Fractures of the Mandible
A Fracture is defined as a breakage or discontinuity of bone structure (integrity)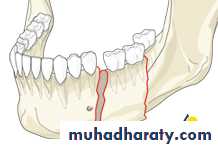
Surgical Anatomy:
*The mandible is basically a tubular long bone which is bent into a blunt V-Shape. The cortical bone is thicker anteriorly and at the lower border of the mandible, while posteriorly the lower border is relatively thin. Thus the mandible is "strongest anteriorly " in the midline with progressively less strength towards the condyle.Surgical Anatomy:


The mandible differs from all other bones in 2 important aspects:
1. Any movement inevitably causes both condyles to move with respect to the base of the skull.2. Although anatomically the condyles are the articular surfaces of the mandible, functionally the occlusal surface of the mandibular teeth observes this role.
The mandible is more commonly fractured than other bones of the face a fact directly related to:1. Its prominent and exposed situation.2. Blows to the mandible are transmitted to the base of the skull through the temporomandibular articulation (unlike the "match box-like" of midfacial skeleton which readily absorbs direct trauma)3. Lines of relative weakness as in cases of long canine tooth, partially-erupted wisdom tooth and unerupted teeth. The alveolar resorption which follows teeth loss weakens the mandible and #of the edentulous body will result from such smaller impact forces.
*The presence of the teeth in the mandible and maxilla is the most important
factor which makes #s of these bones entirely different from #s elsewhere1. The occlusion of teeth is a delicately balanced mechanism and any disturbance resulting from malunion of # leads to reduction in the masticatory efficiency and comfort, and so restoration of the occlusion is the prime aim in the treatment of #s of the mandible.
2. The presence of the teeth is extremely helpful in the reduction and fixation of #s.
3.Complete #s of the body of the dentatic mandible are open (compound) into the oral cavity and exposed to possible infection.
Classification:
A. According to the nature of injury:1. Civilian-type fracture: fractures with no gross comminution and noextensive loss of hard and soft tissue, which is mostly due to fights orroad traffic accidents.2. Gunshot-type fracture: fractures with gross comminution and there isextensive destruction of both hard and soft tissue, which is mostly due to missile injury.The main difference between fractures due to missile injuries and thoseresulting from blunt trauma can be enumerated as follows:1- Fractures are usually extensively comminuted.2- Fractures are always compound and the wounds contaminated by foreignmatter and bacteria
3- The Viability of the bone fragments and the extent of injury to teethcannot be accurately evaluated preoperatively from clinical and radiographic examination.
4- Wound treatment and the management of any underlying fracture is complicated by actual or potential composite tissue loss.
B. According to the type of #:1. Simple fracture:
2. Compound fracture3. Comminuted fracture
4. Pathological fracture
5. Complicated
6. Impacted
7. Greenstick


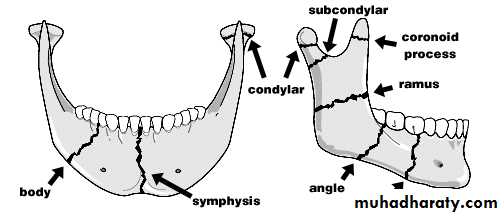
C. According to the site of #:It is the most useful one for practical purposes which is based on theanatomical location of the injury.1. Dento-alveolar
2. Condyle
3. Coronoid4. Ramus
5. Angle
6. Body7. Symphysis (Midline)
8.Parasymphysis (Canine region)
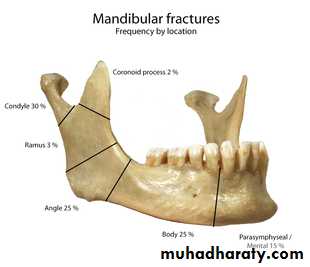
Condyle
30%Angle
5%
Bod
25%
symphysis/Para-symphysis
15%
Ramus
3%
Coronoid
2%
D. According to the cause of # :The direction and type of impact is the factor that determines the pattern ofmandibular injury. Mandibular #ts result from:1. Direct violence
2. Indirect violence
3. Excessive muscle contraction
E From the point of view of treatment :
the pattern of mandibular #s can be considered under the following headings:1. Unilateral2. Bilateral # s
3.Multiple #s
4. Comminuted #s
Clinical Examination:1. General examination of the patient2. Local examination of the mandibular fracture
General examination of the patient:Fractures of the mandible caused by trauma of vary degrees of severity, and this trauma may also cause injury elsewhere in the body. A thorough examination should be done (head, chest, abdomen, and extremities). Thepatient should be carefully inspected and palpated because the patient may have cerebral hemorrhage, fractured vertebrae or other bones or intra abdominal hemorrhage. Failure to diagnose any of these injuries might result in a surgical disaster; in addition, the medical history should be taken.
