Secret Lectures
(5)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
1
The Pleura
Pleural effusion
Types
1. Transudate
2. Exudate ( Empyema ,hemothorax,chylothorax)
Chest radiograph appearances of fluid in the pleural cavity are the same regardless the
type.
US
is the simplest method of determining whether pleural fluid is present.
Radiographic appearances :
1.Free fluid
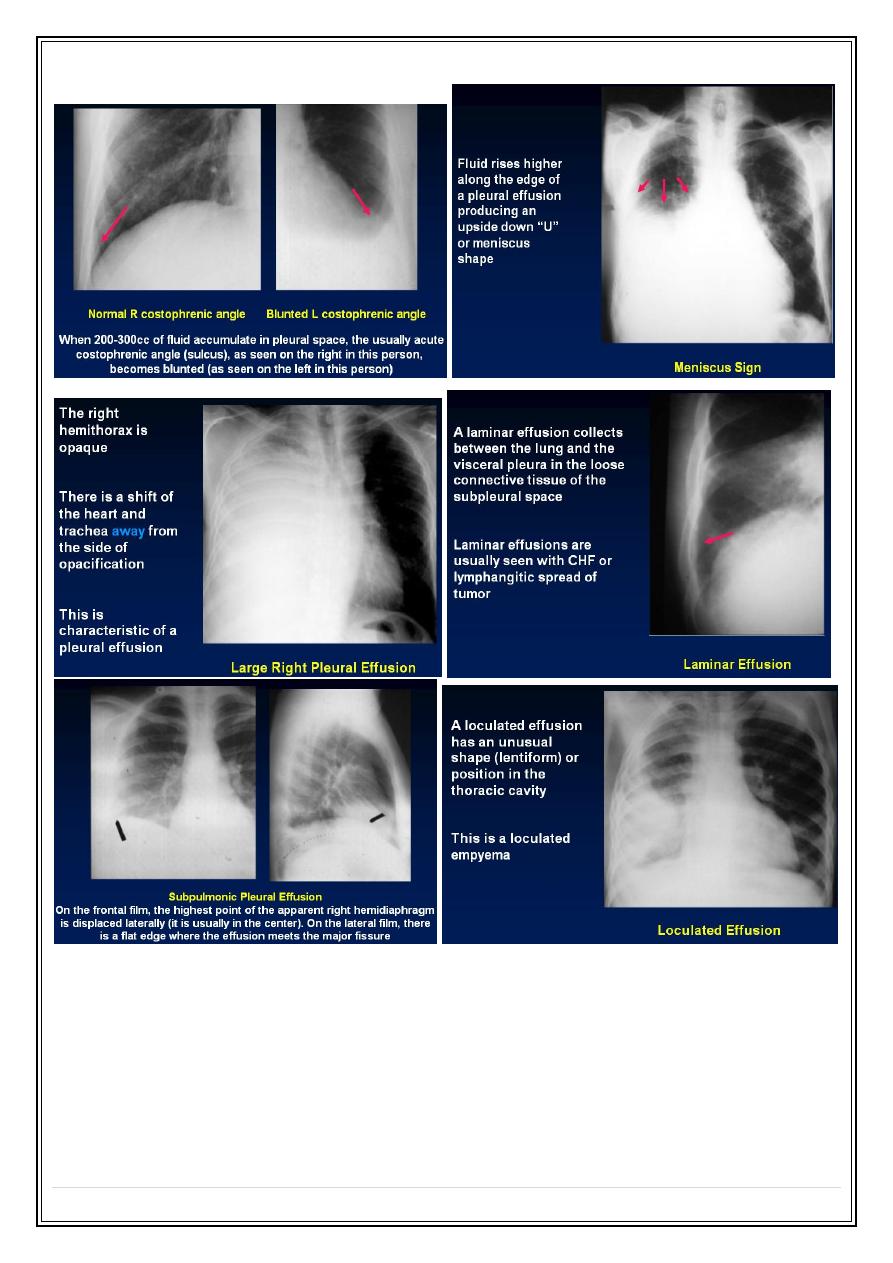
The most dependent recess of the pleura is the posterior recess ( posterior
costophrenic angle). A small pleural effusion will therefore collect posteriorly & in
most patients 100-200 ml of fluid are required to fill this recess before it appear in
frontal radiograph.
So fluid is seen earlier with lateral view. But its possible to identify effusion of only
few milliliters using ( Decubitus view, US or CT ).
