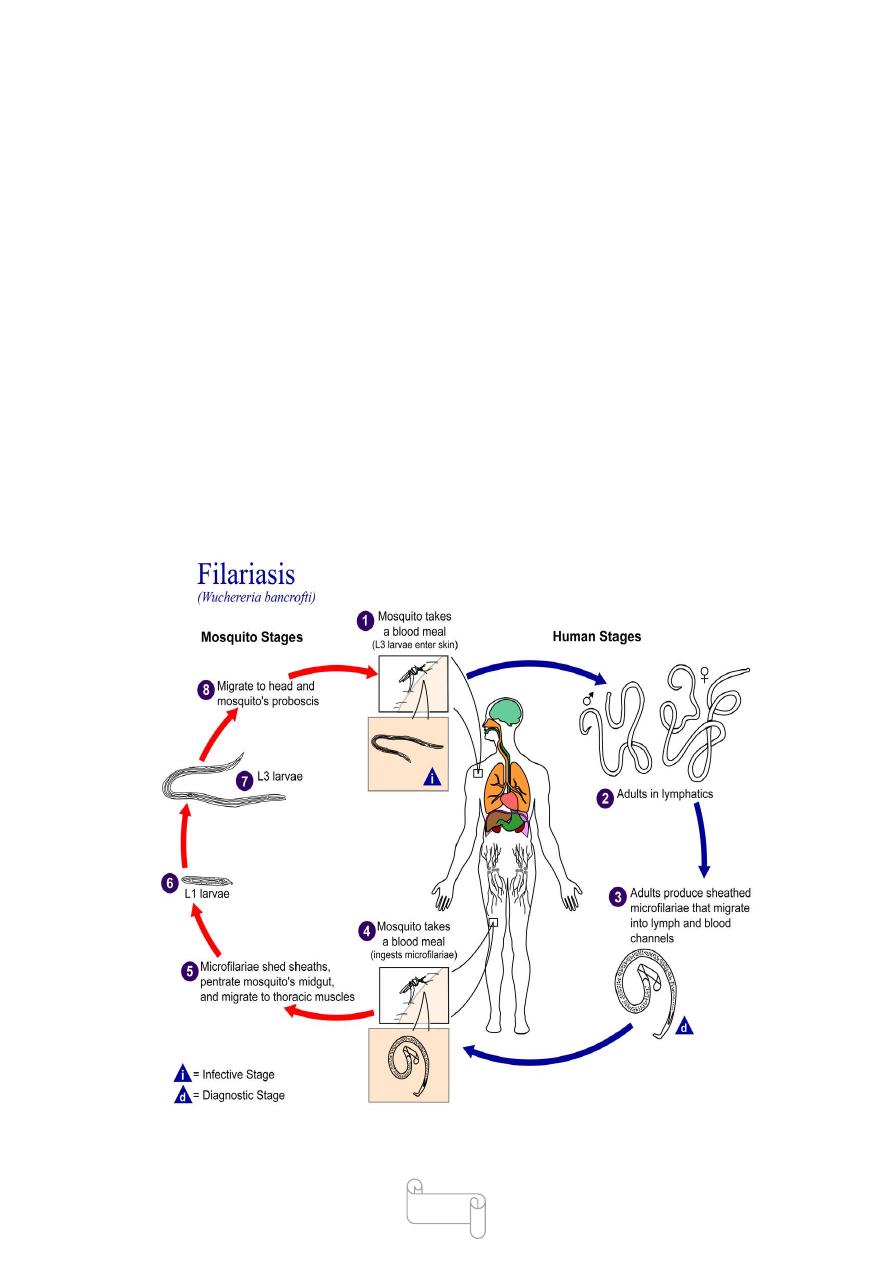
Life Cycle
life cycle need two hosts
Definitive host: Man. No animal host or reservoir is known for W.
bancrofti
Intermediate host: Female mosquito, of different species acts as
vectors in different geographic areas.

31
The major vector in India and most other parts of Asia is Culex.
Infective form: Actively motile third-stage filariform larva is
infective to man.
Mode of transmission: Humans get infection by bite of mosquito
carrying filariform larva
Development in Mosquito
When a vector mosquito feeds on a carrier, the microfilariae are
taken in with the blood meal and reach the stomach of the mosquito.
Within 2–6 hours, they cast off their sheaths (exsheathing), penetrate
the stomach wall and within 4–17 hours migrate to the thoracic
muscles where they undergo further development.
during the next 2 days into .
the first-stage larva, which is a sausage-shaped with a spiky tail,
measuring 125–250 × 10–15 µm with in a week, it moults once or
twice, increases in size and becomes.
the second-stage larva, measuring 225–325 × 15–30 µm In another
week, it develops its internal structures and becomes
the elongated third-stage filariform larva, measuring 1,500–2,000 ×
15–25 µm. It is actively motile and is the infective form . It enters the
proboscis sheath of the mosquito.
There is no multiplication of the microfilaria in the mosquito and 1
microfilaria develops into 1 infective larva only.
The time taken from the entry of the microfilaria into the mosquito
till the development of the infective third stage larva located in its
proboscis sheath (10-20 days)
Devolopment in Man
The larvae enter through the puncture wound or penetrate the skin
by themselves.
The infective dose for man is not known, but many larvae fail to
penetrate the skin by themselves and many more are destroyed in the
tissues by immunological and other
deffence mechanisms.
32
After penetrating the skin, the third-stage larvae enter the lymphatic
vessels and are carried usually to abdominal or inguinal lymph
nodes, where they
develop into adult worm.
There is no multiplication at this stage and only 1 adult
develops from 1 larva, male or female.They become sexually mature
in about 6 months .
The gravid female worm releases large numbers of
microfi lariae, as many as 50,000 per day.
They pass through the thoracic duct and pulmonary capillaries to
enter the peripheral circulation.
The microfi lariae are ingested with the blood meal by mosquito and
the cycle is repeated.

33
د. سعيد طفيليات
02
\
3
\
8102
( عدد االوراق
6
) م
\
3
\
موصل
lec:5+6
Occult Filariasis
It occurs as a result of hypersensitivity reaction to microfi larial antigens,
not directly due to lymphatic involvement.
Clinical manifestations:
€ Massive eosinophilia (30–80%)
€ Hepatosplenomegally
Pulmonary symptoms like dry nocturnal cough, dyspnea, and asthamatic
wheezing.€
Some time see arthritis, glomerulonephritis, thrombophlebitis,
tenosynovitis, etc.
Meyers Kouwenaar syndrome is a synonym for occult fi lariasis.
Tropical pulmonary eosinophilia: presents with low-grade fever, loss of
weight, and pulmonary symptoms such as dry nocturnal cough, dyspnea,
and asthmatic wheezing. €
Classical features of lymphatic fi liariasis are absent
SUBCUTANEOUS FILARIASIS
Loa Loa Common name: African eye worm, loiasis The disease is
endemic in central and West Africa. where about 10 million people are
effected.
Morphology
The adult worm is thin and transparent, measuring about 30–70 mm in
length and 0.3–0.5 mm in thickness.
In infected persons, they live in the subcutaneous tissues through which
they wander. They may also occur in the sub conjunctival tissues.
Adults live for 4–17 years.

34
Microfilaria
The microfilariae are sheathed with column of nuclei extending
completely to the tip of the tail.
They appear in peripheral circulation only during the
day from 12 noon to 2 pm (diurnal periodicity
Life cycle
life cycle is completed in two hosts.
Definitive host: Man
Intermediate host or vectors: Day biting flies (mango flies)
Infective stage - third-stage larvae.
Infection is transmitted to man through the bite of infected vecters during
their blood meal.
The infective third stage larvae enter the subcutaneous tissue, moult then
develop into mature adult worm over 6–12 months in subcutaneous
tissues.
Female worms produce sheathed microfilaria which have diurnal
periodicity.
The microfilaria are ingested by vecters during its blood meal.
They cast off their sheaths, penetrate the stomach wall and reach thoracic
muscles where they develop into infective larvae with in 10 days.
35
Pathogenesis and clinical features:
There is no inflammatory response to the micofilariae or the adults, but
a hypersensitivity reaction causes transient localized, non -erythematous,
subcutaneous edema(Calabar swelling) .
Ocular manifestations range from photophobia to gradual blurring of
vision, progressing to total blindness. lesions may develop in all parts of
the eye.
The most common early finding is conjunctivitis with photophobia.
Other ocular lesions include keratitis, secondary glaucoma,
choroidoretinitis, and optic atrophy.
Other Complications like nephropathy, encephalopathy, and
cardiomyopathy can occur but are rare

36
Treatment:
Diethylcarbamazine eliminates the microfilariae and may kill the
adults.
Worms in the eye require surgical excision
diagnosis
Microfilariae may be shown in peripheral blood collected during the day.
The adult worm can be demonstrated by removal from the skin or
conjunctiva or from a subcutaneous biopsy specimen from a site of
swelling.
High eosinophil count is common
SEROUS CAVITY FILARIASIS
Mansonella Ozzardi
M. Ozzardi is a new world filaria seen only in Central and South America
and the West Indies.
The adult worms are found in the peritoneal and pleural cavities of
humans.
The non periodic unsheathed microfilariae are found in the blood.
Culicoides species are the vectors.
Infection does not cause any illness.
Diagnosis is made by demonstrating microfi lariae in blood
Ivermectin (single dose 6 mg) is eff ective in treatment.
in pericardium.
Mansonella Perstans
Also known as Acanthocheilonema, Dipetalonema, or Tetrapetalonema
perstans.

