NEOPLASIA
Dr Mustafa Salah Fadhil MSc, FIBMS pathDefinitions:
-Neoplasia = “new growth”.-A neoplasm can be defined as an abnormal mass of tissue, the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the same excessive manner after cessation of the stimuli which evoked the change.
-Cancer: all malignant tumors.
-Oncology (Greek oncos = tumor) is the study oftumors or neoplasms.
-The tumors arise from one clone that undergo genetic changes and uncontrolled proliferation.
All tumors have two basic components:
• Neoplastic cells.
• Supportive stroma; made up of connective tissue & blood vessels (providing blood supply and offering support).
Classification of tumors
• Tumors are classified according to their behaviour and histogenesis.• Behavioral classification: benign or malignant
• Histogenetic classification: cell or tissue of origin; epithelial or connective tissue
• Precise classification of individual tumors is important for planning effective treatment
Epithelial
MesenchymalAll epithelia
Fibrous tissue
Squamous
Bone and cartilage
Transitional
Muscle
Glandular
Fat tissue
Columnar
Nerve
Pseudostratified
Vessels
• Benign tumors
• Non-invasive and remain localized• Slow growth rate
•
• Close histological resemblance to parent tissue “differentiated tissue”
• Do not invade the surrounding tissues or spread to other sites
• Malignant tumors
• Invasive and thus capable of spreading directly or by metastasis• Relatively rapid growth rate
• Variable histological resemblance to the parent tissue
• Malignant neoplastic cells show a greater degree of atypical nuclear changes, with enlargement of the nucleus, darker staining (hyperchromasia) and more variability in nuclear size, shape and chromatin clumping (pleomorphism)
• Not all tumors categorized as malignant exhibit metastatic behaviour. For example, basal cell carcinoma of the skin (rodent ulcer) rarely forms metastases, yet is regarded as malignant because it is highly invasive and destructive
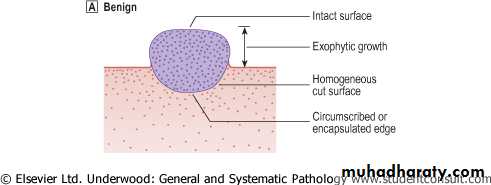
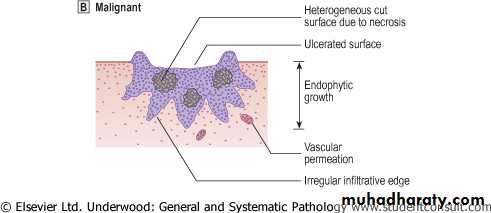
Benign VS Malignant
•
Nomenclature of tumors:
1- Nomenclature of benign tumors:By attaching suffix -oma to cell of origin
**Benign connective tissue (mesenchymal) tumors have a prefix denoting the cell of origin
e.g.:Benign tumor of fibroblastic cells →fibroma
Benign cartilaginous tumor →chondroma.
Benign tumor of adipose tissue →lipoma
Benign tumor of bone → osteoma
Benign tumor of vessels → angioma

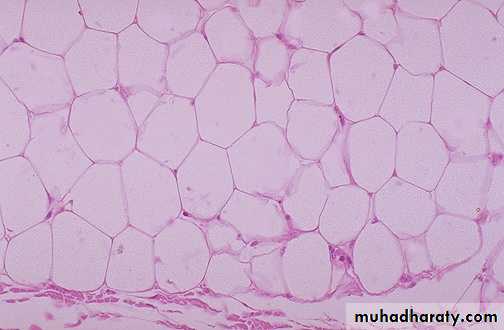
Lipoma (benign tumor of adipose cells)

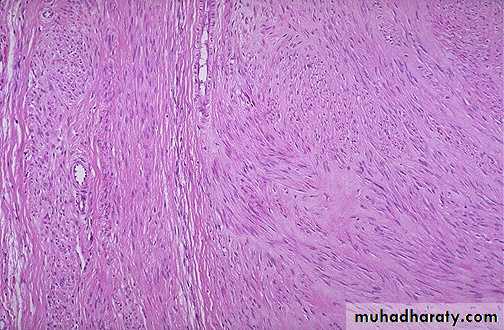
Leiomyoma (benign smooth muscle tumor) of the uterus

Capillary hemangioma, microscopically , dermal proliferation of small blood vessels lined by endothelial cells and containing RBCs.
** Benign epithelial tumors are more complex variously classified according to:
1-Cells of origin2-Microscopic &/or macroscopic appearance
-Papilloma: tumor arising from covering epithelia & producing micro- or macro- visible finger-like (warty) projections from epithelial surfaces, e.g. squamous papilloma arising from tissue that lined by stratified squamous epithelium like skin, esophagus….
-Polyp: producing macro. visible projection above mucosa e.g. Adenomatous polyp of stomach & colon.

Squamous cell papilloma, finger like projections, lined by several layers
of benign looking squamous cells, with central fibrovascular core.

Adenomatous polyp of colon
-Adenoma: benign tumor arising from glandular epithelia or forms glandular structure e.g. renal cell adenoma, breast adenoma, thyroid adenoma……-Cystadenoma: adenoma forming large cystic space(s) e.g. ovarian cystadenoma.