Local examination of the mandibular fracture:First of all the face and the mouth should be gently cleaned with wet gauze to remove the caked blood for accurate evaluation of the soft tissue laceration and bleeding source. Any foreign body as avulsed tooth, fractured fillings or dentures should be removed to keep patent airway tract.
The local examination of mandibular fracture consists of:1. Extra oral examination:I. Inspection: ecchymosis, swelling, soft tissue laceration, obvious deformity of the bony contour or anterior open bite.II. Palpation : by gentle palpation with the tips of the fingers over the condylar region bilaterally and then continued downwards a long the lower border of the mandible. There is tenderness over the fracture sites and feel step defect in the bone and bony crepitus. Also gentle pressure on the 2 angles or symphysis region (compression test) always elicits pain in fractured mandible.
2. Intra oral examination:I. Inspection: ecchymosis ,sublingual hematoma. The teeth should also carefully inspected if there is any avulsed, missing teeth or fractured fillings, and the inner surface of the lip should be examined.II. Palpation:
Common symptoms and signs Mandibular fracture:- Pain: especially on talking and swallowing- Numbness of the lower lip- Swelling and drooling- Trismus and difficulty in moving the jaw- Bone tenderness over fracture site- Altered occlusion- Loosened teeth and gingival bleeding- Mobility of fractured segment- Hematoma associated with fracture site, especially sublingual
Tooth in the fracture line:Teeth in the fracture line are a potential impediment to healing:1. The fracture is compound into the mouth via the opened periodontal membrane.2. The tooth may be damaged structurally and lose its blood supply as a result of the trauma so that the pulp subsequently become necrotic.3. The tooth may be affected by some pre-existing pathological process such asan apical granuloma.
Management Of Teeth Involved In A Mandibular Fracture Line:A. Absolute indications for removal of a tooth from the fracture line:1. Longitudinal fracture involving the root.2. Dislocation or subluxation of the tooth from its socket.3. Presence of periapical infection.4. Advanced periodontal disease.5. Already infected fracture line.6. Acute pericoronitis.7. Where a displaced tooth prevents reduction of the fracture.
B. Relative indications for removal of a tooth from the fracture line:1. Functionless tooth that would probably eventually be removed.2. Advanced caries.3. Doubtful teeth that could be added to existing dentures. (All teeth notcovered these conditions should be retained if possible.)
C. Assessment and treatment of a tooth retained in the fracture line:1. Good quality intra-oral periapical radiograph essential.2. Institution of appropriate systemic antibiotic therapy.3. Splinting of the tooth if mobile.4. Endodontic therapy if pulp is exposed.5. Immediate extraction if fracture becomes infected.6. Follow-up for 1 year and endodontic therapy if thee is demonstrable lossof vitality.
