Secret Lectures
(6)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
1
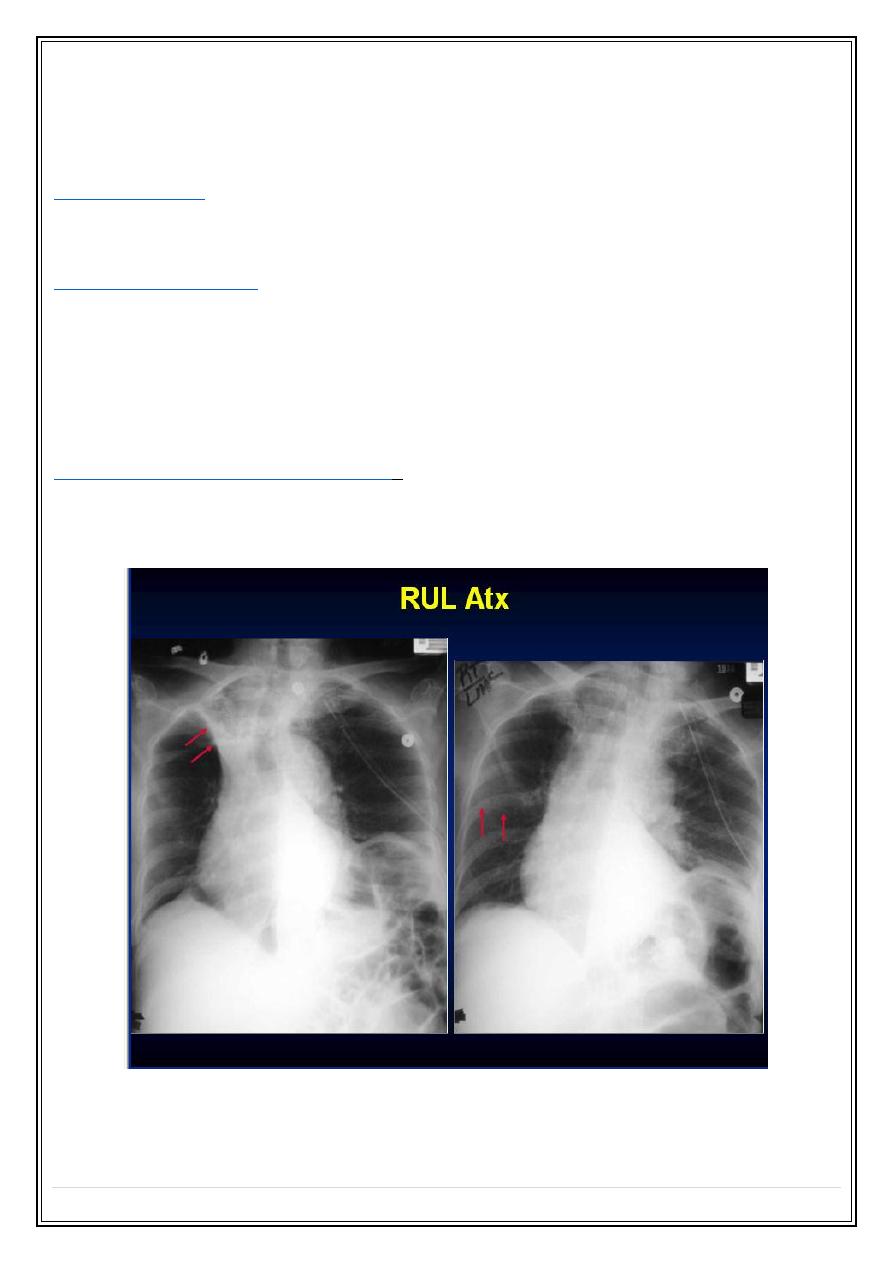
Pulmonary collapse (atelectasis)
Loss of volume of a lobe or lung
Common causes:
1.Bronchial obstruction.
2.Pneumothorax or pleural effusion.
Signs of lobar collapse:
1. Displacement of structures.
2. The shadow of collapsed lobe—consolidation almost invariably accompanies collapse.
3. The silhouette sign.
e.g. collapse of the
anteriorly located lobes (upper &middle lobes)
obliterates portions of
the mediastinal & heart outlines ,whereas collapse of the
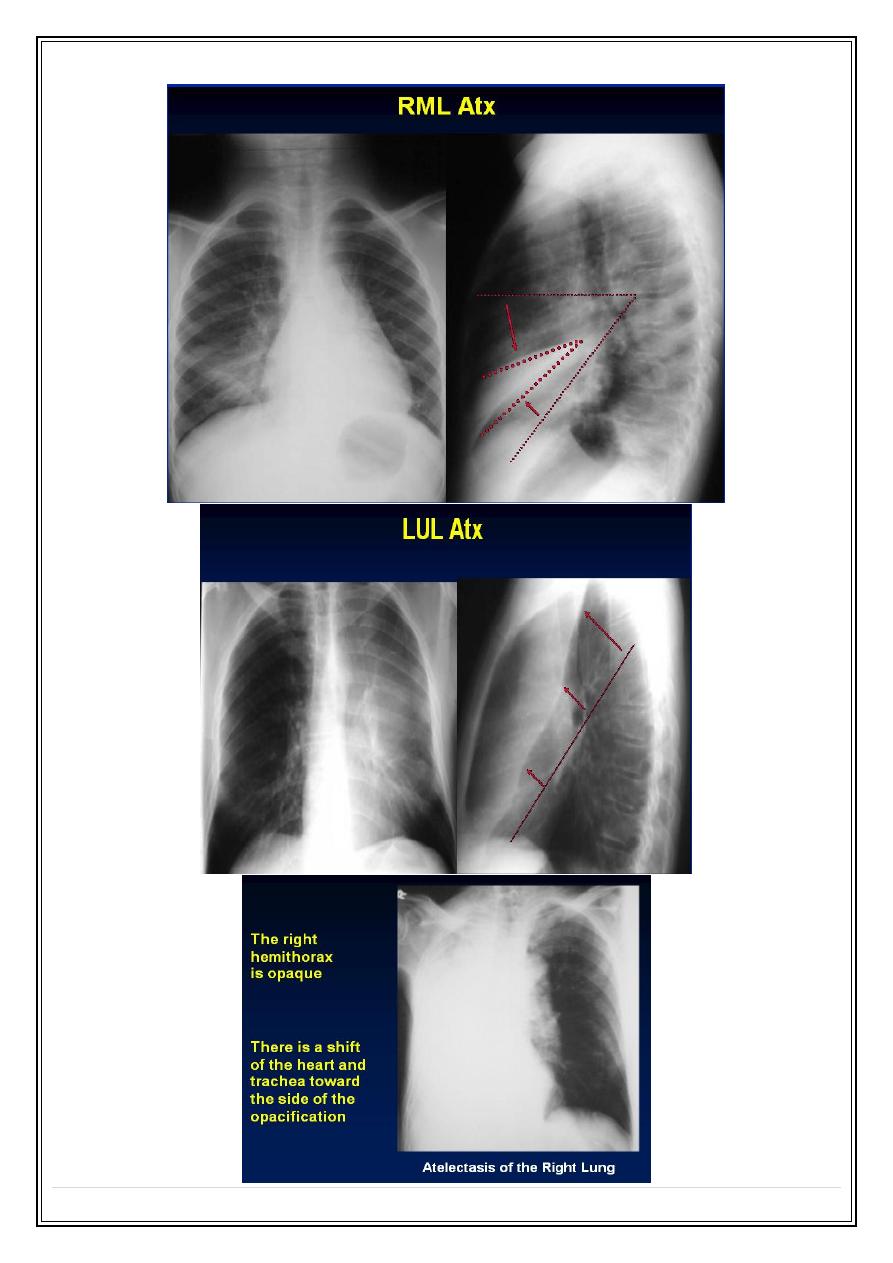
lower lobes
obscures
the outline of the adjacent diaphragm &descending aorta.
