

• Mechanical and chemical plaque controlDR HUSSEIN AL DABBGH
• Definition• Plaque control: the removal of dental plaque on a regular basis and the prevention of its accumulation on the teeth and adjacent gingival surfaces.
• Position: supra- & sub-gingival plaque control
• Methods: mechanical & chemical• Brushing
• Interdental cleaning• Adjunctive aids:
• 1. Dental irrigation devices 2.Tongue scrapers 3.Dentifrices
• Self-performed plaque control
• tooth brush
• 1- handle:The part grasped in the hand during tooth brushing.
• • 2- head : it is the working end of tooth brush that hold bristles.
• • 3- tufts: clusters of bristles secured into head
• Toothbrush bristles
• Natural: hog.• Artificial filaments: nylon which are uniform in size & elasticity, resistant to fracture & doesn’t get contaminated.
• Soft brush: 0.007 inch(0.2 mm(
• Medium brush: 0.012 inch(0.3 mm(• Hard brush: 0.014 inch(0.4 mm(
• Bristle hardness
• American Dental Association (ADA(
• Brush length: 1 -1.25 inches• 2-4 rows
• 5-12 tufts per row
• For most patients, short-headed brushes with straight-cut, round-ended, soft to medium nylon bristles arranged in three or four rows of tufts are recommended.
• Effects and sequelae of the incorrect use of mechanical plaque removal devices
• Gingival erosion
• Gingival recession
• Cervical abrasion
• Toothbrush stiffness
• Method of brushing
• Brushing frequency