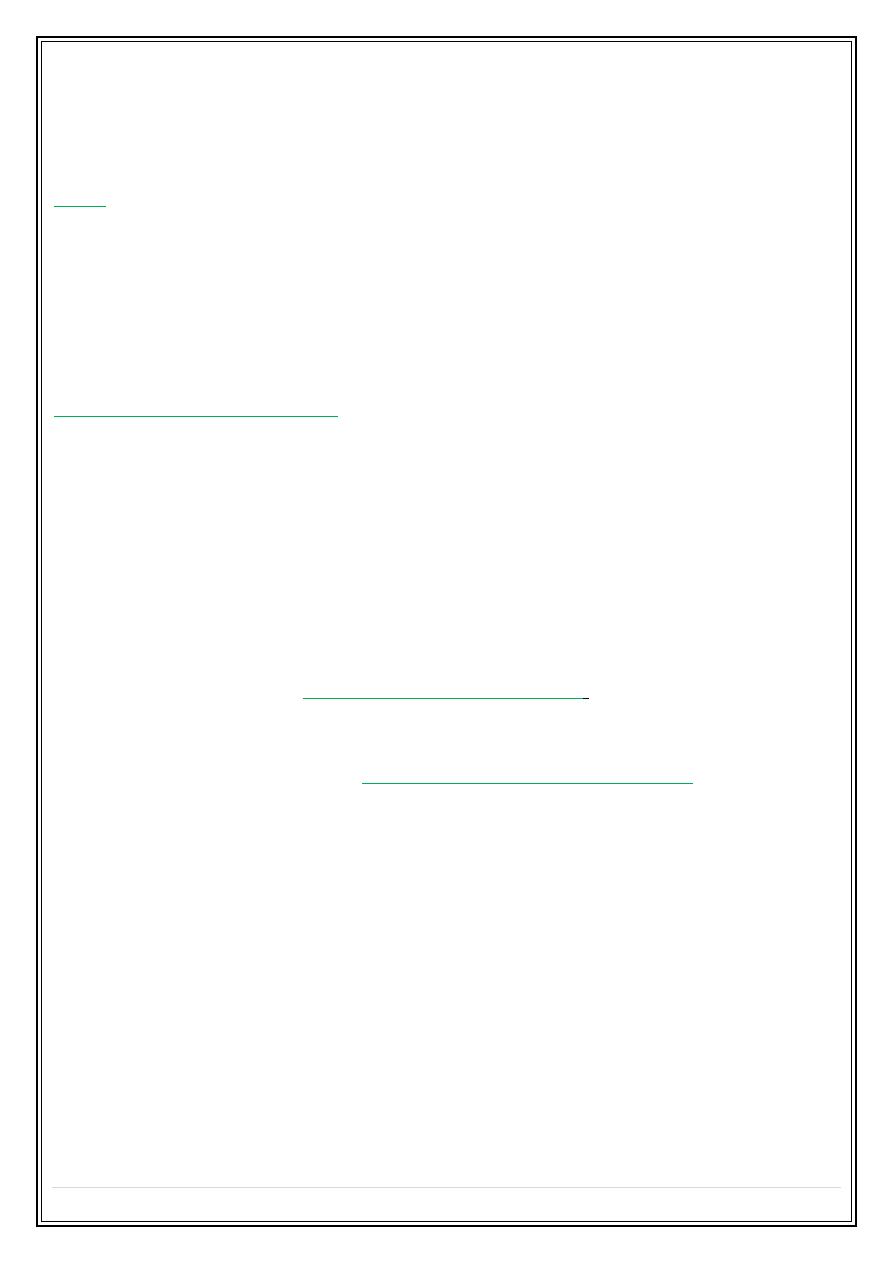
1.Typical ?
➢
homogenous opacity
blunting the costophrenic angle
---- higher laterally than
medially (meniscus sign), it also run into the fissures, particularly the lower end of
oblique fissures.
➢
massive effusion may cause
complete radiopacity of a hemithorax
, the lung will
retract toward the hilum & then the space occupying effect of the effusion will
push the mediastinum toward the opposite side.
Note :In the presence of large ( massive effusion ) lack of displacement is suggest
underlying collapse--- likely to be due to underlying ca bronchus
2.Atypical ?
1.
lamellar
( between lung surface & visceral pleura ).
2.
Sub-pulmonary effusion
---- simulating an elevated diaphragm --- Decubitus or
supine films will verify.
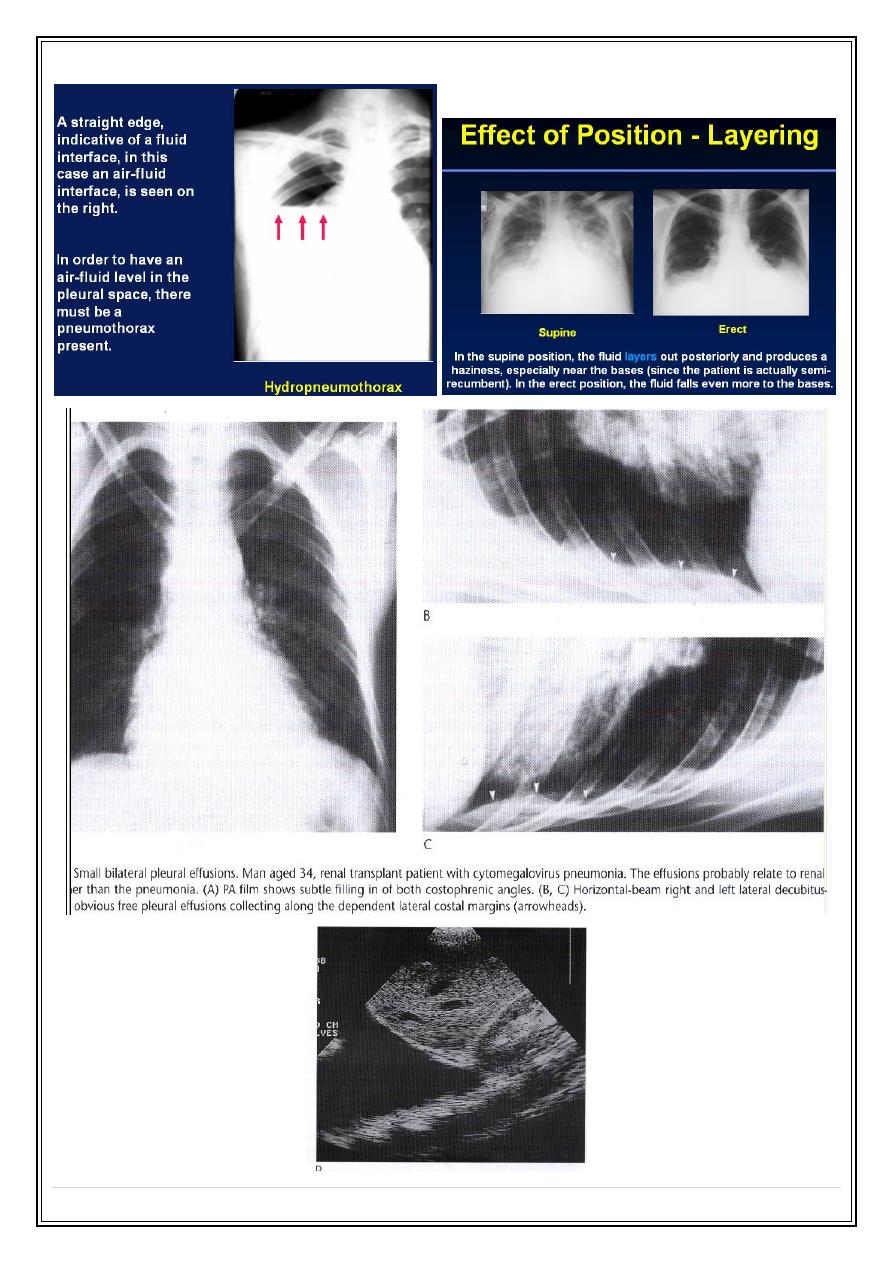
2.