Signs of collapse of whole of one lung
:
1.The entire hemithorax is opaque.
2.Substantial mediastinal & tracheal shift.
Secret Lectures
(6)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
2
Secret Lectures
(6)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
3
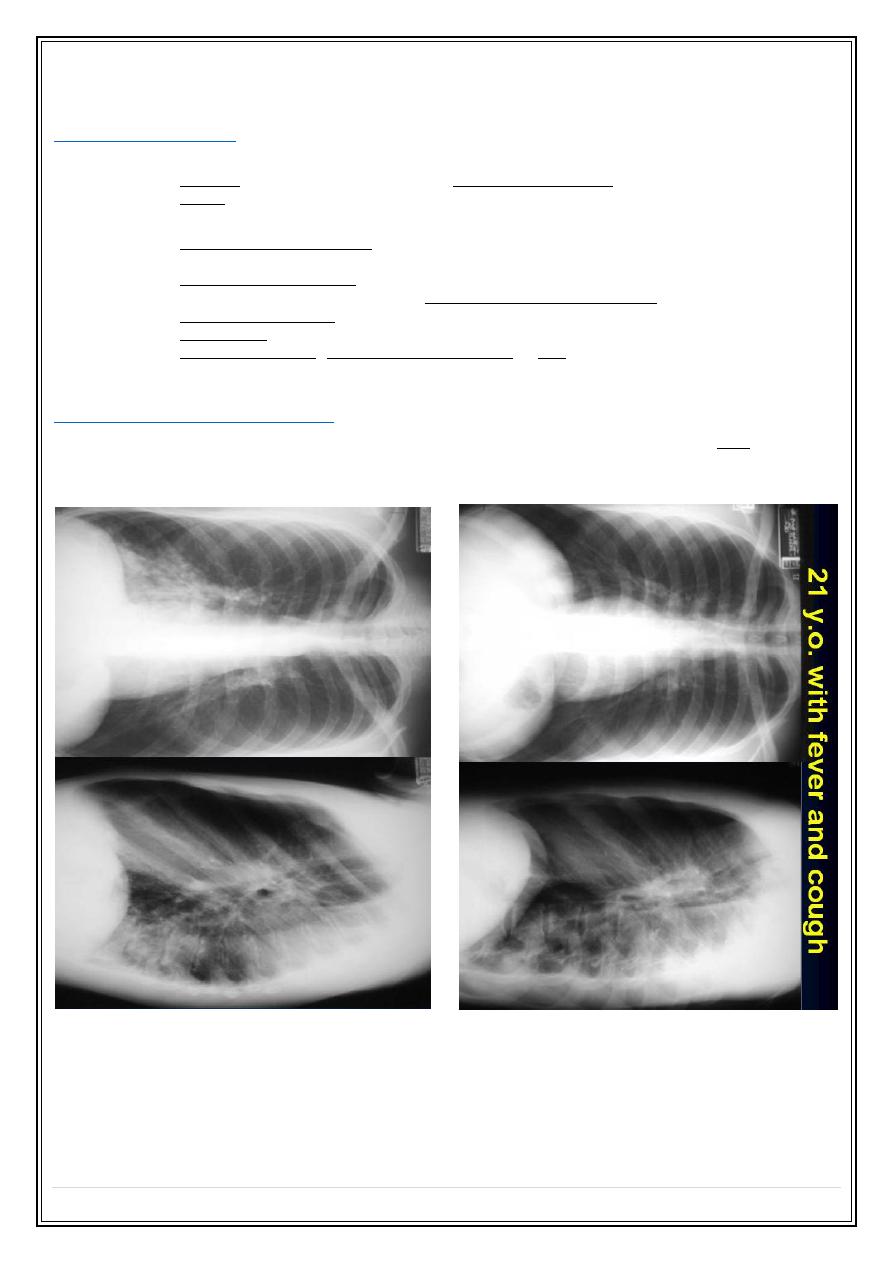
Pneumonia
Bacterial pneumonia
the basic radiological features:
1. patchy consolidation involving one or more lobes(
bronchopneumonia
).
