Central Nervous System Infections
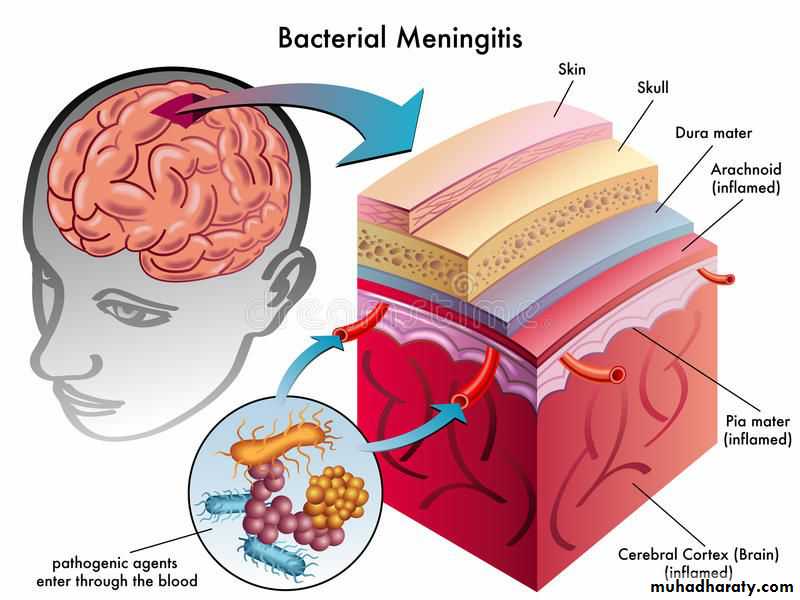
Viral and Bacterial Meningitis
Central Nervous System InfectionsViral infections of the CNS are much more common than bacterial infections, which in turn are more common than fungal and parasitic infections.
Meningitis: means primary involvement of the meninges.
Encephalitis: indicates brain parenchymal involvement.Meningoencephalitis: involvement of both.
Brain abscess is the best example of a focal infection of the CNS.
Acute Bacterial MeningitisEtiology
1- In the neonatal period (0–28 days): Groups B streptococci,E.coli, Klebsiella and Listeria monocytogenes
2- Infants & children (2 mo. to 12 yrs. of age) N. meningitides,
then S. pneumoniae and H. influenzae type b
3- Those with underlying immunologic or anatomic (splenic dysfunction ) disorders increase the risk of meningitis from less common pathogens such as Pseudomonas aeruginosa, pneumococcal pneumonia ,Staphylococcus aureus, coagulase-negative staphylococci, Salmonella spp. and Listeria monocytogenes.
• Epidemiology
• The major risk factors for meningitis include:• Young age (neonates & young infants).
• Recent colonization with pathogenic bacteria paranasal sinusitis, otitis media, mastoiditis, orbital cellulitis, cranial or vertebral osteomyelitis , penetrating cranial trauma or meningomyeloceles..
• Close contact (household, daycare centers) with individuals having disease transmission through respiratory tract secretions or droplets.
• Poverty and male gender.
•

orbital cellulitis
• 5. infants and young children with occult bacteremia.• 6. Specific host defense defects like
• Complement system (C5–C8) defect recurrent meningococcal infection.
• Defects of the properdin system lethal meningococcal disease.
• Splenic dysfunction (sickle cell anemia) or asplenia pneumococcal.
8- Those with meningomyelocele staphylococcal
9- Those with CSF shunt coagulase-negative staphylococci.
• Damage to the cerebral cortex occurs due to vascular occlusion ,hypoxia, bacterial invasion , toxic encephalopathy , elevated ICP, ventriculitis , and subdural effusions.
• Cerebral infarction, resulting from vascular occlusion due to Inflammation , vasospasm , and thrombosis
• Vascular and parenchymal cerebral changes will occur result in vasculitis, , thrombosis of small cortical veins, occlusion of major venous sinuses, necrotizing arteritis producing subarachnoid hemorrhage.
