Head injury 2 ( Dr Mohamed A. J. Al Tamimi)
1. Injuries severe enough to damage scalp may also damage the underlying skull2. A complete examination of the whole patient is mandatory
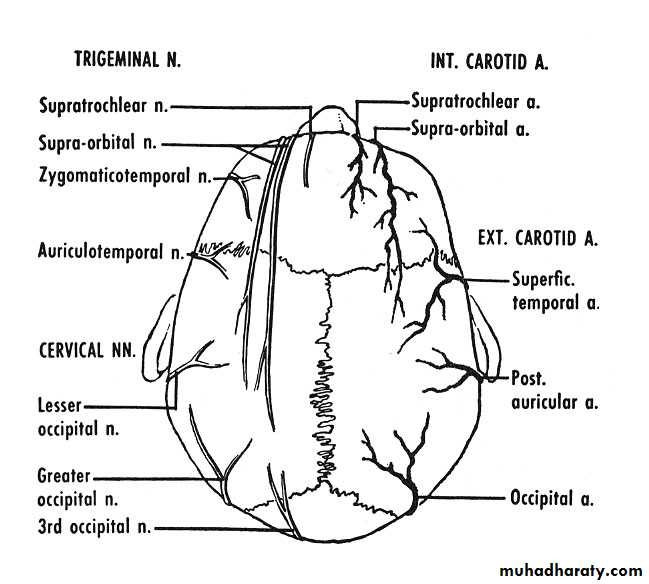
layers of scalp are
S Skin
C C.TA Aponeurotic (Galia)
L Areolar tissue
P Periosteum
Types
Lacerations Avulsions physical injuries Chemical injuriesScalp lacerations( classification)
Small and linear either superficial one (bleeder) or deep one (less bleeder) mostly closed under L.A in 2 layers (Galia and skin)Stellated and large either superficial one (bleeder) or deep one (less beeder) mostly closed under G.A especially in children, extensive debridement is unnecessary, all devitalised tissue should be derbided.
Reconstruction ladder
primary suturing in simple lacerations ,sharp, without tissue loss and gross contamination
secondary intention in wounds with minimum tissue loss
debridement and a split thickness graft in wounds with extensive tissue loss and intact pericranium
local flaps in wounds with extensive tissue loss and stripped pericranium and a split thickness graft for donor area (if a defect is left(
Pedicular flaps can be used if local flaps are not sufficient especially for occipital areas and small defects
Free tissue transplant is used for anterior and large areas
Scalp swelling and hematomas
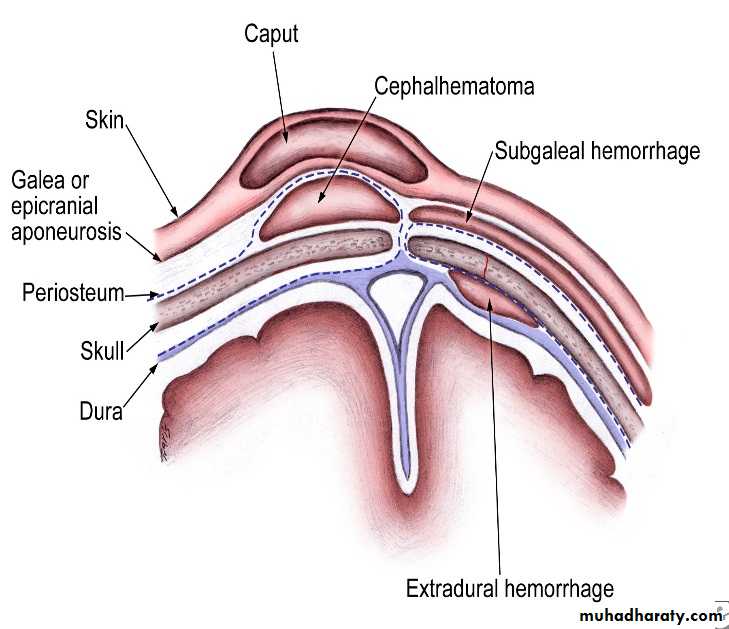
Caput succedanum
Cephal haematoma
Subgalial hematoma