2. lobar consolidation (
lobar pneumonia
)
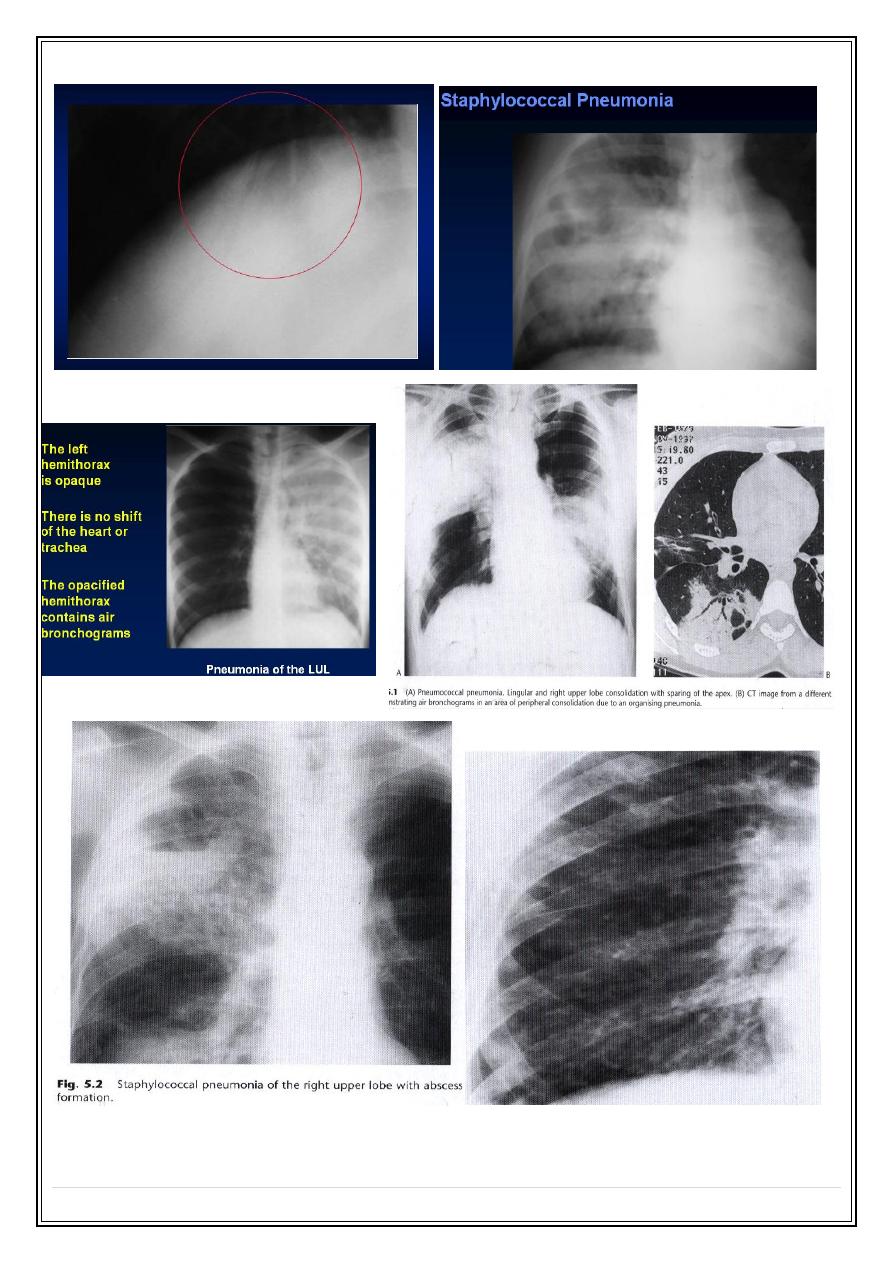
Notes :
1. staphylococcus aureus, various gram negative (klebsilla) & anaerobic
bacteria & mycoplasma pneumoniae classically cause
bronchopneumonia.
2. pneumococcal pneumonia (streptococcal pneumoniae) classically cause
lobar pneumonia.
3. cavitation in consolidated area is a particular feature of infection with
staphylococcal , gram-negative bacilli & TB.
4. consolidation may accompanied by lose of volume of affected lobe a
feature that is particularly common in children.
Viral & mycoplasma pneumonia
wide spread ill-defined consolidation & loss of clarity of vascular markings ddx
pulmonary edema.
Secret Lectures
(6)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
4
Viral pneumonia– H. influenzae
Secret Lectures
(6)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
5
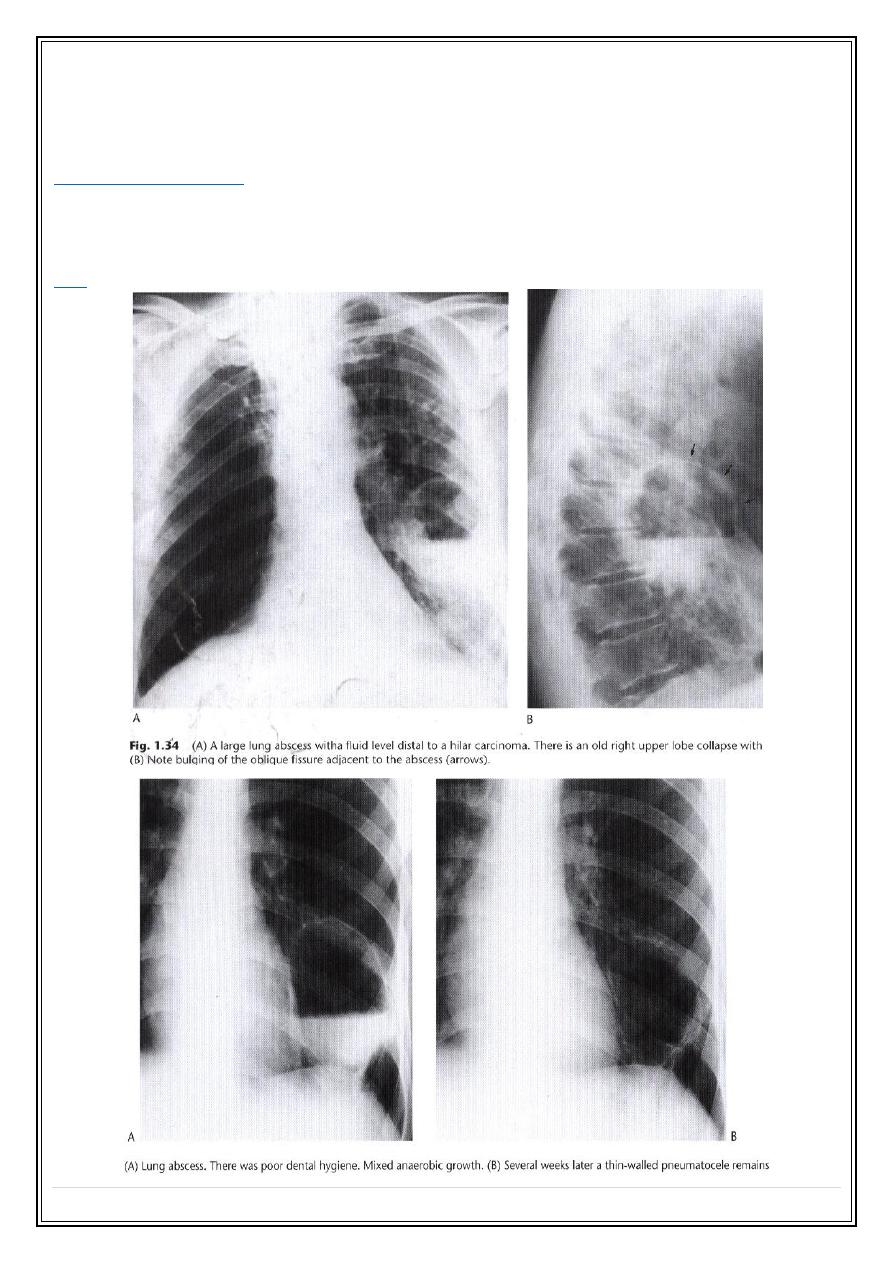
Lung abscess
Localized suppurative lesion of lung parenchyma
Radiological features:
1. usually seen as spherical shadow containing a central lucency
due to air with in the cavity.