• Inflammation of spinal nerves and roots produces meningeal signs, and inflammation of the cranial nerves produces cranial neuropathies of optic, oculomotor, facial, and auditory nerves.
Pathology & pathophysiology
• ↑ CSF protein may be due to ↑ vascular permeability of blood brain barrier with loss of albumin-rich fluid; whereas ↓ CSF glucose is due to ↓ glucose transport by the cerebral tissue.
Meningitis cause Increase Intracranial Pressure (ICP) by several
mechanisms include:-1. Cerebral edema; it is due to cytotoxic, vasogenic or interstitial
edema.2. Hydrocephalus; it is mainly communicating HC due to adhesion
of the arachnoid villi.3. SIADH (syndrome of inappropriate antidiuretic hormone
secretion).4. Subdural effusion
The onset is either sudden or insidious.
• Sudden onset : is less common
• manifestation & associated with• rapidly progressive manifestations
• of shock , purpura, DIC, and
• ↓ consciousness which often progress
• to coma or death within 24 hr.
• Insidious onset : is more common & manifested in infant as: nonspecific findings e.g. excessive crying , irritability, convulsions, fever ,in older children : convulsions, fever ,headache, anorexia, photophobia, myalgia, arthralgia , tachycardia, hypotension, & skin rash e.g. petechiae and purpura.
Clinical manifestations

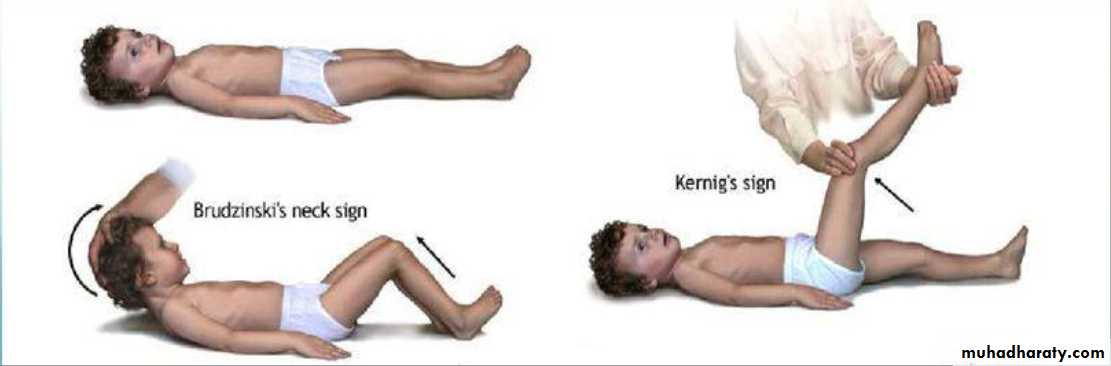
• In older children : Signs of meningeal irritation include nuchal rigidity, back pain, Kernig sign and Brudzinski sign.
• In infants : there is bulging fontanel
• & diastasis (widening) of sutures.
• Kernig and Brudzinski signs are
• not consistently present.

• Signs of Increased ICP include: headache, nausea, vomiting, cranial nerve palsy (especially the abducent & oculomotor); severe cases causing Cushing triad which include hypertension , bradycardia, & irregular respiration (apnea or hyperventilation).


Irregular respiration
Cushing triad• RR
BP
• PR
• Other signs include: papilledema, decorticate or decerebrate posturing, stupor, coma , or signs of herniation.• Note: Papilledema is uncommon in uncomplicated meningitis and usually suggest a more chronic process e.g. presence of an intracranial abscess.
• Seizures (focal or generalized) due to cerebritis , infarction, or electrolyte disturbances occur in 20–30% of patients with meningitis.
• Alterations of mental status
Investigations:
1-Lumbar puncture(LP) & cerebrospinal fluid(CSF) examination :During LP, the patient is placed
in the lateral position, but sick
neonates should be placed in
upright position.