-Papillary cystadenoma: as above + papillary projections e.g. ovarian papillary cystadenoma
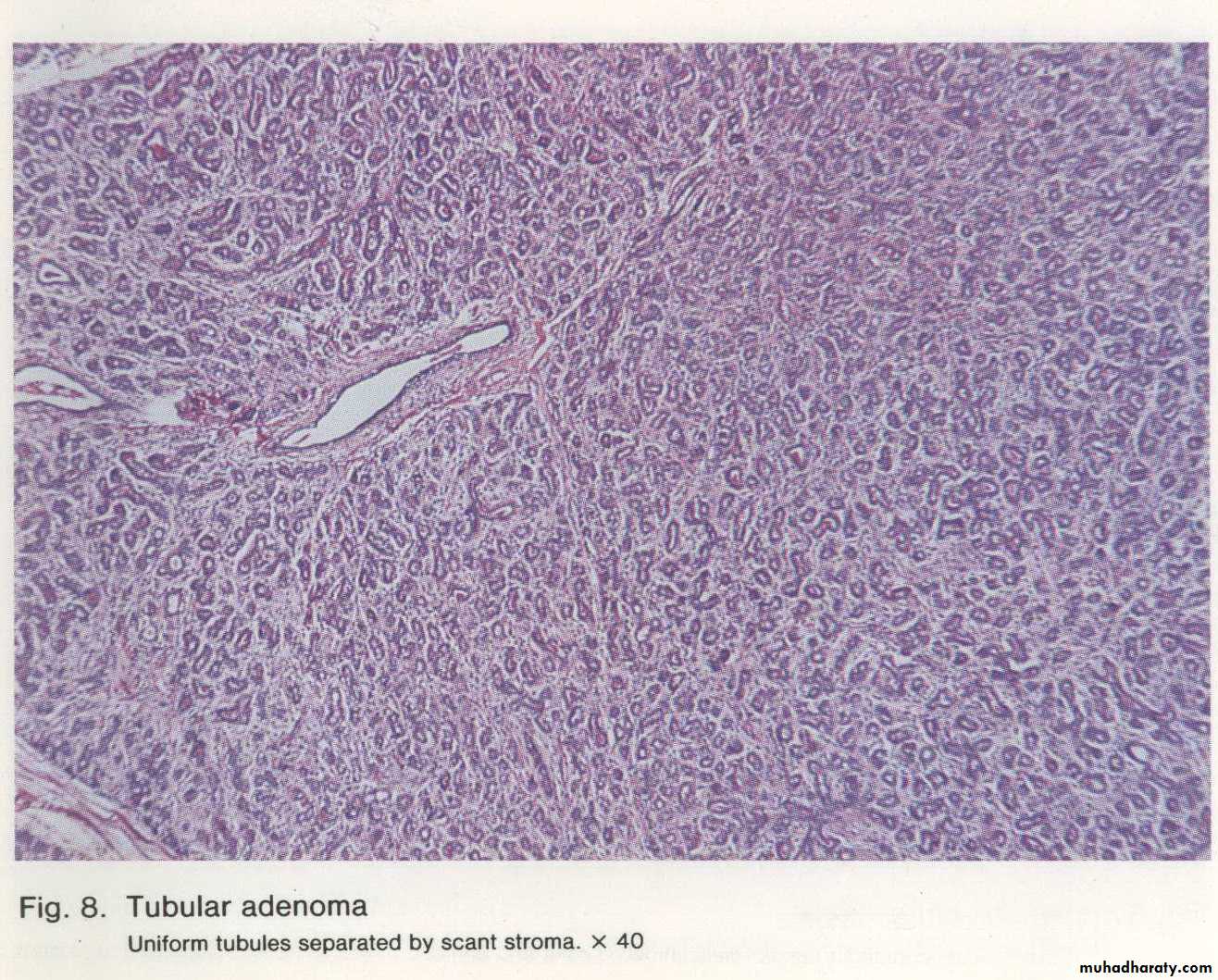
Breast adenoma: uniform tubules separated by scant stroma.
Ovarian cystadenomaOvarian papillary
cystadenoma
2-Nomenclature of malignant tumors:
**Malignant tumors arising in solid mesenchymal connective tissues are called sarcomas (Greek sar = fleshy), e.g.- Fibrosarcoma (fibroblast)
- Liposarcoma (lipocytes)- Leiomyosarcoma (smooth muscle cells)
- Rhabdomyosarcoma (striated muscle cells).