2. an air-fluid level may be present.
ddx
Cavitating lung neoplasm
Secret Lectures
(6)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
6
Pulmonary TB
Types :
1.
Primary
: is the result of the first infection with mycobacterium
tuberculosis & usually occurs in childhood.
2.
Post primary
: believed to be re-infection, the patient having developed
relative immunity following the primary infection.
Primary TB
Radiological features:
➢
an area of consolidation (
Ghon focus
) developed in the periphery of the
lung usually in the mid or upper zones.
➢
often accompanied by visible
enlarged hilar or mediastinal lymph nodes .
(Ghon focus+ large LN = primary complex)
➢
in most cases, whether treated or not , the primary complex heals &
often calcifies. A calcified complex often remains visible throughout life.
➢
Spread of primary TB infection may occurs:
1. via the bronchial tree leading to
tuberculous bronchopneumonia
. Which
appears radiologically as patchy or lobar consolidation, its often involves
more than one lobe, may be bilateral and frequently cavitates.
2. via the blood stream, resulting in
miliary TB
. a pleural effusion may be
present.
➢
primary TB may present with
pleural effusion
, occasionally the primary
complex is also visible, but more often the effusion is the only visible
abnormality.
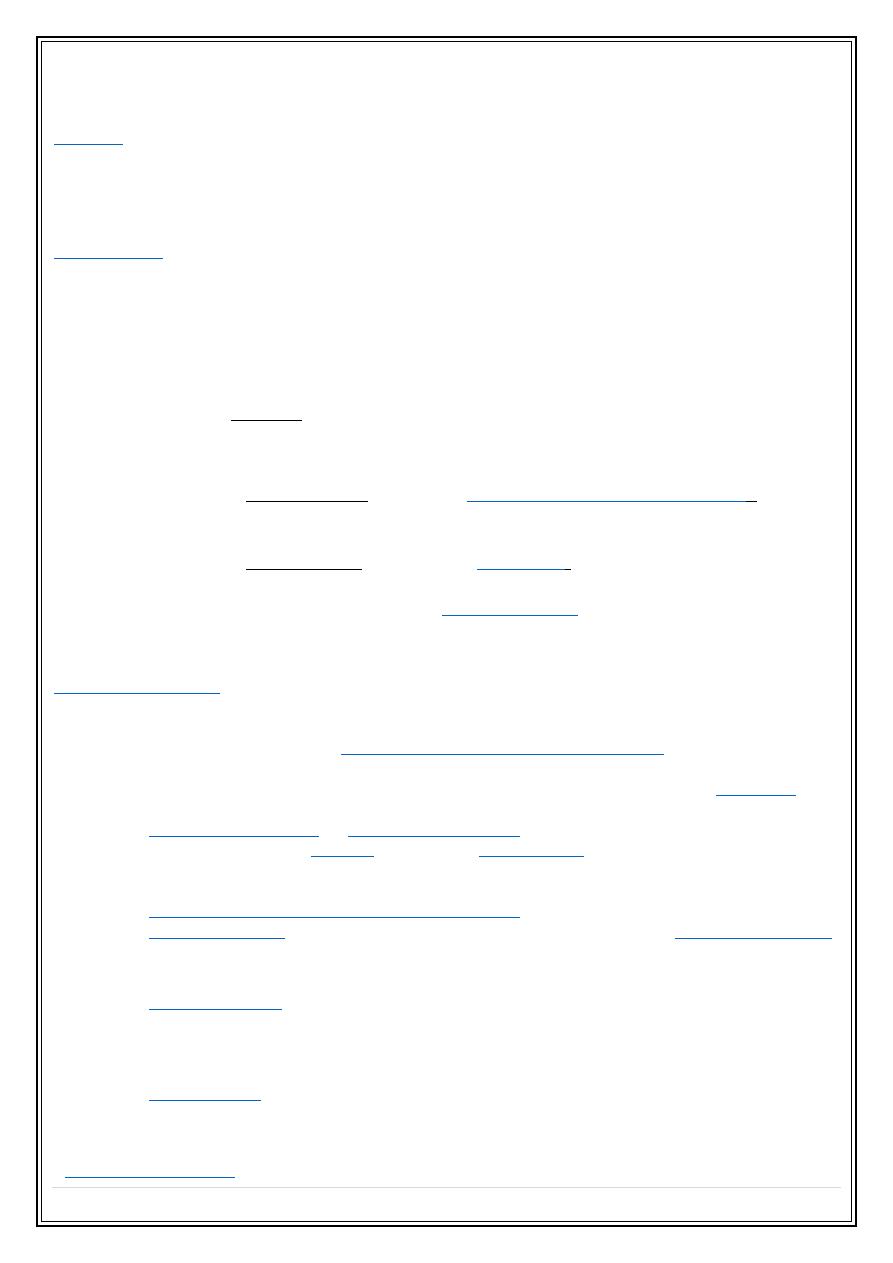
Post primary TB:
➢
Is usually confined to the upper posterior portions of the chest ( the apical &
posterior segments of the upper lobes & the apical segments of lower lobes ).
➢
The initial lesions are
multiple small areas of consolidation
& are often
bilateral.
➢
If the infection progress the consolidations enlarge & frequently
cavitates
.
➢
As with primary form, postprimary TB may spread to give widespread
bronchopneumonia
or
miliary tuberculosis
.