Loculated
( encapsulated or encysted ) effusion loculated pleural cavity
effusion--- loculated fissural effusion.
Secret Lectures
(5)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
2
Secret Lectures
(5)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
3
Secret Lectures
(5)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
4
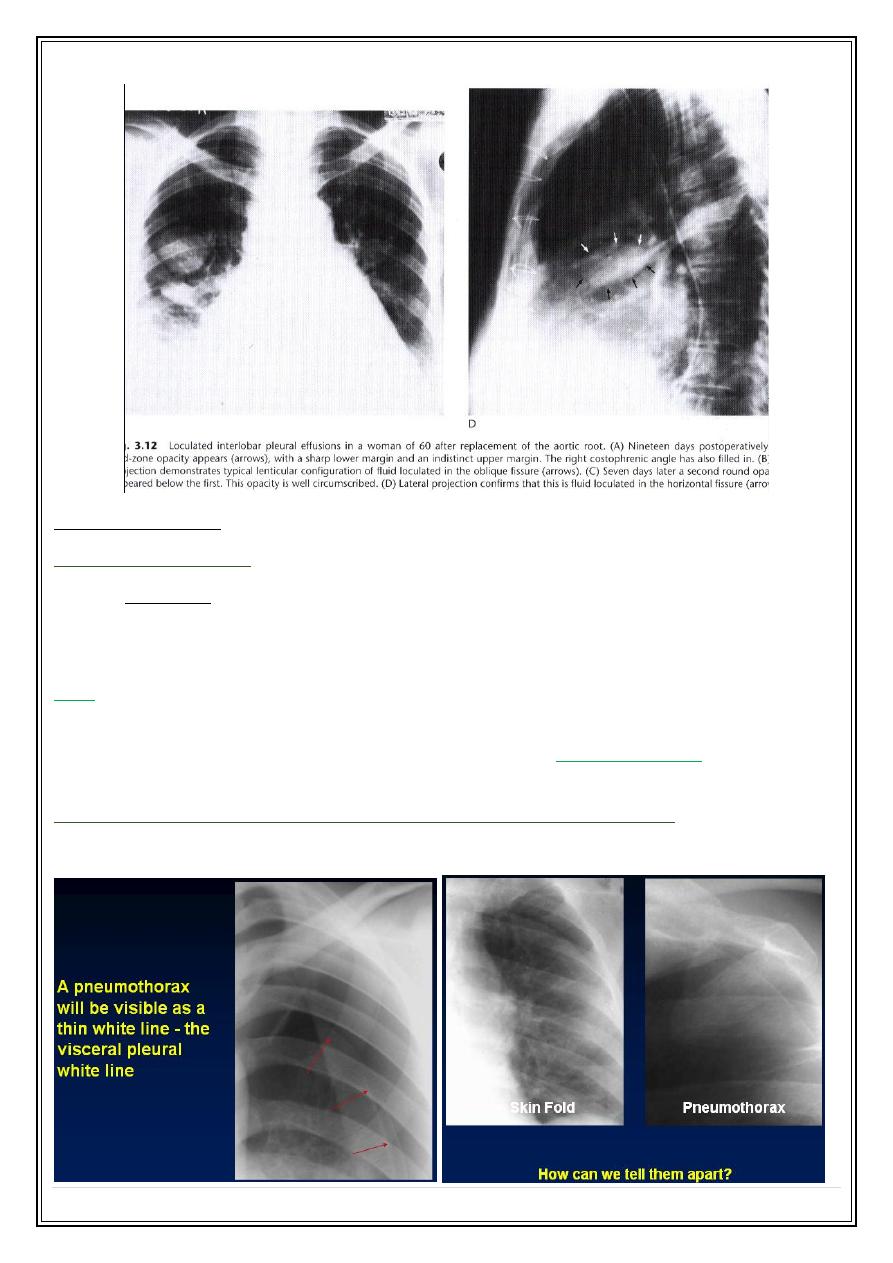
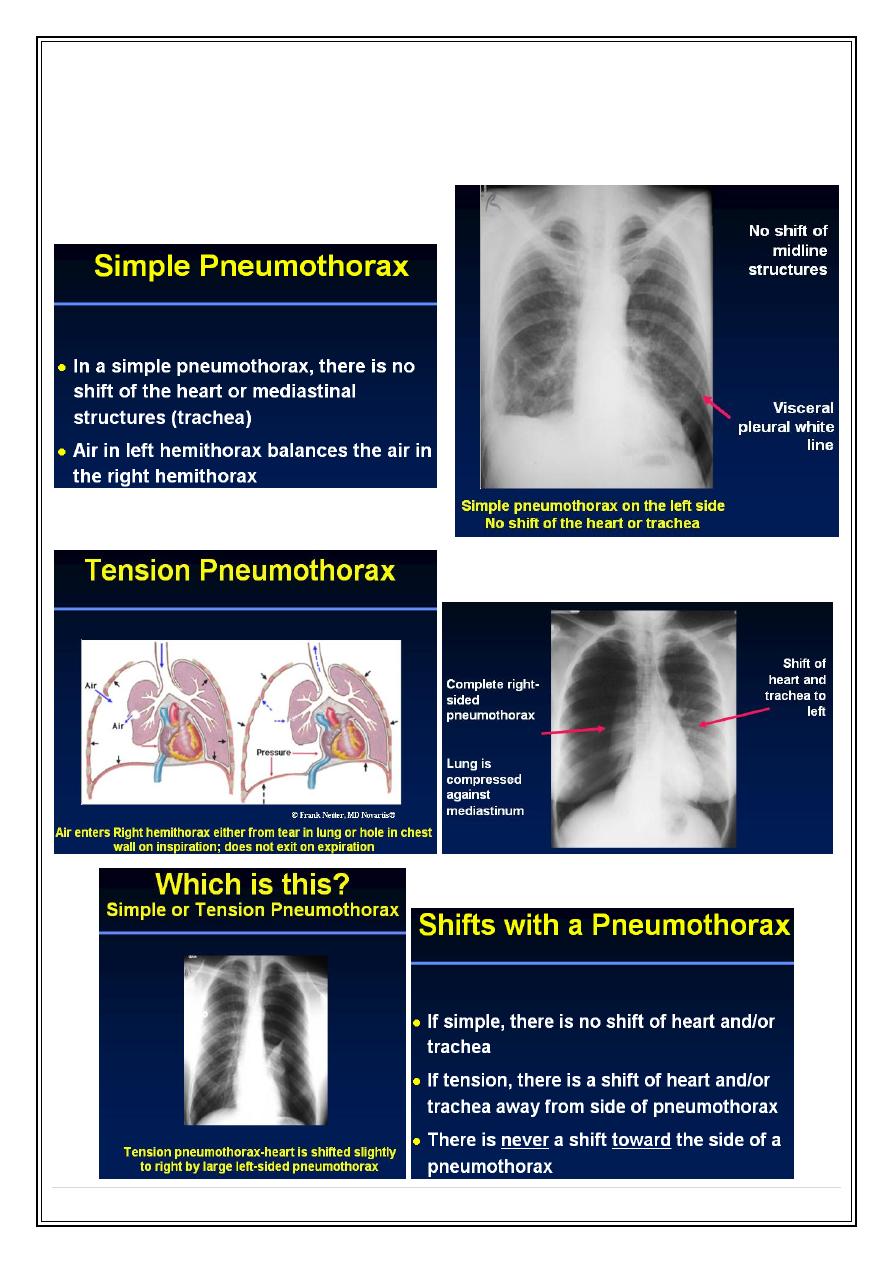
Pneumothorax
Radiological findings ?
➢
A white line of pleura forming the lung edge separated from the chest wall ,
mediastinum or diaphragm by air.
➢
absence of vessel shadow outside this line.
Note
Once the presence of a pneumothorax has been noted, the next step is to decide
whether or not it is under tension. This is easy if there is mediastinal shift & flattening or
inversion of the hemidiaphragm.
Hydropneumothorax, haemopneumothorax, pyopneumothorax
➢
The diagnostic feature is the air fluid level.
Secret Lectures
(5)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
5
Types of pneumothoraces: Two major types of pneumothorax:
•
Simple
•
Tension
Secret Lectures
(5)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
6
Pleural tumours
The commonest cause are metastatic carcinomas.
Primary pleural tumors such as mesothiliomas are relatively uncommon.---many
have history of asbestos exposure.
Lobulated mass based on pleura.
Frequent associated with
pleural effusion
which may obscure the tumour itself.
Sometimes the predominant feature is pleural effusion with no visible mass.
Pleural calcification
✓
Irregular sheet of dense plaque with or with out pleural thickening.
✓
When unilateral they are likely to be due to either an old empyema, usually
tuberculosis or an old haemothorax.
✓
Bilateral calcification is often related to asbestos exposure.
✓
Some time no cause can be identified.