Treatment for all is conservative \
hot sponging, serial HB correction)Don’t aspirate
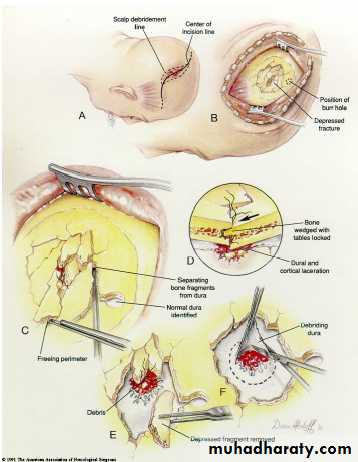
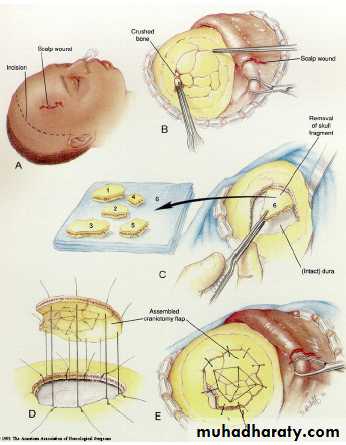
Skull fractures classification
1. by pattern (according to amount of energy,ratio of impact force to surface area)Comminuted, Depressed, Linear, Diastatic, Basal fractures, Growing)2. by type
Opened, Closed
3. by anatomic location
Basal, Convexity
Treatment roles
Comminuted (replacement as a cranioplasty if not infected with treatment of other associated injuries
Linear fractures (no treatment but observation if closed, debridement if infected and compound
Depressed(replacement as a cranioplasty if not infected, otherwise good debridement and craniectomy
Basilar skull fracture (observation for two days, avoid irrigation of the nose or ear, avoid probing, detailed auditory and vestibular examination is performed at6 weeks interval
Frontal sinus fracture (if in the posterior wall cranialization is necessary
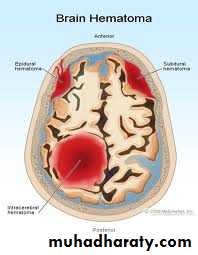
Types of traumatic intracranial leasions
Focal (epidural hematoma-subdural hematoma-brain contussion-intracerebral hematomas-focal subarachnoid hematomaDiffused (subarachnoid hemorhage-diffused axonal injury-concussion)
Traumatic intracranial hematomas
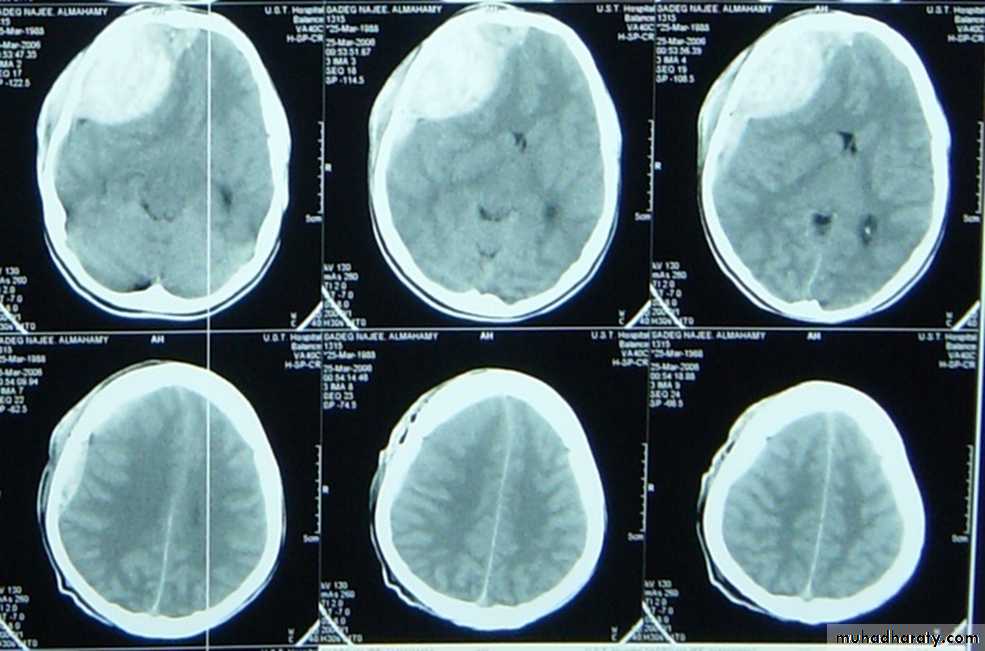
Acute subdural