- Angiosarcoma (vessels)
- Osteosarcoma (bone)
- Chondrosarcoma (cartilage)
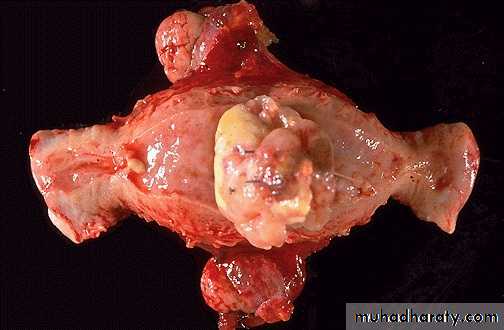
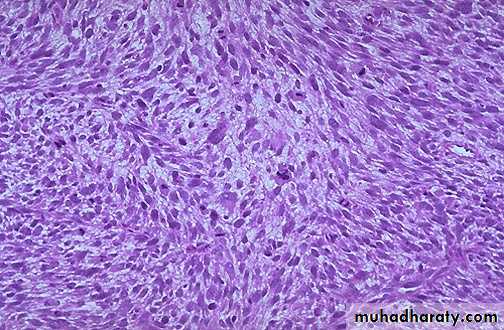
Leiomyosarcoma of the uterus
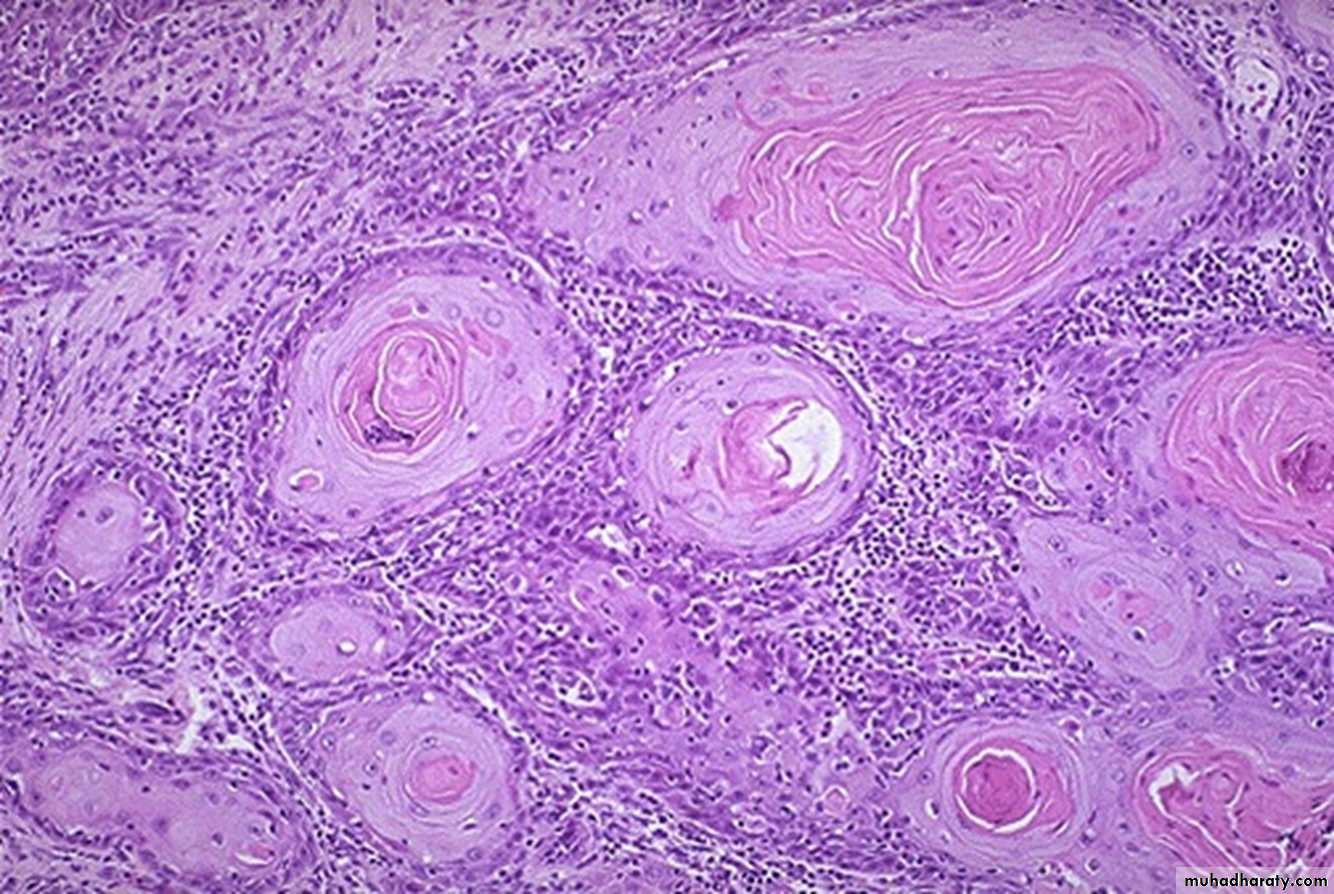
*Malignant tumors of epithelial cell origin, are called carcinomas.-Squamous cell carcinoma; malignant tumor arise from squamous epithelia.
-Adenocarcinoma; malignant tumor arise from glandular epithelia. e.g. adenocarcinoma of colon .-Specify organ of origin e.g.
