Fifth Stage
E.N.T
Dr.Mushtaq – Lecture 19
1
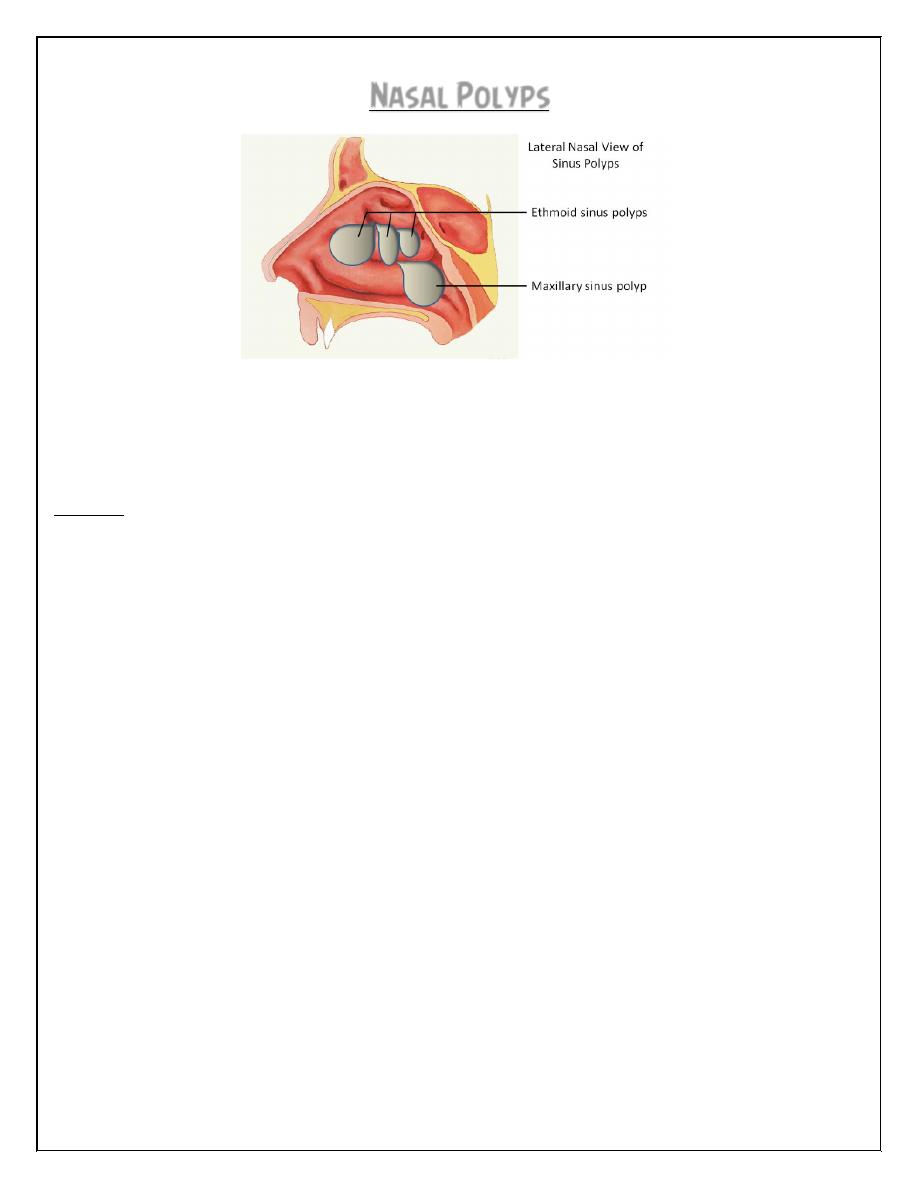
Nasal Polyps
Nasal polyps
A pedunculated portion of edematous mucosa of the nose or para-nasal sinuses.
Aetiology and pathology
Types:
1. Simple. oedematous submucosa, very loose fibrillary stroma, with intercellular
serous (not mucinous) fluid. The surface is covered with ciliated columnar epithelium
in the early stage: metaplasia to a transitional and then to a squamous type occurs
in some cases..
Allergic: usually multiple,eosinophils and plasma cells are found in large numbers
similar to allergic, but no allergen identifiable.
Inflammatory: the role of infection is unclear They are not common but may be :
(a) 'Acute', an uncommon type, usually associated with influenza. The polypus is
usually single, very soft, and slightly haemorrhagic.
(b) 'Chronic non-specific' often multiple.
(c) 'Chronic specific'. Rhinosporidiosis causes a friable bleeding polypus .
Mixed infective-allergic: Probably represents secondary infection in the allergic or
vasomotor type.
Aspirin intolerance: the mechanism of development is not known but is not
allergic. When associated with asthma the recurrence rate is particularly high.