The ideal interspace for LP
is L3-L4 or L4-L5 whichDetermined by drawing
horizontal line from
one anterior superior iliac
crest to the other.
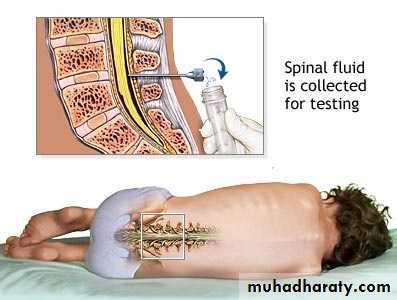
CSF should be sent for G-stain, culture, & biochemistry ( protein, sugar ,WBC with differential).
Turbid CSF is present when the CSF leukocyte count exceeds 200–400/mm3.
-The Gram stain is positive in 70–90% of patients with untreated bacterial meningitis.The analysis of CSF obtained from children already receiving antibiotics (partially treated meningitis), was negative on Gram stain and culture. Neutrophilic Pleocytosis, elevated protein level, and a reduced concentration of CSF glucose usually not affected.
Bacterial antigen may be detected in the CSF by agglutination test.
Bloody CSF indicated either traumatic LP or subarachenoid hemorrhage & these differentiated by centrifuged the CSF, if traumatic it become clear, but if hemorrhage it remain xanthochromic.
In traumatic CSF, WBC count & protein are affected, but G-stain, culture & glucose level not influenced.
-CSF sent also for:
• Lactate & LDH which may be high in bacterial meningitis• while normal in Viral meningitis.
• LP should be performed whenever bacterial meningitis is
suspected, but there are some CONTRAINDICATIONS for (immediate) LP include:-
1. Evidence of ↑ ICP e.g. ↓ consciousness, cranial nerve palsies, cushing triad, papilledema ; whereas bulging fontanel alone in infants is not a contraindication.
2. Severe cardiopulmonary compromise
3. Infection of skin that overlying the site of LP.
4. Thrombocytopenia is a relative contraindication for LP.
age
WBC(mm3)
Protein
(mg/dl)
Glucose(mg/dl)
Pressure
(mmH2o)
colour
Infant &
Older children
lymphocytes 5
neutrophiles Nill
20-45
60% of blood
glucose
50-80
clear
Normal value of CSF analysis:
CSF findings in CNS infections
WBC(mm3)
Protein
(mg/dl)
Glucose(mg/dl)
Pressure
(mmH2o)
Acute bacterial
meningitis
100-10,000 PMN
Predominate
(75-95%)
100-500
Decrease
(60% of
blood glucose)
Usually
elevated
Viral meningitis
or
encephalitis
Rarely 1000,PMN early but lymphocyte
predominate later
Normal or Slightly
elevated
(50-200)
Normal
Normal


2.Blood culture When LP is delayed, Blood culture should be taken (which is +ve in 80- 90% of cases), then empirical antibiotic therapy can be initiated.
3.CT scan for evidence of a brain abscess or increased ICP
4.CRP, ESR, and pro calcitonin have been used to differentiate bacterial (usually elevated) from viral causes of meningitis.Other investigations may include : CBP, blood urea, serum electrolytes, urine for specific gravity (for SIADH), & tests of coagulation function if there is evidence of DIC.
Treatment
It consists of supportive care& antibiotic therapy.
Supportive Care include:-
• ABC , Repeated medical and neurologic assessments especially in the 1st 72 hr e.g. chart for vital signs, fluid input & urine output, pupillary reflexes, level of consciousness…etc.• 2.Patients should initially receive nothing by mouth.
• Shock should be treated with fluid resuscitation +/- inotropic agents;• whereas if there is no hypotension , IV fluid should be restricted to
• half or two thirds of maintenance until it can be established that
• ↑ ICP or SIADH is not present, then full maintenance can be given.

• Empirical antibiotic therapy can be initiated after taken CSF culture as :
• IV Dexamethasone use for 1`2 days to patients• Vancomycin vial Cefotaxime vial or Ceftriaxone
• until the result of culture appear then change the treatment accordingly .