37
the worm is extensively distributed in tropical Africa and coastal South
America.
The adult worms live in the body cavities of humans, mainly in
peritoneum, less in pericardium.
The microfi lariae are unsheathed and subperiodic.
Vectors are Culicoides species.
Diagnosis is by demonstration of the microfi lariae in peripheral blood or
serosal effusion.
Doxycycline (200 mg twice a day for 6 weeks)
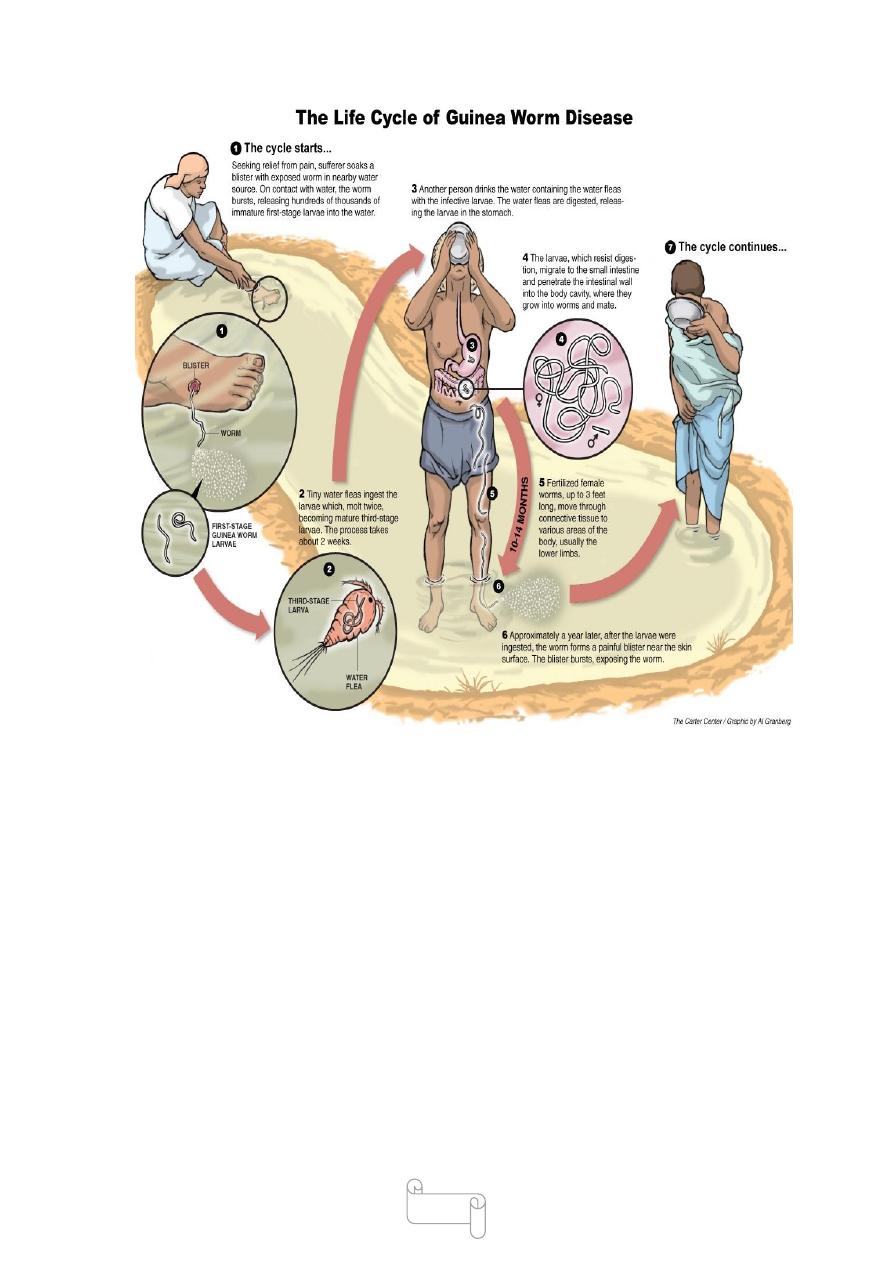
Dracunculus Medinensis
Common name: Guinea Worm
The worm was present in tropical Africa, the Middle-East
in Iraq, Iran, and in Pakistan and India.
About 50 million people were estimated to be infected with the worm.
D. medinensis causes dracunculiasis or dracunculosis.
.
The disease still remains endemic in 13 African countries
including Sudan (highest incidence), Niger, etc
Morphology
The adult female is a long, cylindrical worm with smooth milky-white in
colour.
It has a blunt anterior end and a tapering recurved tail
It measures about (60–120 cm) in length and 1–2 mm in thickness
The body of the gravid female uterus containing about 3million
embryos ,the female worm is viviparous.
The male worm, which is rarely seen, is much smaller than female being
10–40 mm long and 0.4 mm thick. Female worm survives for about an
38
year. life span of male worm is not more than 6months. The larva
measures 500–750 µm in length and 15–25 µm thick
Life Cycle
life cycle need two hosts.
Defi nitive host: Man
Habitat in cutaneous and subcutaneous tissues
Intermediate host: Cyclops, in which embryos undergo developmental
changes. There is no animal reservoir.
Infective form: Third-stage larva present in the hemocele
of infected cyclops.
Mode of transmission: Humans get infected by drinking unfiltered water
containing infected cyclops with third –stage larva .
Incubation period: about one year
39
Pathogenicity and Clinical Features
Infection induces no illness till the gravid female worm comes to lie
under the skin, ready to discharge its embryos.
The body fluid of the adult worm is toxic and leads to
blister formation.
A few hours before the development of the blister, there may be
constitutional symptoms such as nausea, vomiting, intense pruritus, and
urticarial rash.
The blister develops initially as a reddish papule with a vesicular center .
40
The most common sites for blister formation are the feet between the
metatarsal bones or on the ankles.
Secondary bacterial infection is frequent. Sometimes, it may lead to
tetanus.
Sometimes, the worm travels to unusual sites such as the pericardium,
the spinal canal, or the eyes, with sever effects
Diagnosis
Detection of adult worm and larval form in ulcer.
Demonstration of dead worm by X-ray.
Serology–ELISA and IFA
Skin test: An intradermal test with guinea worm antigen
elicits positive response.
Treatment
Antihistaminics and steroids are of help in the initial
stage of allergic reaction.
Metronidazole, niridazole, and thiabendazole are useful in treatment .
Surgical removal of the worm under anaesthesia
د
1
سعيد حميد
Helminthes (Cestodes)
Classification of Cestodes
-Phylum Platyhelminthes .
- class Cestoidea.
41
The class Cestoidea includes 2 orders:
1-Pseudophyllidea
2-Cyclophyllidea
Cestodes in (Greek kestos—girdle or ribbon) are multisegmented,
dorsoventrally flattened tapelike worms sizes vary from a few millimeters
to several meters
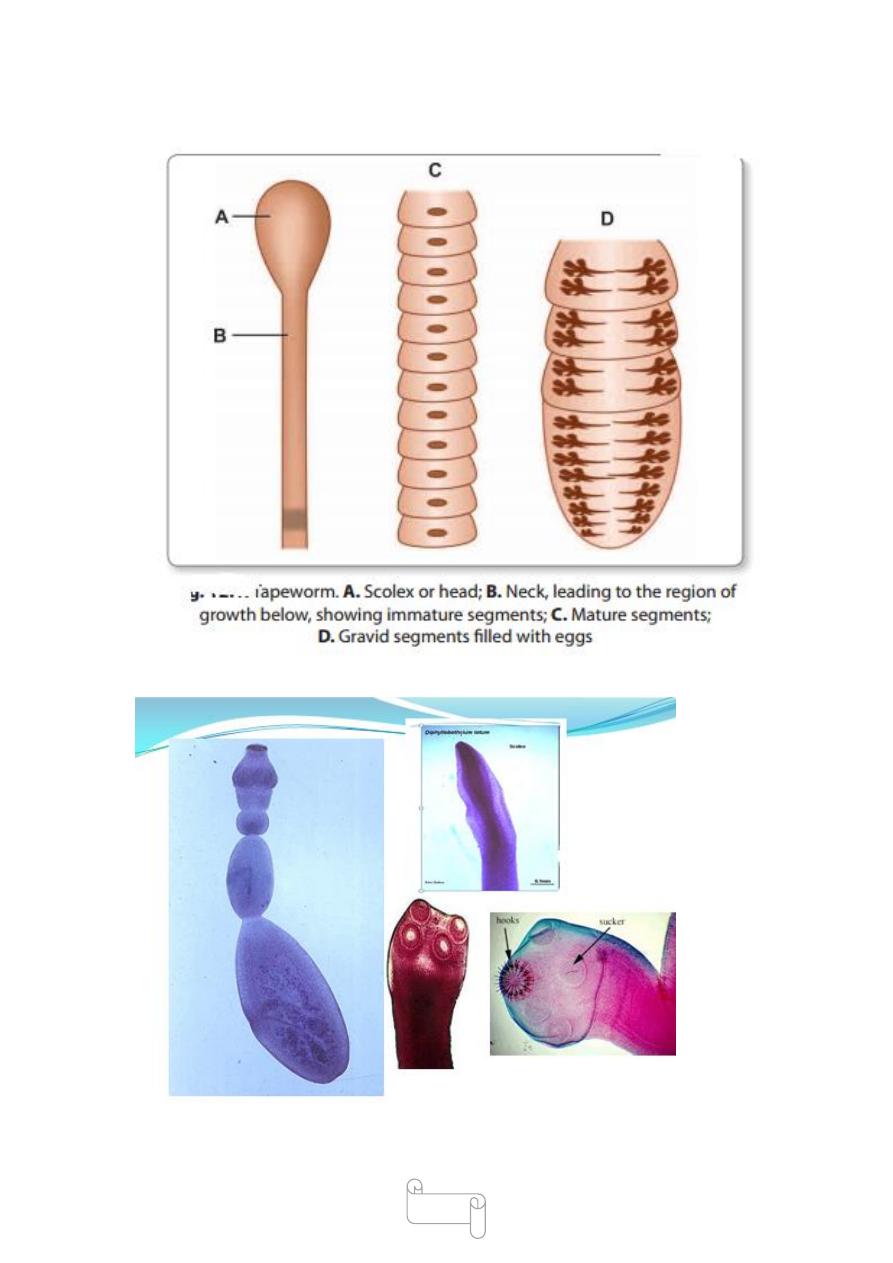
The adult worm consists of 3 parts:
€ 1- Head (scolex)
€ 2-Neck
€ 3-Trunk (strobila)
Head (Scolex) It is the organ of attachment to the intestinal mucosa of the
definitive host .
In the order cyclophyllidea
the scolex possesses 4 suckers(or acetabula). In some cyclophyllidea
like Taenia solium, scolex has an apical protrusion called as
the rostellum.
The rostellum may or may not be armed with hooks.
In the order pseudophyllidea.
the scolex does not possess suckers but possesses a pair of longitudinal
grooves called as bothria,by which it attaches to the intestine mucosa of
the host
42
43
Neck
It is the part, immediately behind the head and is the region of growth
from where the segments of the body (proglottids) are being generated
continuously.
Trunk (strobila)
The trunk also called as strobilais composed of a chain of
Proglottids or segments.
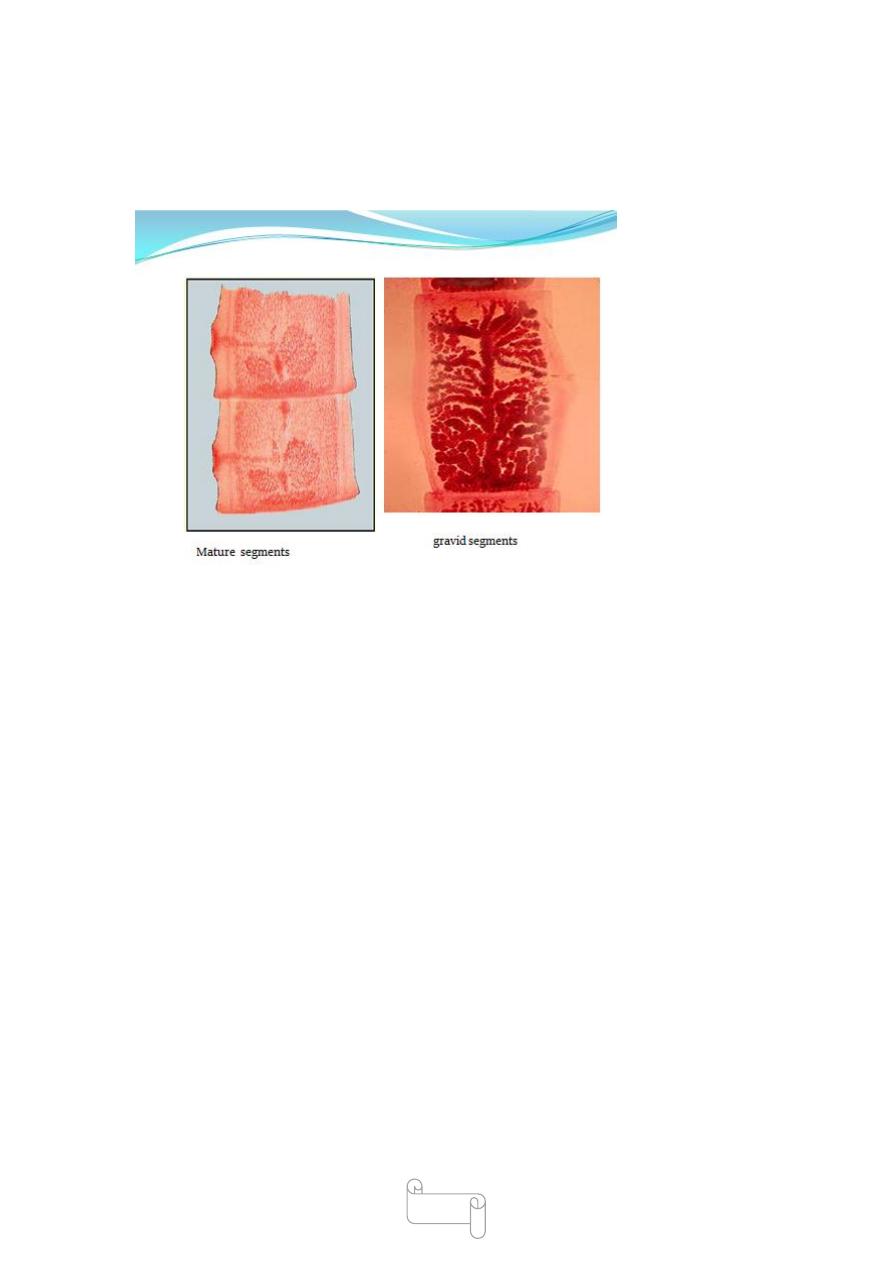
The proglottids
- immature segments.
- mature segments.
- gravid segments.
44
Tapeworms are hermaphrodites ,mature segment contains both male and
female sex organs.
In the immature segments, the reproductive organs are not well
developed.
They are well developed in the mature segments.
The gravid segments are completely occupied by the uterus filled with
eggs.
Tapeworms do not have a body cavity or alimentary canal
Rudimentary excretory and nervous systems are present.
Tape worm is a hermaphrodite. There is one complete set of male and
female organs for each
proglottids
egg
The embryo inside the egg is called the oncosphere
(meaning ‘hooked ball’) because it is spherical and has
hooklets.
Oncospheres of human tapeworms typically have 3
45
pairs of hooklets and so, are called hexacanth(meaning
6-hooked) embryos.
Cestodes complete their life cycle in 2 different hosts.
Exceptions are:
Hymenolepis nana that requires only 1 host, man .
Diphyllobothrium latum that requires 3 hosts.
- definitive host: man.
-first intermediate host: cyclops.
-second intermediate host: fish
46
د. سعيد
طفيليات
82
\
3
\
8102
( عدد االوراق
0
) م
\
3
\
موصل ملحك محاضرة
lec: 6
Treatment
diethyl carbamazine (DEC ) is the drug of choice. It is given orally in a
dose of 6 mg/ kg body weight daily for a period of 12 days amounting to
a total of 72 mg of DEC per kg of body weight.
It has both macro- and micro-fi laricidal properties
The administration of DEC can be carried out in 3 ways.
1. Mass therapy:
The dose recommended is 6 mg/kg body weight.
In some countries it is used alone and in some, with albendazole or
ivermectin. Mass therapy is indicated in highly endemic areas
2. Selective treatment: The recommended dose in the Indian
programme is DEC 6 mg/kg of body weight daily for 12 doses, to be
completed in 2 weeks. In endemic areas, treatment must be repeated
every 2 years.
3. DEC medicated salts: Common salt medicated with
1–4 g of DEC per kg has been used for fi lariasis control .
Ivermectin: In doses of 200 µg/kg can kill the microfi lariae but has no
eff ect on adults.
Tetracyclines: Also have an eff ect in the treatment of fi lariasis

47
Supportive Treatment
Chronic condition may not be curable by antifi larial drugs and require
other measures like elevation of the aff ected limb, use of elastic
bandage, and local foot care reduce some of the symptoms of
elephantiasis.
Surgery is required for hydrocele.
Medical management includes bed rest, high protein diet with
exclusion of fat, drug therapy with DEC, and use of abdominal binders.
Surgical management of refractory case includes endoscopic
sclerotherapy using silver nitrate
Prophylaxis
The 2 major measures in prevention and control of fi lariasis
are
i. Eradication of the vector mosquito
ii. Detection and treatment of carriers.
Eradication of Vector Mosquito
Antilarval measures: The ideal method of vector control would be
elimination of breeding places by providing adequate sanitation
underground waste and water disposal system. €
Chemical control: Using antilarval chemicals like Mosquito larvicidal oil,
Pyrosene oil,Organophosphorous larvicides like temephos, fenthion etc.
€
Antiadult measures: Adult mosquitoes can be restricted by use of DDT,
dieldrin, and pyrethrum.
Personal prophylaxis: Using mosquito nets and mosquito repellants is
the best method.
Detection and Treatment of Carriers
The recommended treatment is DEC 6 mg per kg body weight daily for
12 days, the drug being given for 2 weeks, 6 days in a week
48
د. سعيد طفيليات
82
\
3
\
8102
( عدد االوراق
01
) م
\
3
\
موصل
lec:7+8
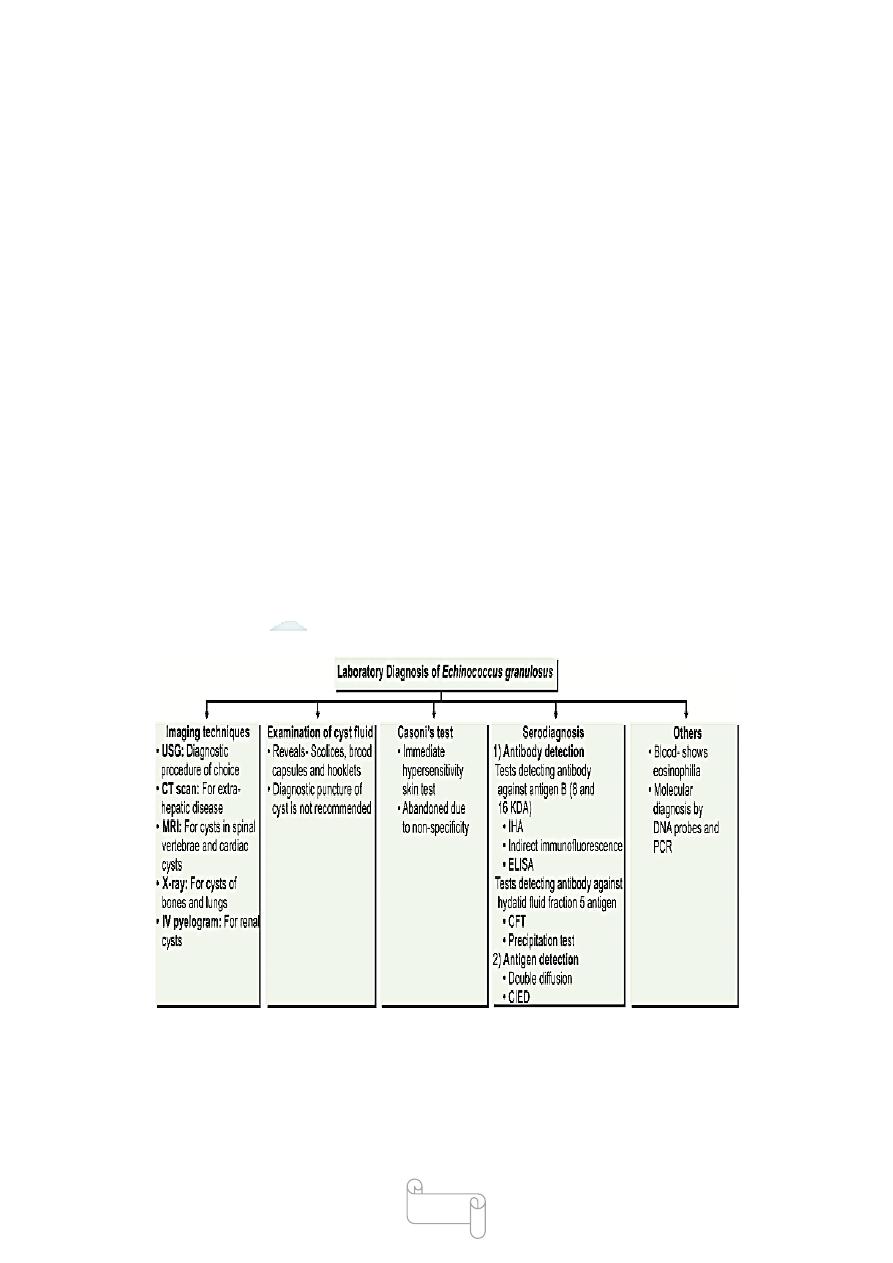
Echinococcus species
Four Echinococcus species
• Echinococcus granulosus : Hydatid disease
49
• Echinococcus multilocularis : Alveolar or multilocular hydatid disease
• Echinococcus vogeli and Echinococcus oligarthrus : Polycystic hydatid
disease
Echinococcus granulosus
Common name: dog tape worm, hydatid tape worm.
Disease: unilocular hydatid disease.
Hydatid disease also known as Echinococcosis or hydatidosis is caused
by infection with larva (meta cestode) of the tapeworm of the genus
Echinococcus
(Family Taenidae, Order Cyclophyllidea, Class Cestoda, Phylum
Platyhelminths).
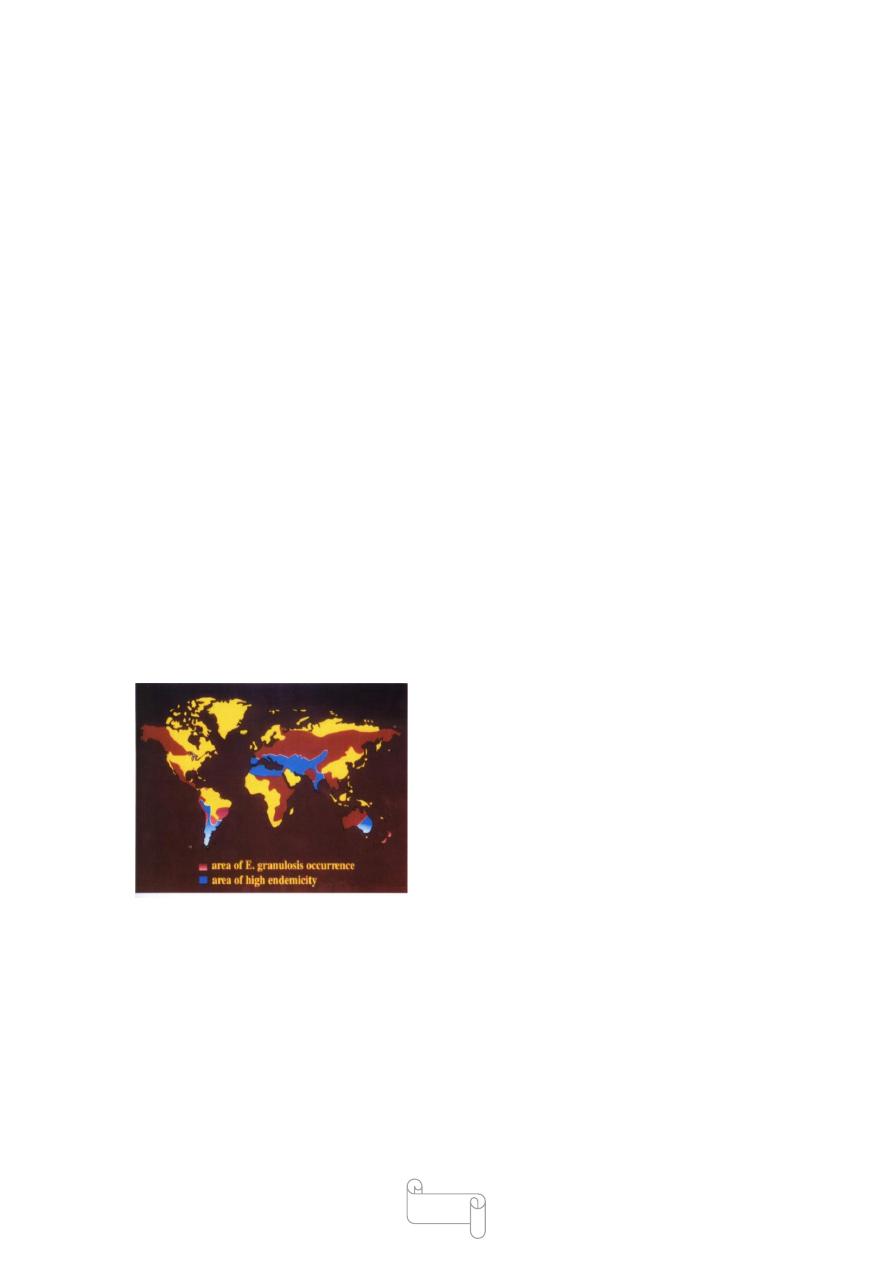
The disease is endemic in many parts of the world specially middle east (
include Iraq ), Australia, New Zealand, South America, Central and South
Europe
Geographical distribution of cystic hydatid disease
Morphology
Adult Worm
It is a small tapeworm, measuring only 3–6 mm in length.
It consists of a scolex, a short neck, and strobila.