2. Neoplastic
Benign: fjbroangioma, granuloma, neurofibromas, transitional-cell tumours. and
fibromas
Malignant: carcinomatous, melanoma , lymphomatous or sarcomatous,
2
Sites of origin
1. Ethmoidal the commonest
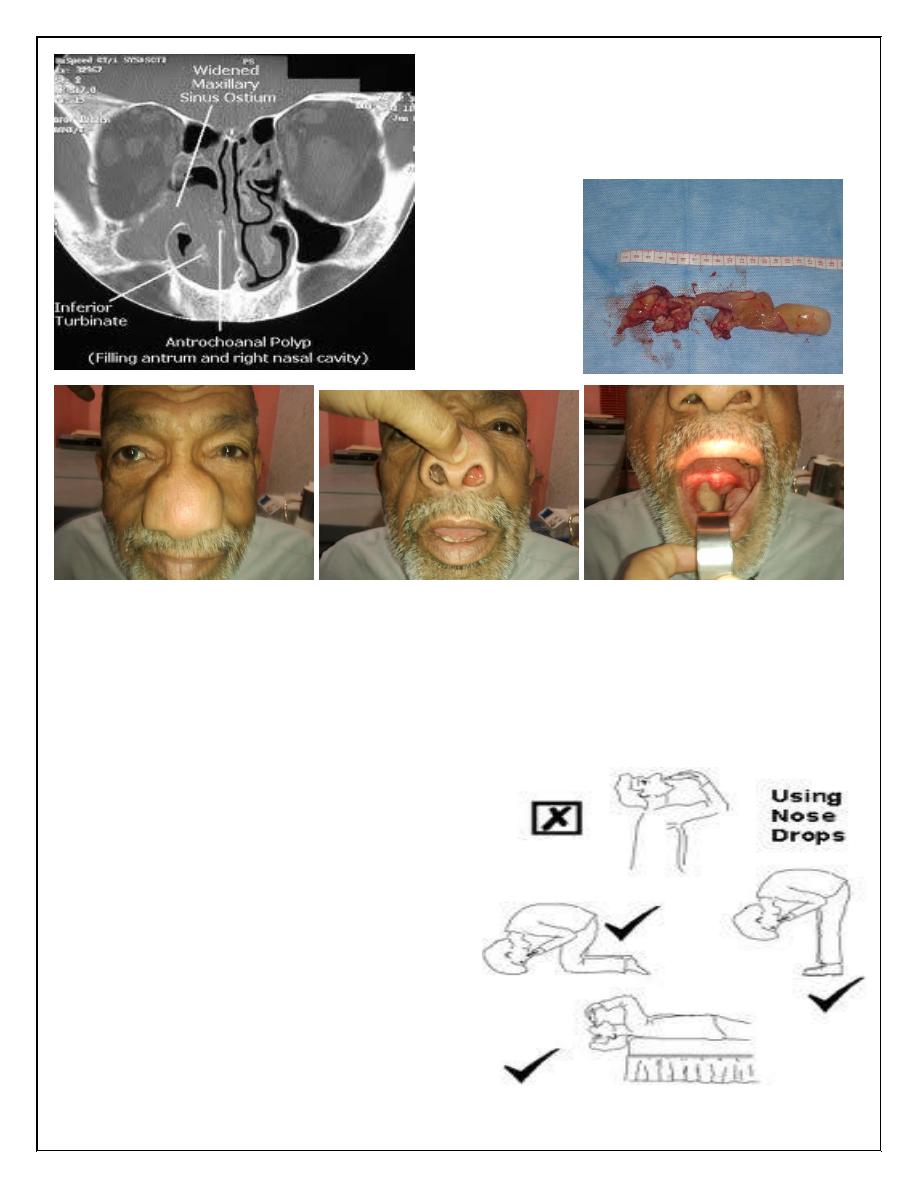
2. Antral (maxillary). less , may be multiple or a single polypus may emerge from
the sinus ostium and extend backwards to the posterior choana (antrochoanal
polypus).
3. frontal or sphenoidal.
Age incidence
Simple ethmoidal polypi usually occur in adults but children with cystic fibrosis can
have them.
Antrochoanal polypi occur more commonly in children and young adults.