Characters, Signs and Symptoms of each mandibular fracture are:Dento-alveolar Fractures:Classification of dento-alveolar injuries:1. Dental hard tissue injurya. Crown infraction (crack of enamel or incomplete fracture)b. Crown fracture - Enamel onlyc . Crown fracture Enamel+ dentined . Crown fracture - Enamel dentine + pulpe . Crown-root fracture (vertical fracture)f. crown-root fracture (oblique fracture)g. Root fracture
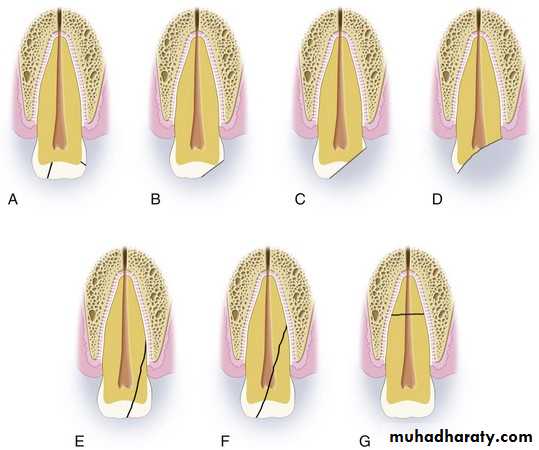
2. Periodontal injurya. Concussion (no displacement of tooth but tender to percussion)b. Subluxation (loosening of tooth without displacement)c. Intrusiond. Extrusione. Lateral luxation (loosening of
tooth with displacement) f. Avulsion
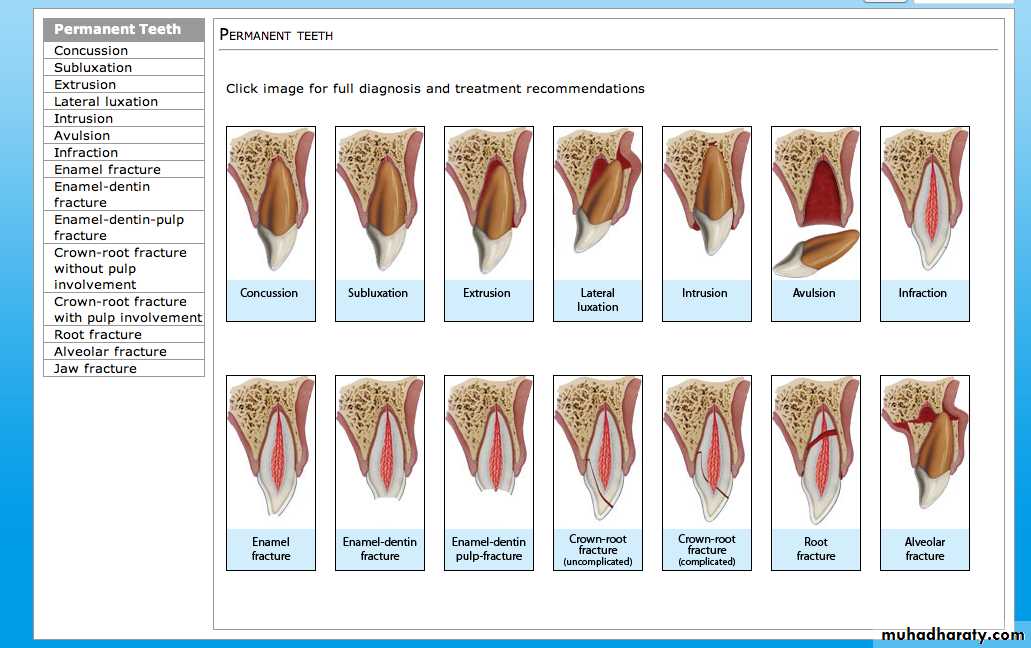
3. Alveolar bone injurya. Intrusion of tooth with comminution of socketb. Fracture of single wall of socket or alveolusc. Fracture of both walls of socket or alveolusd. Fracture of mandible or maxilla involving the alveolus and/ortooth Socket
4. Gingival injurya. Contusionb. Abrasionc. Laceration
5. Combinations of the aboveCondylar Fracture:
1. Contusion:2. Traumatic dislocation
3. Fracture:

Condylar fracture classified as extracapsular and intracapsulr fracture. The extracapsular fracture may exist with or without dislocation of the condylar head inferiorly, medially or laterally due to the pull action of the lateral pterygoid muscle which is attached to the anteromedial aspect of the condylar head. Features:1- Swelling and tenderness-hemorrhage from the ear ,Bruises in theregion should not be mistaken with Battle's sign associated withcranial base #s. clicking and crepitus on TMJ.2- deviation of occlusion towards the fracture side and this is especially obvious when the patient open his mouth. Mandibular protrusion is also limited and painful.
Condylar fractures can be classified according to:1. Age:
• Under 10 years• 10-17 years
• Adults
2. Surgical anatomy:- Involving joint surface: intra-capsular- Not involving joint surface: extracapsularHigh condylar neckLow condylar neck
3. Site:- Unilateral- Bilateral4. Occlusion:- Undisturbed- Malocclusion
Coronoid Process Fracture:This is a rare fracture. If the tip of the coronoid process is detached, thefragment is pulled upward towards the infratemporal fossa by the pull actionof the temporalis muscle.1. Intra oral ecchymosis on the coronoid process region.2. Tenderness on palpation over the region of the coronoid process.3. Pain and limitation of mandibular movement especially on protrusion.