Antibiotic Therapy:-
S. pneumonia is sensitive to Vancomycin .H. influenza is sensitive to Cefotaxime or Ceftriaxone.
N. meningitides is sensitive to Penicillin G .
Note: 3rd generation cephalosporins are also effective in N. meningitides & β-lactam- sensitive S. pneumonia infection.
L. Monocytogenes ( in neonate ) is only sensitive to Ampicillin.
Duration of antibiotic Treatment in uncomplicated meningitis as follows:-
N. Meningitides for 5-7 daysH. influenza for 7-10 days
S. pneumonia for 10-14 days
• 2.↑ ICP can be treated by:
• head elevation, restriction of IV fluid, furosemide (1 mg/kg) or mannitol , and endotracheal intubation with hyperventilation. Glycerol has also been used to ↓ cerebral edema by ↑ plasma osmolality & enhance cerebral circulation.
• 4. Seizures should be treated with IV diazepam (0. 3 mg/kg/dose) or lorazepam; for maintenance Treatment of seizures, give phenytoin which is better than phenobarbital because it produces less CNS depression
Corticosteroids use in meningitis to decrease release of cytokine-mediated inflammatory changes from the cells.
IV Dexamethasone use for 2 days to patients with meningitis specifically due to H. influenzae type b
that lead to shorter duration of fever , lower CSF protein and
lactate levels, and reduction in sensorineural hearing loss.
The maximum benefits of corticosteroids if given 1–2 hr before antibiotics are initiated.
Complications
• Acute Complications include: seizures, increased ICP, cranial nerve palsies, stroke, cerebral or cerebellar herniation, thrombosis of dural venous sinuses, SIADH, & DIC.Subdural effusions; it occur in the minority of patients
treated by aspiration.
Thrombocytosis, eosinophilia, and anemia may develop during therapy of meningitis.
Pericarditis or arthritis may occur after Treatment of meningitis, especially due to N. meningitides.Late complications(outcome) : 35% of patients have late sequelae, particularly after pneumococcal meningitis include:
1-Sensorineural hearing loss:
occurs in 30% of patients with pneumococcal meningitis,10% with meningococcal,
and 5–20% of those with H. influenzae type b meningitis.
It is due to labyrinthitis or direct auditory nerve inflammation.
2-recurrent seizures.
3-mental retardation.4-blindness.
5-behavioral problems & learning disabilities.
6-ataxia.
Factor associated with poor prognosis include:-
• Seizures that persist after the 4th day of illness or seizures that are difficult to control.• Coma or focal neurologic signs on presentation.
• High concentration of bacteria or low leukocyte count in the CSF.
• Infants < 6 mo.
Prevention
It is either by vaccination or antibiotic prophylaxis.
• S. pneumonia; pneumococcal vaccine is recommended for children
• < 2 yr of age and those at high risk e.g. asplenia or immunodeficiency.
No antibiotic Prophylaxis is required.
• H. influenza type b; Conjugated vaccines for Hib started at 2 mo of age. Rifampin once for 4 days should be given to all house-hold contacts (except pregnant women)
• N. meningitides; vaccine is recommended for high-risk children > 2yr, asplenia, immunodeficiency .
Rifampin for 2 days ; ciprofloxacin or ceftriaxone (single dose) also can be given. They should be given to all contacts (regardless of immunization status) e.g. household, daycare center, direct exposure to oral secretions .
Follow up
1- Daily assessment of:• Vital signs, body weight, urine output, OFC,& neurologic
assessment.
This important to detect the complications as early as possible & interfere rapidly such as:
• blood pr.& HR ICP
• body wt.& oliguria SIADH• OFC subdural effusion or hydrocephalus.
2- Long term follow up include monthly visit to check for OFC, mentality, vision, hearing.

Viral meningoencephalitis
Viral meningoencephalitis is the most common cause of CNS infection Et .
