ANEMIA
Defined as decrease in the amount of red
blood cells ( RBC) OR in the amount of
hemoglobin ( Hb) in the blood , so there will
be lowered ability of the blood to carry O2 to
the tissues .
In order to define anemia you have to know what is the
normal values of hemoglobin ( according to the sex ) !
Male 13 - 18 g/dl ( 130 -180 g/l )
Female 11.5
– 16.5 g/dl ( 115 – 165 g/l)
Hematocrit (HCT) = Hb * 3
Anemia itself is not a diagnosis !!
It is a sign of many underlying diseases .. i.e , you should
look for the cause of anemia ..
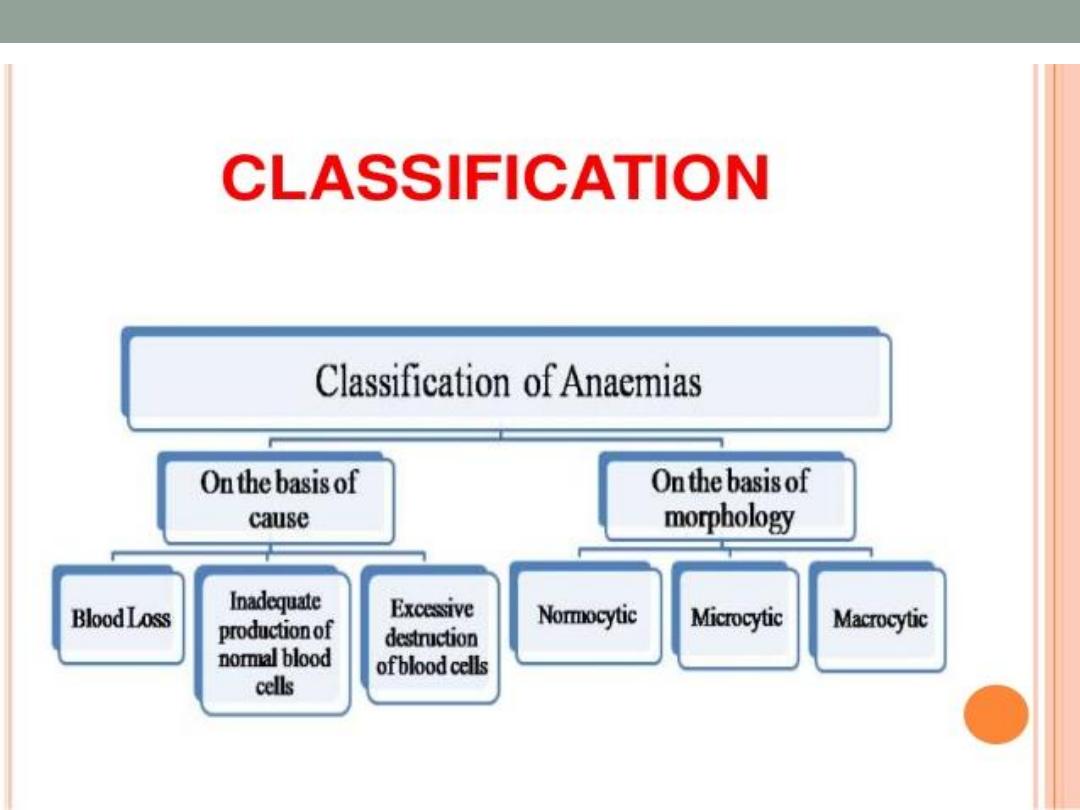
Causes :
Anemia generally caused by the following mechanisms :
1.Blood loss ( trauma , surgery , GIT bleeding , GUT bleeding ,
menorrhagia …etc)
2. Inadequate RBC producation ( iron difficiency anemia, vitamin
B 12 difficiency , folic acid difficiency , anemia of chronic
diseases )
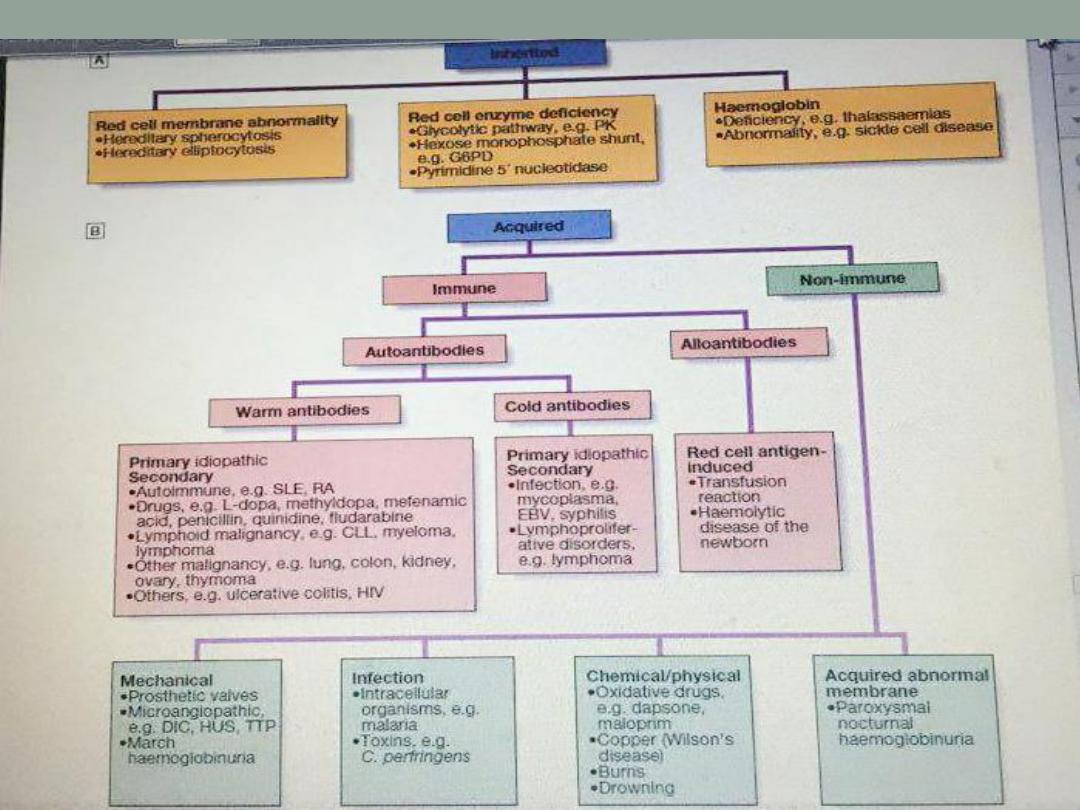
3. RBC destruction ( hemolysis, which is either caused by
intrinsic causes like defect in the hemoglobin chain e.g
thalasemia, defect in the membrane e.g spherocytosis , or defect
in the enzymes e.g G6PD difficiency ,, or caused by extrinsic
factors like infection & drugs.