➢
Healing occurs by
fibrosis
, often with
calcification
, but both fibrosis &
calcification may be seen in the presence of continuing activity.
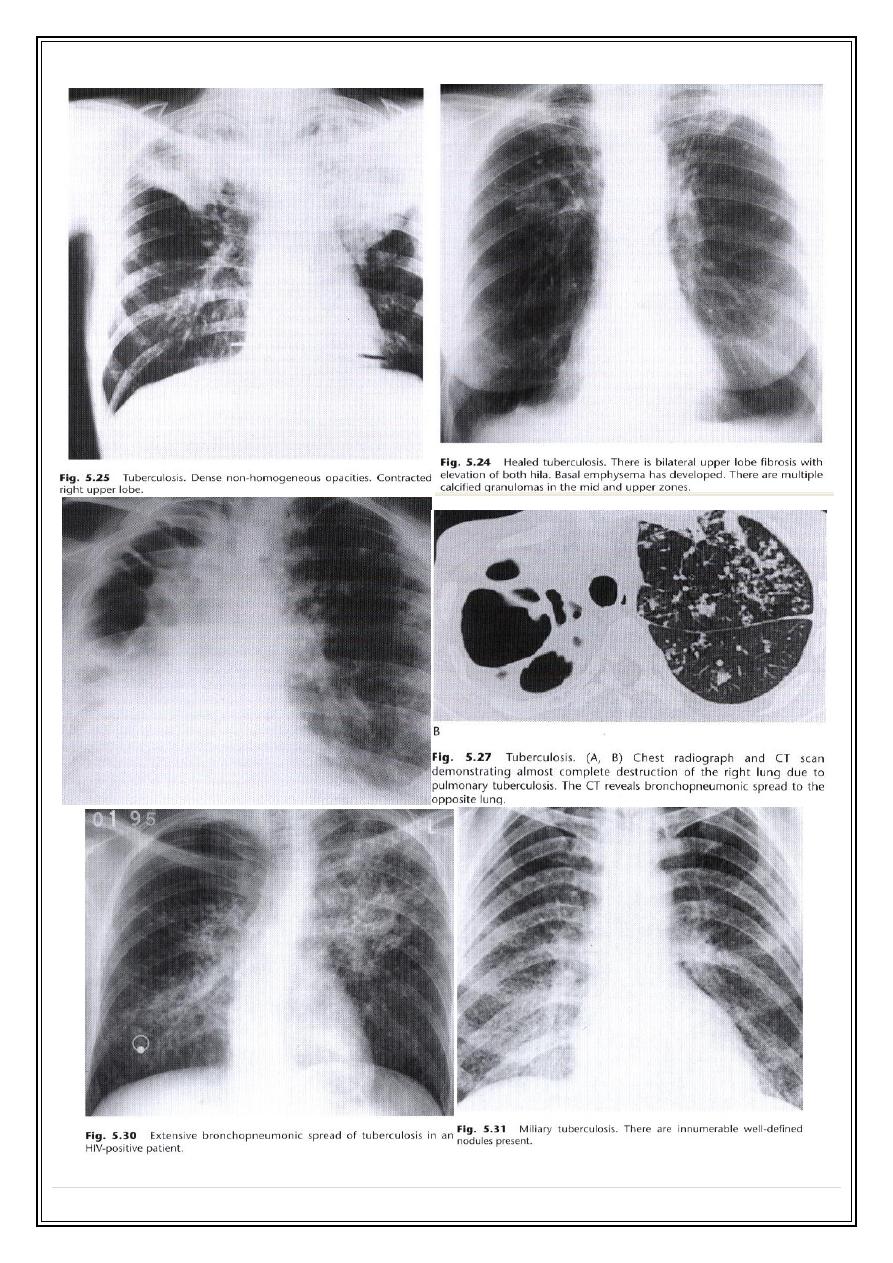
➢
The predominant or sole feature, particularly in non Caucasian , may be
mediastinal and/or hilar lymphadenopathy
.
➢
Pleural effusion
are frequent. They often leaves permanent
pleural thickening
which may on occasion
calcify.
➢
Tuberculoma
a tuberculous granuloma in the form of a spherical mass ,
usually less than 3 cm in diameter. the edge is usually sharply defined and
these lesions are often partly calcified ( CT may needed to demonstrate the
calcifications ).
➢
Mycetomas
a fungus Aspergillus fumigatus may colonize old TB cavity to
produce a ball of fungus ( mycetoma ) lying freely within the cavity. Air seen
between the mycetoma and the walls of the cavity (crescent sign).
Is the TB active ?
Secret Lectures
(6)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
7
Secret Lectures
(6)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