Caused by accelerate high speed impact resulting into tearing of bridging veins or bleeding from cortical vessels, venous sinuses. acute brain trauma may coexist with altered level of consciousness and focal neurological deficit are common. Diagnosis is by CT(crescent hyperdense extraaxial mass) and rapid evaluation are necessary. the treatment depends on many factors such If no signs of rapid deterioration or progressive neurological deficit with no mass effect on CT so observation and control of intracranial p. is necessary, otherwise surgery is the role)
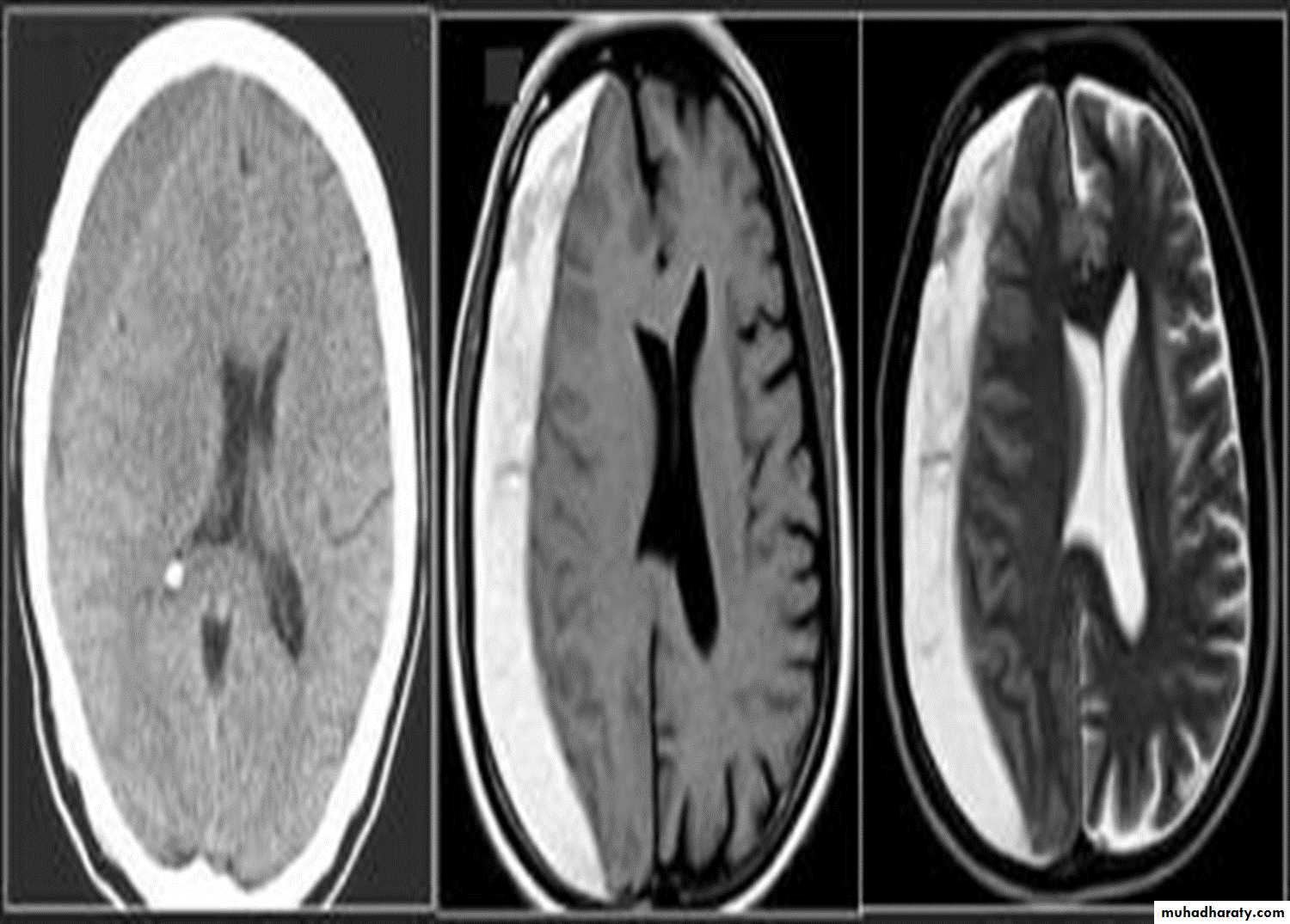
Chronic subdural
Mostly occurs in those over 50 years old,½ of patients have got no history of trauma (If there is any history of trauma then it is trivial), Alcoholism, epilepsy, coagulopathy are common, Dementia is common presentation. The treatment is medical In minimal neuological deficit. If not successful or with deterioration of neurological picture so surgery is the role by burr hole evacuation.( the CT picture is hpodense crescent exraaxial mass)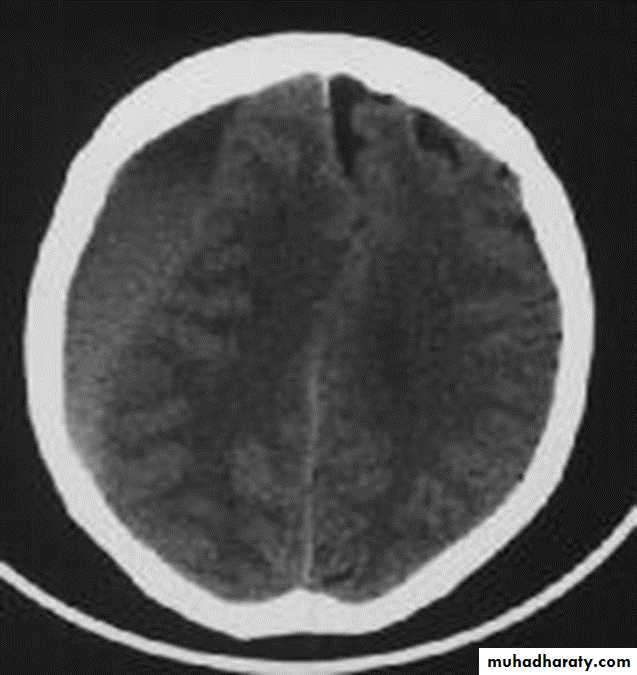
Extradural hematomas
Mostly resulting from meningial vessel tear (arteries > Veins > sinuses) and Fractures are common associated injury. Severe associated brain injury is rare. Usually the Level of consciousness is variable(lucidity interval is common). The haematoma with mass effect must be evacuated within ½ hour. if small follow up is recommended. The Prognosis depends on level of consciousness at time of presentation ( C picure is that of biconvex or lense hyperdense exrtracranial mass)