50
The scolex is pyriform,with 4 suckers and a prominent rostellum bearing
2 circular rows of hooklets (25–30)
The neck is short than the rest of the worm .
The strobila is composed of only 3 proglottids, the anterior immature, the
middle mature, and the posterior gravid segment
The terminal proglottid is longer and wider than the rest
of the worm and contains a branched uterus filled with 500eggs.
51
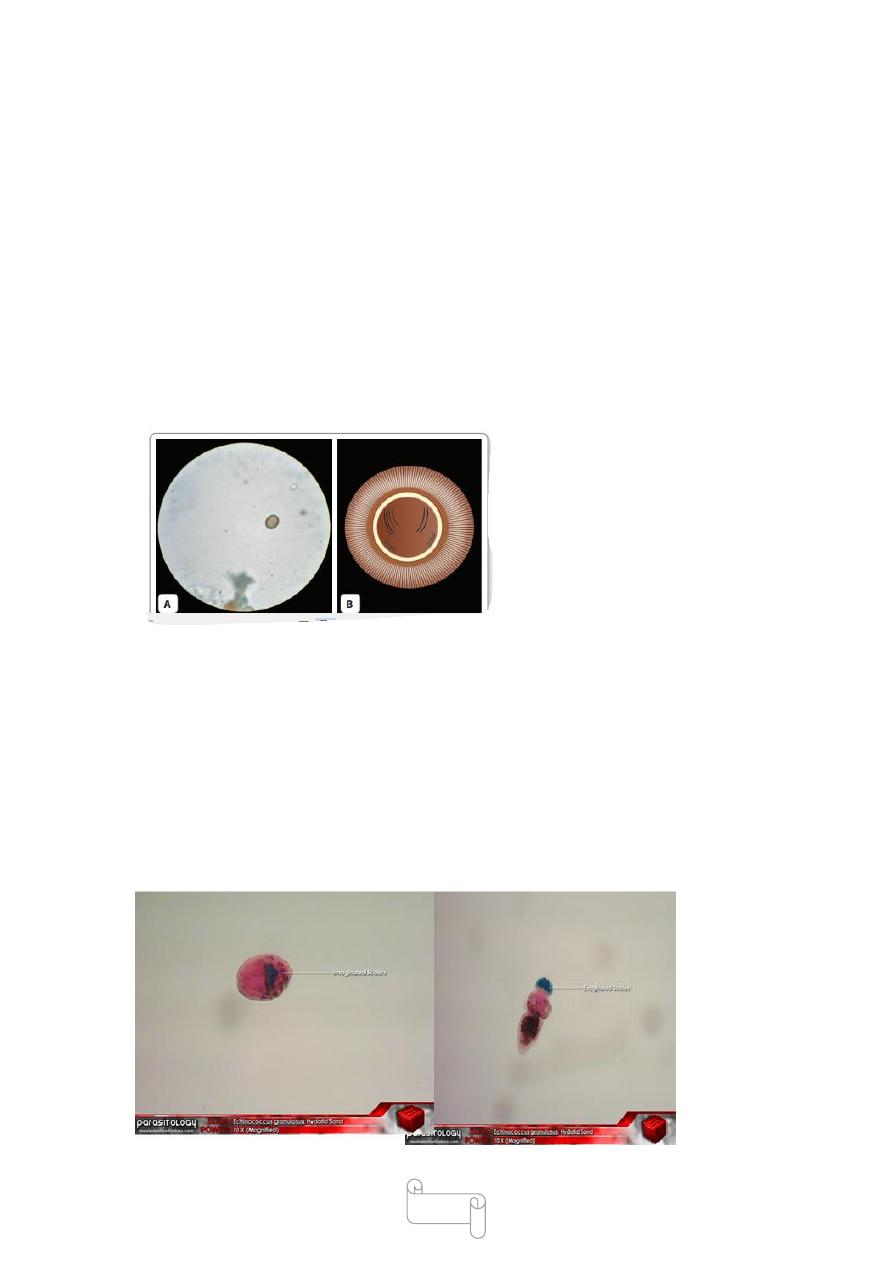
Eggs
The egg is spherical, measuring 30–40 µm in diameter.
It has a thin hyaline embryonic membrane around it.
The inner embryophore is radially
striated and is yellowbrown
due to bile staining
In the center is a fullydeveloped
embryo(oncosphere) with 3 pairs of hooklets (hexacanth embryo).
Larval Form
The larval form is found within the hydatid cyst developing
inside various organs of the intermediate host.
It represents the structure of the scolex of adult worm and remains
invaginated within a vesicular body.
After entering the definitive host, the scolex with suckers and rostellar
hooklets, becomes exvaginated and develops into adult worm.

52
Mode of Transmission
Transmission of E. granulosus to humans is affected by such factors as
prevalence of the parasite in domestic dogs, behavior of humans towards
dogs, immunological and genetic factors .
Direct contact between human and dogs .
Indirect transmission via water sources and vegetable, contaminated by
E. granulcosus eggs deposited by infected dogs may be the most
important route of transmission to humans .
Flies may also be implicated in transmission of the disease
Direct transmission of E. granulcosus from human to human does not
occur
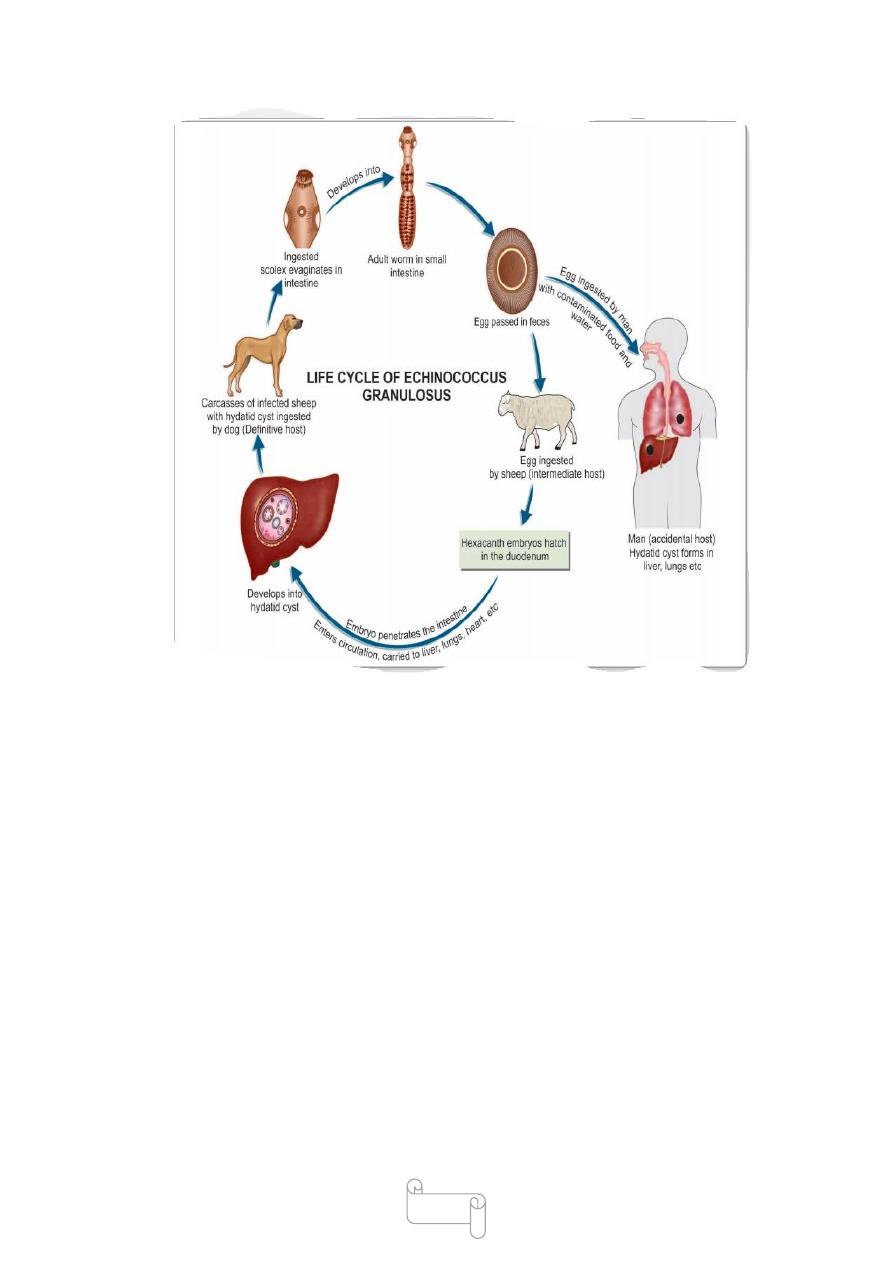
Life Cycle
The worm completes its life cycle in 2 hosts
Definitive hosts: Dog (optimal host), wolf, and fox
Intermediate host: Sheep and Cattle. (Sheep is the ideal intermediate
host).
€
Man acts as an accidental intermediate host (dead end).
€ The adult worm lives in the small intestine of dogs and other canine
animals. These animals discharge numerous eggs in the feces,the
intermediate hosts (sheep and cattle) ingest them while grazing.
Human infection follows ingestion of the eggs due to intimate handling of
infected dogs or by eating raw vegetables or other food items
contaminated with dog feces.
The ova ingested by man or by sheep and cattle are liberated from the
chitinous wall by gastric juice liberating the hexacanth embryos which
penetrate
the intestinal wall and enter the portal venules, to be carried to the liver
along the portal circulation.

53
These are trapped in hepatic sinusoids, where they eventually develop
into hydatid cyst.
About 65% of hydatid cyst develop in liver, which acts as the first filter
for embryo.
However, some embryo which pass through the liver, enter the right side
of heart and are caught in pulmonary capillaries(forming pulmonary
hydatid cysts 15% ), so that the lung acts as the second filter.
A few embryo enter the systemic circulation and get lodged in various
other organs and tissues such as the spleen, kidneys, eyes, brain, or bones.
The hydatid cyst may be present in any tissue except hair, nail
When sheep or cattle harboring hydatid cysts die or are slaughtered, dogs
may feed on the carcass or offal. Dogs are infected by ingesting
protoscoleces in the fertile hydatid cyst in viscera of intermediate host
specially sheep, goat, cattle and camel
Inside the intestine of dogs, the scolices develop into the adult worms in
about 6-7 week and produce eggs to repeat the life cycle .
One dog may have up to 17120 adult worms.
The adult worm lives from 6-30 month
When infection occurs in humans accidentaly, the cycle comes to a dead
end because the human hydatid cysts are unlikely to be eaten by dogs
54
Pathogenesis
At the site of deposition, the embryo slowly develops into a hollow
bladder or cyst filled with fluid. This becomes the hydatid cyst (Greek
hydatis: a drop of water).
the hydatid cyst enlarges slowly and reaches a diameter of 0.5–1 cm in
about 6 months. The growing cyst evokes host tissue reaction leading to
the deposition of fibrous capsule around it.
The cyst wall secreted by the embryo consists of 3 indistinguishable
layers.
€
Pericyst is the outer host inflammatory reaction consisting of fibroblastic
proliferation, mononuclear cells, eosinophils, and giants cells, eventually
developing into dense fibrous capsule which may even calcify.
€
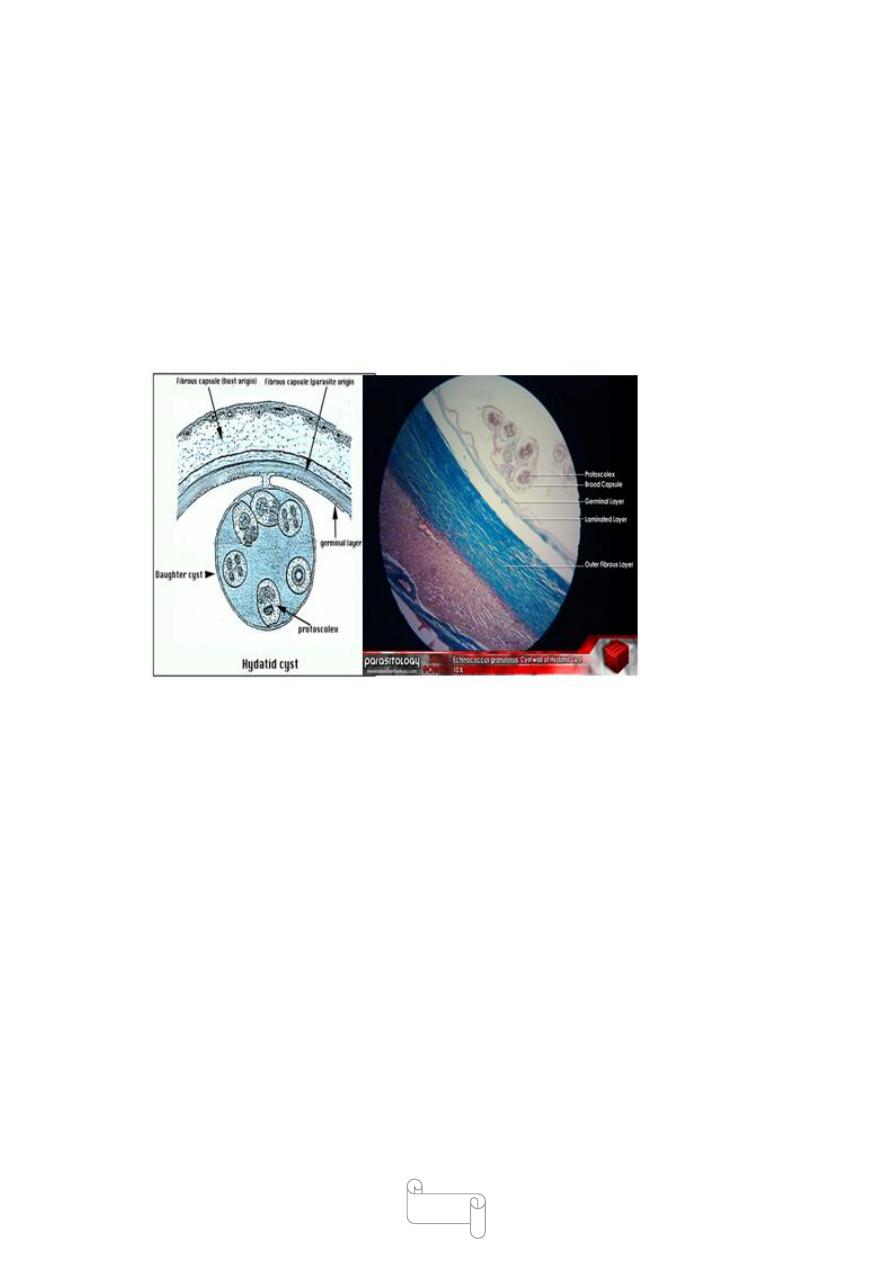
55
Ectocyst is the intermediate layer composed of characteristic a cellular,
chitinous, laminated hyaline material. It has the appearance of the white
of a hard boiled egg.
Endocyst is the inner germinal layer which is cellular and consists of
number of nuclei embedded in a protoplasmic mass and is extremly thin .
The germinal layer is the vital layer of the cyst and is the site of asexual
reproduction giving rise to brood capsules with scolices. It also secretes
hydatid fluid, which fills the cyst.
Hydatid fluid: The interior of the cyst is filled with a clear colorless or
pale yellow fluid called as hydatid fluid.
hydatid fluid :It contains salts (sodium chloride 0.5%, sodium sulphate,
sodium phosphate, and salts of succinic acid) and proteins.
The fluid was used as the antigen for Casoni’s intradermal test.
A granular deposit or hydatid sand is found at the bottom of the cyst,
consisting of free brood capsules and protoscolices and loose hooklets.