8
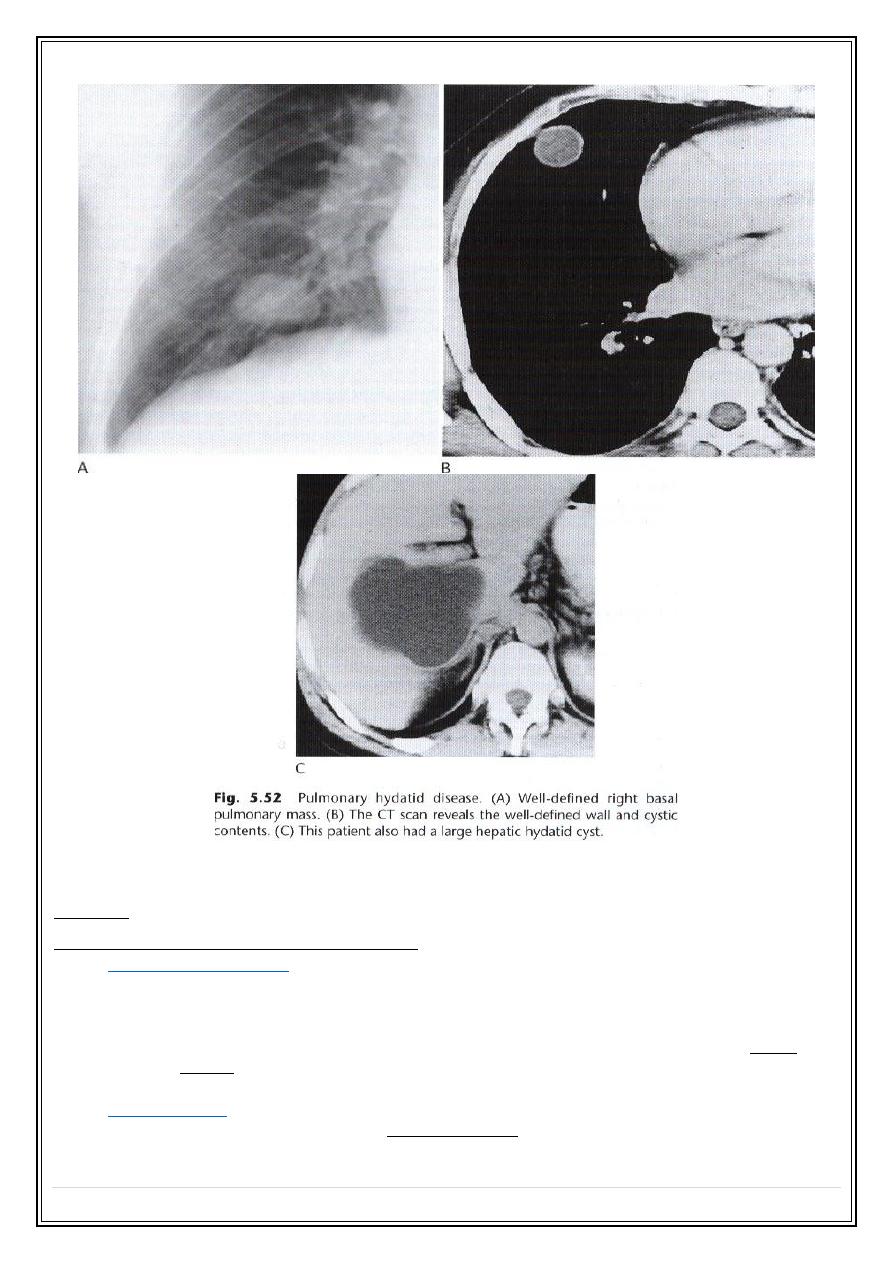
Hydatid disease
Pulmonary infection with Echinococcus granulosus may results in cysts
in the
lung or pleural cavity
.
These cysts may be
solitary or multiple
and are seen as
spherical shadows
with very well-defined borders. may be up to 10 cm in diameter
Approximately 20% of pulmonary cysts are bilateral &10% associated with
liver cysts.
Hydatid cysts occasionally
rupture
to produce complex cavities (air fluid
level, double walled cysts).
Secret Lectures
(6)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
9
Diseases of the airways
Asthma :
Chronic obstructive airways disease:
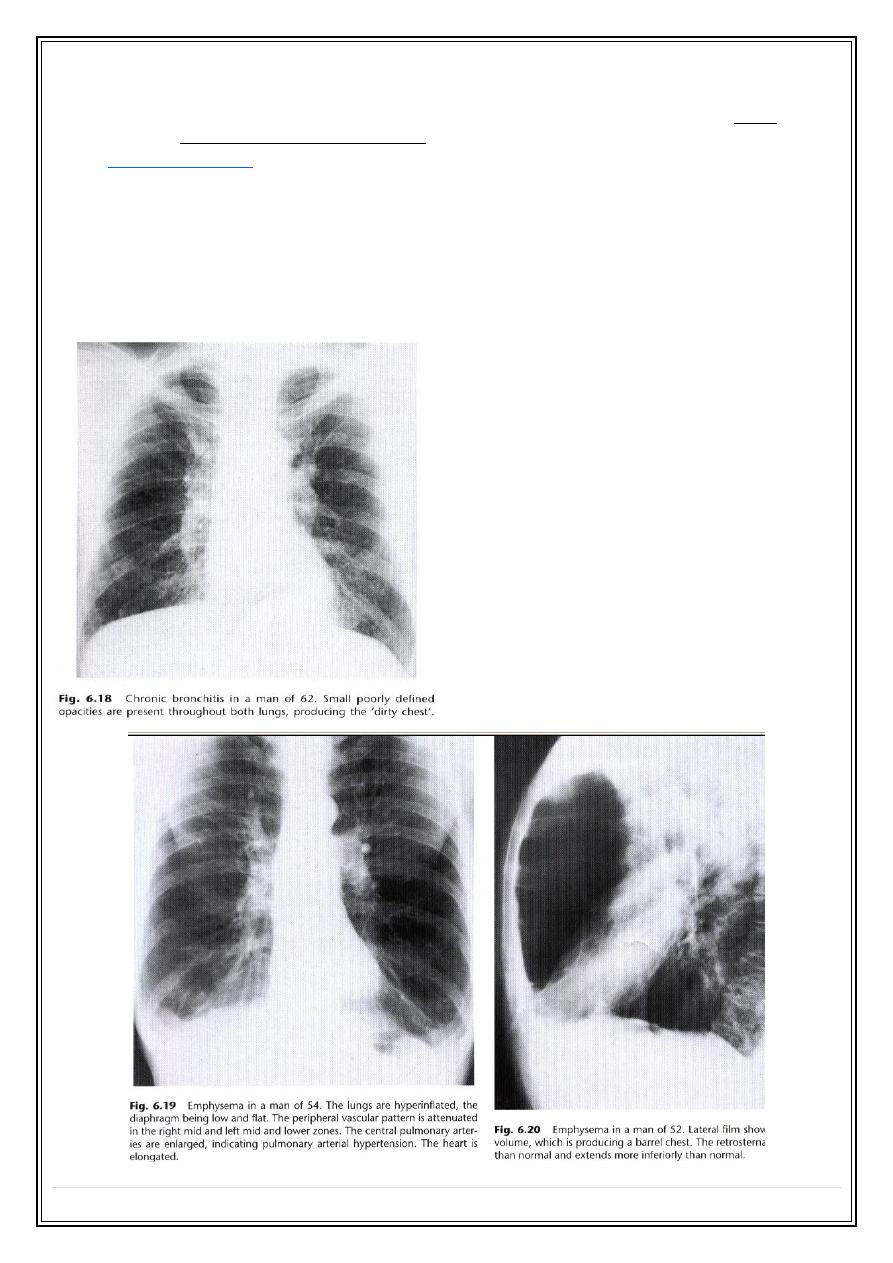
•
Chronic bronchitis
•
The chest film in uncomplicated chronic bronchitis is
usually normal .
•
If the film is abnormal , a complication such as emphysema, pneumonia or
core pulmonale has occurs .
•
An appearance which suggest chronic bronchitis is the so-called dirty
chest( generalized accentuation of bronchovascular marking & small
poorly defined opacities).