What is mean corpuscular volume ( MCV ) ? Significance ?
MCV reflects erythrocyte size , its normal range 78
– 98fl
Understanding the MCV can guide the doctors to
charactarize certain anemia .. How ?!
MCV below 78 fl called
microcytic anemia
MCV 78
– 98 called
normocytic anemia
MCV above 100 fl called
macrocytic anemia
MCV > 100
( Macrocytic)
MCV 78
– 100
( normocytic)
MCV < 78
( Microcytic)
1.B12 dificiency
2. Folic acid dificiency
3. Myelodysplastic
syndrome ( MDS)
4. Hypothyroidism
5. Alcohol
6. Liver disease
7. Drugs ( hydroxurea ,
zidovudin, Methotrexate)
1.Anemia of kidney
diseases
2. Anemia of chronic
infections
3. Anemia of malignancy
4. Anemia of chronic
inflammatory diseases.
1.Iron dificiency anemia
( IDA)
2. Thalassemia
3. Occasionally anemia of
chronic diseases .
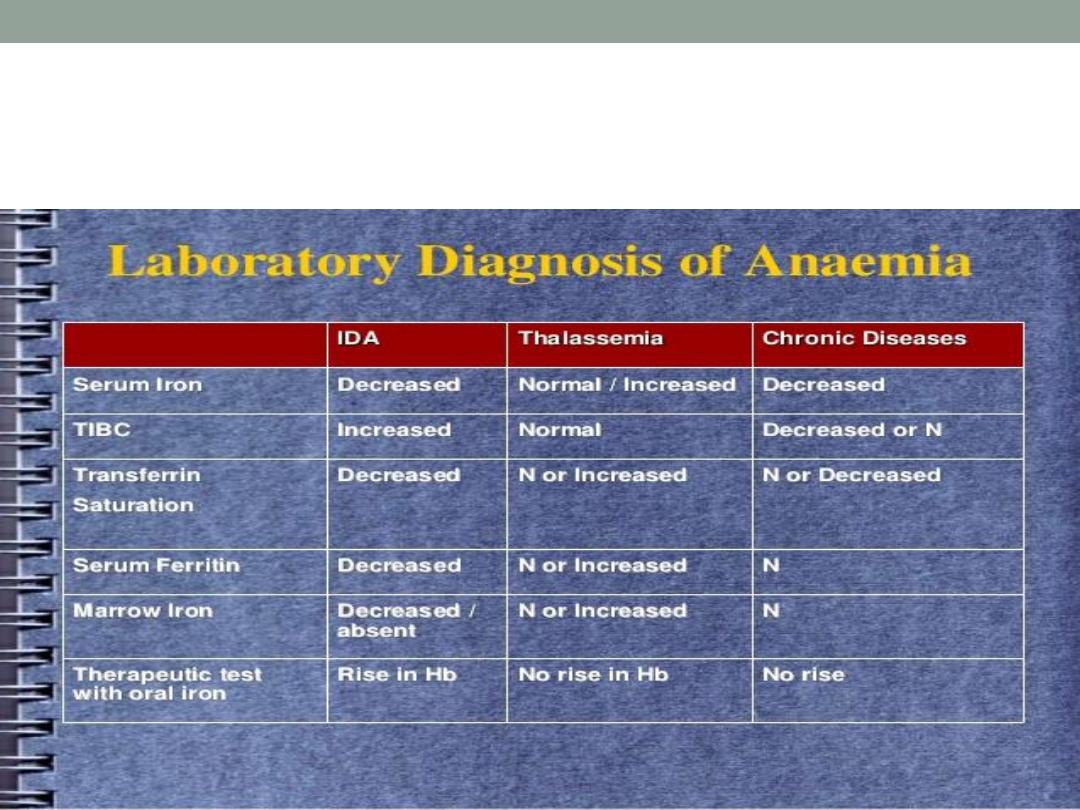
Differentiate IDA , thalassemia & anemia
of chronic disease
Clinical features of anemia
SYMPTOMS :
Most of the symptoms result from poor perfusion of the tissues
1.Fatigue
2. Dizziness
3.Headache
4.Blurred vision
5. Exertional dyspnoea
6.Chest pain
7.Palpitation
8. Pica ! ( IDA )( ingestion of non nutritional materials , ice , clay ,
papers …..)
9. Neuropathy ( B12 D-) .

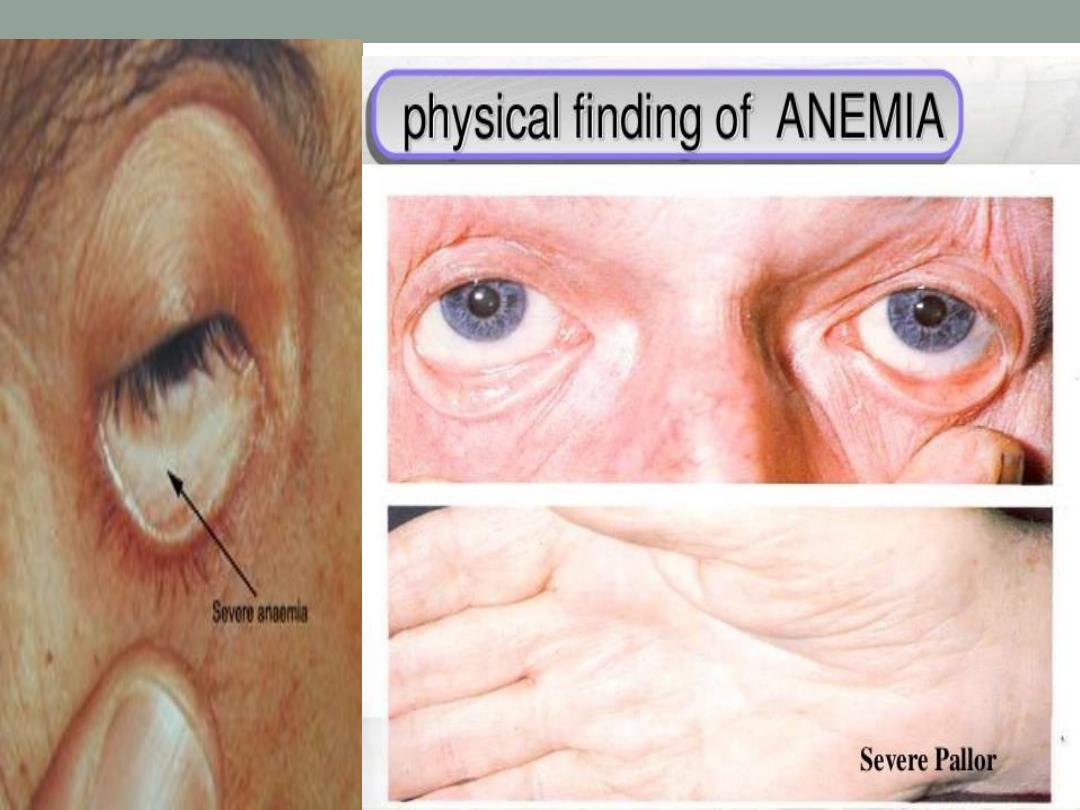
SIGNS :