56
Brood capsules
Which have only the germinal layer , containing protoscolices They are
initially attached to the germinal layer by a stalk, but later escape free into
the fluidfilled cyst cavity ,
From the inner wall of the brood capsules, protoscolices (new larvae)
develop, which represent the head of the potential worm, complete with
invaginated scolex,
Several thousands of protoscolices develop into a mature hydatid cyst, so
that this represents an asexual reproduction bearing suckers and hooklets
Inside mature hydatid cysts, further generation of cyst, daughter cysts
and grand-daughter cysts may develop. which are replicas of the mother
cysts .
The cyst grows slowly often taking 20 years or more to become big
enough to cause clinical illness
57
Acephalocysts
Some cysts are sterile and may never produce brood capsules, while some
brood capsule may not produce scolices. These are called acephalocysts.
Fate of hydatid cysts
The cyst may get calcified or spontaneously evacuated following
inflammatory reaction. Hydatid cyst of liver may rupture into lung or
other body cavity producing disseminated hydatid lesions
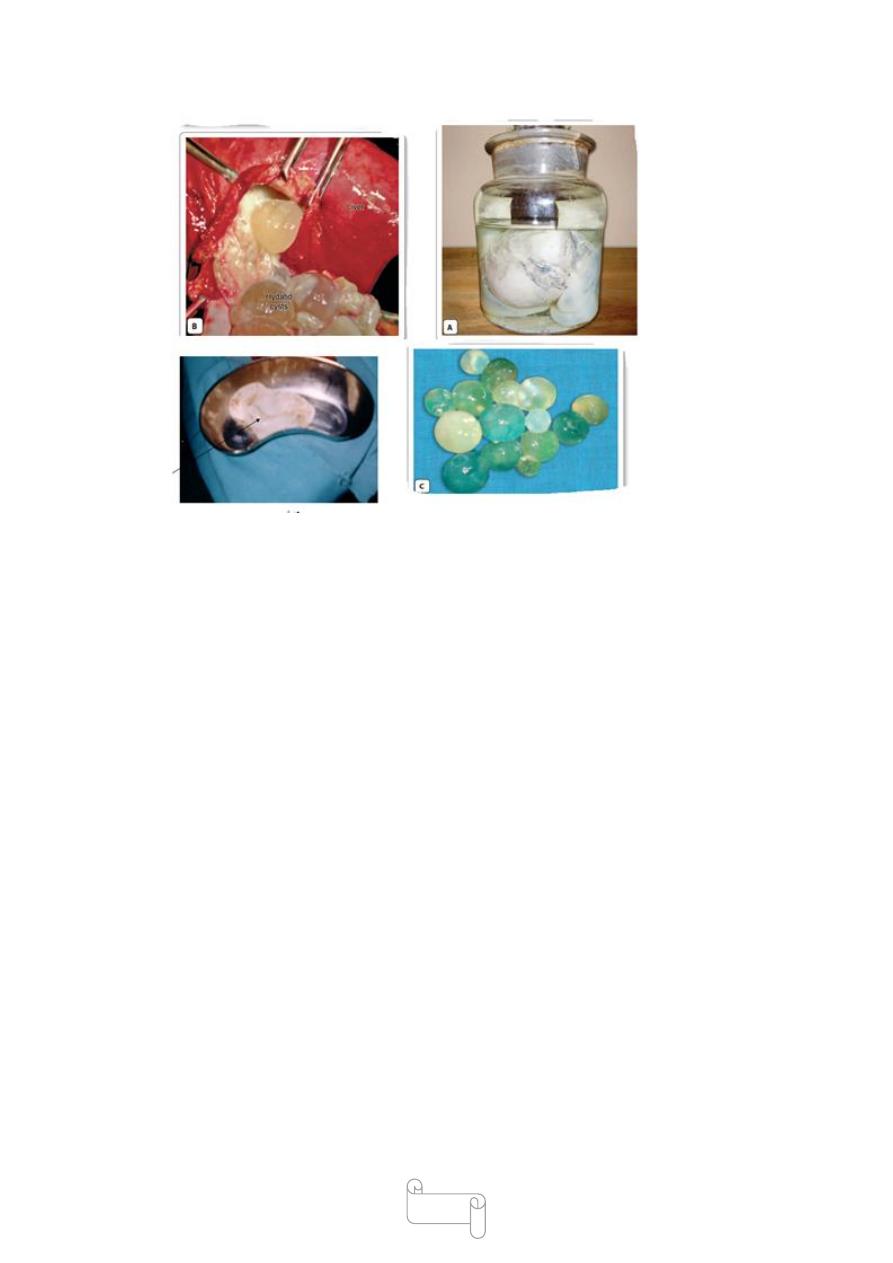
Clinical Features
Most of the times infection is asymptomatic and accidentally
discovered.
Clinical disease develops only when the hydatid cyst has grown big
enough to cause obstructive symptoms. Disease results mainly from
pressure effects caused by the enlarging cysts.
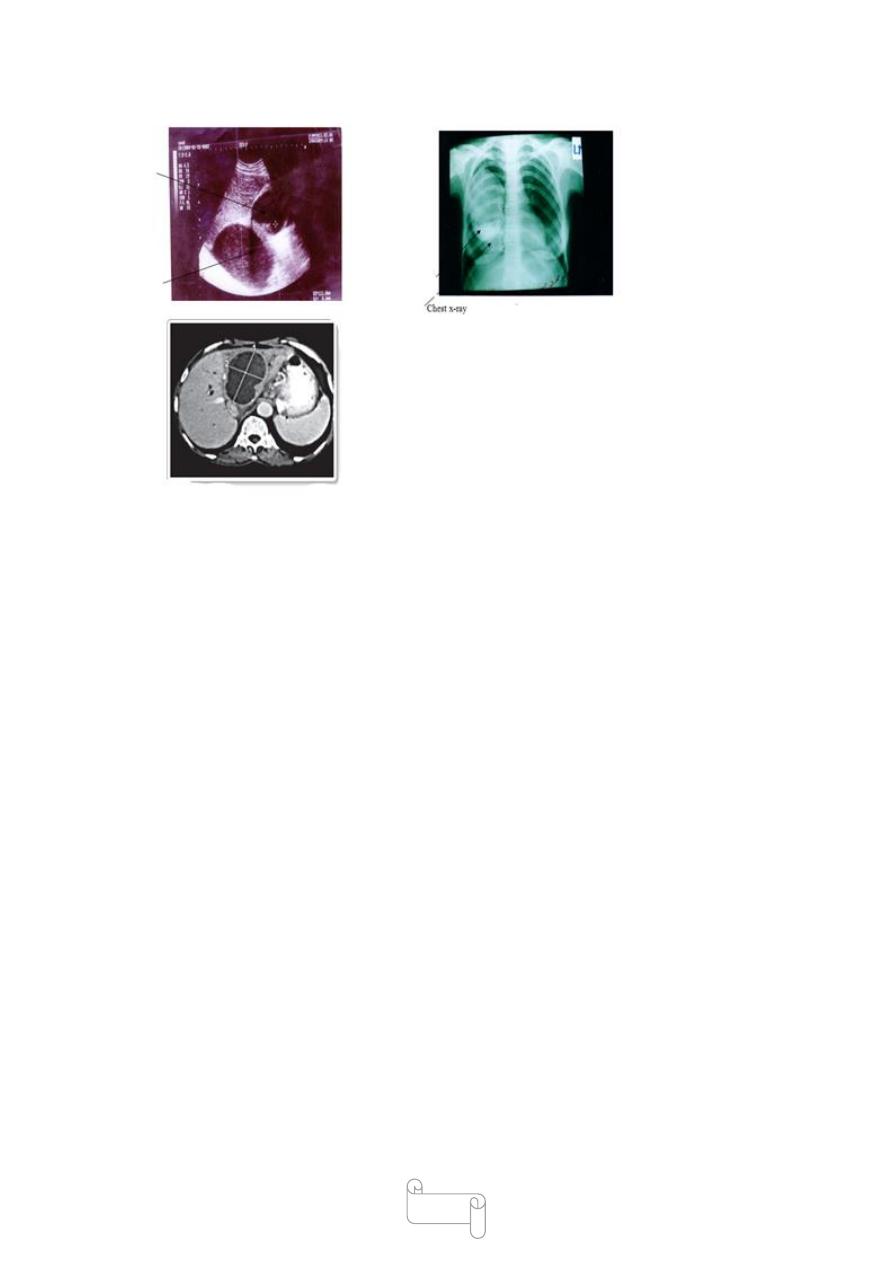
the primary hydatid cyst occurs in liver(65%) , mostly in the right lobe.
Hepatomegaly, pain, and obstructive jaundice are the usual
mainfestations.
The next common site is the lung(15%) (most common being the lower
lobe of the right lung). Cough, haemoptysis, chest pain, pneumothorax,
and dyspnea constitute the clinical picture.
58
In the kidney (2%), hydatid cyst causes pain and haematuria.
Other sites affected include spleen (1%), brain (1%), pelvic organs, orbit,
and bones (3%).
Cerebral hydatid cysts may present as focal epilepsy.
€
When hydatid cyst is formed inside the bones, the laminated layer is not
well developed . This is called osseous hydatid cyst. Erosion of bone may
lead to pathological fractures.
hypersensitivity to the echinococcal antigen.
The Hypersensitivity may cause urticaria.
But if a hydatid cyst ruptures spontaneously or during surgical
interference, massive release of hydatid fluid may cause severe, even
fatal anaphylaxis.
59
Treatment
Traditionally surgical removal was considered as the the
best mode of treatment of cysts. Currently, ultrasound
staging is recommended and management depends on the
stage.
In early stages, the treatment of choice is punture, aspiration, injection,
and reaspiration (PAIR).
(PAIR) Scolicidal agents and their complications
• Cetrimide—can cause acidosis
• Alcohol 95%—can cause cholangitis
• Hypertonic saline—hypernatraemia
• Sodium hypochlorite—hypernataraemia
Note: In cases with biliary communication only hypertonic
saline (15–20%) is used

60
Surgery
It is the treatment of choice for complicated E. granulosus
cysts
like those communicating with the biliary tract and in those cysts where
PAIR is not possible.
Recurrence after surgery is common.
Preand postoperative chemotherapy with albendazole
for 2 years after curative surgery is recommended .
Other new treatment modalities include .
1-laparoscopic hydatid liver surgery .
2-percutaneous thermal ablation (PTA) of the germinal layer of the cyst
using radiofrequency ablation device.
Chemotherapy
Chemotherapy with benzimidazole agents are restricted to
residual, postsurgical, and inoperable cysts.
Albendazole and praziquantel have proved beneficial
Prophylaxis
. Echinococcus granulosus infection can be prevented by
-Ensuring pet dogs do not eat animal carcass or offal.
-Periodical deworming of pet dogs.
- Destruction of stray and infected dogs.
-Mantaining personal hygiene such as washing of hands
after touching dogs and avoidance of kissing pet dogs

61
Echinococcus Multilocularis
causes rare but serious condition of alveolar or multilocular hydatid
disease in humans.
It is found in the northern parts of the world, from Siberia in the East to
Canada in the West.
The adult worm is smaller than E. granulosus and lives in the intestines
of foxes, dogs, and cats which are the definitive host.
Rodents are the main intermediate hosts.
Human infection develops from eating fruits or vegetables contaminated
with their feces.
E. multilocularis leads to multilocular hydatid cyst
The liver is the most commonly affected organ. The multilocular
infiltrating lesion appears like a grossly invasive growth, without any
fluid or free brood capsule or scolices which can be mistaken for a
malignant tumor
Patients present with upper quadrant and epigastric pain. Liver
enlargement and obstructive jaundice may also be present. It may also
metastasize to the spleen, lungs, and brain in 2% cases.
The prognosis is very bad if untreated,
Surgical resection, when possible, is the best method of treatment.
Albendazole therapy is recommended for 2 years after curative surgery.
In those cases, where surgery is not possible, treatment with albendazole
is recommended.
Hydatid cyst of Echinococcus vogeli
Disease: Polycystic hydatid disease .
Habitat: in the small intestine of bush dog (definitive host) in latin
America.
Rodent (natural intermediate host).