Ramus Fracture:This is a rare fracture, may be simple or comminuted, the fragments aresplinted between the masseter and the medial pterygoid muscles and littledisplacement occurs.In both types of fractures; there are swelling, ecchymosis and tendernessmandibularon palpation over the ramus extra and intra-orally and painfulmovements.

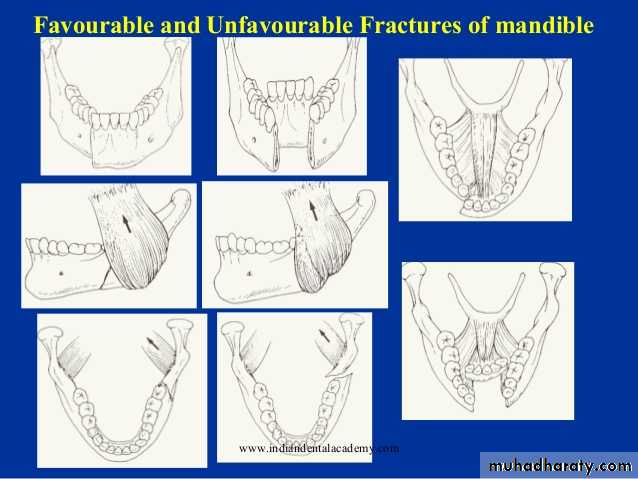
Angle Fracture:This is the most common fracture after condylar neck fracture. The angle is a weak area since it is the junction of the ramus and the body of the mandible, also the presence of an impacted mandibular third molar weakens the area. The fracture in this area may be classified as favorable and unfavorable fracture depending on the severity of posterior fragment displacement. The displacement depends on the pull direction of the masseter and / or the medial pterygoid muscles, and the direction of the fracture line vertically andhorizontally through the bone.
In practical view, if the fracture is relatively stable, itis considered a favorable fracture irrespective of the direction of the fracture line, also the presence of an erupted tooth in the posterior fragment which aid in the reduction and immobilization of such fracture regarded as favorable fracture. The signs and symptoms are ecchymosis, swelling, tenderness and bony step deformity.
Body Fracture:Little displacement of the fragments occurs in a unilateral fracture in thepremolar and molar areas. Fibers of the mylohyoid on either side of thefracture line probably play an important part in minimizing the displacementin this type of fracture. Features:1. Extra and intra-oral edema and ecchymosis.2. Derangement of the occlusion and deformity of the alveolus.3. Tenderness of the fractured region, and pain on mandibular movement.4. Unnatural mobility across the fracture site on gentle pressure.5. Anesthesia or paresthesia of the lower lip, if the inferior alveolar nerve isinvolved.
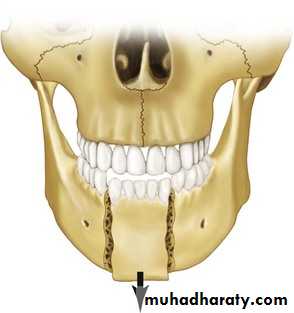
Fracture of the Symphysis (Midline):This fracture cause minimal displacement as the fracture line runs betweenthe genial tubercles, and the pull of the geniohyoid and the genioglossus muscles tends to impact the bone ends together. This fracture can be seen inepileptic patient due to fall directly on the chin. This fracture mostly associated with bilateral condylar fracture.
Para-syhyseal (Canine region) fracture:The fracture line running to one side of the genial tubercles and the displacement depend on the pull of the geniohyoid and genioglossus muscleswhich pull the greater fragment lingual to the lesser fragment.
