Supracondylar Fractures Of The Femur
Dr. Jamal Al-Saidy
M.B.Ch.B. .F.I.C.M.S
Supracondylar fractures of the femur are encountered:
(a) in young adults, usually as a result of high energy
trauma
(b) in elderly, osteoporotic individuals.
Direct violence is the usual cause.
The fracture line is just above the condyles (Last 10
– 15 cm of femur)
but may extend between them.
In the worst cases the fracture is severely comminuted
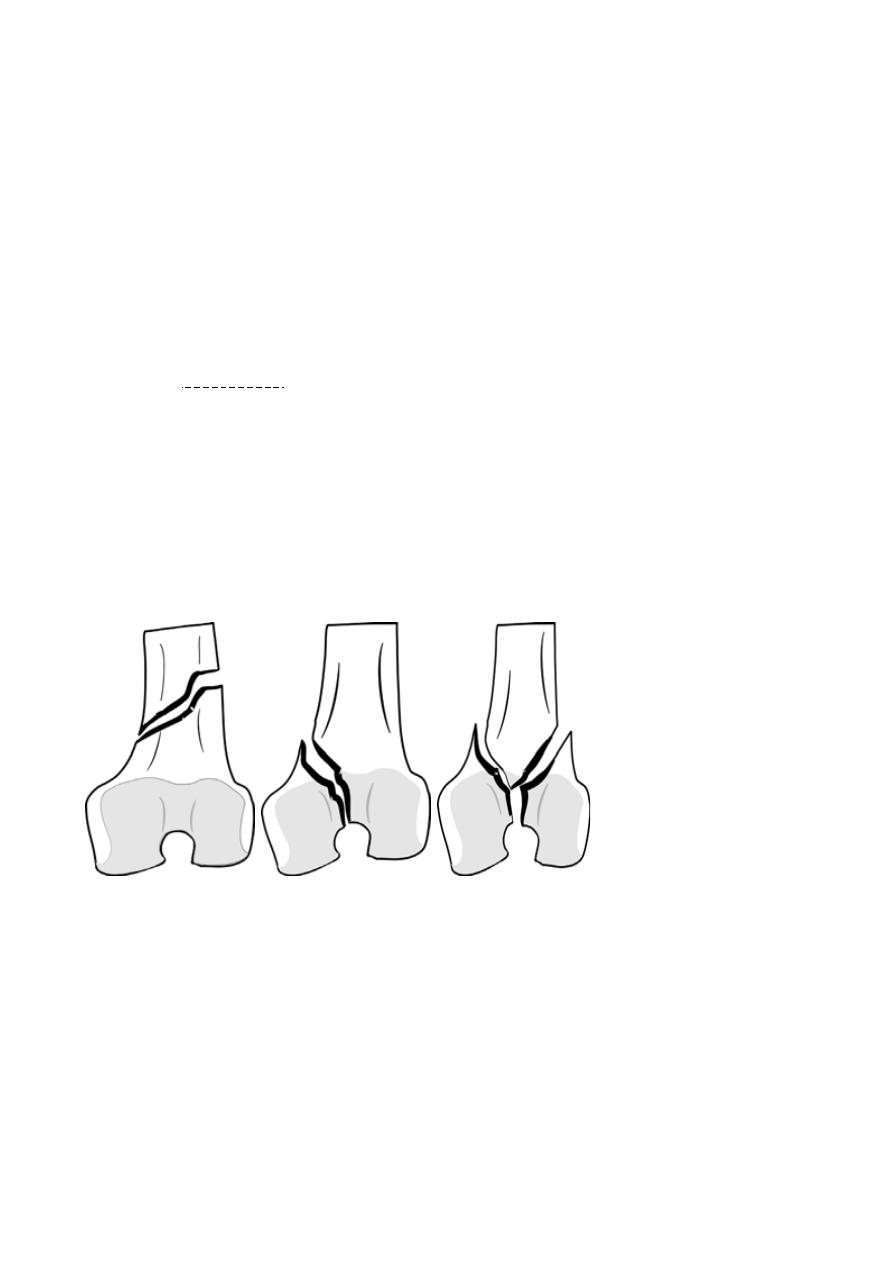
A useful classification is from the AO group:-
a. Type A fractures have no articular splits and are truly supracondylar (Extraarticlar).
b. Type B fractures are simply shear fractures of one of the condyles(Intraarticular unicondylar).
c.