1. Dyspnoea !
2. Tachycardia
3.Pallor ( every anemic pt. is pale , but not every pale pt. is
anemic !! ) ( conjunctiva , palmer creases & mucus membranes)
4.. Angular cheilitis (IDA)
5 . Glossitis ( B12 , IDA )
6 . Jaundice ( hemolysis , megaloblastic anemia
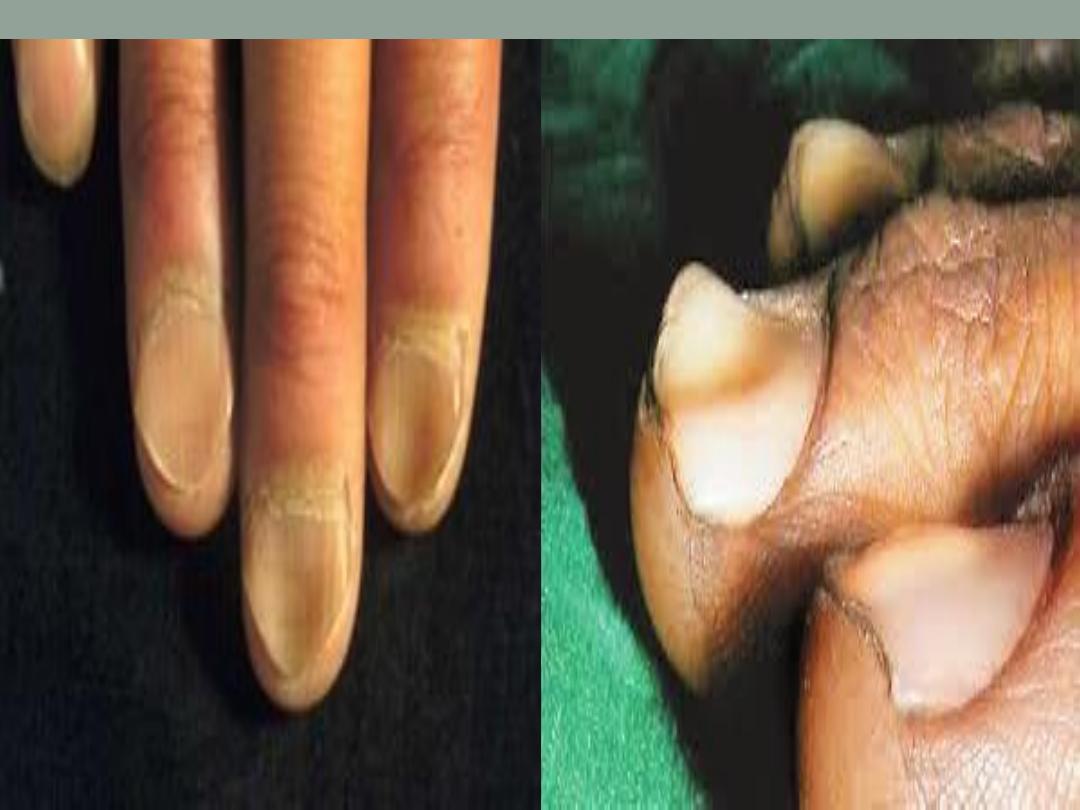
7. Koilonachia ( spoon nails ) ( IDA)
8 . Bruises ( bleeding tendency )
9 . Lymph node !
10. Organomegally
11. Evidence of the underlying disease ! ( features of renal
disease , liver disease , malignancy , rheumatoid arthritis , SLE
…..)

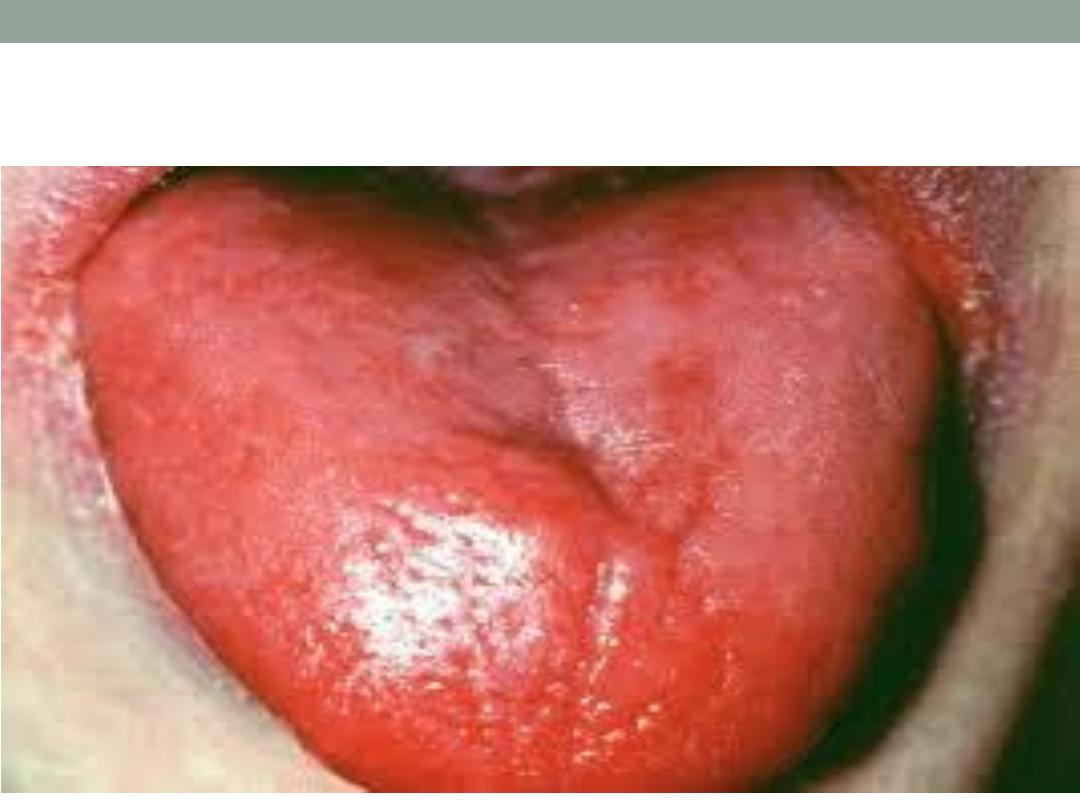
Glossitis


Work up !
