Proximal Femoral Fractures in Children
Dr. Jamal Al-Saidy
M.B.Ch.B. .F.I.C.M.S
Hip fractures rarely occur in children but when they do they are potentially very
serious.
The fracture is usually due to high velocity trauma; for example, falling from a
height or a car accident.
Pathological fractures sometimes occur through a bone cyst or benign tumour.
In children under two years, the possibility of child abuse should be considered.
There is a high risk of complications, such as:
avascular necrosis
premature physeal closure
coxa vara.
Classification
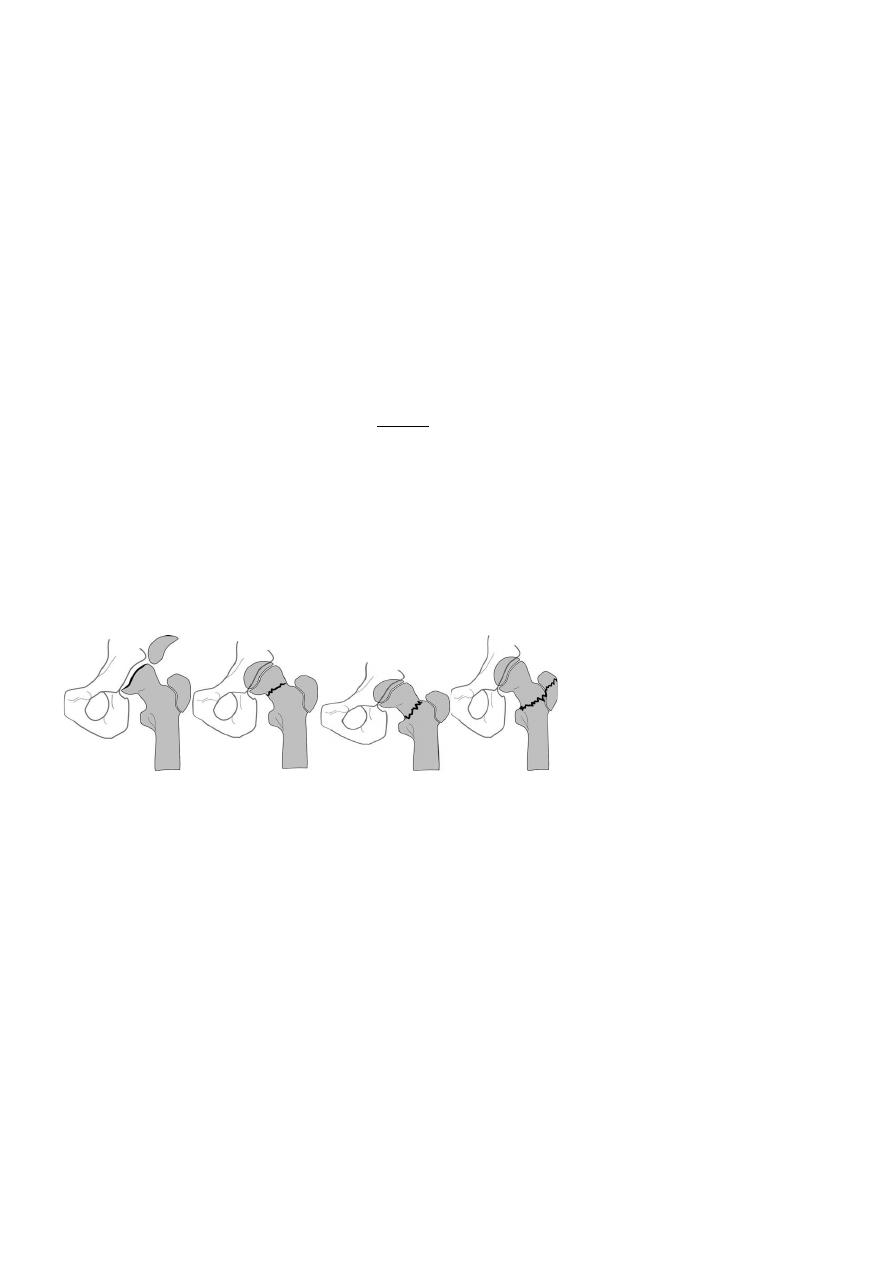
The most useful classification is that of Delbet, which is based on the level of the
fracture (Hughes and Beaty 1994) :-
.
o Type I is a fracture-separation of the epiphysis; sometimes the epiphyseal
fragment is dislocated from the acetabulum.
o Type II is a transcervical fracture of the femoral neck; this is the commonest
variety, accounting for almost half of the injuries.
o Type III is a basal (cervico-trochanteric) fracture, the second most common
injury.
o Type IV is an intertrochanteric fracture.
Type I Type II Type III Type IV
Clinical features
Diagnosis can be difficult, especially in infants where the epiphysis is not easily
defined on x-ray.
Type I fractures are easily mistaken for hip dislocation.
Ultrasonography, MRI and arthrography may help.
In older children the diagnosis is usually obvious on plain x-ray examination.
Treatment
These fractures should be treated as a matter of urgency, and certainly within
24 hours of injury.
Initially the hip is supported or splinted while investigations are carried out.
Early aspiration of the intracapsular haematoma is advocated as a means of
reducing the risk of epiphyseal ischaemia.
Undisplaced fractures may be treated by immobilization in a plaster spica for 6–
8 weeks, but there is a risk of late displacement and Malunion or non-union.

Displaced type IV fractures also can be treated nonoperatively: - closed
reduction, traction and spica immobilization. Careful follow-up is essential; if
position is lost, operative fixation will be needed.
Type I, II and III fractures are treated by closed reduction and then internal
fixation with smooth pins or cannulated screws.
Complications
Avascular necrosis of the femoral head , it occurs in about 30 per cent of all
cases.
Coxa vara Femoral neck deformity may result from malunion, avascular
necrosis or premature physeal closure.
Diminished growth Physeal damage may result in retarded femoral growth. Limb
length equalization may be needed.
THANK YOU
Dr. Jamal Al-Saidy
M.B.Ch.B. .F.I.C.M.S