Renal cell carcinomaBreast carcinoma
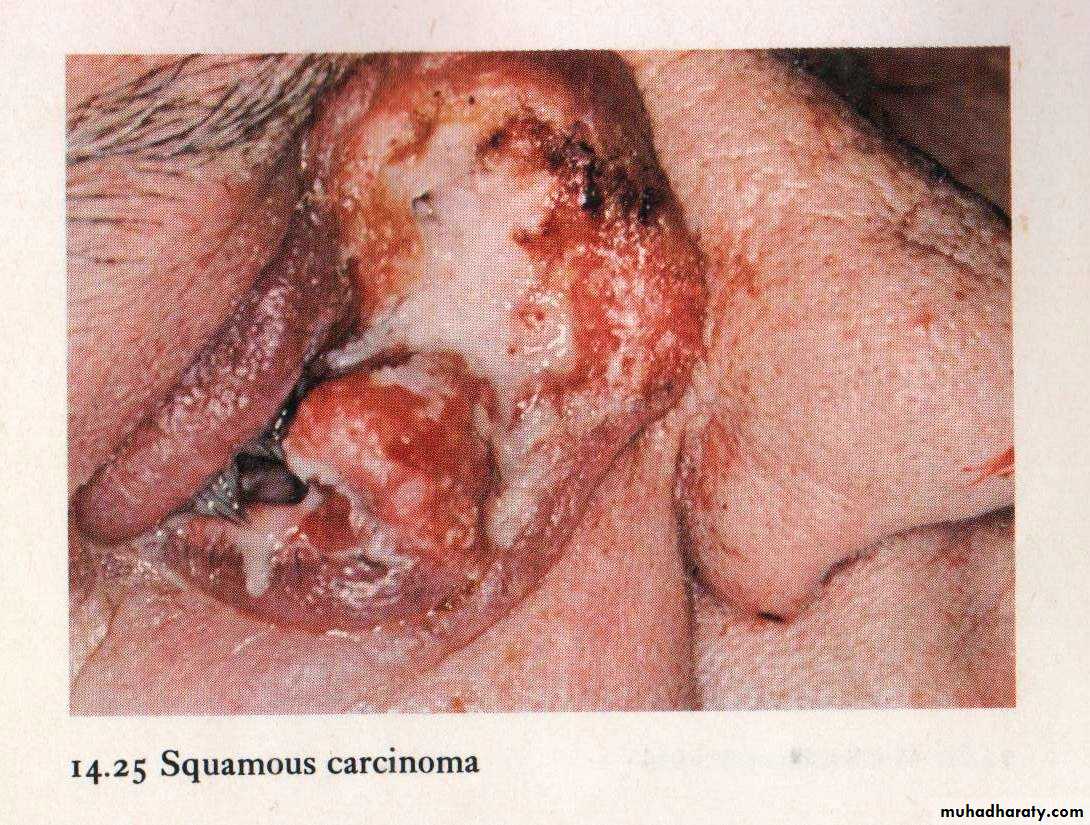
Squamous cell carcinoma
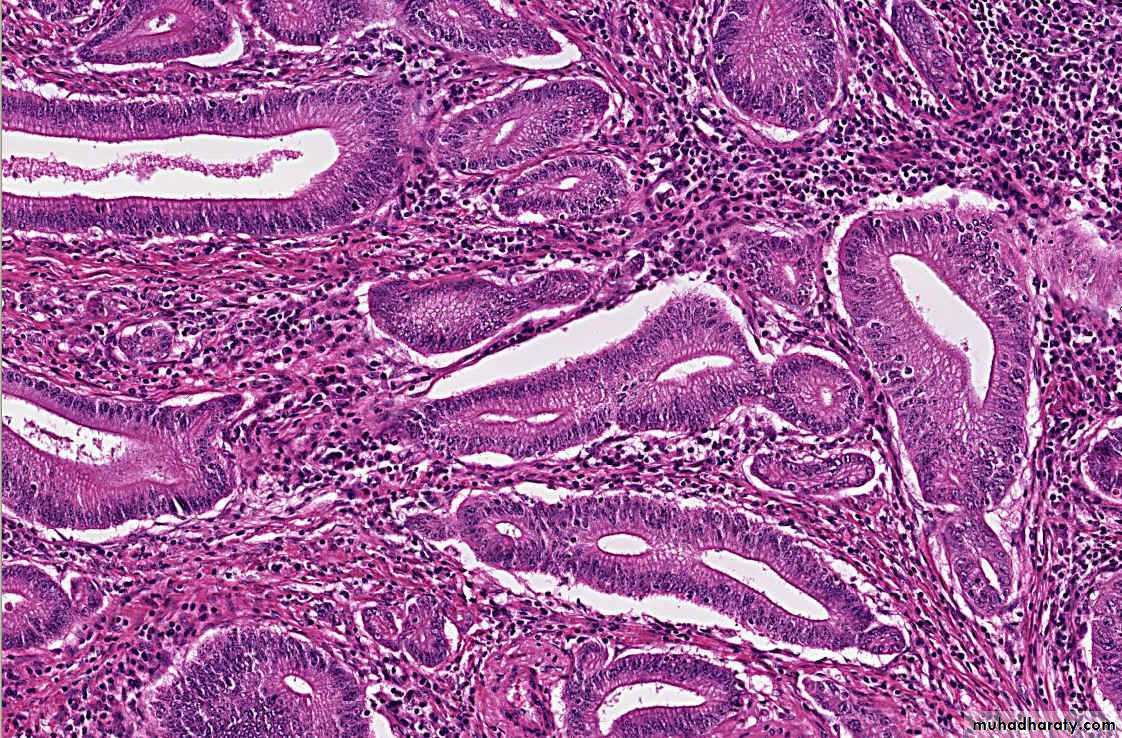
Adenocarcinoma of colon (well differentiated)
Tumors of Haemopoietic and Lymphoid Tissues-Tumors that arise from stem cells of white blood cells in the bone marrow leukemia
-Malignant solid tumors of lymphocytic origin, most of which arise in lymph nodes, spleen, thymus or bone marrow Lymphoma
Mixed tumors (Tumors with mixed differentiation):
• A single line of neoplastic cells show divergent differentiations into other tissues, e.g.:• Mixed tumor of salivary glands (pleomorphic adenoma), in reality adenomas, these tumors contain epithelial/myoepithelial components scattered within a myxoid stroma that may contain islands of cartilage or bone.