1
.Careful history : don’t forget nutritional hx. , gynecological hx in
women , drugs , family hx
of anemia…etc.
2. Proper physical examination
3. Investigations:
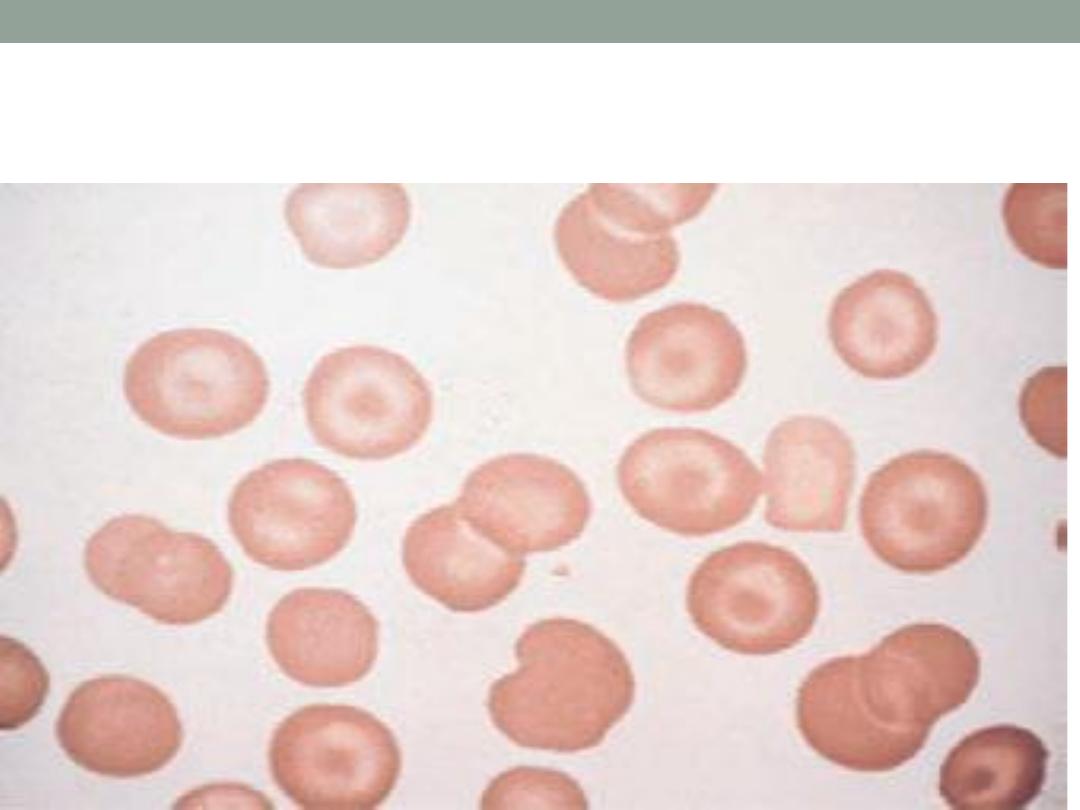
a. CBC & Blood film ( Hb, HCT, MCV , MCH , MCHC , WBC &
differential , platelets , reticulocytes ( will be high in hemolytic
anemia & bleeding) , the blood film may show anisocytosis (