Cerebral contusions
It is a macroscopical focal laceration of brain tissue. Level of consciousness depends on size of contusion and location and the CT picure is that of irregular focal mixed densi intraaxial mass. Therec are 3 types, coupe, counter coupe and intermediate coupe). Small and deep ones needs follow upwhile Large with mass effect ones need lobectomy. the Large one may herniate as late as 9 days post trauma.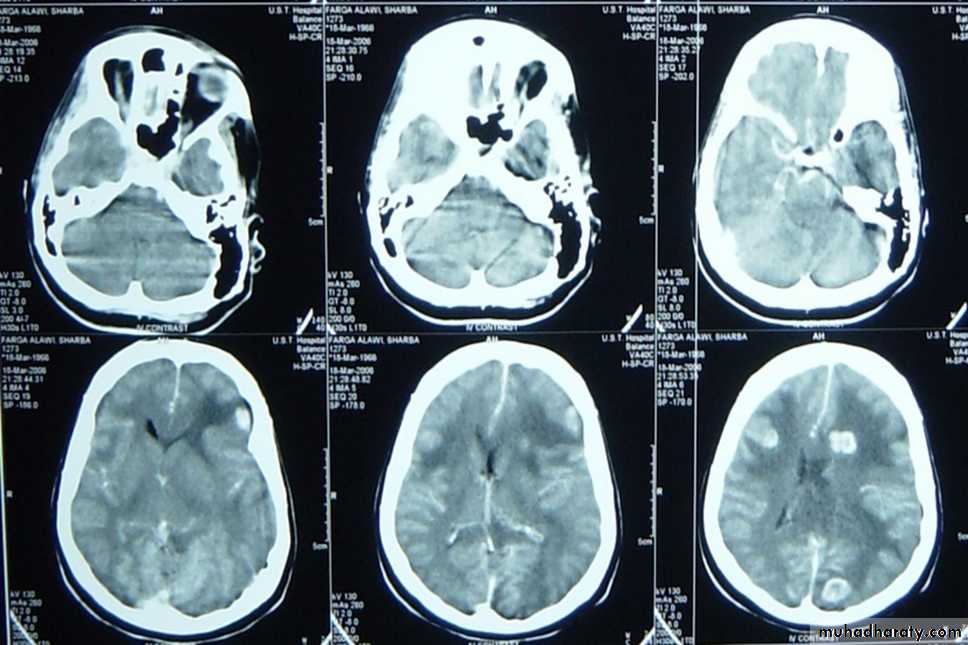
Subarachnoid bleeding
Diffused post traumatic bleeding in the subarachnoid space resulting from acceleration decceleration global forces ,the patient presents with agitation and LOC. Treatment is conservative plus measures to decrease intracranial pressure

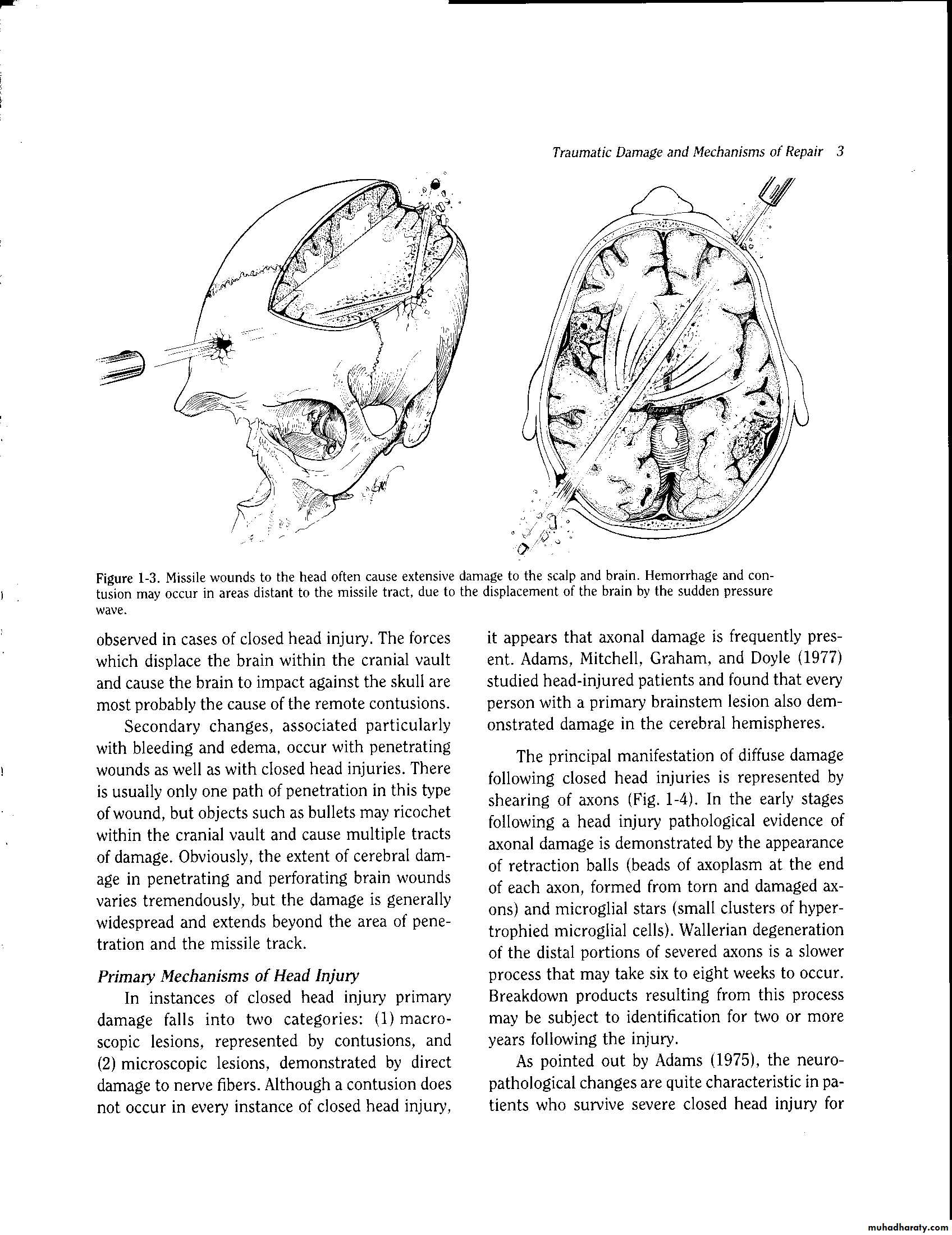
Penetrating head injuries
Sonic waves and cavitations and decavitation and secondary insults are the injurious mechanisms, Infection rates are high, Injury far away from site of entrance and exit is common. Control of homodynamic state is the initial management and Surgical interventions are limited to debridement and removal of mass hematomas and for selected cases. Prognosis is usually bad
Radiological evaluation for head injured patients
CT scan : almost without exception , an unenhanced (i.e.- non – contrast ) CT scan of brain suffices for patients seen in emergency department presenting after trauma or with new neurological deficit .The main emergent conditions to rule out :