• Fibroadenoma of breast.
Mixed tumor of salivary glands (pleomorphic adenoma)
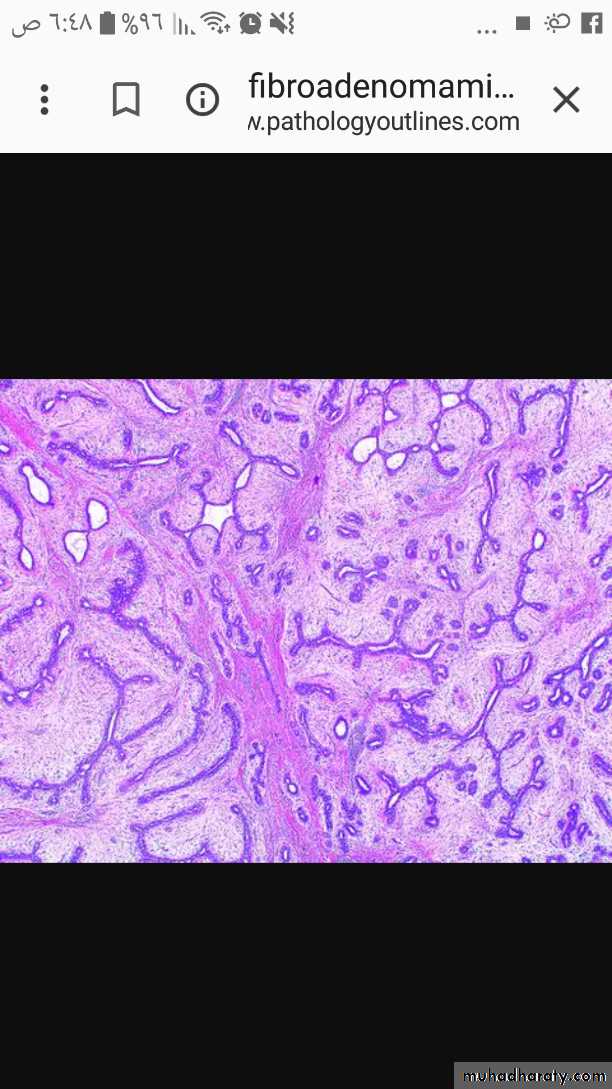
Fibroadenoma breast (mixed tumor)
Embryonal tumours: the ‘blastomas’• Some types of tumor occur almost exclusively in the very young, and bear a histological resemblance to the embryonic form of the organ in which they arise.
• Examples include:
• • Retinoblastoma, which arises in the eye
• • Nephroblastoma or Wilms’ tumor, which arises in the kidney
• • Neuroblastoma, which arises in the adrenal medulla or nerve ganglia
• • Hepatoblastoma, which arises in the liver.
Teratoma (germ cell tumor):
Tumor consists of mature and/ or immature cells belonging to one or more of the 3 germ cell layers (ecto-, endo- & mesoderm).
It originates from totipotential germ cells that are normally present in the gonades (ovary and testis).
Totipotent cells differentiate along various germ lines and producing different tissues, so this neoplasms may contain skin (ectoderm), bone, muscle, fat, brain tissue (mesoderm), gut epithelium (endoderm).
A common example, cystic teratoma (dermoid cyst) seen in ovary.