abnormality in the size of the RBC), poikilocytosis ( abnormality
in the shape of RBC) ,or abnormal cells like : tear drop cells (
myelofibrosis ) , cigar shape cells ( iron difeciency anemia) ,
target cells ( thalasemia , liver disease ) , RBC fragments (
shistocytes ) ( in microangiopathic hemolytic anemias) , howel
jolly bodies ( splenectomy ) , blister cells & bite cells ( G6PD
dificiency
) , burr cells ( uremia ) … etc.
Target cells
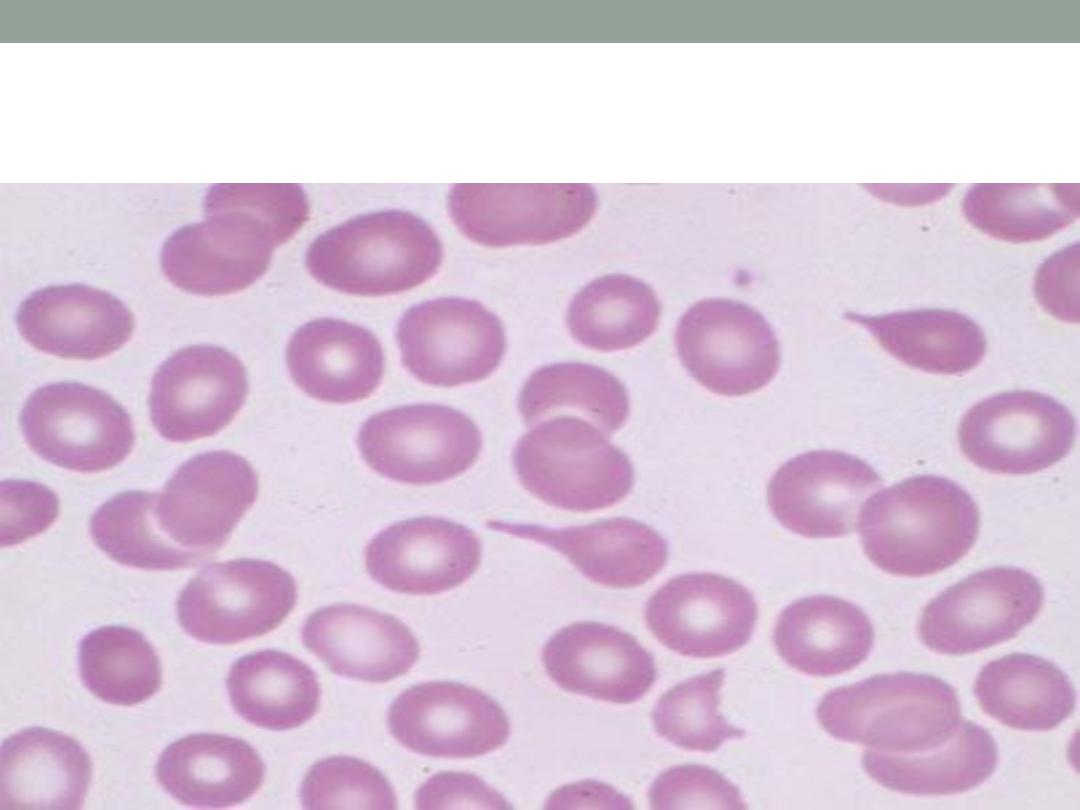
Tear drop cells ( myelofibrosis )
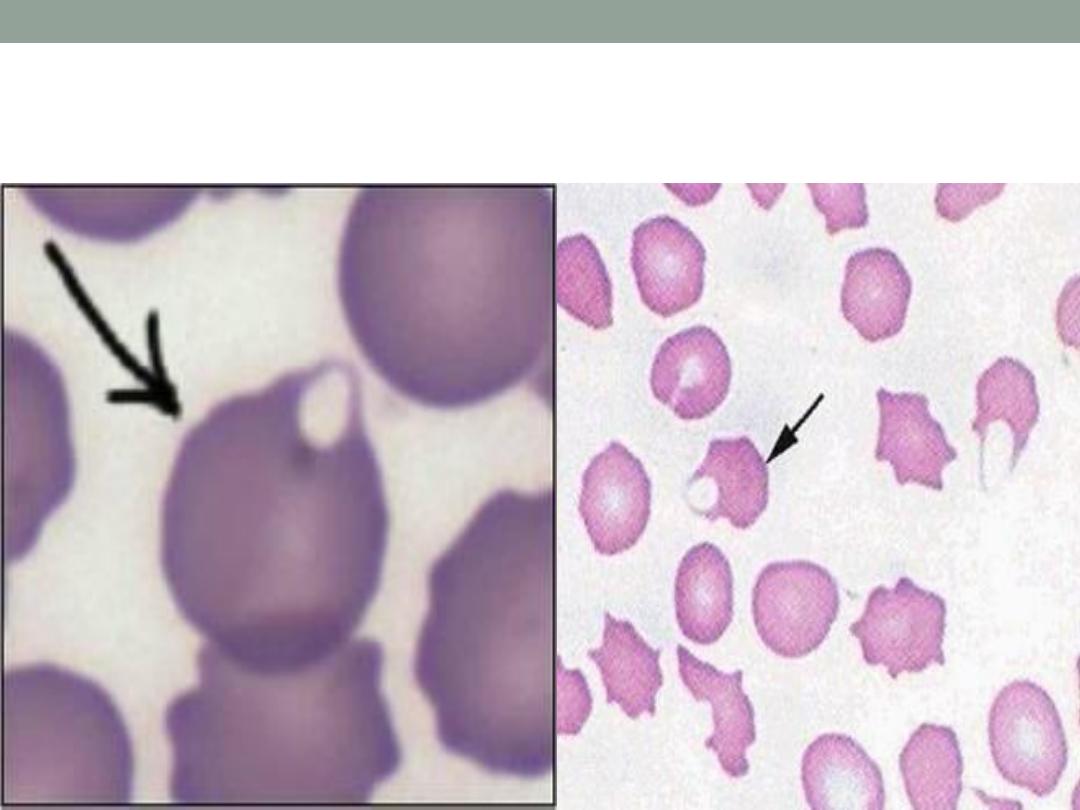
Blister cells ( G6PD D-)
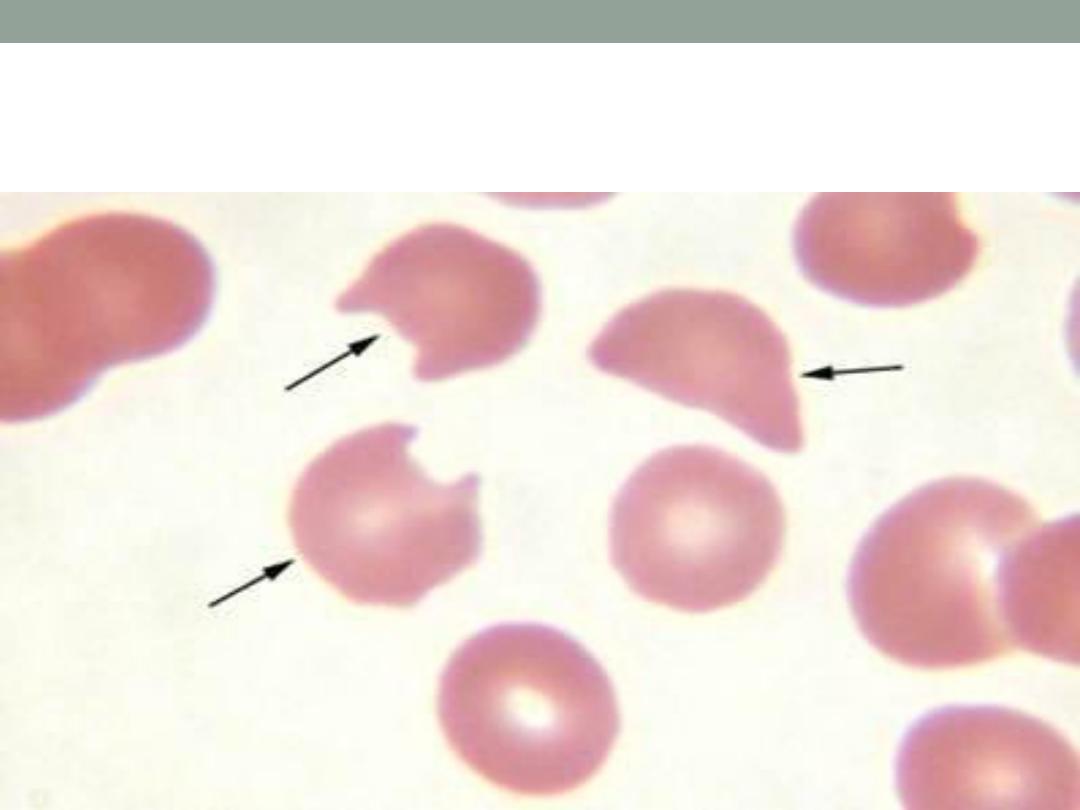
Bite cells ( G6PD D-)
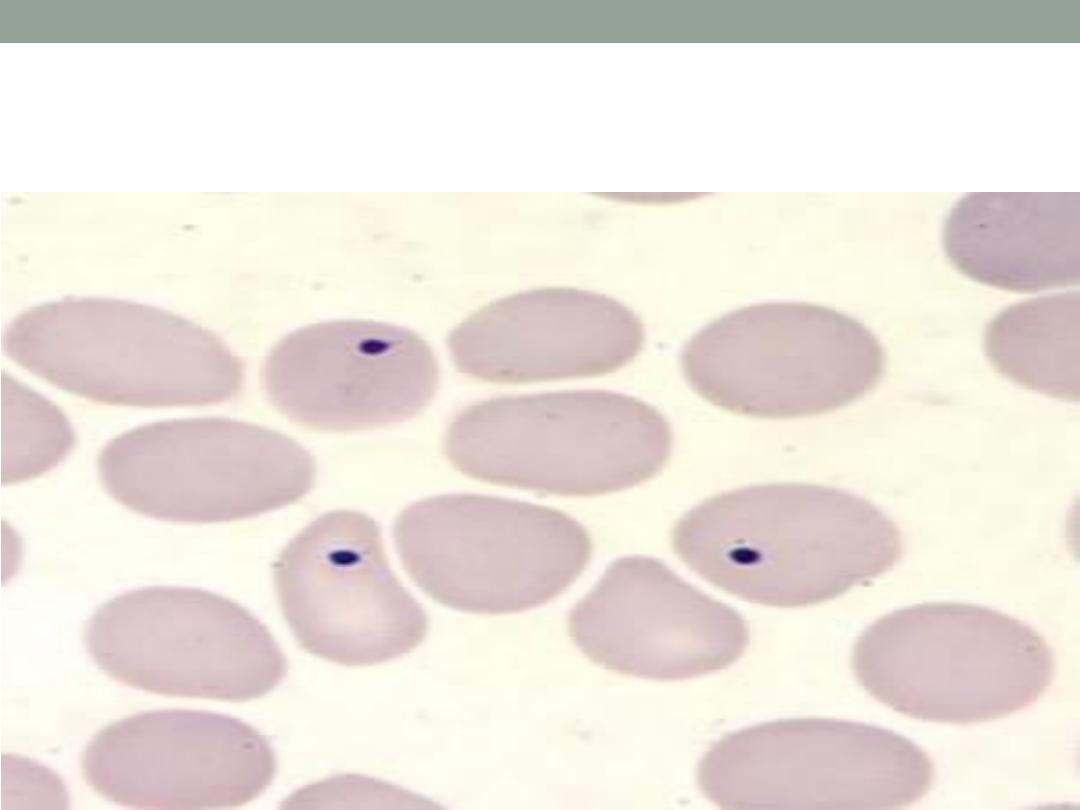
Howel jolly bodies
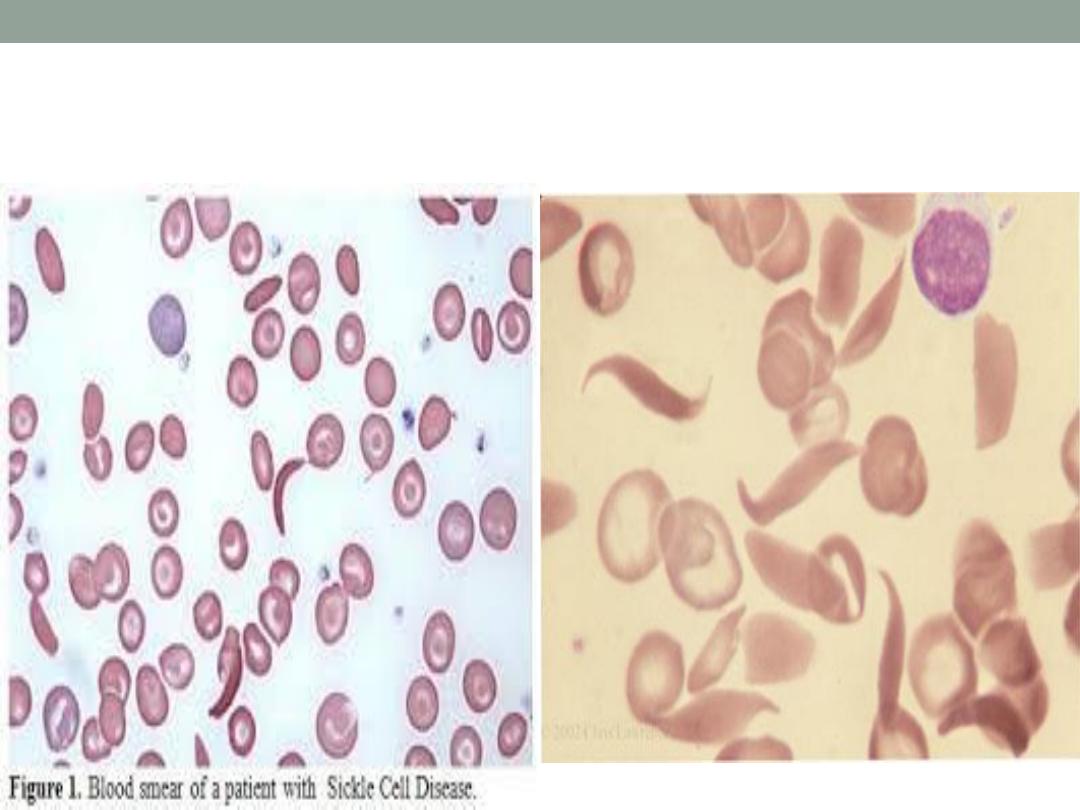
Sickle cells

RBC fragments
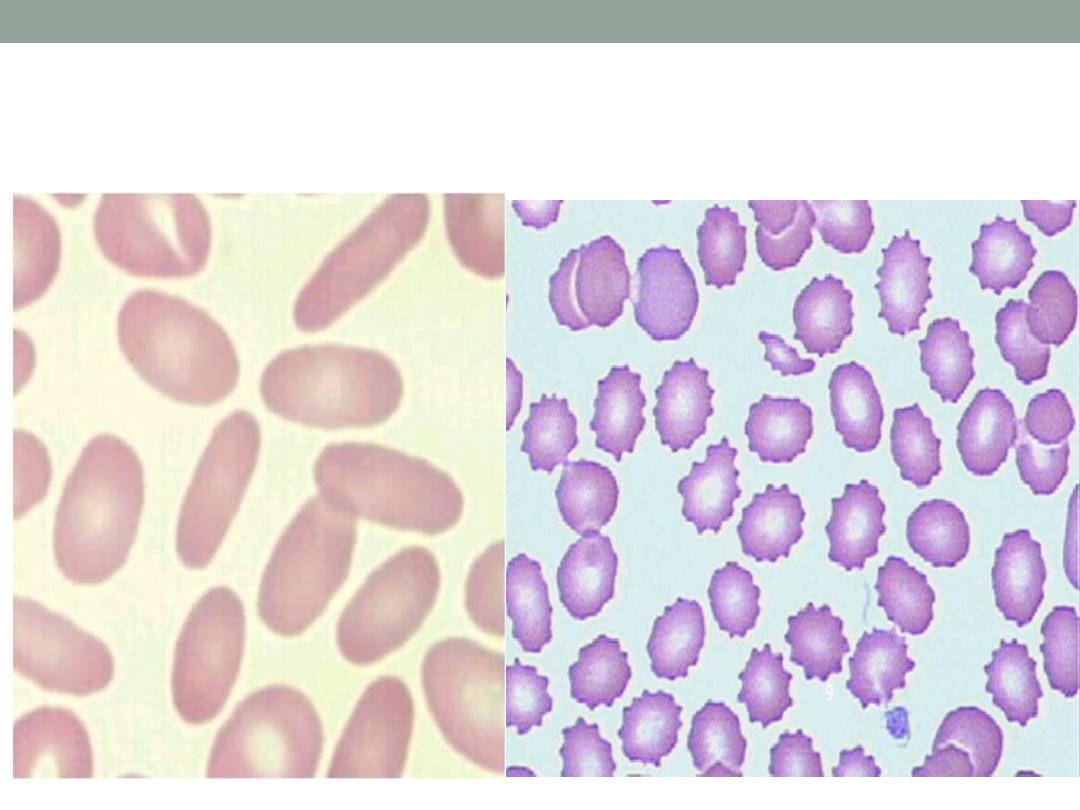
Burr cells( right ) , cigar shape cells (lt.)