The mediastinum
The modality of choice are CT & MRI
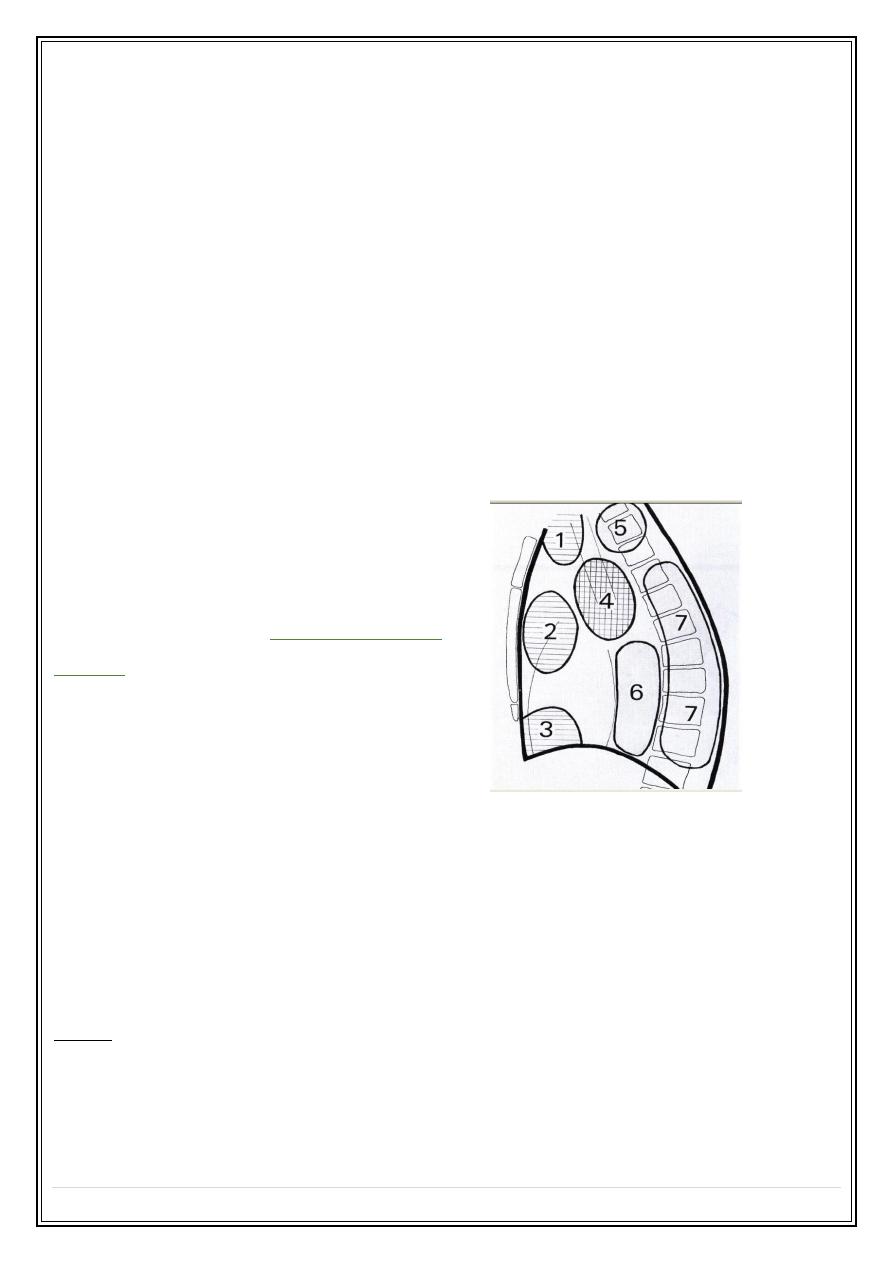
Mediastinal masses
Anterior
1. Retrosternal goiter & thyroid tumours.
2. Lymph node enlargement
Thymic tumour or cyst
Teratoma / dermoid cyst
Aneurysm of ascending aorta.
3. Pleuro-pericardial cyst
Fat bad
Diaphragmatic hump
Morgagni hernia.
Middle
4. Lymphadenopathy.
Bronchogenic cyst.
Aneurysm of aortic arch
Secret Lectures
(5)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
7
Posterior
5. Neurogenic tumour
Pharyngio -esophageal pouch.
6. hiatus hernia
Aneurysm of descending aorta.
7. Neurogenic tumour
Paravertebral mass
Bockdalecks hernia.
Plain chest films in mediastinal masses:
❖
Intrathoracic thyroid masses ( goiters)
are the most frequent cause of superior
mediastinal mass.
The characteristic feature is that the mass extends from the superior mediastinum
into the neck and almost invariably compresses or displace the trachea.