1. blood ( hemorrhages or hematomas(
a. EDH ( extradural hematoma (
b. SDH ( subdural hematoma (
c. subarachnoid hemorrhage
d. intracerebral hemorrhage
e. intraventricular hemorrhage
2. hydrocephalus .
2.cerebral swelling
3.evidence of cerebral anoxia , loss of gray –white interface
4. skull fracture : linear , depressed , diastatic ….
5. ischemic infarction
6. pneumocephalus → air inside skull ( in skull fracture (
7. shift of midline structures
Indication for initial CT scan
A. moderate to severe head injury which criteria:
GCS less than 11
unresponsiveness
focal deficit
amnesia for injury
altered mental status
deterioration in neurological status
sign of basal or vault fractures
B. assessment prior to general anaesthesia for other procdures .
skull x ray:- it affect management of only 0.4-2% patients in most reports .
Skull x. ray may be helpful in following :-
in patients with moderate risk for intracranial injuries by detecting unsuspected depressed skull fracture
in patients with penetrating missile injuries
III . MRI :- usually not appropriate for acute head injuries while MRT is more sensative than CT, there were no surgical lesions demonstrated on MRI that were not evident on CT .
IV . arteriogram in trauma :- cerebral arteriogram useful with non missile penetrating trauma , also useful in experienced hands if CT is unavailable for diagnosing EDH .