•
Emphysema
•
increase lung volume ( hyperinflations )—low or flat diaphragms, the heart
elongated or narrowed, the ribs are widely spaced.
Secret Lectures
(6)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
10
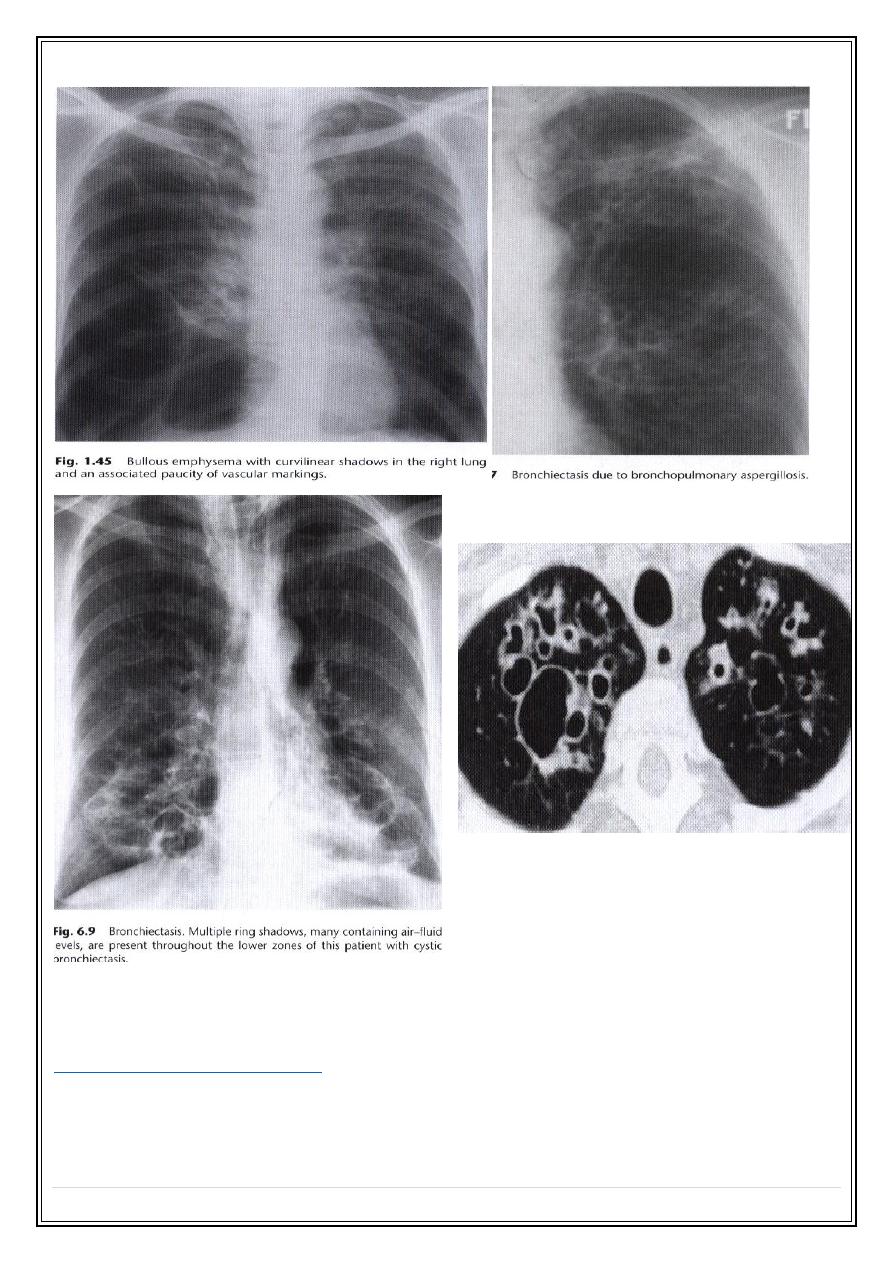
•
attenuation of the vessels—reduction in size and numbers , can be
generalized or localized. If severe the involved area is called a bulla
(localized destructive area )
•
Bronchiectasis
1. visibly dilated bronchi –
the thickened walls of the dilated bronchi may be
seen as tubular or ring shadows
, if fluid filled may be
opaque or air-fluid
level
.
2. a proportion of cases of symptomatic bronchiectasis have
norma
l chest X-
ray.
3. High resolution CT (HRCT ) both diagnostic & assess extent.
Secret Lectures
(6)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
11
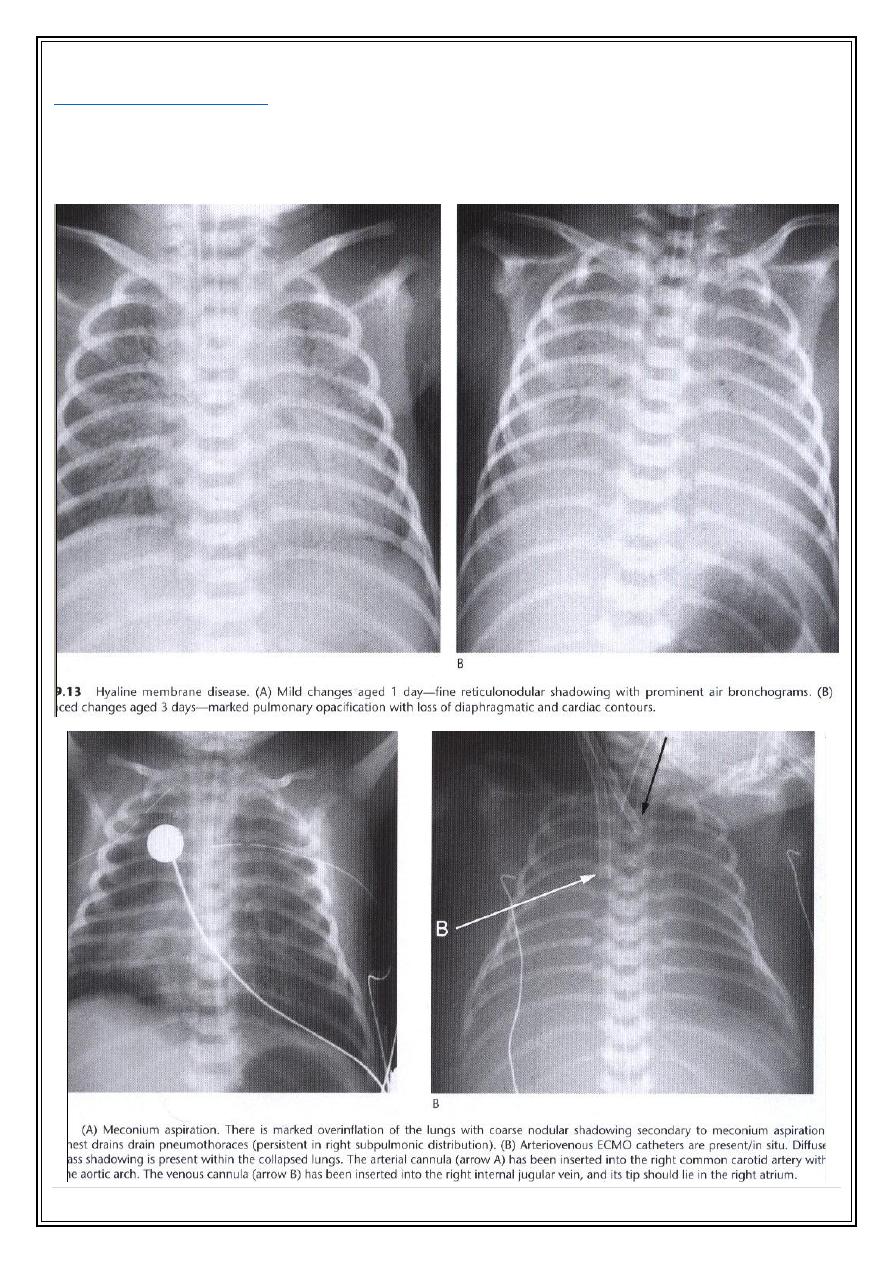
Respiratory distress of the new born
:
Hyaline membrane disease
- Premature infant.