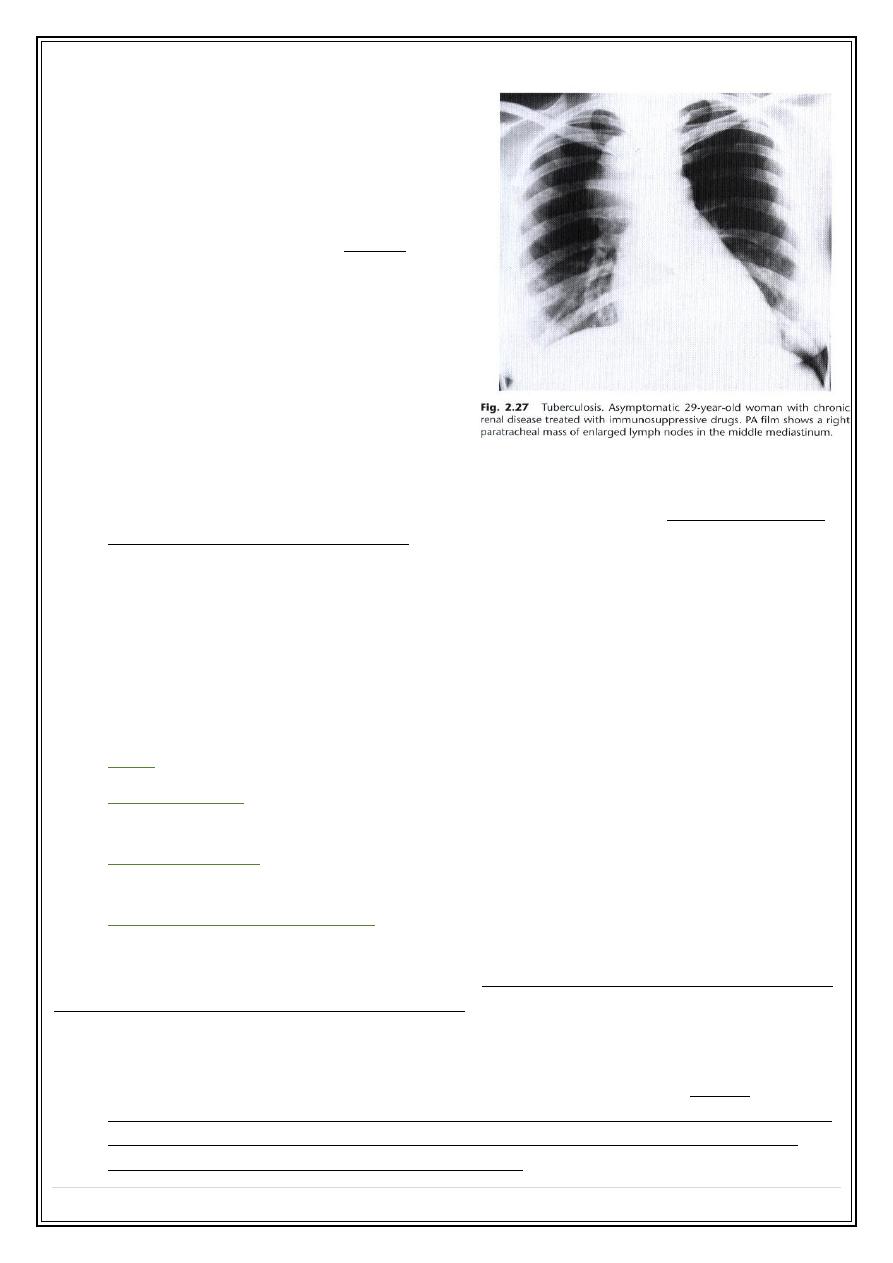
❖
Lymphadenopathy
is the next most frequent cause of a mediastinal swelling.
Lymphadenopathy may occur in any of the three compartment & its often possible
to diagnose enlarged lymph nodes from their lobulated outlines & the multiple
locations involved .
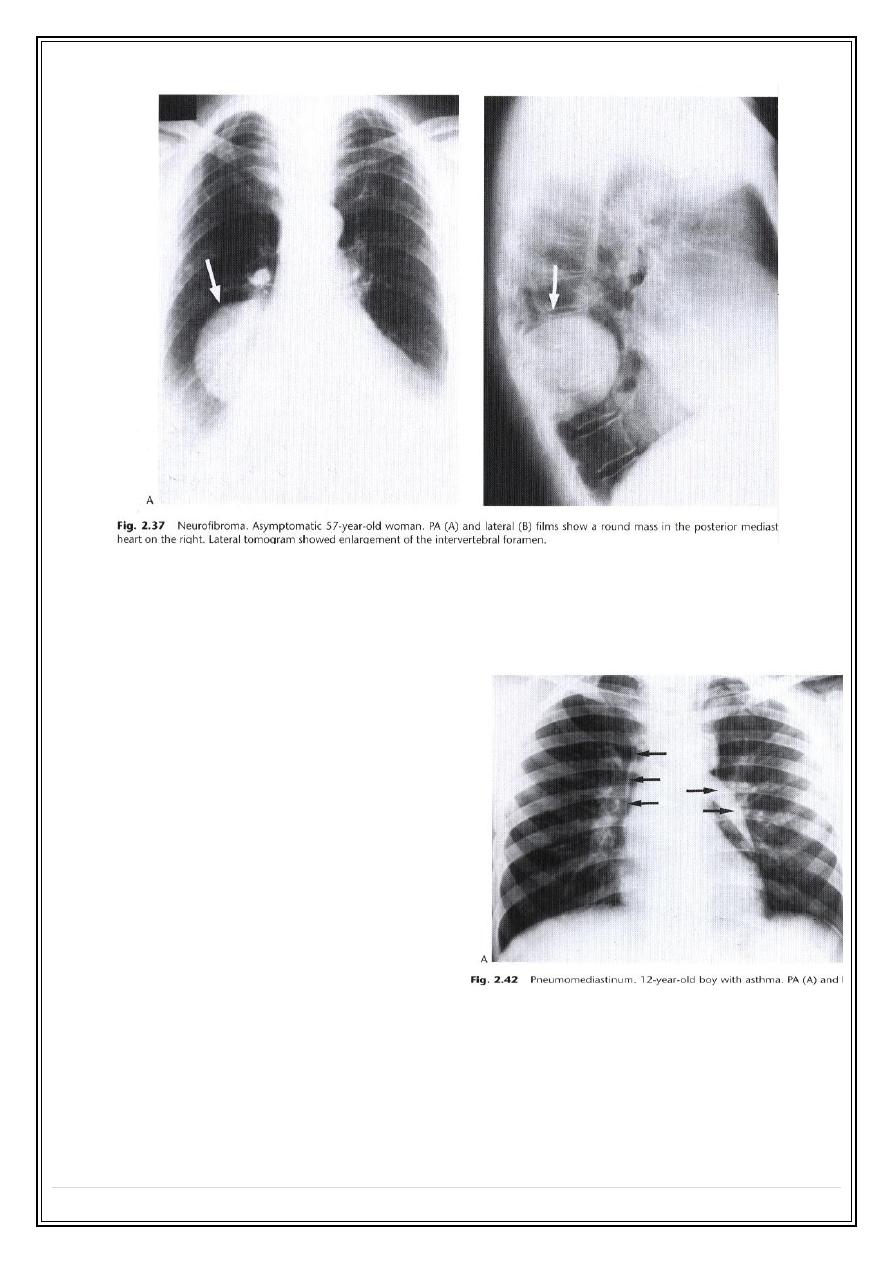
❖
Neurogenic tumours
are by far the commonest cause of posterior mediastinal
masses. Pressure deformity of the adjacent ribs & thoracic spine is often visible
❖
Certain tumours such as
dermoid cysts& thymomas
, are, for practical purposes,
confined to the anterior mediastinum.