• Brushing technique
• Horizontal brushing (scrub(• Leonard method (vertical(
• Bass method
• Modified Stillman method (roll(
• Charters method
• Methods of cleaning with powered toothbrushes
• MODIFIED STILL MAN
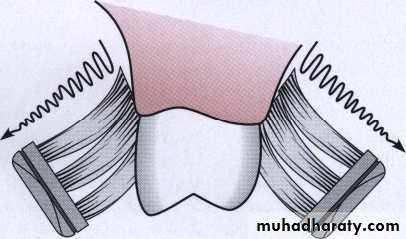
• Modified Stillman method. This method requires placement of the sides of the bristles against the teeth and gingiva while moving the brush with short, back-and-forth strokes in a coronal direction.
• Dental plaque removal from cervical areas below the height of contour of the enamel & from exposed proximal surfaces .
• General application for cleaning tooth surfaces and massage of the gingiva
• Recommended for cleaning in areas with progressing gingival recession & root exposure to prevent further tissue destruction.
• Bass method
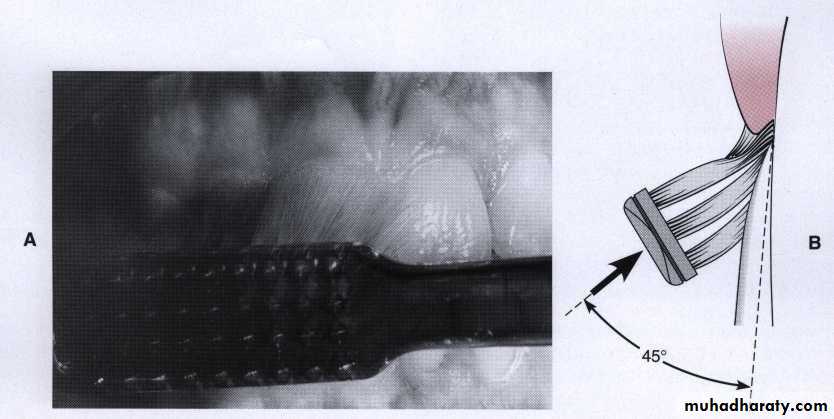
• Bass method. A, Proper position of the brush in the mouth aims the bristle tips toward the gingival margin. B, Diagrams shows the ideal placement, which could permit slight subgingival penetration of the bristle tips
• Technique:
• Place the head of a soft brush parallel with the occlusal plane, Place the bristles at the gingival margin, establishing an angle of 45 degrees to the long axis of the teeth. Exert gentle vibratory pressure, using short back and- forth motions without dislodging the tips of the bristles. This motion forces the bristle ends into the gingival sulcus area as well as partially into the interproximal embrasures. The pressure should produce perceptible blanching of the gingiva. Complete approximately 20 strokes in the same position.• This repeated motion cleans the tooth surfaces, concentrating on the apical third of the clinical crowns, the gingival sulci, and as far onto the proximal surfaces as the bristles can reach. Lift the brush, move it to the adjacent teeth, and repeat the process for the next three or four teeth.
• Advantage
• The short back-and-forth motion is easy to master because• it is a simple movement familiar to most patients who brush using a scrub technique.
• It concentrates the cleaning action on the cervical and interproximal portions of the teeth, where microbial
• plaque is most likely to have accumulated.
• The Bass technique is efficient and can be recommended for any patient with or without periodontal involvement.
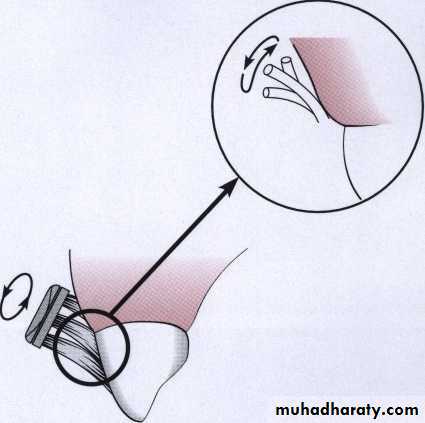
• Charters method. The Charters method requires that the bristles be pressed against the sides of the teeth and gingiva.The brush is moved with short circular or back-and-forth strokes
• CHARTER’S METHOD
• INDICATIONS
• - Individual’s having open inter- dental spaces with missing papilla & exposed root surfaces.• For patients who have had periodontal surgery
• Patients with moderate gingival recession particularly inter-proximal (receded interdental papillae(.
• Disadvantages
• Brush ends don’t engage the gingival sulcus to remove sub gingival bacterial accumulations.• Requirements in digital dexterity are high.
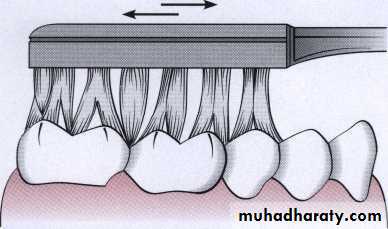
• This brush position on occlusal surfaces of the teeth is used with any technique, including the Bass, Stillman, or Charters method.
• Powered toothbrushes
• Powered toothbrushes are not generally superior to manual ones• The heads of these tooth brushes
• oscillate in a side - to – side motion or in a rotary motion• •

• Powered toothbrushes have been shown to improve oral health:
• Children and adolescents• Children with physical or mental disabilities
• Hospitalized patients
• Patients with fixed orthodontic appliances
• Interdental cleaning aids
• Dental floss
• Interdental brushes
• Wooden or rubber tips• Dental floss
• Multifilament vs. monofilament• Twisted vs. untwisted
• Waxed vs. unwaxed
• 12-18 inches for use
• Stretch: thumb and forefinger
• wrapped around proximal surface, and removes plaque by using
• several up-and-down strokes. The process must be repeated for the distal surface of tooth

• Flossing can be made easier by using a floss holder
• Although use of such devices can be more time consuming than finger flossing, they are helpful for patients lacking manual dexterity and for nursing personnel• assisting handicapped and hospitalized patients in cleaning their teeth.
• Floss holders



• Powered flossing devices are also available These devices have a single bristle that moves in a circular motion. The devices have been shown to be safe and effective but no better at plaque removal than finger flossing


• Interdental brush
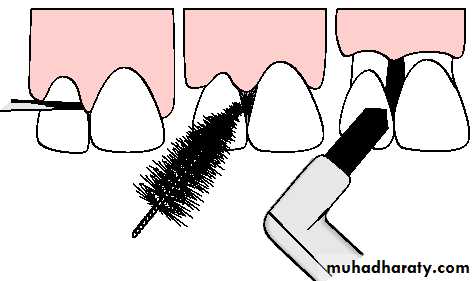
• Interdental brushes
• Interdental brushes are coneshaped or cylindric brushes made of bristles mounted on a handle .• single-tufted brushe particularly suitable for cleaning large, irregular, or concave tooth surfaces adjacent to wide interdental spaces.