- Wide spread very small pulmonary opacities and visible airbronchogram.
- The changes are nearly always uniform in distribution.
Secret Lectures
(6)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
12
Meconium aspiration:
-The pulmonary shadowing is usually patchy and distinctly streaky.
- Air bronchogram is not an obvious feature.
- The diaphragm is often lower than normal
Secret Lectures
(6)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
13
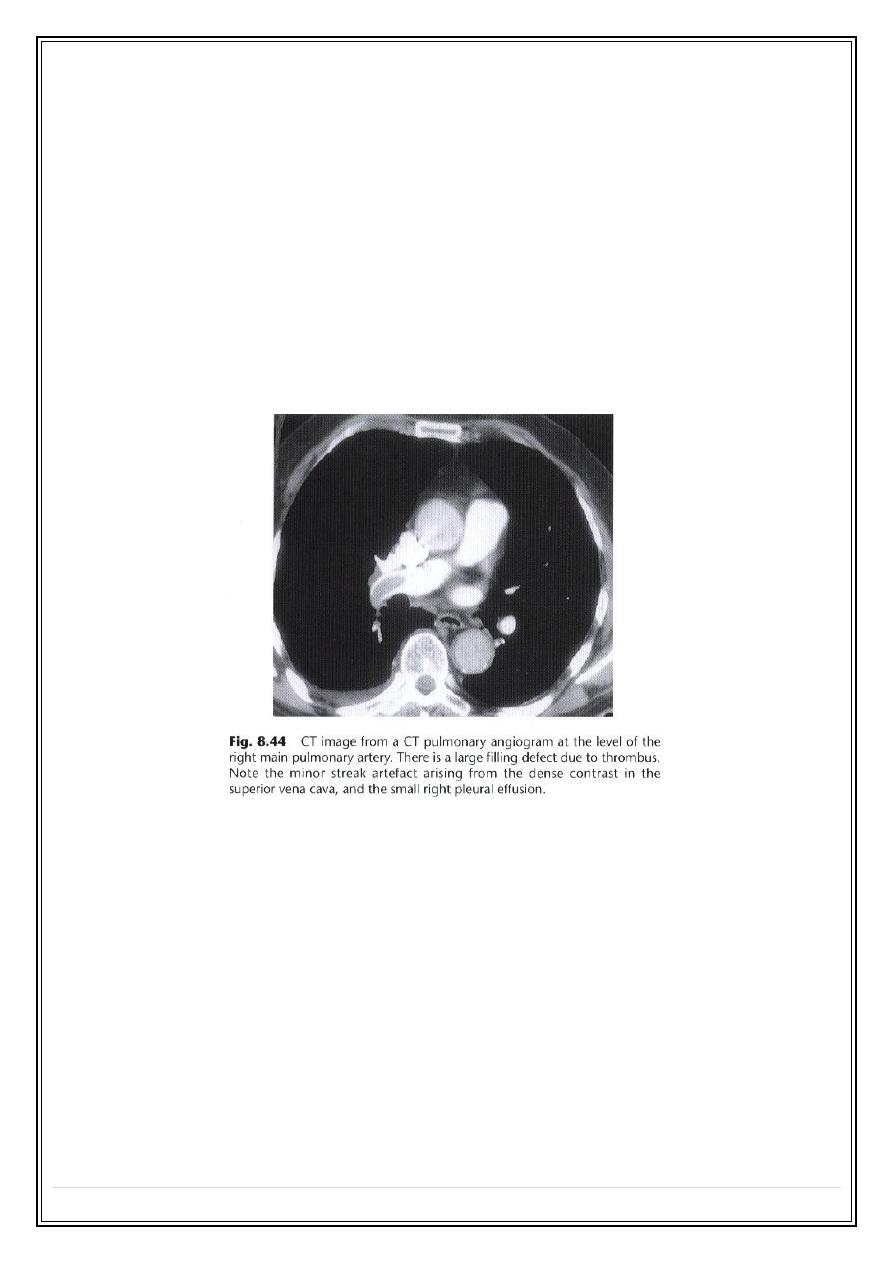
Pulmonary emboli and infarction
➢
In most cases even with massive pulmonary embolism the chest radiographs
show no abnormalities .
➢
Direct evidence of pulmonary embolism ; (
emboli
( --- conventional or CT
angiography.
➢
Indirect evidence of pulmonary embolism, (
infarction
).
➢
Radiologically , infarcts cause one or more areas of consolidation based on
the pleura and diaphragm. They often affect both lungs and are
indistinguishable from pneumonia. The differentiation depends on clinical
rather than radiological factors.
➢
Small emboli occurring over along period of time may cause pulmonary
hypertension ( radiological features of pulmonary hypertension)
Thank you,,,