62
Morphology:
Adult differs from E. granulosus in greater length 3.9 - 5.6 mm
Polycystic hydatid: is alveolar in characters but less than that of E.
multilocularis,
so it is intermediate between cystic and alveolar hydatid disease, present
like a mass of tumor in the liver
lec:8
CYCLOPHYLLIDEAN TAPEWORMS
د
1
سعيد
حميد
Taenia Saginata and Taenia Solium
Common name
Taenia saginata Beef tapeworm
Taenia solium Pork tapeworm .
The name Taeniais derived from the Greek word meaning tape or band.
T. saginata is worldwide in distribution, but the infection
is not found in vegetarians and those who do not eat beef .
T. Solium is also worldwide in distribution except in the
countries and communities, which proscribe pork as
taboo.
Cestodes living in small intestine
• Diphyllobothrium latum
• Taenia solium
• Taenia saginata
• Hymenolepis nana

63
Habitat
The adult worms of both T. saginata and T. solium live in the small
intestine, commonly in the jejunum.
Morphology
Adult Worm of T. saginata
The adult T. saginata worm is white in color, ribbonlike, dorsoventrally
flattended, and segmented, measuring 5–10 meter in length.
The adult worm consists of head (scolex), neck, and strobila (body).
The general features of adult worm are similar to any cyclophyllidean
cestodes.
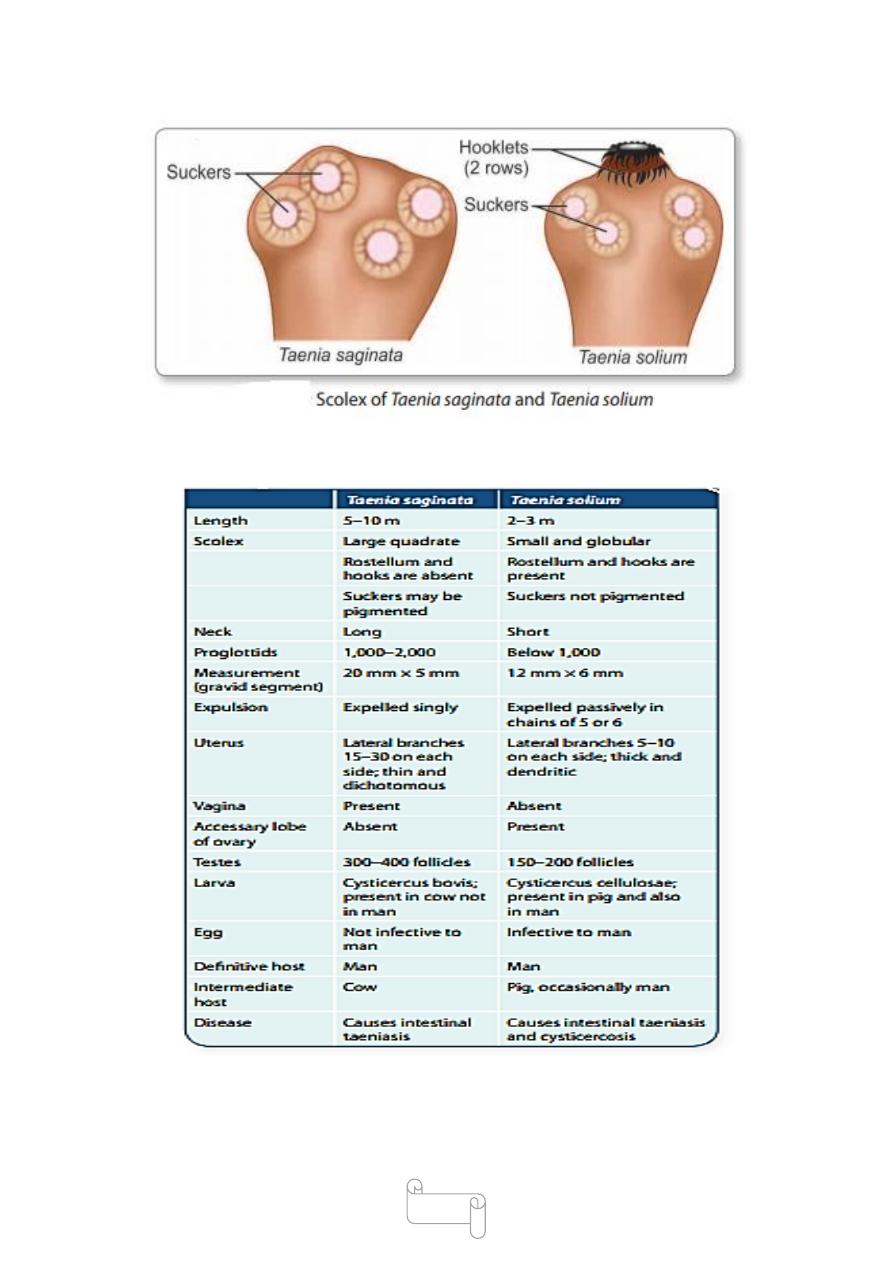
Scolex:The scolex (head) of T. saginata is about 1–2 mm in diameter,
quadrate in crosssection, bearing 4 hemispherical suckers situated at its
four angles.
The scolex has no rostellum or hooklets (which are present in T. solium)
T. saginata is, therefore called the unarmed tape worm.The suckers serve
as
the sole organ for attachment

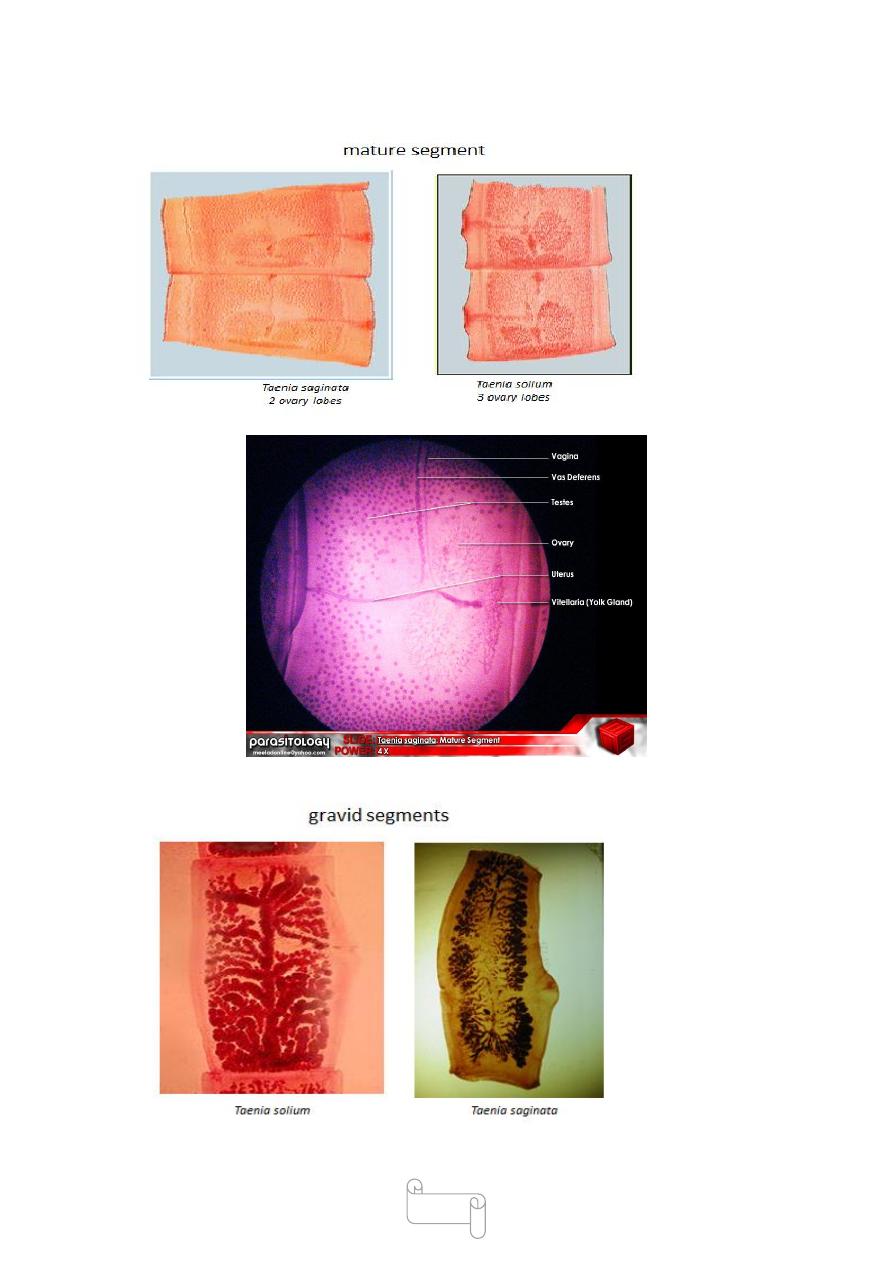
64
The neck is long and narrow.
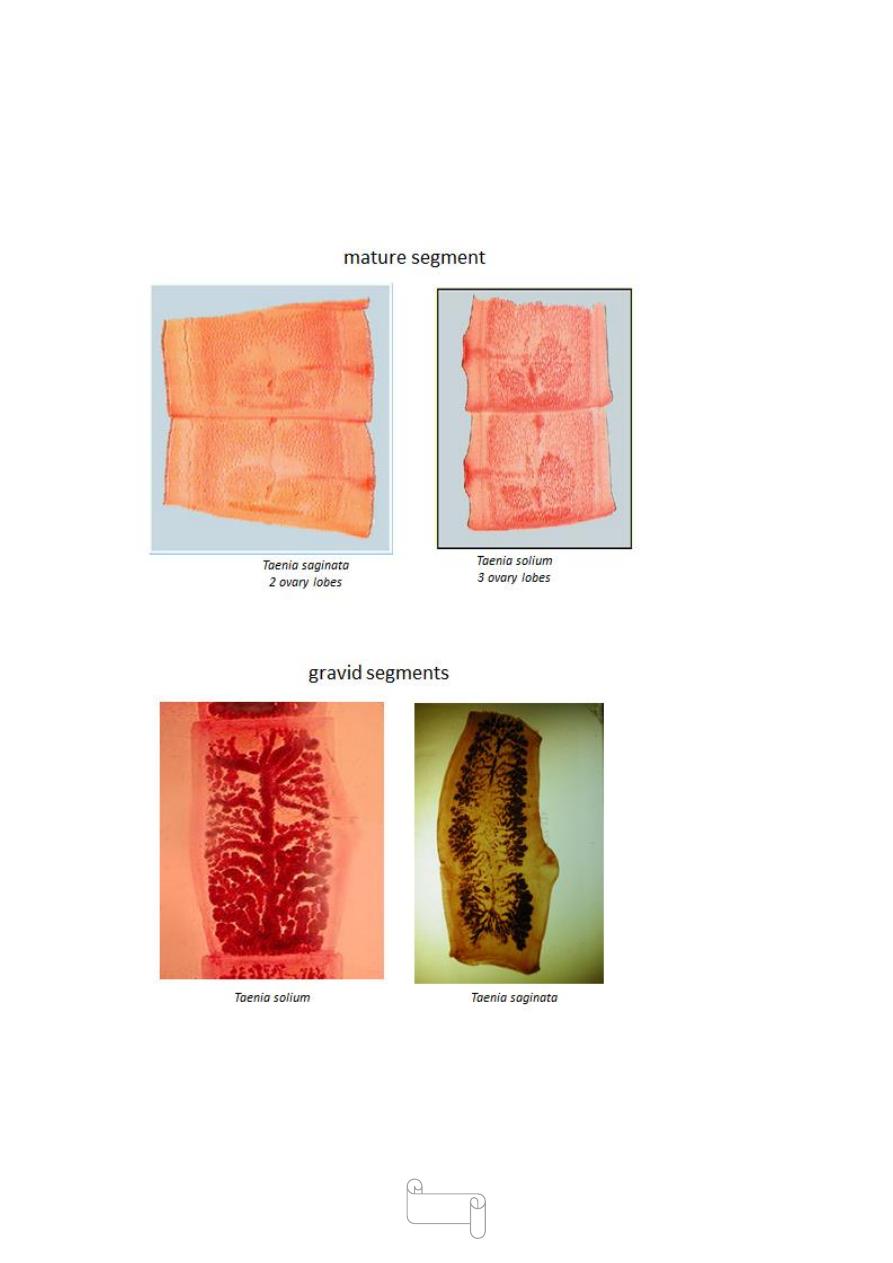
The strobila (trunk) consists of 1000 to 2000 proglottides or segments—
immature, mature and gravid.
The gravid segments are nearly about 20 mm long and 5 mm broad.
The segment contains male and female reproductive structures.
The testes are numerous, 300 to 400 (twice as many as in T. solium).
The gravid segment has 15 to 30 lateral branches (as against 7 to 13 in T.
solium). It differs from T. solium also in having a prominent vaginal
sphincter and in lacking the accessory ovarian lobe. The common genital
pore opens on the lateral wall of the segments.
The gravid segments break away and are expelled singly, actively
forcing their way out through the anal sphincter.
As there is no uterine opening, the eggs escape from the
uterus through its ruptured wall.
Adult Worm of T. solium
The adult worm is usually 23 meters long.
The proglottides number less than a thousand. They resemble those of T.
saginata in general
The scolex of T. solium is small and globular about 1 mm in diameter,
with 4 large cuplike suckers (0.5 mm in diameter), and a conspicuous
rounded rostellum, armed with a double row of alternating round and
small dagger-shaped hooks, 20–50 in number.
The neck is short .
The gravid segments are twice as long as broad, 12 mm by 6 mm.
The testes are composed of 150 to 200 follicles. There is an accessory
lobe for the ovary. The vaginal sphincteris absent.
The uterus has only 5 to 10 (under 13) thick lateral branches. A lateral
thicklipped genital pore is present, alternating between the right and left
sides of adjacent segments.
65
The gravid segments are not expelled singly, but pass passively out as
short chains. The eggs escape from the ruptured wall of the uterus.
66
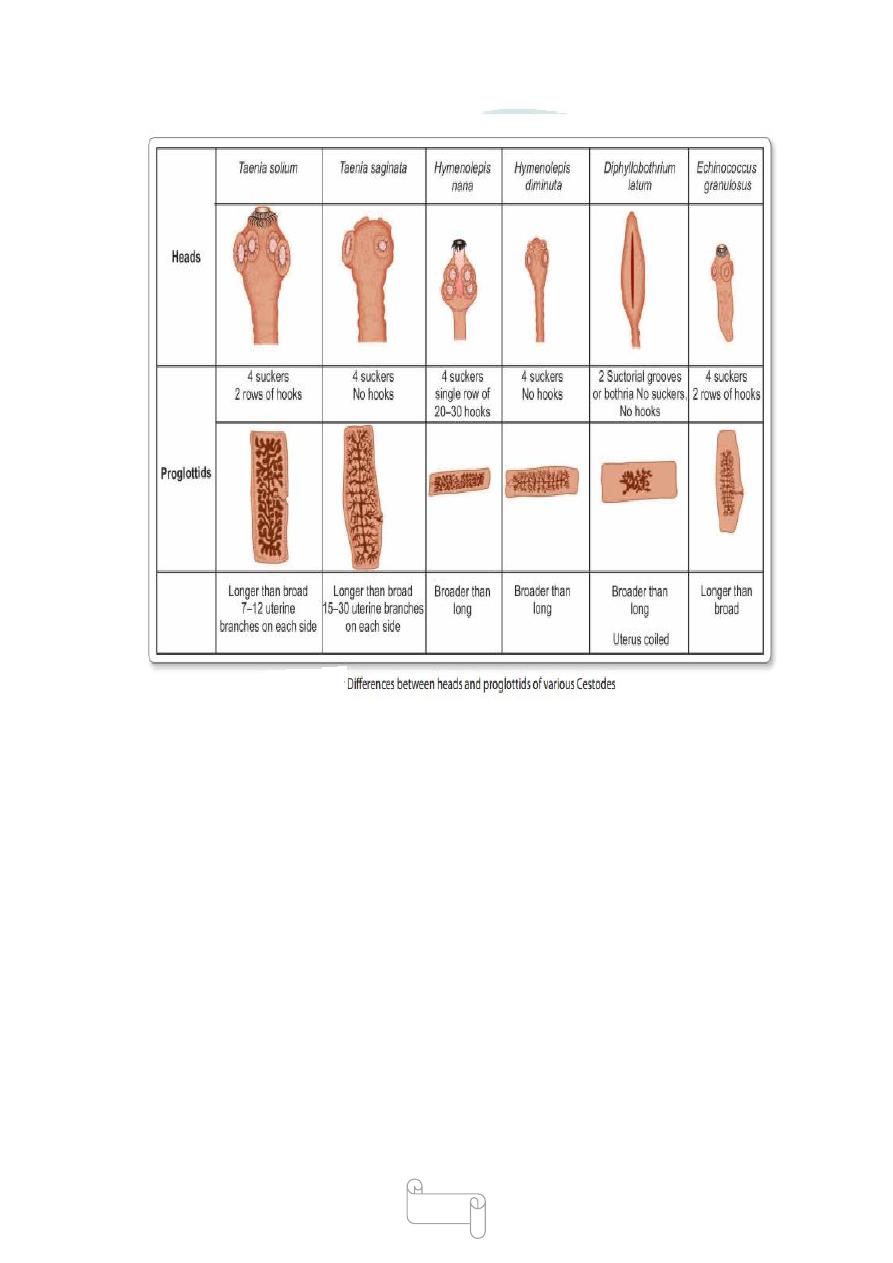
Difference between Taenia saginata and Taenia solium
67