❖
Calcifications occurs in many conditions
but almost never in malignant
lymphadenopathy.
❖
Mediastinal mass due to
hiatus hernia
usually easy to diagnose on plain films
because it often contain air and may
have a fluid level, best seen on lateral
view .
❖
Masses in the RT cardiophrenic angle
anteriorly
are virtually never of clinical
significance. They are nearly all either
large fat bad, diaphragmatic hump,
benign pericardial cysts or hernia
through the foramen of Morgagni
.
Secret Lectures
(5)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
8
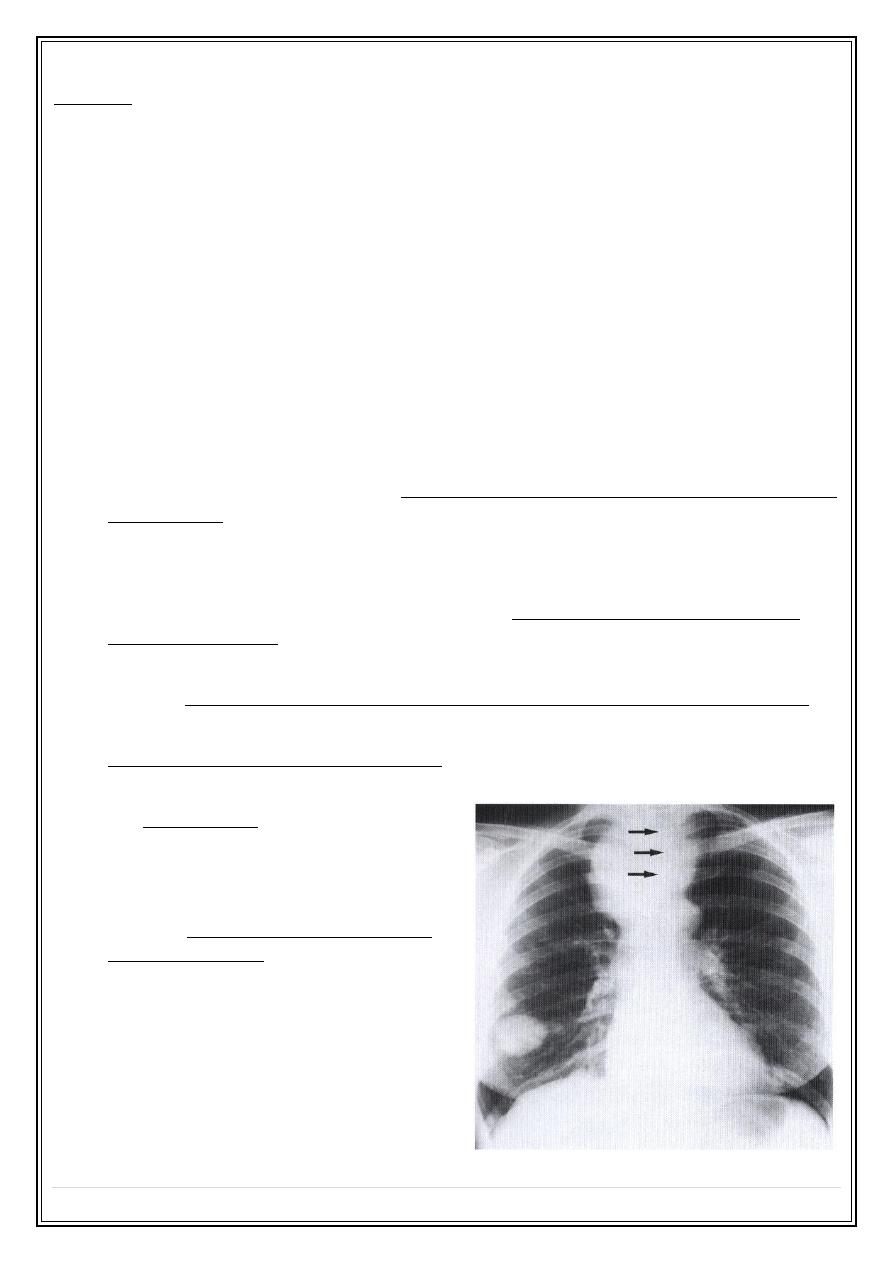
Pneumomediastinum
Common causes:
o
Air tracked from the neck, adjacent chest wall ( trauma ).
o
Air track from retroperitoneum .
o
Tear in the esophagus e.g. trauma,
endoscopy or following F.B
o
Spontaneous Leak from the bronchi in
the mediastinum or the lung e.g.
asthma
Plain film findings :
Fine streaks of transradiancy within the
mediastinum often extending up into the
neck.