• Technique
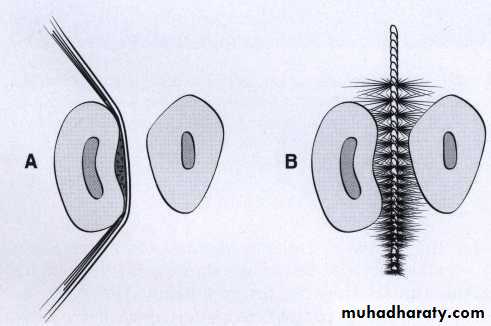
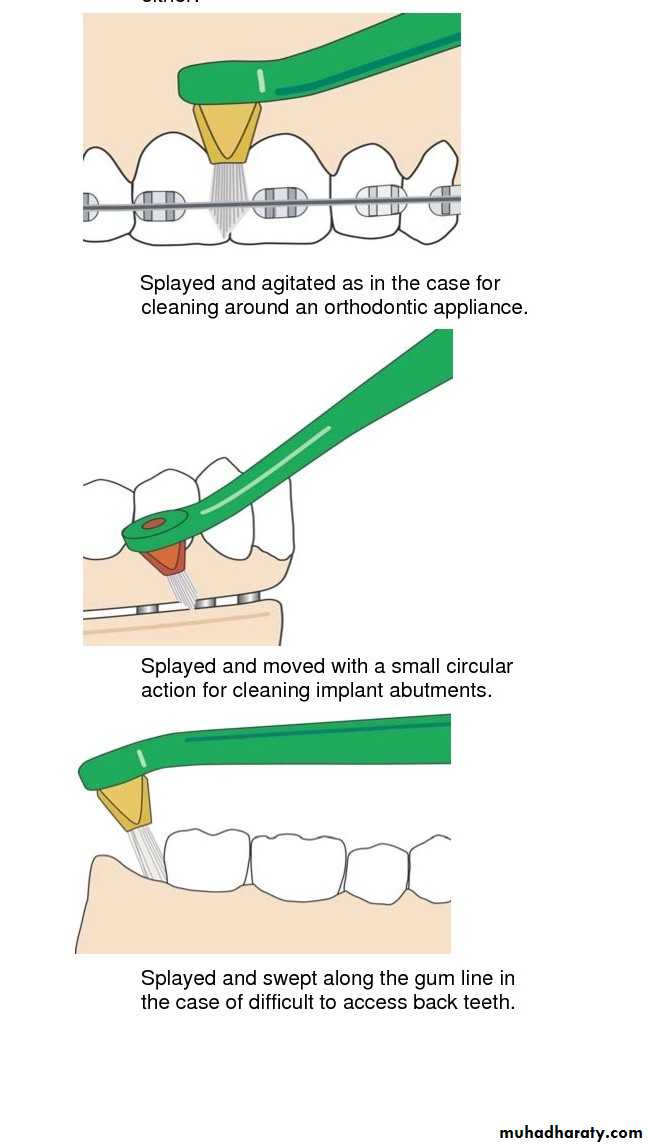
• Interdental brushes of any style are inserted through interproximal spaces and moved back and forth between the teeth with short strokes. For most efficient cleaning, it is probably best to select the diameter of brush that is slightly larger than the gingival embrasures to be cleaned. This size permits bristles to exert pressure on both proximal tooth surfaces, working their way into concavities on the roots.• Single-tufted brushes are highly effective on the lingual surface of mandibular molars and premolars, where the tongue often impedes a regular toothbrush, and may provide access to furcation areas and isolated areas of deep recession

• Wooden or rubber tip
• Wooden tips are used either with or without a handle. Access• is easier from the buccal surfaces for those tips without
• handles, primarily in the anterior and bicuspid areas.