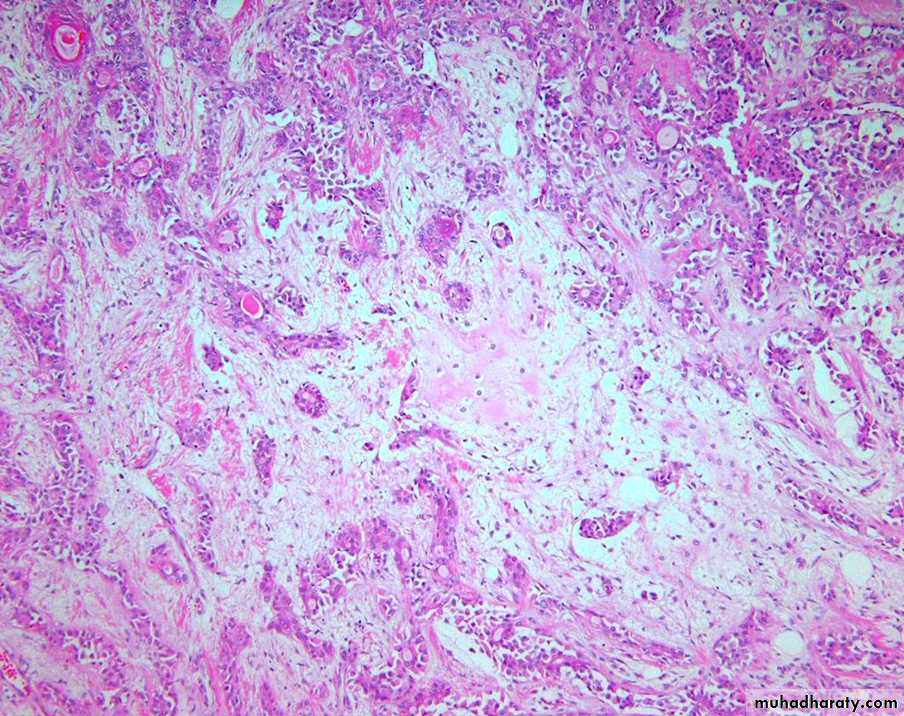
Mature teratoma of the ovary, cystic tumor lined by skin with hair, sebaceous glands, and tooth structures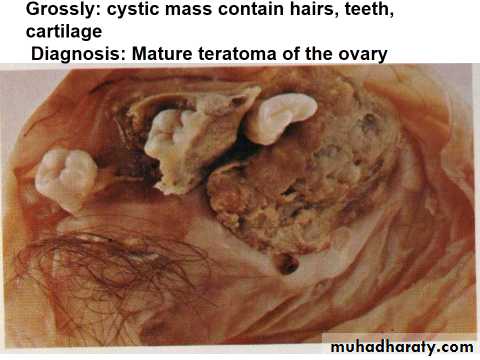
Microscopically a mature teratoma of the ovary contain cartilage, adipose tissue, and intestinal glands at the right, while at the left is a lot of thyroid tissue.

Misnomers/Inappropriate designations
Hepatoma: malignant liver tumor (correctly hepatocellular carcinoma)Melanoma: carcinoma of the melanocyte
Seminoma: testicular germ cell carcinoma
Mesothelioma: aggressive tumor of the mesothelium.
These terms are not neoplasms
• ‘granuloma’ (an aggregate of macrophages)
• ‘tuberculoma’ (the large fibrocaseating lesion of tuberculosis)• ‘atheroma’ (lipid-rich intimal deposits in arteries)
• ‘mycetoma’ (a fungal mass populating a lung cavity)
• ‘haematoma’ (mass of coagulated blood)
‘
Two entities ending with –oma but not true neoplasms: anomalous development
1. Choristoma (ectopia; heterotopia) :- presence of a normal tissue in an unexpected location e.g. pancreatic tissue in wall of esophagus/stomach or small intestine, may form masse mimicking neoplasm grossly.2. Hamartoma: mass of disorganized mature tissue related to site of origin
e.g. lung hamartoma: islands of cartilage/blood vessels/bronchial mucosa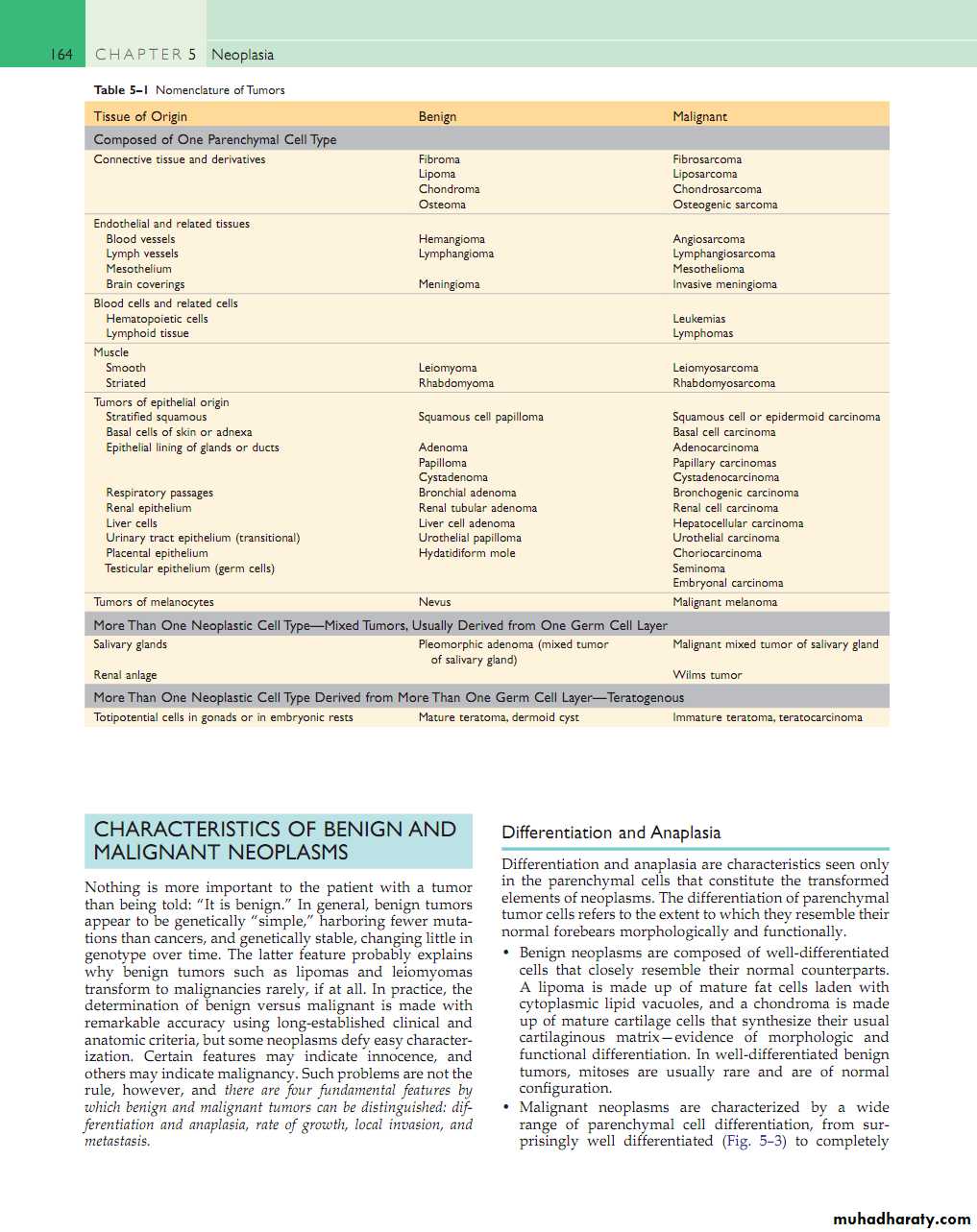
Nomenclature of Tumors
Feature
BenignMalignant
Growth rate
Slow
Relatively rapid
Mitoses
Infrequent
Frequent & often atypical
Histological resemblance to normal tissue
Good