68
Eggs
Eggs of both species are indistinguishable.
The egg is spherical, measuring 30–40 µm in diameter. It has a thin
hyaline embryonic membrane around it, which soon disappears after
release.
The inner embryophore is radially striated and is yellowbrown due to
bile staining .
In the center is a fullydeveloped embryo (oncosphere) with 3 pairs of
hooklets (hexacanth embryo).
The eggs do not float in saturated salt solution.
The eggs of T. saginata are infective only to cattle and not to humans,
whereas the eggs of T. solium are infective to pigs and humans too.
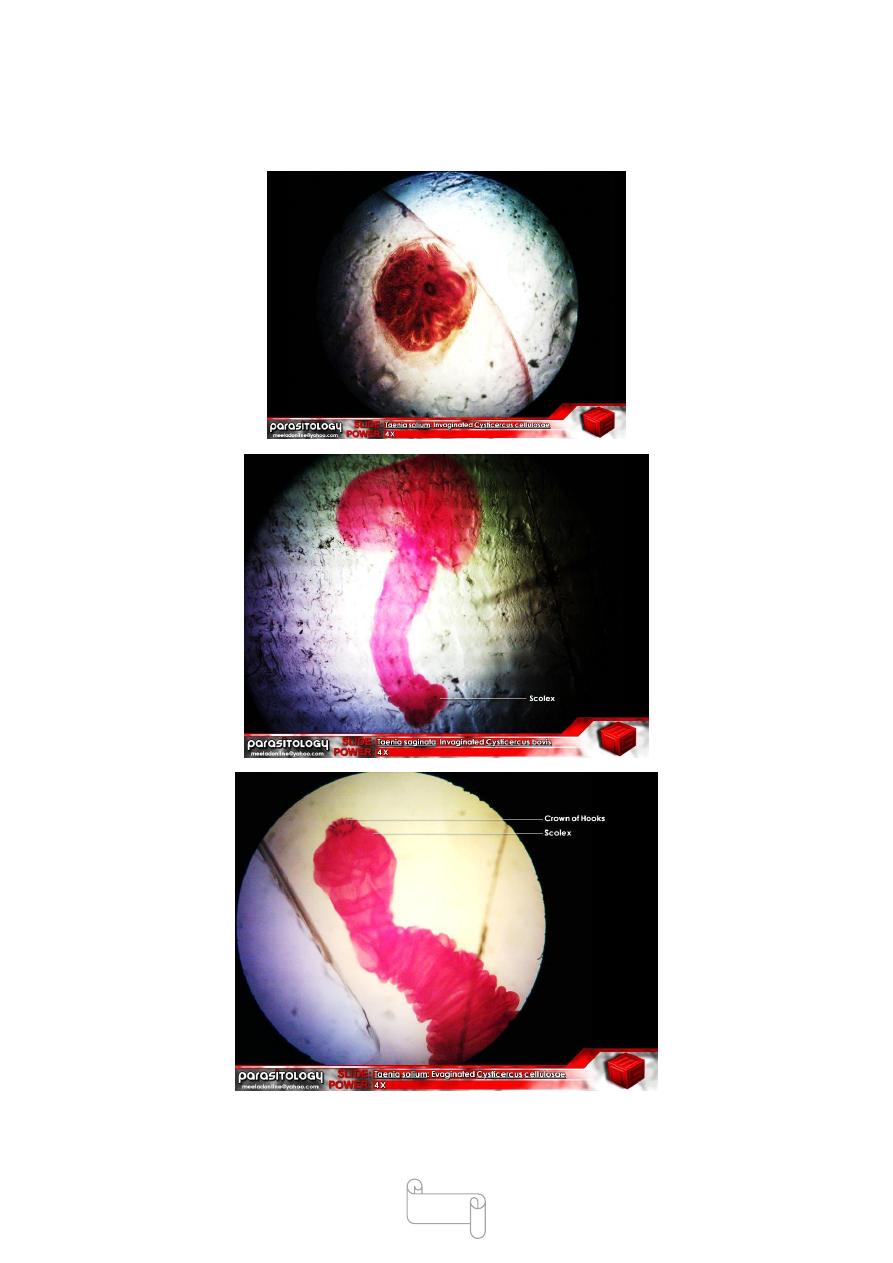
Larva
The larval stage of Taeniais called as cysticercus.
Cysticercus bovis is the larva of T. saginata.
Cysticercus cellulosae is the larva of T. solium .
€ The larva (cysticercus bovis) is infective stage for humans.
€ The cysticercus is an ovoid, milkywhite opalescent fluidfilled vesicle
measuring about 5 mm × 10 mm in diameter, and contains a single
invaginated scolex (bladder worm).
The cysticercus are found in the muscles of mastication, cardiac muscles,
diaphragm and tongue of infected cattle .
€
They can be seen on visual inspection as shiny white dots in the infected
beef (measly beef).
Cysticercus bovis is unknown in humans

69
Cysticercus cellulosae
€ It is the larval form of T. solium and also the infective
Stage of these parasite.
€ It can develop in various organs of pig as well as in man.
€ The cysticercus cellulosae or ‘bladder worm’is ovoid opalescent
milkywhite, measuring 8–10 mm in breadth and 5 mm in length
€
The scolex of the larva, with its suckers, lies invaginated within the
bladder and can be seen as a thick white spot. It remains viable for
several months .
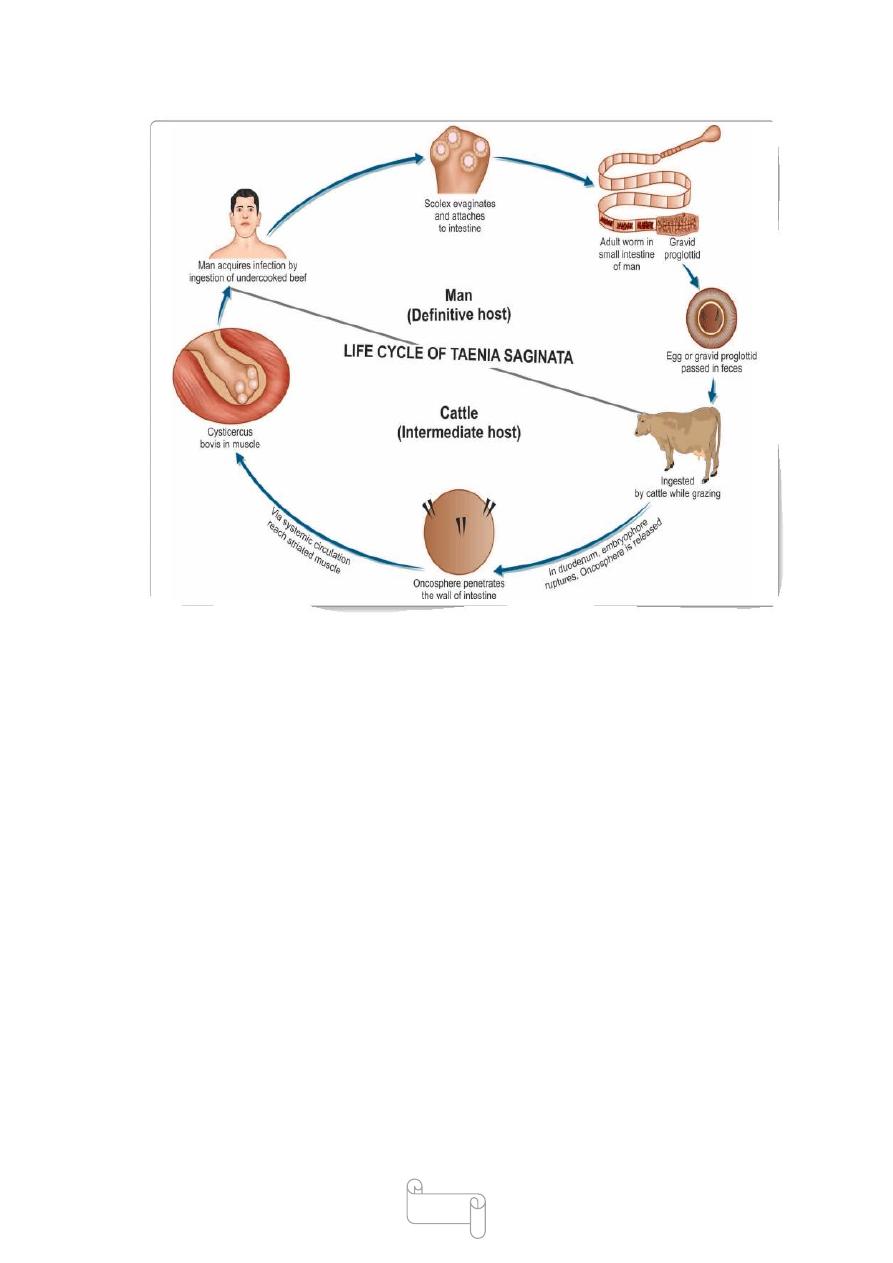
Life Cycle of Taenia Saginata
T. Saginata passes its life cycle in 2 hosts.
Definitive host: Humans are the definitive hosts .
Intermediate host: Cattle (cow or buffalo) .
Infective stage: Cysticercus bovis (larval stage) is the infective stage to
man, while eggs are infective to cattle
The adult worm lives in the small intestine of man.
The gravid segments from the adult worm breakaway and are expelled
singly. They actively force their way out through the anal sphincter.
The eggs or gravid segments are passed out with feces on the ground.
The eggs deposited in soil remain viable for several weeks. They are
infective to cattle, which ingest the eggs while grazing.
Development in Cattle
When egg ingested by cattle (cow or buffalo), the egg shell
ruptures releasing onchosphere in the duodenum.
The onchospheres, with their hooklets penetrate the intestinal wall, reach
the mesenteric venules or lymphatics and enter the systemic circulation.

70
They get filtered out in the striated muscles, particularly
in muscles of the tongue, neck, shoulder, and in the myocardium. In
these sites, the onchosheres lose their hooks and in about 60–70 days
develop in the
mature larva, cysticercus bovis.
The cysticercus can live in flesh of cattle for about 8
months, but can develop further only when ingested by
man, its definitive host
Development in Man
Man acquires infection by ingesting raw or undercooked
beef containing cysticercus .
The cysticercus are digested out of the meat in the stomach.
In the upper part of the small intestine, the head (scolex)
evaginated out of the cysticercus, becomes attached to
the mucosa, and by gradual strobilization develops into
the adult worm in about 2–3 months.
The adult worm has a life span of 10 years or more.
Infection in usually with a single worm, but sometimes
multiple infection is seen and 25 or more worms have been
reported in patients.
71
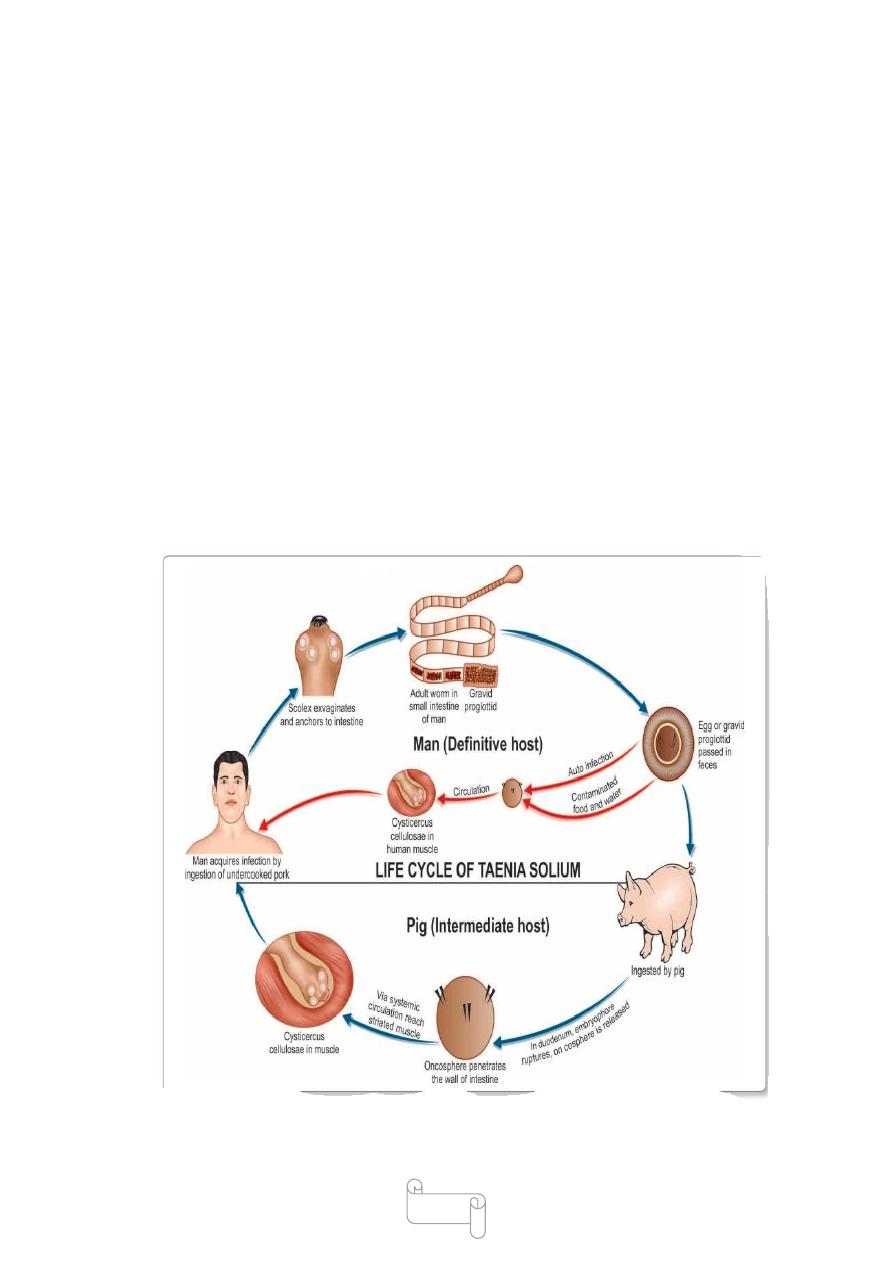
Life Cycle of Taenia Solium
Definitive host: Man
Intermediate host: Pig
Infective stage:Cysticercus cellulosae (larva)
Humans are infected by consuming inadequately cooked
pork containing cysticercus cellulosae (measly pork).
When Taenia leads to cysticercosis, the life cycle is as
follows:
Definitive host and Intermediate host: Both man
Infective stage:Eggs of T. solium(not larva)
Mode of infection:Man acquires infection by ingesting
eggs with contaminated food and water.
€
72
Autoinfection: man harboring adult worm may autoinfection oneself,
either by unhygenic personal habits or by reverse peristalsis of the
intestine.
The further development of the eggs is similar in man
and pigs.
The oncospheres are released in the duodenum or jejunum and penetrate
the intestinal wall.
They enter the mesenteric venulesor lymphatics and are carried in
systemic circulation to the different parts of the body .
They are filtered out principally in the muscles, where they develop into
the larval stage, cysticercus cellulosae in about 60–70 days.
In humans, it is a dead end and the larvae die without
further development

73
Pathogenicity and Clinical Features
Intestinal Taeniasis
It can be caused by both T. saginata and T. solium.
Patients may be frightened by noticing the proglottids passed in their
feces.
When the infection is symptomatic, vague abdominal discomformt,
indigestion, nausea, diarrhea, and weight loss may be present. Occasional
cases of acute intestinal obstruction, acute appendicitis, and pancreatitis
have also been reported.
Cysticercosis
It is caused by larval stage (cysticecus cellulosae) of T. solium.
Cysticercus cellulosae may be solitary or more often multiple.
Any organ or tissue may be involved, the most common being
subcutaneous tissues and muscles. It may also affect the eyes, brain, and
less often the heart, liver,lungs, abdominal cavity, and spinal cord.
The cysticercus is surrounded by a fibrous capsule except in the eye and
ventricles of the brain.
The larvae evoke a cellular reaction starting with infiltration of
neutrophils, eosinophils, lymphocytes, plasma cells, and at times, giant
cells. This is followed by fibrosis and death of the larva with eventual
calcification.
The clinical features depend on the site affected Subcutaneous nodules
are mostly asymptomatic
€ Muscular cysticerosis may cause acute myositis
€ Neurocysticerosis (cysticercosis of brain) is the most common and
most serious form of cysticercosis. about 70% of adultonset epilepsy is
due to neurocysticercosis.
Other clinical features of neuro cysticercosis are increased intracranial
tension, hydrocephalus, psychiatric disturbances, meningoencephalitis,
transient paresis, behavioral disorders
aphasia, and visual disturbances.
74
the second most common cause of intracranial space occupying lesion
(ICSOL) after Tuberculosis in India.
€
In ocular cysticercosis, cysts are found in subretinal space and
conjunctiva, vitreous humor
The condition may present as blurred vision or loss of vision, iritis,
uveitis, and palpebral conjunctivitis
Prophylaxis
Beef and pork to be eaten by man should be subjected to effective
inspection for cysticercus in slaughter house.
Avoidance of eating raw or undercooked beef and pork. The critical
thermal point of cysticercus is 56°C for 5 minutes.
Maintainence of clean personal habits and general sanitary measures.
For control of cysticercosis, prevention of fecal contamination of soil,
proper disposal of sewage and avoidance of eating raw vegetables
grown in polluted soil are useful measures