Type C fractures have supracondylar and intercondylar fissures(Intraarticular bicondylar)
Gastrocnemius, arising from the posterior surface of the
distal femur, will tend to
pull the distal segment into extension and tilt the # posterior, thus risking injury
to the popliteal artery or compression of popliteal vessels & tibial nerve .
# may be T- or Y-shaped
# may be in the coronal plane (Hoffa #)
Type A Type B Type C
The AO classification of supracondylar fractures
(a) Type A fractures do not involve the joint surface
(b) type B fractures involve the joint surface (one condyle) but leave the
supracondylar region intact
(c) type C fractures have supracondylar and condylar components.
Clinical features
The knee is swollen because of a haemarthrosis – this can be severe enough to
cause blistering later.
Movement is too painful to be attempted.
The tibial pulses should always be checked to ensure the popliteal artery was not
injured in the fracture.
X-RAY :- The entire femur should be x-rayed so as not to miss a proximal
fracture or dislocated hip.
Treatment
Non-operative :-
o If the fracture is only slightly displaced and extra-articular, or if it reduces
easily with the knee in flexion, it can be treated quite satisfactorily by traction
through the proximal tibia; the limb is cradled on a Thomas’ splint with a
knee flexion piece and movements are encouraged. when the fracture is
beginning to unite, traction can be replaced by a cast and the patient allowed
up and partially weightbearing with crutches.
o Nonoperative treatment should be considered as an option if the patient is
young or the facilities and skill to treat by internal fixation are absent.
Operative :-
o Surgical treatment with internal fixation can enable accurate fracture
reduction, especially of the joint surface, and early movement.
o If the necessary facilities and skill are available, this is the treatment of
choice.
o For the elderly, early mobilization is so important that internal fixation is
almost obligatory.
o Several different devices are available:-
1.
Locked intramedullary nails.
2.
Plates that are applied to the lateral surface of the femur: traditional
angled blade-plates or 95 degree condylar screw- plates.
3.
Simple lag screws.
o Knee movements are started soon after operation, if wound healing allows.
This limits adhesions forming within the knee joint.
Complications
EARLY
o Arterial damage :- There is a small but definite risk of arterial damage and
distal ischaemia. Careful assessment of the leg and peripheral pulses is
essential, even if the x-ray shows only minimal displacement.
LATE
o Joint stiffness :- Knee stiffness – probably due to scarring from the injury and
the operation – is almost inevitable. A long period of exercise is needed in all
cases, and even then full movement is rarely regained. For marked stiffness,
arthroscopic division of adhesions in the joint or even a quadricepsplasty may
be needed.
o Malunion :- Internal fixation of these fractures is difficult and malunion –
usually genu varus, valgus and recurvatum – is not uncommon. Corrective
osteotomy may be needed for patients who are still physically active.
o Non-union:- If non-union does occur, autogenous bone grafts and a revision
of internal fixation will be needed.
o OA of the knee.
Fracture-Separation Of Distal Femoral Epiphysis
In the childhood or adolescent equivalent of a supracondylar fracture,
the lower femoral epiphysis may be displaced – either to one side (usually
laterally) by forced angulation of the straight knee or forwards by a
hyperextension injury.
This injury is important because of its potential for causing abnormal growth
and deformity of the knee.
The fracture is usually a Salter–Harris type 2 lesion – i.e. physeal separation
with a large triangular metaphyseal bone fragment.
This type of fracture usually has a good prognosis, asymmetrical growth
arrest is not uncommon and the child may end up with a valgus or varus
deformity.
The fracture can usually be perfectly reduced manually, but further x-ray
checks will be needed over the next few weeks to ensure that reduction is
maintained.
Occasionally open reduction is needed; a flap of periosteum may be trapped
in the fracture line. Salter– Harris types 3 and 4 should be accurately reduced
and fixed.
THANK YOU
Dr. Jamal Al-Saidy
M.B.Ch.B. .F.I.C.M.S