Variable, from well differentiated to completely undifferentiated (anaplastic).
Nuclear morphology
Near normal
Usually enlarged, hyperchromatic , irregular outlines, multiple nucleoli & pleomorphic ( variable sizes & shapes
Invasion
No
Yes
Metastasis
Never
Frequent
Border
Often circumscribed or encapsulated
Often poorly defined or irregular
Necrosis
rare
Common
ulceration
Rare
Common on skin or mucosal surface.
Direction of growth on skin or mucosal surface
Often exophytic
Often endophytic
Fibroadenoma of breast (mixed tumor)
Well-defined fibrotic capsule surrounding the tumor. The latter consists of compressed ducts set within fibroblastic stroma.
Carcinoma of the breast
Invasive breast cancer is seen as an irregular whitish yellow area with nipple retraction.
Certain terms
• Dysplasia• Carcinoma in situ
• Anaplasia
• Metastasis
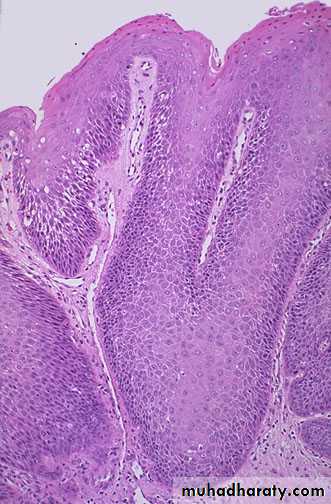
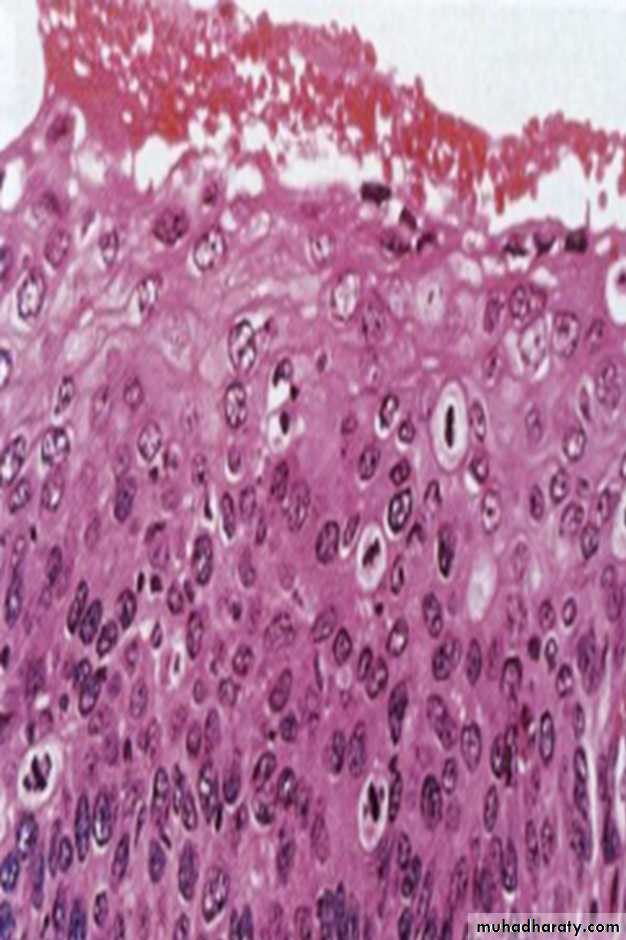
Dysplasia
Disordered growth in epithelial membranes (e.g. the squamous epithelium of the cervix, skin, and bronchial mucosa) characterized by1. Pleomorphism
2. Loss of polarity
3. Nuclear Changes
a. hyperchromasia
b. ↑N/C
c. ↑Mitotic figures
Some dysplastic lesions are almost certainly reversible
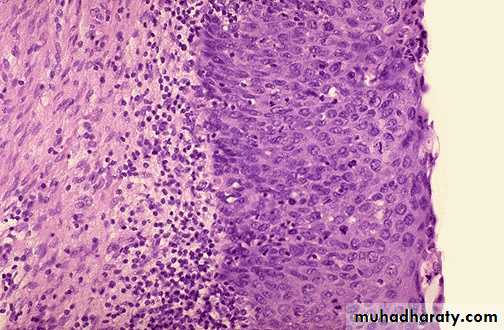
Carcinoma in situ
When dysplastic changes involve the full thickness of the epithelium, but does not penetrate the basement membrane, it is called carcinoma in situ (CIN).• Only in epithelia. Not in mesenchymal tissues
• Complete excision at this very early stage will guarantee a cure.