Radiographical Examination
1. Intra-oral radiographs I. PeriapicalII. Occlusal and oblique occlusal
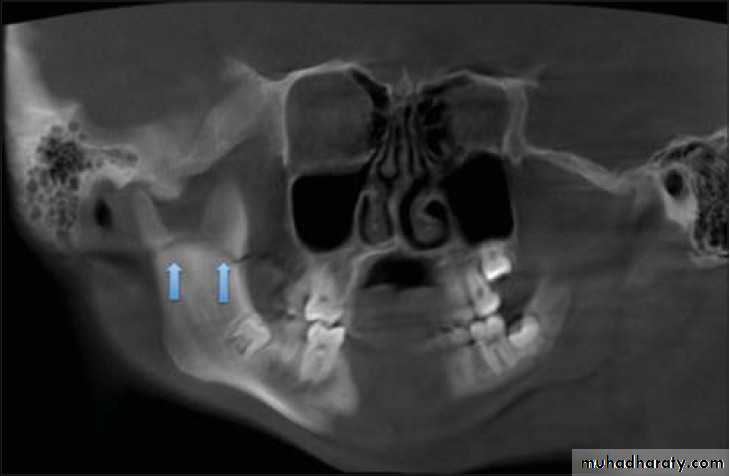
2. Extra-oral radiographsI. Oblique lateral of mandible (right and left side views); to evaluate thefracture line in the body, angle and condylar neck fracture.II. Postero-anterior view of mandible; to evaluate body and angle #together with the type of displacement.III. Panoramic tomogram, or orthopantomogram (OPT): the best single overallview of the mandible, including excellent view of the condyles.tic resonance imaging); which gives very accurate details.
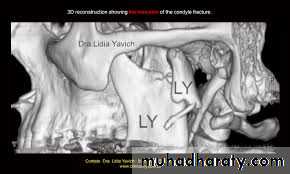
IV. Reverse Towne's view (elongated PA); to demonstrate fractures of thecondylar neck.v. Temporomandibular joint views (in open and close mouth); todemonstrate the presence of TM dislocation (Transcranial,Transpharyngeal, Arthrography, and Arthroscopy)VI. CT scan (computerized tomography scanning); to evaluate intracapsular fracture of the condylar head.VII. MRI
Definitive treatment:Factors affecting method of treatment of mandibular fractures:1. Fracture pattern.2. Skill of the operator.4. General medical condition of the patient.6. Degree of local contamination and infection.3. Resources available.5. Presence of other injuries.7. Associated soft tissue injury or loss.
The steps of definitive treatment consist of:A- ReductionB- Fixation and immobilizationC- Follow up and rehabilitation
A-Reduction:It is the process of approximation and repositioning ends of the fracturedbone in the proper position. The reduction is usually done under localanesthesia, or by giving sedation as 100mg pethidine or under generalanesthesia. There are two types of reduction:
a- Closed reductionThis reduction done by manual manipulation by elastic traction or by wires,without surgically exposing the fracture bone ends and no need for general anesthesia. Perfect reduction of the fracture is achieved, if the teeth arerestored to their normal alignment and normal bony contour.

b- Open reductionThis type of reduction done by manual manipulation after exposing the fracture bone ends surgically, usually under general anesthesia
Advantages of open reduction:1-The fracture can be reduced exactly by direct vision, so results in perfectapproximation of the fracture ends.2- For the refracturing of malunited or nonunited fracture in order to refreshthe bone ends from organizing connective tissue.
Disadvantages of open reduction:1- As the fracture area is exposed, there is more risk of infection.2- If done under general anesthesia, so more risk and cost to the patient.3- Submandibular or preauricular skin scar.