2. Iron study ( s.iron , s.ferritin, TIBC) , S.B12 , RBC folate
(in case of megaloblastic anemia ) , & other investigations
according to the case ! .
3. Bone marrow aspiration & biopsy ( specially in case of
bi-cytopenia or pancytopenia .
Iron dificiency anemia
This occurs when there is iron loss or physiological requirements
exceed absorbtion.
1. Blood loss : the most common cause in men & post
menopausal women is GIT bleeding ( peptic ulcer , esoph.
Varices
, inflammatory bowel diseases , colorectal CA…)
Other causes including severe hemoptysis , hematuria …
In women with child bearing age , menstrual blood loss is a
contributing factor .
2. malabsorption: iron is actively absorbed in the upper small
intestine , so it can be affected by celiac disease , another point
is gastric acid required to release iron from food & helps to keep
iron in the soluble ferrous state , achlorhydria in the elderly or
that caused by drugs like PPI may contribute to the lack of iron
availability from the diet , as may previous gastric surgery .
3. Physiological demands :
This is occur when the iron requirements exceeding its
absorption , e.g. at time of rapid growth ( puberty ) & in
pregnancy ( iron is diverted to the fetus & placenta ) .
Investigations of IDA :
1. Investigate the cause ( bleeding , malabsorption ,
parasitic infection..
2. s.iron ( LOW) . S.ferritin ( LOW , very specific, confirm
iron dificiency) , TIBC ( HIGH ) , transferrin saturation ( iron
/TIBC * 100 ) ( LOW ), Bone marrow iron store ( rarely
used ) .
Management of IDA
1. Treatment of the underlying disease .
2. Iron replacement therapy :
Ferrous sulphate 200 mg 3 times daily for 3-6 months is
appropriate , in patient who cannot tolerate oral form due to
GI side effects , parentral form is available like iron dextran
or iron sucrose & more recently iron isomaltose & iron
carboxymaltose ( preferred , fewer allergic reactions ).
Failure to respond to treatment may be due to non
compliance , continued blood loss , malabsorption , or even
another diagnosis ! .
Blood transfusion is usually not necessary unless severe
anemia with angina or heart failure or cerebral hypoxia.
Megaloblastic anemia
Result from dificiency of vitamin B12 or folic acid
•
Causes of vit. B12 dificiency :
.1
1.Dietary dificiency : occur in strict vegans .
2. Gastric pathology :release of B12 from food require normal acid
secretion , therefore hypochlorhydria or gastric surgery ( gastrectomy
)associated with B12 dificiency .
3. Pernicious anemia : autoimmune disease , charactarized by atrophic
gastric mucosa , loss of parietal cells & intrinsic factor dificiency , it may
be associated with other autoimmune diseases ( vetiligo , graves dis. ,
hashimoto thyroiditis, addison
…) , the finding of anti intrinsic factor
antibodies in the context of B12 D- is diagnostic of pernicious anemia ,
other Ab include antiparietal cell Ab ( present in over 90% of pernicious
anemia , but also present in 20 % of normal females) , schilling test is
no longer used .
4. Small bowel pathology : e.g , bacterial overgrowth , fish
tapeworm , IBD (
crohn”s disease ) & surgery .
Causes of folic acid dificiency
:
1. Diet : poor intake of vegetables.
2. Malabsorption : e.g. celiac disease
3. Increase demand : e.g. pregnancy , hemolysis
4
. Drugs : e.g. phenytoin , methotrexate…
Note :
Vit. B12 D- ( but NOT folic acid D- ) , is associated with
neurological disease up to 40 % of cases , the main
pathological finding is focal demylination affecting the
spinal cord ( subacute combined degeneration of the cord )
, peripheral n. , optic nerve & cerebrum . Manifestations
include peripheral parasthesia & ataxia of gait . So the
most coomon presentation is sensory .
Neurological finding in B12 D- :
* Peripheral n.: glove & stocking pararsthesia, loss of ankle
reflexes
*spinal cord : subacute combined degeneration of the cord
, mainly affecting the posterior column ( vibration & position
sensation )
*cerebrum : dementia , optic atrophy
*autonomic neuropathy .
Investigations ( megaloblastic anemia)
-Hb : low , sometimes severly reduced
-MCV: high , often more than 120 fl .
-WBC: norrmal or reduced
-Platelets : normal or reduced
-Reticulocytes : low
-Blood film : oval macrocyte , poikiloctosis , hypersegmented
neutrophil
-Bone marrow : increased cellularity , megaloblastic changes in
the erythroid
series , increase iron store…
-LDH : Elevated
-homocystein elevated in both folic acid & B12 D- ,
methylmalonic acid elevated only in B12 D-.
- s. B12 assay
- s. folic acid , RBC folate ( accurate).