• Once the tumor cells breach the basement membrane, the tumor is said to be invasive
• The phase of in situ growth may last for several years before invasion commences.
• The term ‘intraepithelial neoplasia’, as in cervical intraepithelial neoplasia (CIN), is used increasingly to encompass both carcinoma in situ and dysplasia
Cervix: part of stratified squamous epithelium shows disorderly arranged cells, hyperchromatic nuclei with mitosis . The basement membrane is intact, and there is no tumor cells in the subepithelial stromaDiagnosis: Carcinoma In Situ
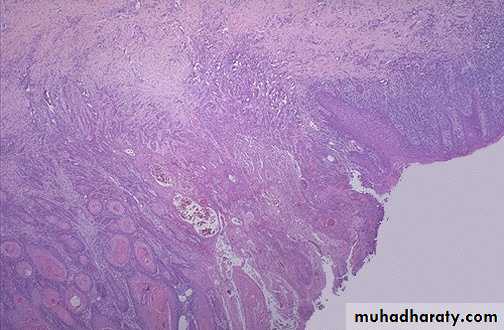
Squamous cell carcinoma following in situ carcinoma
Anaplasia
Total lack of differentiation of malignant cells, (i.e the tumor consist of primitive-appearing/ unspecialized cells/can not be assigned to any of normal cells).
The features of anaplasia or malignancy
1- Pleomorphism : variation in size and shape
2- Abnormal nuclear morphology:
a. Hyperchromasia (more darkly stained than normal)
b.↑Nuclear/Cytoplasmic ratio: N/C ratio may approach 1:1 (normal 1:4 or 1:6).
c. Variations in shape/abnormal chromatin clumping & distribution.
d. Large nucleoli
3- Mitoses :↑/atypical.
4-Loss of polarity: disturbed orientation of cells.
5-others: Tumor giant cell
Metastases
Metastases: tumor implants discontinuous with primary tumor. It is only definite criterion of malignancy.The major exceptions (locally infiltrative and rarely metastasize) are:
1. Most malignant gliomas of CNS2. Basal cell carcinoma of the skin.
3. Some soft tissue tumors
• Metastases strongly reduces the possibility of cure
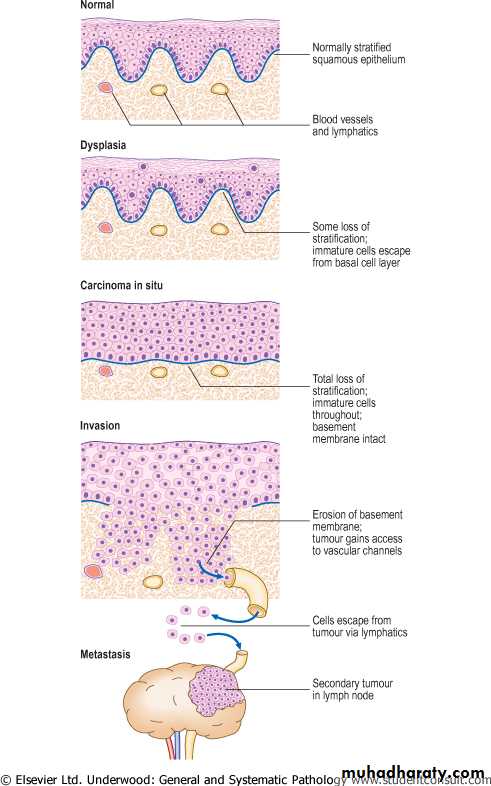
Evolution of an invasive squamous cell carcinoma from the precursor lesions of dysplasia and carcinoma in situ (usually grouped together as intraepithelial neoplasia). Note that the tumor cells cannot reach routes of metastasis such as blood vessels and lymphatics until the basement membrane has been breached