75
Detection and treatment of persons harboring adult worm, as they can
develop cysticercosis due to autoinfection
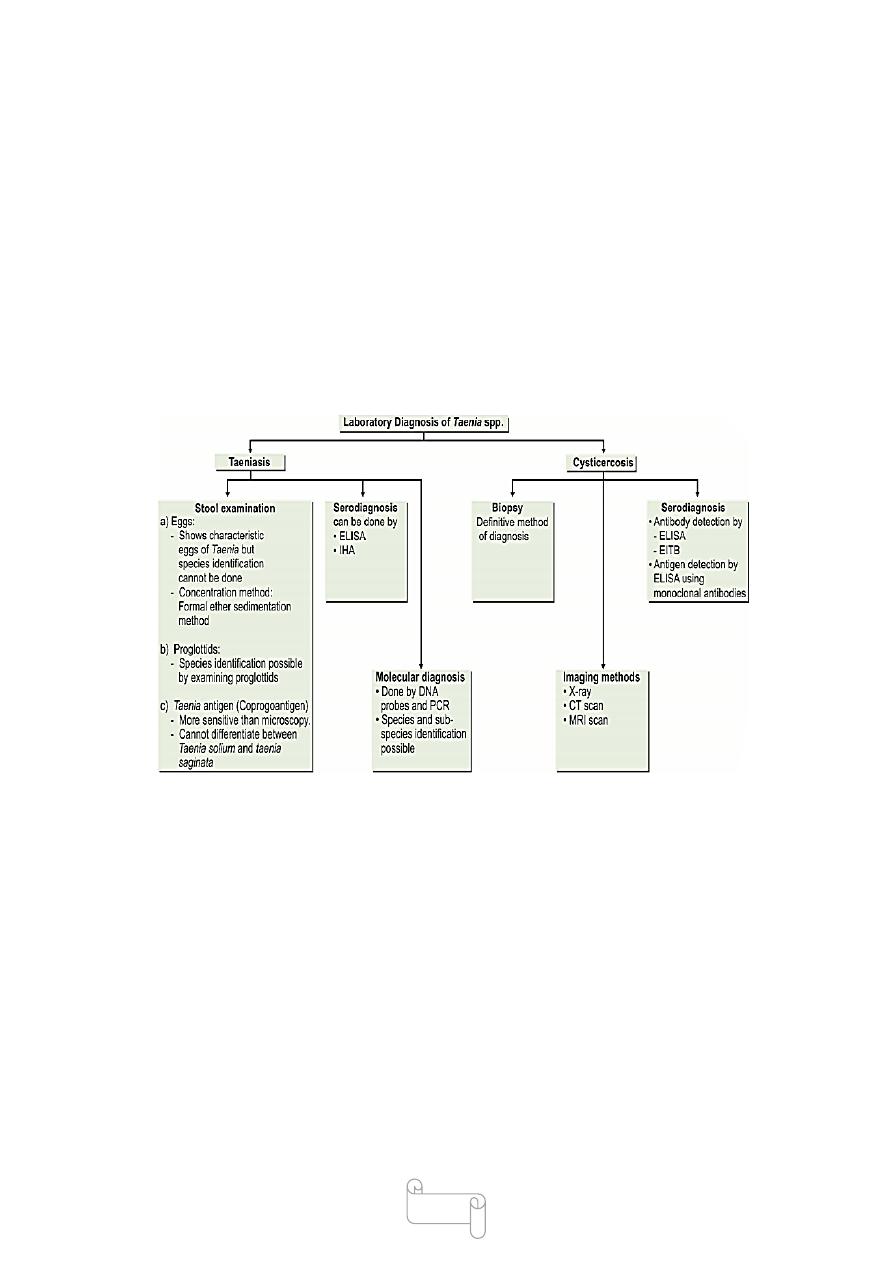
Treatment
Intestinal Taeniasis
Single dose of praziquantel (10–20 mg/kg) is the drug of choice.
Niclosamide (2 g), single dose, is another effective drug.
Purgation is not considered necessary.
Cysticercosis
For cysticercosis, excisionis the best method, wherever
possible.
Asymptomatic neurocysticercosis requires no treatment.
.For symptomatic cerebral cysticercosis.
praziquantel in a dose of 50 mg/kg in 3 divided doses for 20–30 days
albendazole in a dose of 400 mg twice daily for 30 days may be
administered.
Corticosteroids may be given along with praziquantel or albendazole to
reduce the inflammatory reactions caused by the dead cysticercus larva.
In addition, antiepileptic drugs should be given until the reaction of the
brain has subsided.
Operative intervention is indicated for hydrocephalus
Taenia Saginata Asiatica
T. saginata asiatica is closely related to T. saginata and is found mainly
in Asia.
It is morphologically similar to T. saginata except. It is smaller than T.
Saginata.
€ Intermediate host is pig (not cow).
Its cysticerci are located primarily in liver of the pig (not muscle).
Clincial features, diagnosis and treatment are similar to that of T.
saginata

76
د. سعيد
طفيليات
3
\
1
\
8102
( عدد االوراق
6
) م
\
3
\
موصل
lec: 9
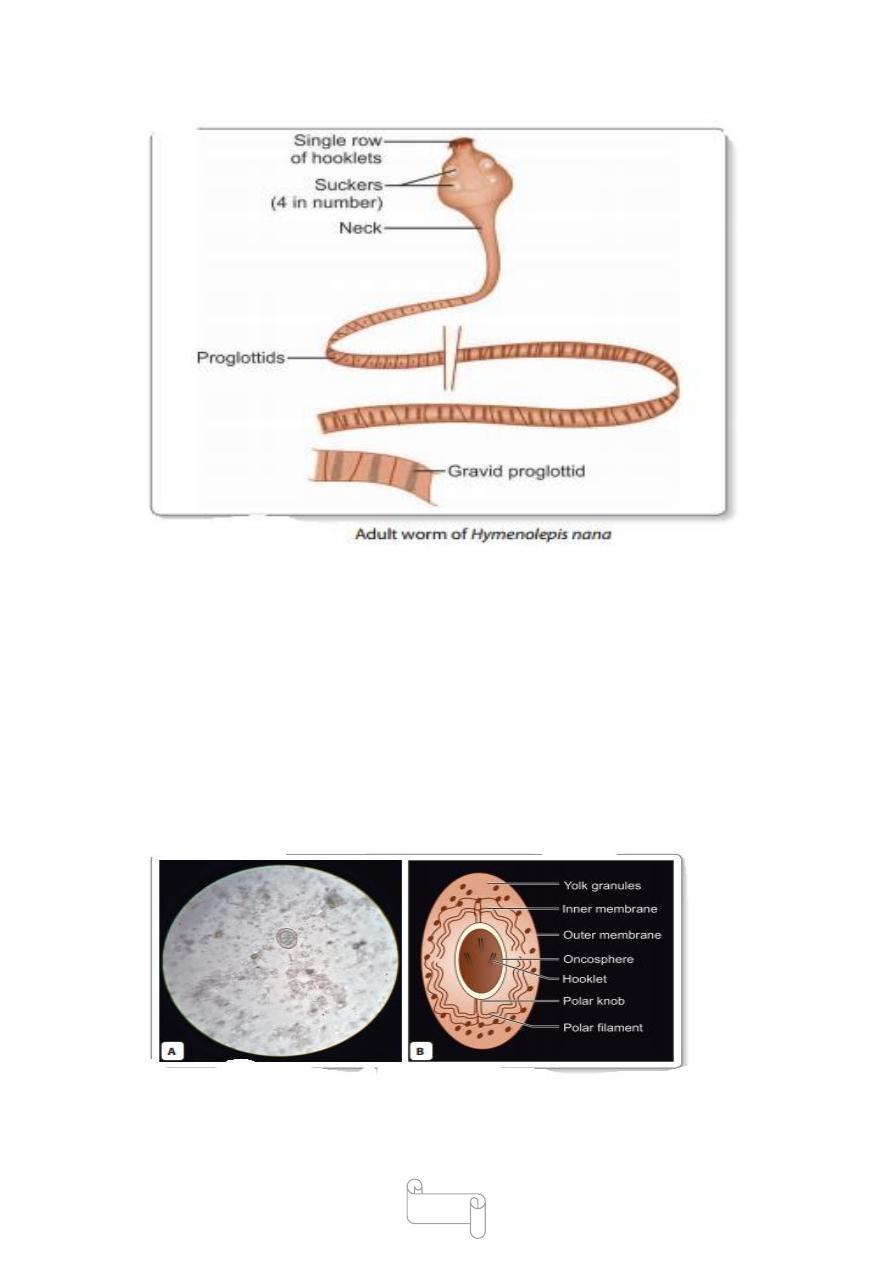
Hymenolepis Nana
Common name: Dwarf tape worm .
Smallest cestode infecting man: Hymenolepis nana.
Longest cestode infecting man: Diphyllobothrium latum
Distribution
It is cosmopolitan in distribution but is more common in
warm than in cold climates.
Infection is most common in school children .
The adult worm lives in the proximal ileum of man
Morphology
Adult Worm
H. Nana is the smallest intestinal cestode that infects man.
It is 5–45 mm in length and less than 1 mm thick.
The scolex has 4 suckers and a retractile rostellum with a single row of
hooklets.
The long slender neck is followed by the strobila consisting of 200 or
more proglotlids, which are much broader than long.
Genital pores are situated on the same side along the margins.
The uterus has lobulated walls and the testis are round and 3 in number.
Eggs are released in the intestine by disintegration of
the distal gravid segments
77
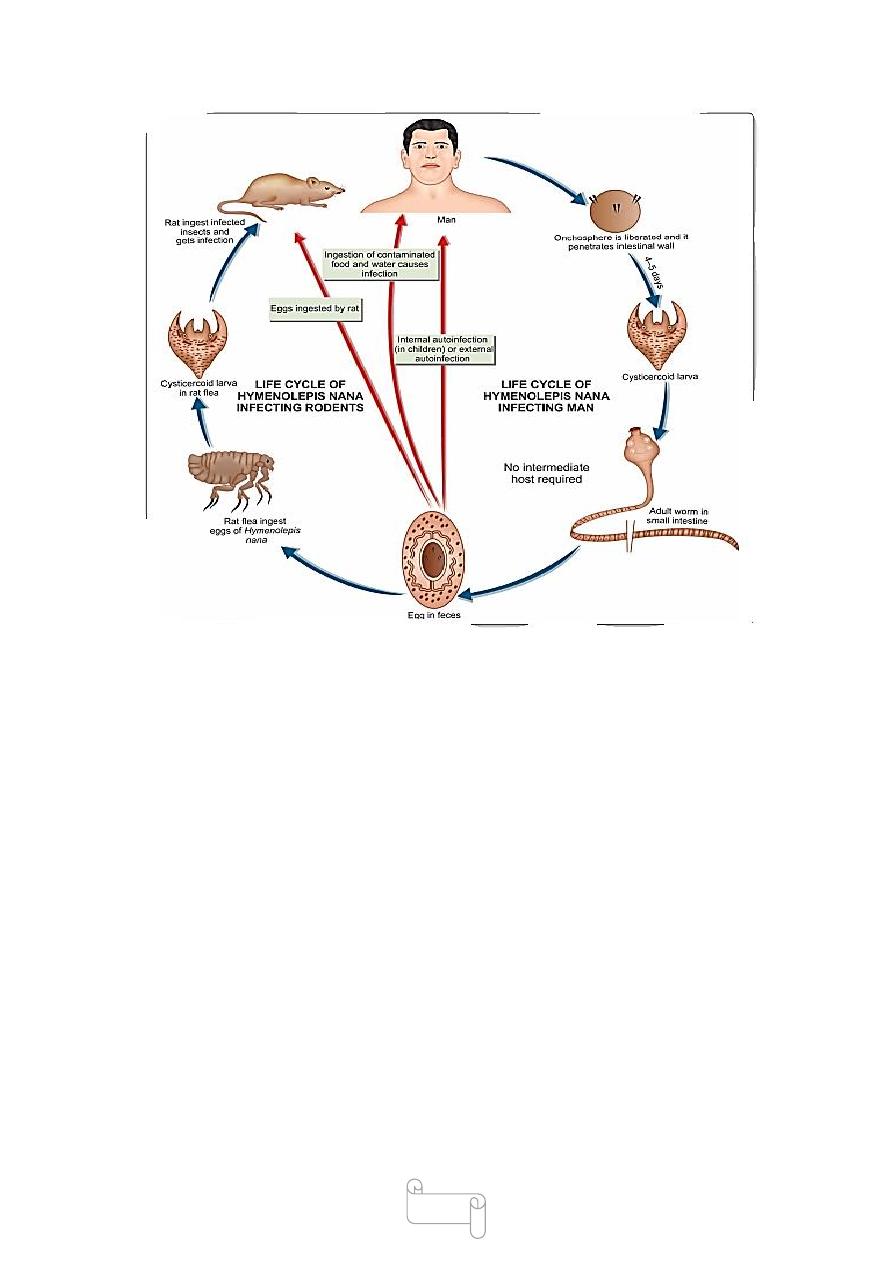
Egg
The egg is roughly spherical or ovoid, 30–40 µm in size.
It has a thin colorless outer membrane and inner
Embryophore enclosing the hexacanth oncosphere
The space between 2 membranes contains yolk granules and 4–8 thread
like polar filaments arising from 2 knobs on the embryophore.
They
are immediately infective and unable to survive
for more than 10 days in external environment.

78
Life Cycle
Definitive host : Man.
There is no intermediate host.
Mode of transmission: Infection occurs by ingestion of the food and
water contaminated with eggs
€
Internal autoinfection may also occur when the eggs released in the
intestine hatch there itself .
External autoinfection occurs when a person ingest own eggs by fecal
oral route.
When the eggs are swallowed, or in internal autoinfection, they hatch in
the small intestine.
The hexacanth embryo penetrates the intestinal villus and develops into
the cysticercoid larva.
.
This is a solid pyriform structure, with the vesicular anterior end
containing the invaginated scolex and a short conical posterior end.
After about 4 days, the mature larva emerging out of the villus
evaginates its scolex and attaches to the mucosa.
It starts strobilization, to become the mature worm, which begins
producing eggs in about 25 days.
A different strain of H. nana infects rats and mice.
The eggs passed in rodent feces are ingested by rat fleas (Xenopsylla
cheopis and others), which acts as the intermediate host
79
Clinical Features
Hymenolopiasis occurs more commonly in children.
There are usually no symptoms but in heavy infections, there is nausea,
anorexia, abdominal pain, diarrhea, and irritability.
Sometimes pruritus may occur due to an allergic response
Diagnosis
The diagnosis is made by demonstration of characteristic
eggs in feces by direct microscopy
ELISA test has been developed with 80% sensitivity
Treatment
Praziquantel (single dose of 25 mg/kg) is the drug of choice, since it acts
both against the adult worms and the cysticercoid larva in the intestinal
villi.