• Soft, triangular wooden picks or plastic alternatives are placed in the interdental space in such away that the base of the triangle rests on the gingiva and the sides are in contact with the proximal tooth surfaces The pick is then repeatedly moved in and out of the embrasure, removing soft deposits from the
• teeth and mechanically stimulating the papillary gingiva.
• The disadvantage of the triangular toothpick is that:
• it is very hard to access any surfaces other than the facial
• surfaces in the more anterior region of the mouth. Only used in large gingival embeassure
• Rubber tips come mounted on handles or the ends of toothbrushes and can easily be adapted to all proximal surfaces in the mouth.
• Various plastic tips are also available and can be used in a manner similar to wooden tips.
• Both rubber and plastic tips can be rinsed and reused and easily carried in a pocket or purse, features that are attractive to some patients.
• Rubber tips should be placed into the embrasure space and used in a circular motion. They can be applied to interproximal spaces and other defects throughout the mouth and are easily adaptable to lingual surfaces.


• Adjunctive aids
• Dental irrigation devices• Tongue scrapers
• Dentifrices
• Water Flosser
• The two main physical features of water flossing action include pulsation and pressure. Pulsation essentially regulates pressure.• A combination of these two actions allows for disruption of bacterial activity, the expulsion of subgingival bacteria and the
• removal of loosely lodged debris and food particles.
• The elderly who suffer from arthritis or other conditions that compromise the use of their hands may find the Water Flosser easy to manage and control
• These inserts are designed to address patient needs tongue cleansing, orthodontic appliances, fixed restorative appliances, deeper periodontal pocket areas



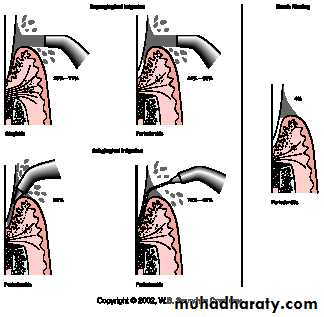
• Irrigation devices
• subgingival irrigation performed with an oral irrigator• using chlorhexidine diluted to one-third strength, performed
• regularly at home after scaling, root planing, and
• in-office irrigation therapy, has produced significant gingival
• improvement compared with controls.
on of sulfur compou
• Tongue scraber is an oral hygiene device designed to clean the bacterial builed up, food debris, fungi and dead cells from the surface of the tongue bacteria and fungi that grow on the tongue may cause halitosis due to producti nd
• Tongue scrapers




• Chemical plaque control
• Antiadhesive• Antimicrobial
• Plaque removal
• Antipathogenic
• Vehicles for the delivery of chemical agents
• Toothpaste• Mouthrinses
• Spray
• Irrigators
• Chewing gum
• Dentifrices
• Dentifrices aid in cleaning and polishing tooth surfaces
• Paste, powder and gel
• Abrasive: silica, alumina, dicalcium phosphate, and calcium carbonate make up 20% to 40% of a dentifrice. Tooth powders contain about 95% abrasives and are five times more abrasive than pastes.• Detergent: sodium lauryl sulfate
• Thickeners: silica and gums
• Sweeteners: saccharine
• Humectants: glycerine and sorbitol
• Flavors: mint, peppermint
• Actives: fluorides, triclosan and stannous fluoride
• Mouthrinse
• ADA has accepted two agents for treatment of gingivitis:• solutions of chlorhexidine digluconate mouthrinse
• essential oil mouthrinse thymol, eucalyptol,menthol, and mythyl salicylate work by altering bacterial cell wall
• Chlorohexidine action:
• Increase bacterial membrane permeability followed by coagulation of cytoplasmic macromolecules• Has substantivity ability of substance to adher to the structur to be released for long time
• Chlorhexidine-side effects
• Brown discoloration
• Taste perturbation
• Oral mucosal erosion
• Disclosing agents
• Solutions or wafer capable of staining bacterial deposits on the surfaces of teeth, tongue, and gingiva
• Erythrosine, fuchsin
• Fluorescein-containing dye