Outcome prediction in severe head injury
neurological statusGCS
Brain stem function
Pupillary responsiveness .
age of patients younger children , infant and elderly patient had a poor prognosis
vital sign :- hypoxia , hypotension .
CT scan finding like brain shift or cisternal obliteration → poor prognosis .
increase ICP for those more than 30 mmHg after medical and surgical treatment → poor prognosis
Indications for admission to hospital in patient with head trauma
1. history
1. history of impaired consciousness or fits
2. progressive headache
.3. vomiting
4. post traumatic amnesia > 30 min
5. Dizziness or blurring of vision .
6. unreliable or inadequate history .
7.unaccompanied patient or patient with diffuclt access to hospital
2. examination
8. any neurological abnormality or impaired consciousness .
9. evidence of basal or depressed fracture .
10. suspected skull penetration .
3. difficult to assess
11.all children under 6 years
12patient under the effect of alcohole or drugs.
4.Radiological evaluation:
13. all skull fracture .
14. abnormality on CT scan
5. Medical indication :
15. diabetic , hypertensive or with history of other chronic diseases
16. patient under treatment with anticoagulant , insulin or other potential drugs
Complications of head injury
infections :- meningitis , abscess
CSF fistula
chronic subdural hema toma
late epilepsy
post concussion syndrome
carotid cavernous ( cc fistula )