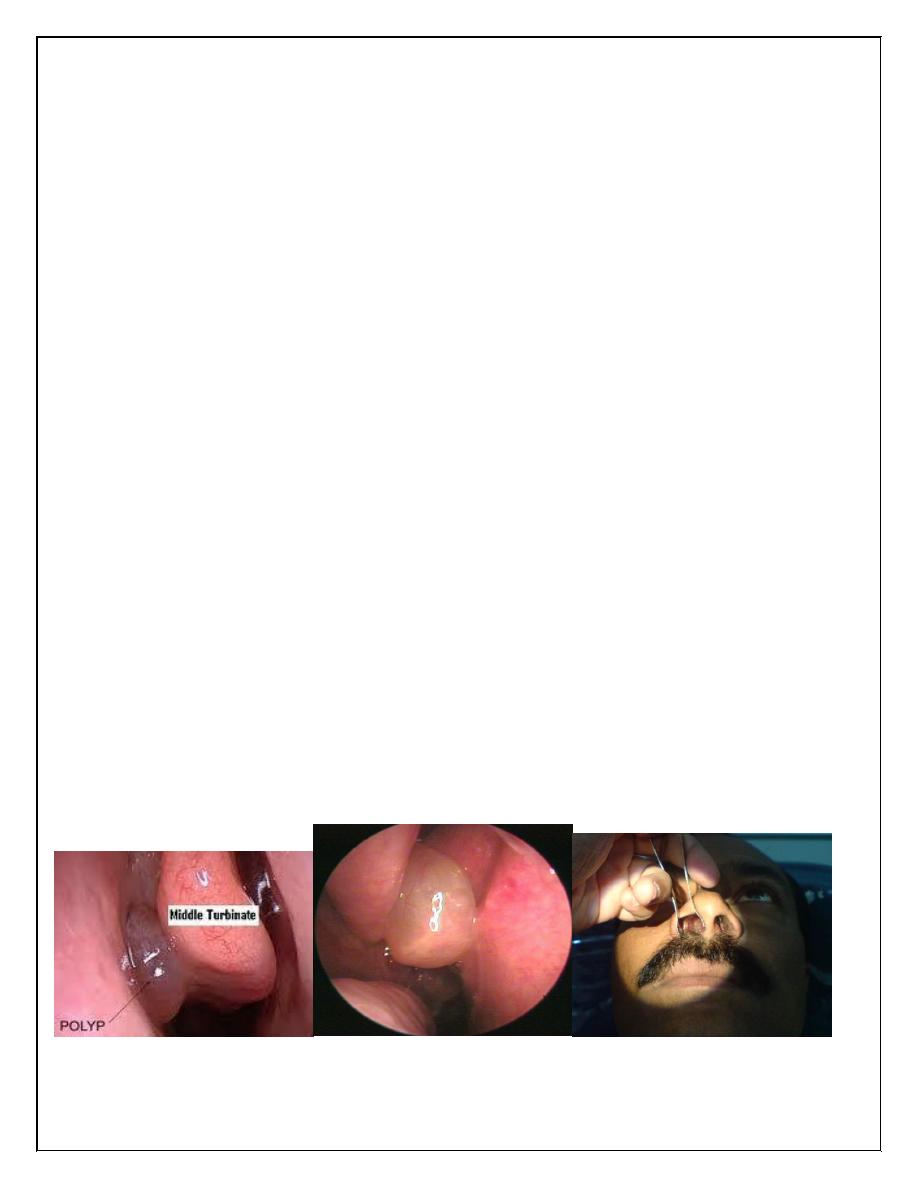
Clinical features
Male/ Female; 3/1.
Onset usually insidious, but may be sudden and rapid after an acute infection.
Nasal obstruction is the chief symptom.
Other features : anosmia, epiphora, postnasal 'catarrh' (irritation and drip),
headaches, snoring and speech defects.
Purulent rhinorrhoea
Expansion of the nasal bones ('frog-face').
Diagnosis
Biopsy is essential when the polypus is unilateral and haemorrhagic.
Radiography CT scan is best
3
Treatment
Conservative; in early cases
1.Antihistamine applied locally or given by mouth.
2. Topical steroid therapy.
Beclomethasone aerosol spray often shrink existing polypi and prevent recurrence
of those removed surgically.
3.Combination therapy.
a. Oral prednisolone on a reducing dose
regimen is given for 15 days starting with
60 mg/day.orally
b. steroid nasal drops(ophtamethasone)
are administered four times daily for a
month.
c. An antibiotic is given for a week if
infection is clear.
d. Antihistamine as well
4
Surgical
Required when obstructive symptoms are established.
1. Minor procedures. Removal with the cold-wire snare
2. Major procedures are indicated for recurrent multiple polypi; for gross
infection; for antrochoanal polyp.
may be performed by :
(a) Intranasal
. Functional endoscopic surgery
(b) External
Sublabial antrostomy is used for recurrent antrochoanal polypi. .
Long-term management
Removal of polypi is best followed by long-continued antihistamines by mouth, and
regular courses of topical steroid aerosol or drops.
Thank you,,,