80
Prophylaxis
Maintenance of good personal hygiene and sanitary
Improvement
Avoiding of consumption of contaminated food and
Water with eggs.
Rodent control
Hymenolepis Diminuta
This is called the rat tapeworm and is a common parasite of rats and
mice.
Size 10–60 cm in length.
life cycle is similar to that of the murine strain of H. nana.
Rarely, human infection follows accidental ingestion of
infected rat fleas.
Human infection is asymptomatic.
Dipylidium Caninum
This common tapeworm of dogs and cats, it may accidentally
cause human infection, mainly in children.
Morphology
The adult worm in the intestine is about 10–70 cm long
The scolex has 4 prominent suckers and a retractile rostellum with upto 7
rows of spines .
The mature proglottid has 2 genital pores, 1 on either side, hence the
name Dipylidium (dipylos—2 entrances)
Gravid proglottids are passed out of the anus of the host singly or in
groups

81
Life Cycle
Definitive host: Dogs, cats, and rarely man.
Intermediate host: Fleas.
Man acquires infection by ingestion of flea harboring cysticercoid larva.
The eggs or proglottids passed in feces of dogs and cats .
Eggs are eaten by dog fleas and cat fleas. The embryo develops into a
cysticercoid larva .
infection is transmitted when the adult fleas containing the larvae are
eaten by dogs, cats, or rarely humans,
Clinical Features
Human infection is generally asymptomatic, but the actively motile
proglottids passed in stool .
Diagnosis
The diagnosis is made by detection of proglottids or eggs in stool
Treatment
The drug of choice is praziquantel
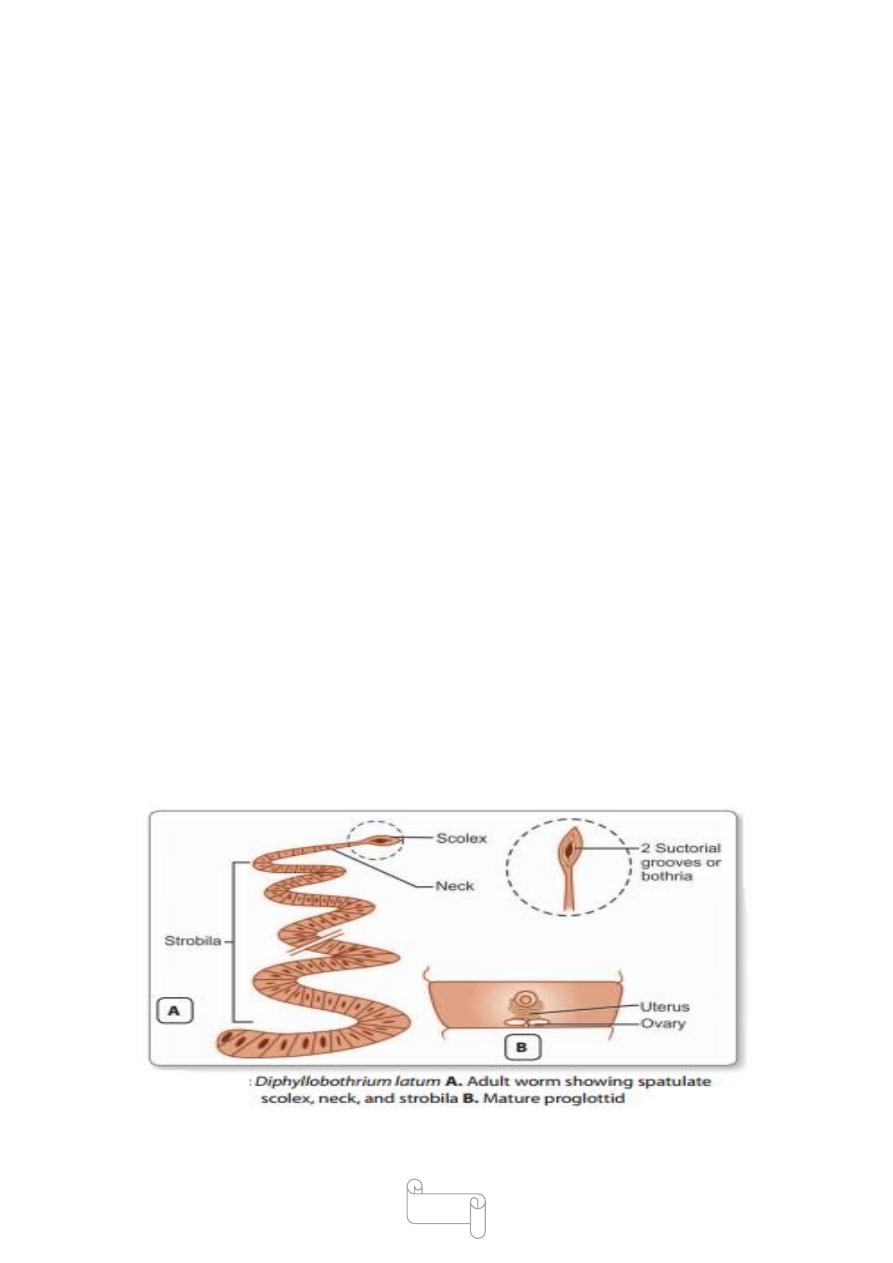
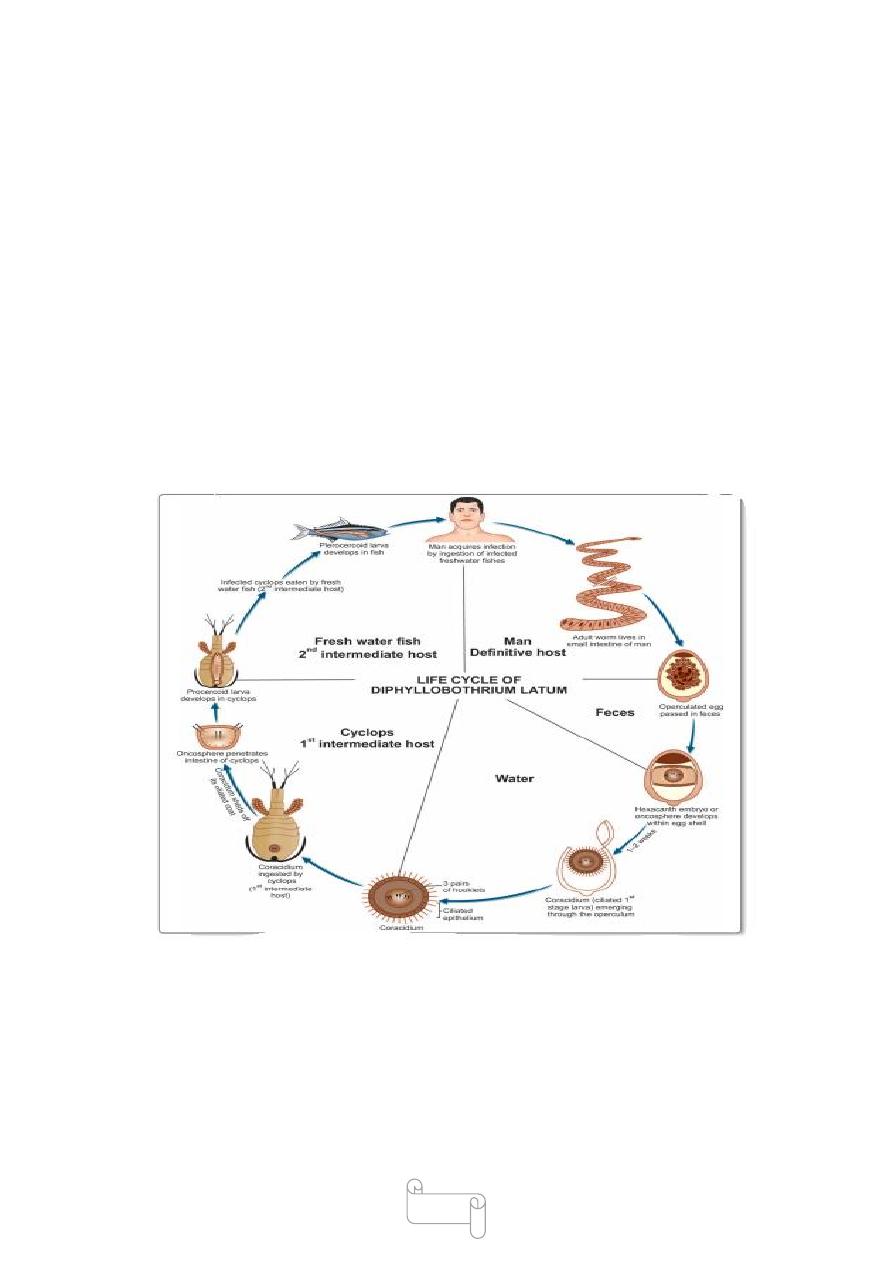
Diphyllobothrium Latum
Common name: Fish tape worm/Broad tape worm.
disease called Diphyllobothriasis
Distribution
occurs in central and northern Europe, particularly in the Scandinavian
countries. It is also found in Siberia, Japan, North America, and Central
Africa.
Habitat
The adult worm is found in the small intestine, usually in the
ileum,
82
Morphology
Adult worm
It is ivory-colored and very long, measuring upto 10 meters or more. It is
the largest tape worm inhabiting the small intestine of man
the adult worm has 3 parts: scolex, neck, and strobila
Scolex (head) is spatulate or spoon-shaped, about 2–3 mm long and 1
mm broad. It carries 2 slitIike longitudinal sucking grooves (bothria),
one dorsal and the other ventral.
The scolex lacks suckers and hooks.
Neck is thin.
Strobila consists of 3,000–4,000 proglottids, consisting of immature,
mature, and gravid segments .
The mature proglottid is broader than long, about 2–4 mm long and 10–
20 mm broad and is practically filled with male and female reproductive
organs .
The female reproductive organs are arranged along the midline, lying
ventrally. The ovary is bilobed. The large rosettelike uterus lies
convoluted in the center.
Three genital openings are present ventrally along the mid line
The fertilized ova develop in the uterus and are discharged periodically
through the uterine pore.
83
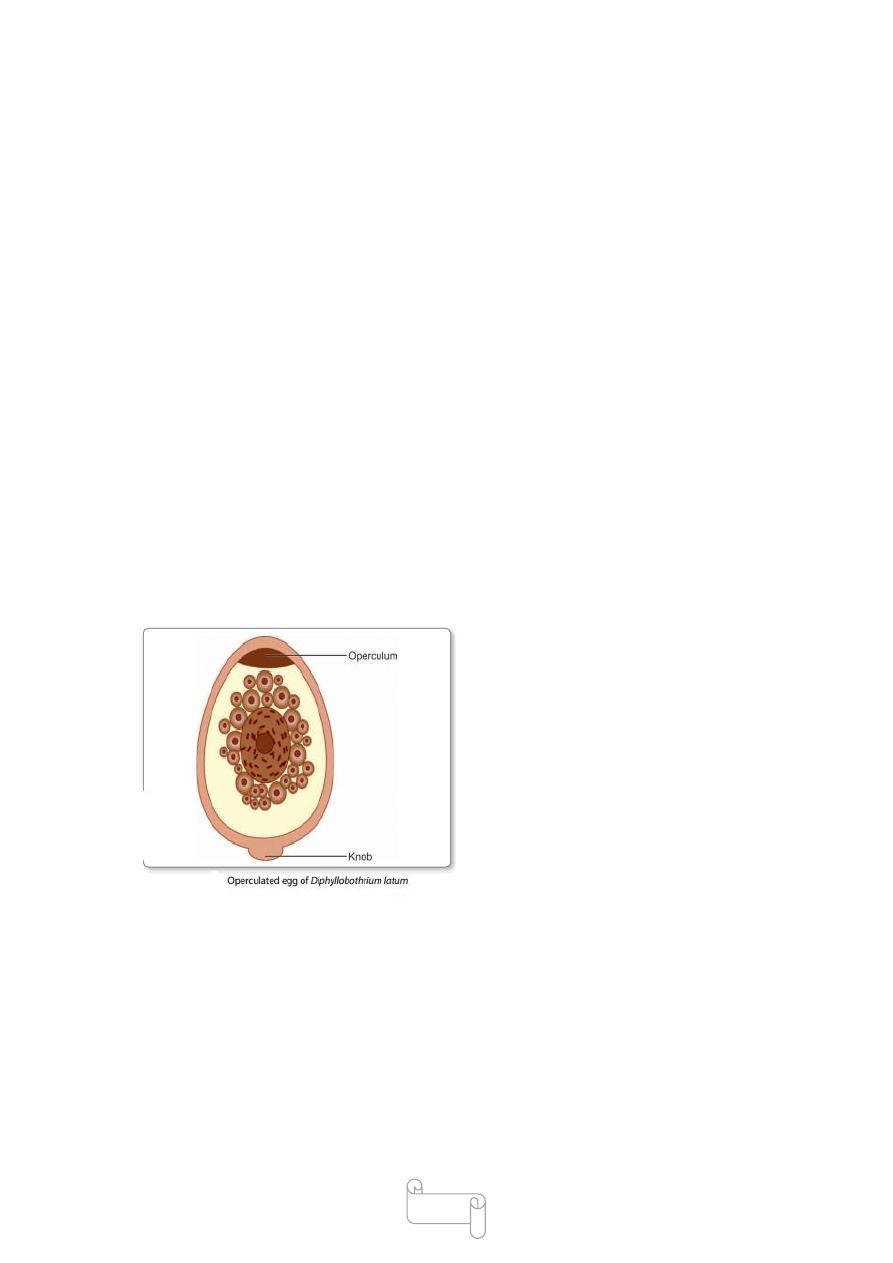
Egg
a single worm may pass million eggs in a day
Egg is broadly ovoid, about 65 µm by 45 µm, with a
thick, light brown shell .
It has an operculum at one end and often a small knob at the other.
The freshly passed egg contains an
immature embryo surrounded by
yolk granules.
The eggs are resistant to chemicals
but are killed by drying.
The embryo with 6 hooklets inside
the egg is called the oncosphere.
Larval Stages
There are 3 stages of larval development:
First stage larva (coracidium)
Second stage larva (procercoid)
Third stage larva (plerocercoid).

84
Life Cycle
Definitive hosts: Man, dog, and cat. Man is the optimal host.
First intermediate host: Fresh water copepod, mainly of
genera Cyclops or Diaptomus.
Second intermediate host: Fresh water fish (salmon, trout etc.).
Infective form to human: Third stage plerocercoid larva.
The adult worm lives in the small intestine. It lays operculated eggs
which are passed along with the feces in water .
The freshlypassed egg contains an immature embryo surrounded by yolk
granules..
The embryo with 6 hooklets (hexacanth embryo) inside the egg is called
the oncosphere.
In water, it matures in about 10–15 days and ciliated first stage larva,
called coracidium emerges through the operculum.
Coracidium (first stage larva) can survive in water for about 12 hours, by
which time it should be ingested by the fresh water crustacean copepod
cyclops, which is the first intermediate host .
In the midgut of the cyclops, the coracidium casts off its ciliated coat and
by means of its 6 hooklets, penetrates into the hemocele (body cavity).
In about 3 weeks, it develop into the elongated second stage Larva about
550 µm long, which is called the procercoid larva,
Procercoid larva has a rounded caudal appendage.
.
If the infected cyclops is now eaten by a freshwater fish
(second intermediate host), the procercoid larva penetrates the intestine of
the fish and grows.
85
In the fish, procercoid larva looses its caudal appendage
and develops into the third stage larva called the plerocercoid larva
Plerocercoid larva
This is the infective stage for humans.
Man gets infection by eating raw or undercooked fish containing
plerocercoid larva.
The larva develops into adult worm in the small intestine
in about 5-6 week and produce eggs to repeat the life cycle
The adult worm may live for about 10 years or more
Pathogenicity and Clinical Features
The pathogenic effects of diphyllobothriasis depend on the mass of the
worm
In some persons, infection may be entirely asymptomatic,
while in others there may be an evidence of mechanical

86
obstruction.
Transient abdominal discomfort, diarrhea, nausea, weakness,.
Weight loss, and anemia are the usual manifestations.
The anemia (pernicious anemia) develops because the tape worm absorbs
large quantity of vit B12 and interferes with its ileal absorption, leading
to vit B12deficiency
Patients may be frightened by noticing the strands of proglottids passed
in their feces.
Diagnosis
Stool Microscopy
Eggs are passed in very large number in feces, and therefore,
their demonstration in feces offers an easy method of diagnosis.
The Proglottids passed in feces can also be identified by their
morphology.
Serodiagnosis
A coproantigen detection test is available to diagnose
diphyllobothriasis.
Treatment
Praziquantel in a single dose of 10 mg/kg is effective.
Parenteral vit B12 should be given, if B12 deficiency is present.
Prophylaxis
Infection can be prevented by
-Proper cooking of fish
-Deep freezing of fish(–10°C for 24–48 hours ) .
-Prevention of fecal pollution of natural waters
-Periodical deworming of pet dogs and cats