Hilar enlargement :
causes of hilar enlargement:
1. Large blood vessel ( artery or vein ).
2. Hilar mass A-- Lymph node enlargement
B -- carcinoma of bronchus
Secret Lectures
(5)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
9
➢
Its usually possible to decide from plain
films when hilar enlargement is due to
enlargement of
pulmonary arteries
because:-
1.Both hila shows a branching pattern
2.Vascular enlargement is usually
bilateral and accompanied by
enlargement of the heart and main
pulmonary artery.
➢
Primary carcinoma of bronchus
frequently present as hilar mass (
central form ). If lobar
collapse/consolidation or narrowing of
the adjacent bronchus is visible, the
diagnosis of carcinoma is virtually certain .
➢
its often possible to diagnose
enlarged lymph nodes
from their lobulated outlines
& the multiple locations involved .
The Diaphragm
Bilateral elevation
Unilateral elevation.
- Unilateral loss of volume of ipsilateral lung.
- Abdominal pathology such as subphrenic abscess
✓
Note subpulmonary effusion may mimic elevation of one or both hemidiaphragm.
✓
Minor elevation
of a hemidiaphragm is a relatively common incidental finding of
no significant.
✓
Marked elevation
of one hemidiaphragm with no other possible abnormality
suggest either paralyses or eventration
✓
Paralyses of a hemidiaphragm
results from disorder of phrenic nerve e.g. invasion
by ca bronchus
The signs are elevation of one diaphragm which on fluoroscopy or US shows paradoxical
movement i.e. it moves upward on inspiration.
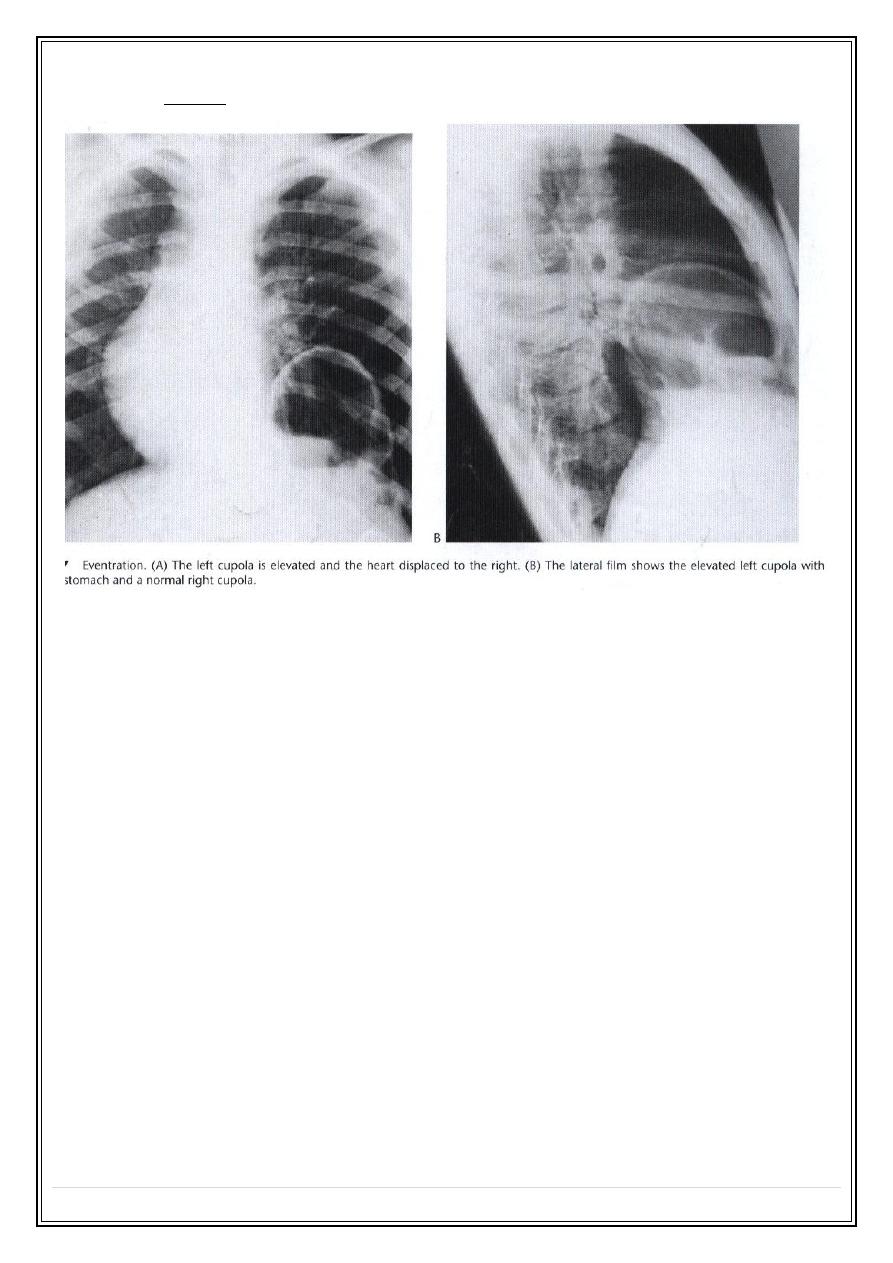
✓
Eventration of diaphragm
is a congenital condition in which the diaphragm lacks
muscle & becomes a thin membranous sheet. Except in neonatal period it is
almost always an incidental finding & does not cause symptoms . almost
invariably Lt sided. characteristically associated with marked shift of mediastinum
to the right side, a feature rarely seen with paralysis of diaphragm. Movement
reduced, paradoxical or absent on fluoroscopy.
Secret Lectures
(5)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
10
✓
When partial of part of hemidiaphragm it called
diaphragmatic hump
Thank You,,,