• Enteroviruses are the most common cause of viral• meningo-encephalitis. It spread directly from person to person
• Herpes simplex virus type 1 (HSV-1) is an important cause
• of severe sporadic encephalitis. Brain involvement usually is
• focal .
• Herpes simplex virus type 2 (HSV-2) may cause severe encephalitis with diffuse brain involvement in neonates .
• Varicella-zoster virus (VZV) may cause CNS infection (especially cerebellar ataxia) in associated with chickenpox.
The onset is generally acute, CNS signs and symptoms are preceded by a nonspecific febrile illness of a few days' duration.
In the infant the presenting manifestations are irritability and lethargy.
In older children are headache(frontal or generalized) and hyperesthesia.; adolescents frequently complain of retrobulbar pain. Fever, nausea and vomiting, photophobia, and pain in the neck, back, and legs are common. As body temperature increases, progressing to stupor with convulsions.Focal neurologic signs may be present, especially in HSV-1 which cause sever encephalitis, progression to coma & death occurs in 70% of cases without antiviral treatment.
Loss of bowel and bladder control may occur. Skin rash may occurs with enteroviruses & measles infection.
CLINICAL MANIFESTATION
• The onset is generally acute, CNS signs and symptoms are preceded by a nonspecific febrile illness of a few days' duration.• In the infant the presenting manifestations are irritability and lethargy.
• In older children are headache (frontal or generalized) and hyperesthesia.;
• adolescents frequently complain of retrobulbar pain. Fever, nausea and vomiting, photophobia, and pain in the neck, back, and legs are common. As body temperature increases, progressing to stupor with convulsions.
Other manifestations include:
Focal neurologic signs may be present, especially in HSV-1 which cause sever encephalitis, progression to coma & death occurs in 70% of cases without antiviral treatment.Loss of bowel and bladder control may occur. Skin rash may occurs with enteroviruses & measles infection.
Enteroviruses may cause anterior horn cell injury and
acute flaccid paralysis. Exanthemas (skin rash) mayprecede or accompany the CNS signs, especially with
echoviruses, coxsackie viruses, VZV, measles, rubella.
Investigations
• CSF exam
• Serology of blood may be useful in determining of some viral CNS infection e.g. arboviral infection, but it is of no value in Enteroviruses.
• EEG show diffuse slow wave activity.
• CT & MRI show swelling of brain parenchyma.
Note: HSV encephalitis is suggested by focal seizures & focal finding on EEG, CT, or MRI especially if involve the temporal lobe.
Treatment
HSV encephalitis is treated with IV Acyclovir, for 2-3 wk.Otherwise, Treatment of viral meningoencephalitis is supportive.
Mild disease may require only symptomatic relief. More severe disease may require hospitalization and intensive care.
• Headache and hyperesthesia are treated with rest, non–aspirin- containing analgesics & reduction in room light, noise, and visitors.
• Fever ; acetaminophen.
• Vomiting ; phenothiazine.
• Poor oral intake ; IV fluids .Total parenteral nutrition may be required in prolonged coma.
Complications Guillain-Barre syndrome, Transverse myelitis, Hemiplegia, and Cerebellar ataxia.
Prognosis Most children recover completely from viral infections of the CNS, especially those due to enteroviruses, whereas others have high mortality rate e.g. HSV.
severe sequelae e.g. intellectual, motor, psychiatric, epileptic, visual, or auditory.
Prevention
Isolation of cases, vaccination is available for some viruses e.g.
rabies, varicella, & measles with control of vector for some viral infections e.g. arboviruses.

Thanks
The most common sequela associated with bacterial meningitis is :• Mental retardation
• Chronic seizure disorder• Impaired vision
• Impaired hearing
• Behavioral disturbance
The most common cause of viral meningoencephalitis is:
• An enterovirus
• Herpes simplex virus
• An arbovirus
• Mumps virus
• A respiratory virus
CSF result
sugar :45 mg/dl
Protien :100
Wbc :100 000 PMN
RBS:180 mg/dl