B-Fixation and immobilization:It is maintaining and securing the proper reduction until healing occurs. A simple guide to the time of immobilization for fractures of the tooth bearing area of the lower jaw is as follows:
If:a. Tooth retained in fracture lineb. Age 40 years and over add 1-2 weeksc. Patients who are smokersd. Mobile or comminuted fracturese. Children and Adolescents --------- subtract 1 week
With early uncomplicated treatment in a healthy young adult union can on average be achieved after 3 weeks
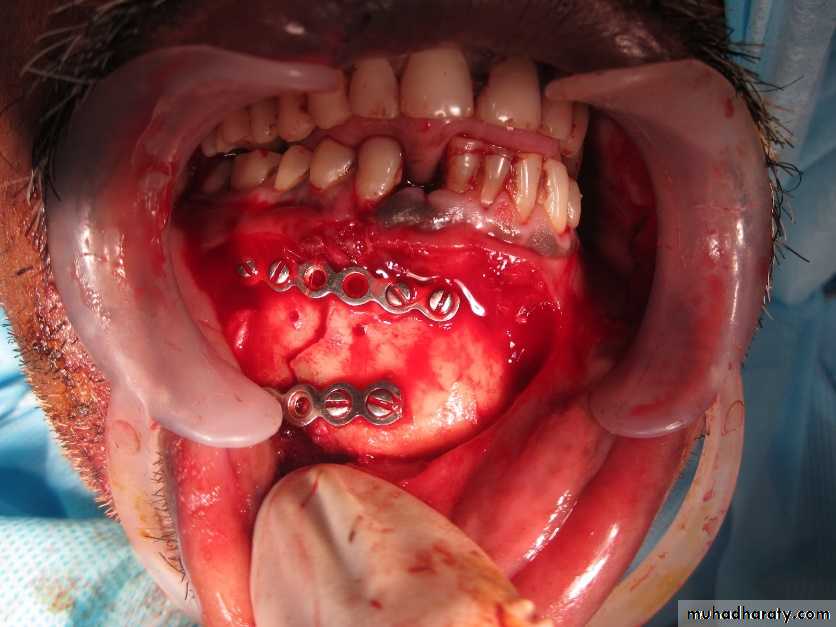
Methods of immobilization for fractures of the dentate mandible (Michael Perry 2015):a. Direct fixation (Osteosynthesis):- semi-rigid plates (manipulates)- Rigid plates (non-compression)- Compression plates- Lag screws- Resorbable plates and screws
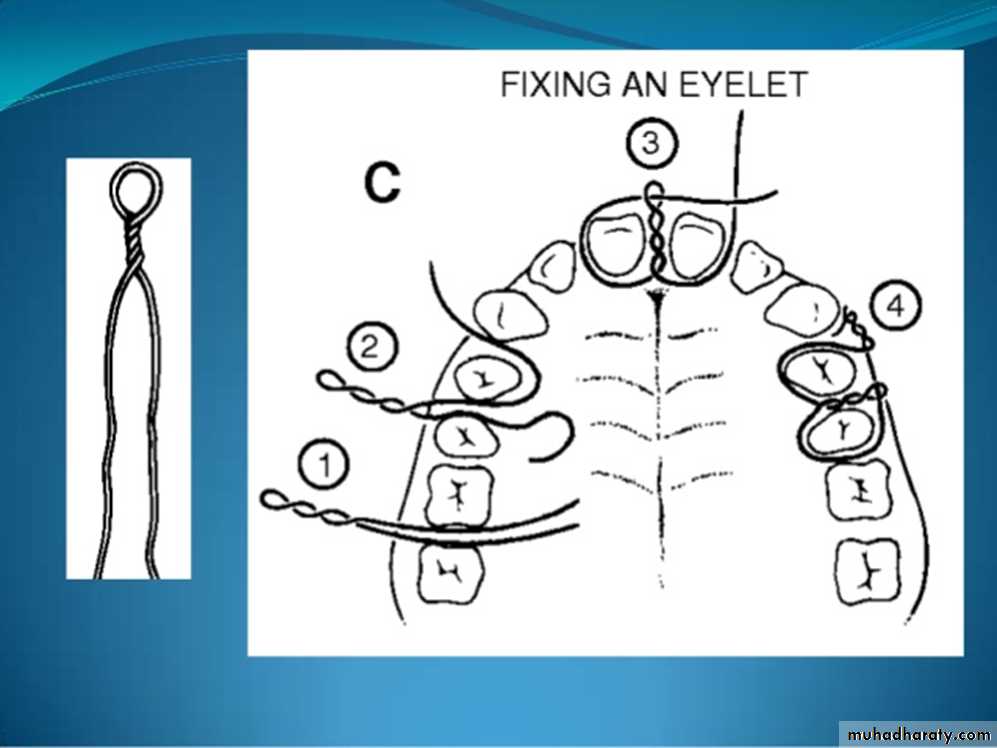
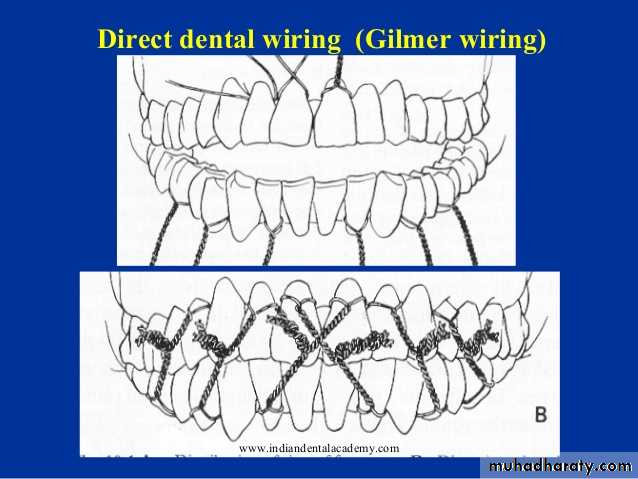
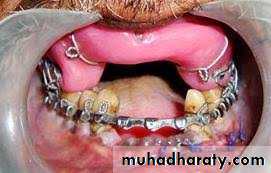
b. IMF:- Bonded orthodontic brackets- Inter-dental wiring (direct wiring. eyelet wiring etc.)- Arch bars- IMF Screws
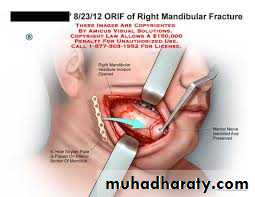
c. External fixationd. Other methods (largely historical or where plates not available)- Trans-osseous wiring- Circumferential wiring- Transfixion (kirschner wires)1.e. in most circumstances open reduction and internal plate fixation(ORIF: Open Reduction and Internal Fixation) is now the main form oftreatment for mandibular fractures.