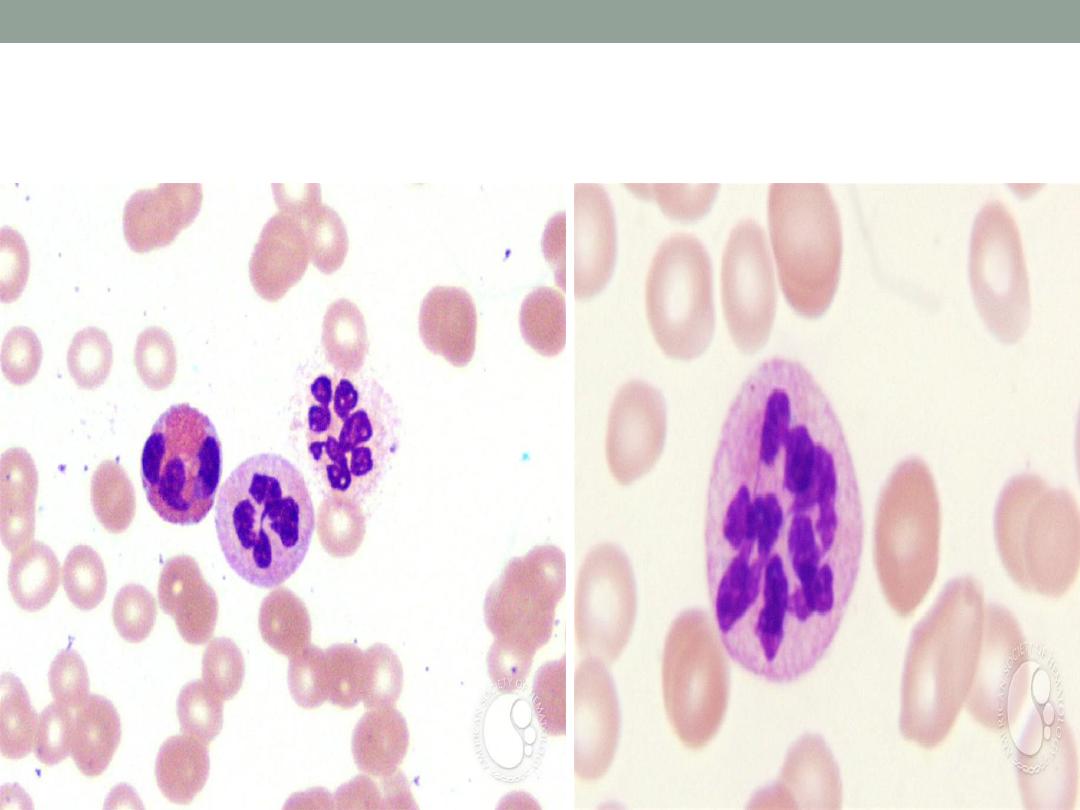
Hypersegmented neutrophil
Treatment of megaloblastic anemia
Important note :
The use of folic acid alone in the treatment of megaloblastic anemia
due to B12 D- my result in worsening of the neurological deficit .
VITAMINE B12
Treatment is usually by hydroxycobalamin 1000ug IM for 6 doses (
twice a week ) , followed by maintainance therapy of 1000 ug every 3
months for life .
The 1
st
response to treatment is increase in reticulocyte count within 5-
10 days , the Hb will rise by 10 g/l every week until normalised , be
ware of hypokalemia after starting treatment ! ( when u give B12 , you
are building new cells , these cells will take up potassium ) .
** when there is inadequate response to treatment & there is dimorphic
picture ( mixture of microcytic & macrocytic cells ) , think of
concomittant iron D- anemia .
** neurological symptoms & signs my take 6-12 months to improve &
sometimes the damage is permenant .
FOLIC ACID D-:
oral folic acid 5 mg daily for 3 weeks will treat acute
dificiency & then 5 mg once weekly is adequate
maintainance therapy .
Prophylactic folic acid in pregnancy is important to prevent
neural tube defect in the fetus , folic acid also given in
hematological diseases associated with reduced RBC life
span like hemolysis.
Recent studies stated that folic acid can reduce the risk of
coronory & cerebrovascular diseases by lowering
homocystein level !.
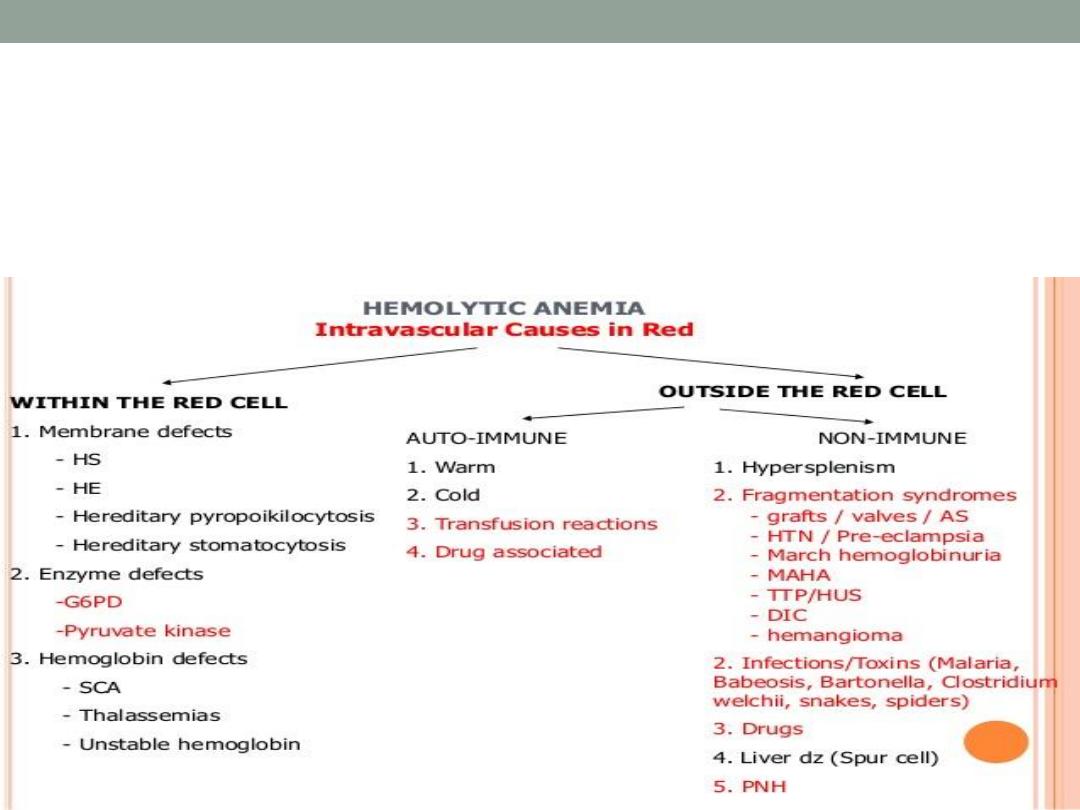
Hemolytic anemia
Hemolysis means shortening of the normal RBC lifespan (
less than 120 days) by inherited or acquired causes .
Investigations indicating active hemolysis
1. Low Hb
2. Increase indirect bilirubin
3. Increase LDH
4.Increase reticulocytes
5. Increase urinary urobilinogen
Features of intravascular hh :
1. Decreased haptoglobin
2. Increase methaemalbumin
3. Positive urinary hemosiderin
4. Haemoglobinuria
In most hemolytic states , the hemolysis is predominantly
extravascular ( in the reticuloendothelial system like liver &
spleen)
Less coomonly red cell lysis occur within the blood stream , i.e.
intravscular hh
causes of intravascular hh :
1. Transfusion reaction
2. PNH ( paroxysmal nocturnal hemoglobinuria)
3. Infections ( malaria , clost. Perfringes)
4
.Mechanical : heart valves, DIC ) ….
Causes of extravascular hh :
1. hemoglobinopathy
2. Membrane defects
3. Autoimmune hh anemia.