Dental wiring:There are two types ofdental wiring:a. Direct wiring:
b. Interdental eyelet wiringc. Arch bar:d. modified Gunning type splints

Methods of immobilization for fractures of the edentulous mandible:a. Direct fixation (osteosynthesis):- Bone plates- Trans-osseous wiring
- Fixation supplemented by cortico-cancellous bone graft. b. Indirect skeletal fixation: - Pin fixation - Custom external fixator c. inter-maxillary fixation (using Gunning-type splints): - Used alone - Combined with other methods
Transosseous wiring:
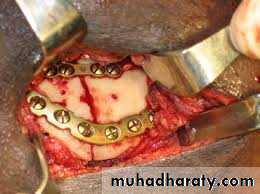
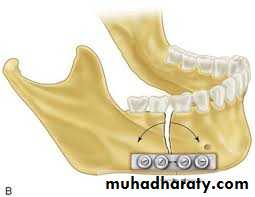
This method must not be used if the fracture is infected for the presence of metallic foreign body may cause bone necrosis and ulceration of the skin..Extra oral pin fixation:This method is rarely used because:1- May cause electrolytic action which may produce bone necrosis and2- The pin may project from the patient's jaw and may cause trauma and discomfort to the patient.Bone plating:The main advantage of bone plating is that it provides an extremely rigid fixation and therefore avoids unnecessary IMF at the conclusion of the operation and the patient can eat within few days after fixation.
(Rigid internal fixation is defined as: 'any form of fixation applied directly to the bones which is strong enough to prevent inter fragmentary motion across the fracture when actively using the skeletal satructure
The disadvantages of this method are:1. fracturing of the roots of the teeth2. metal fatigue fracture of the plate3. fracture of the small fragments of bone ends at the point of screw insertion4. scar5. infection and bone necrosis
Compression plates:
Trans-fixation:Fixation of fractures in the symphysis or angle region can be used afterreduction of the fracture by transfixing them with Steinmann pin orKirschner wire through the fragments. This method also called "ShishKebab" method.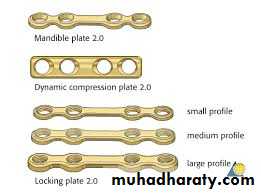

Fractures of the tooth bearing section of the mandible: synopsis1. Accurate reduction is essential if there is a good functional occlusion.2. All of these fractures are compound into the mouth.3. Teeth in the line of fracture are a potential source of infection and delayed healing. 4. The mandible can be immobilized by direct osteosynthesis, IMF or acombination of both.5. Non compression miniplate fixation is currently the preferred methodwherever the necessary resources are available.6. Although compression plating is based on sound general orthopedicprinciples these are less relevant to the treatment of mandibular fractures healing. than to the skeleton as a whole.7. Malunion is much more likely than non-union.
Definitive treatment of Condylar region fractureClinical management: an overviewCurrently there are 3 treatment options:1. Functional (conservative)2. Indirect immobilization (IMF3. Osteosynthesis (ORIF)
Indications for open reduction and fixation of condylar neck fractures:|Absolute indications:- Displacement of condyle into middle cranial fossa- Impossibility of restoring occlusion without ORIF- Lateral extra-capsular displacement- Invasion by foreign body (e.g. missile)
Relative indications:- Bilateral fracture with associated mid-face fracture (particularlywhere one condylar fracture is dislocated or angulated)- Bilateral fracture with severe open bite deformity- Unilateral fracture with dislocation. overlap or significantangulation of the condylar head- When inter -maxillary fixation is cotraindicated for medical reasons
Fractures of the condylar region: synopsis1. Fractures of the condylar region involve the temporomandibular joint eitherdirectly or indirectly.2. Permanent disturbance of function of the TMJ is common when carefully looked for but is usually not significant. Fractures that involve the subcondylar area in children can occasionally lead to significant disturbance of growth. Fractures into the joint space can result in fibrous or bony ankyloses that appears to be more common in some racial groups than others.3. All intracapsular fractures and all fractures in growing children should be treated Conservatively. Immediate or early mobilization should be encouraged. However, if the occlusion is disturbed IMF is applied and maintained until stable union can be expected to be present.
4. Significantly displaced subcondylar fractures in adults, particularly when there are bilateral fractures, should be treated by ORIF.5. Retromandibular or trans-parotid surgical approaches to the subcondylar region give rapid and sufficient access for the application of bone plates that must be of adequate strength.6. Treatment of fractures of the condylar region in all age groups is still less than ideal and although guidelines exist they remain to be evaluated fully.
C-Follow up and rehabilitation:The postoperative care of a patient with mandibular fracture may be dividedinto three phases:1- The immediate post-operative phase; when the patient is recovering from the general anesthesia until about one week:-
2.The intermediate postoperative phase, from 2nd week to 4th week; when the intermaxillary fixation is still in position-. 3-The late postoperative phase, from 4th week to 6th week
Fractures of the mandible in children: synopsis1. Modification of the principles of treatment is necessary to take account of:a. capacity for rapid bony union fractures are stable between I and3 weeksb. the mixed dentition and multiple buried developing teethc. potential interference with subsequent growth2. Accurate reduction less important as further growth will oftencompensate for occlusal discrepancies.
3. Direct osteosynthesis should be avoided if possible. However, plating orwiring the lower border may occasionally be indicated.4. IMF can be applied to deciduous teeth if needed but finer diameter wireshould be used. Bonded orthodontic brackets are preferred if possible.5. Fractures of the condyle require special consideration.6. A prolonged period of follow-up is important
Complications of Mandibular Fracture:1- Paraesthesia or anesthesia2- Skin scar3-Derangement of occlusion4 Ankylosis of TMJ
5- Mal-union, delayed union or non-union 6- Deformity of the mandible and malposition of the fragments 7- Pyogenic infection, gingivitis, actinomycosis 8- Traumatic myositis ossificans of the masseter muscle
Malunion:It means unacceptable malpostion and incorrect union of the fracture, usually as a result of imperfect reduction & fixation of the fracture. Post-reduction radiographs must always be taken to evaluate the union of the fracture. Mild malunion can be left without treatment in certain situations (children, edentulous); however, selective grinding or extraction of teeth may be sufficient in dentulous patients. Gross deformity of the bony contouror derangement of occlusion may necessitate surgical re-fracturing and immobilization.
Delayed union:If the time taken for a mandibular fracture to unite is unduly protracted it is referred as "delayed union". Bone fracture heals at different rates, in children takes less time than older patients. If union is delayed beyond the expected time for that particular fracture (taking the site and the patient's age into consideration) it must assumed that the healing process has been disturbed. Delayed union may be due to inadequate reduction and immobilization or infection at the fracture site.
Non-union:It means that the fracture is not only not united but will not unite on itsown. Radiographs show rounding off and sclerosis of the bone ends reveals acondition referred to as "eburnation", or the bone ends unite by fibroustissue "fibrous union'". Non-union of the fracture may be due to the presence of infection, presence of non-vital tooth in the fracture line, inadequate reduction and immobilization and insufficient blood supply to the bone ends.radiographs reveal marked eburnation of the bone ends or excessive boneloss or fibrous union, the fracture site should be explored surgically torefresh the fracture bone ends or bone graft may be required.
