Pelvic fractures

Introduction :
Fractures of the pelvis account for less than 5% of all skeletal injuries, but it is important because it associated with:-blood loss and shock.
Soft tissue injuries ( esp urogenital )
Sepsis.
ARDS.
Because of those mortality rate exceeds 10%.
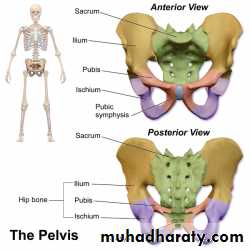
Relevant anatomy :
BONES :Pelvis formed of tow innominate bones
Attached to the sacrum posteriorly .
Each innominate bone formed from fusion of 3 bones ( pubis , ischium and ileum )
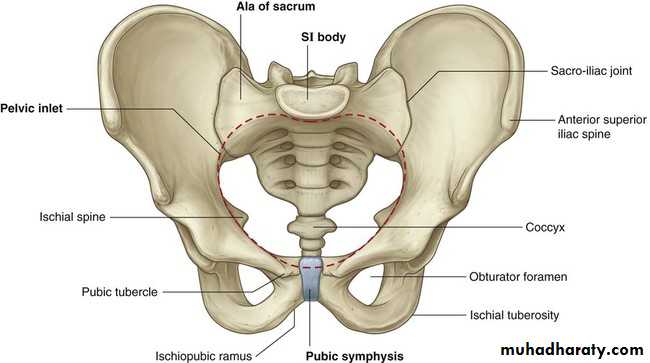
Pelvic ring :
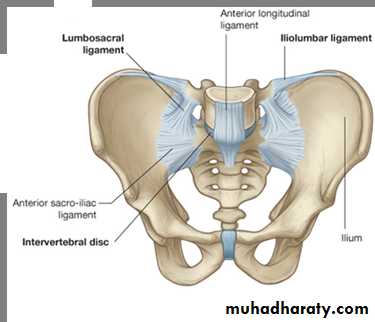
Ligaments :
Anterior ligaments - Symphyseal ligaments (resist external rotation)posterior sacroiliac complex (posterior tension band)
strongest ligaments in the body , more important than anterior structures for pelvic ring stability
– anterior sacroiliac ligaments
– interosseous sacroiliac lig
– posterior sacroiliac lig
Clinical assessment
History/mechanism of injury
• pelvic injuries usually caused by high energy mechanisms (Most commely MVA)
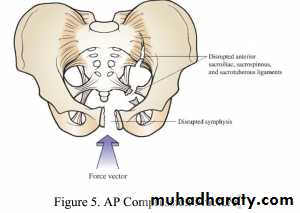
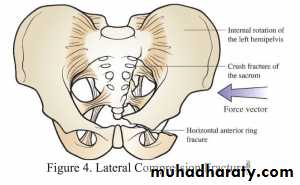
Anterior posterior compression – secondary force in an AP direction leading to diastasis of the symphysis pubis, with or without diastasis of the sacroiliac joint.Lateral compression – lateral compression force, which cause rotation of the pelvis inwards, leading to fractures in the sacroiliac region and pubic rami.
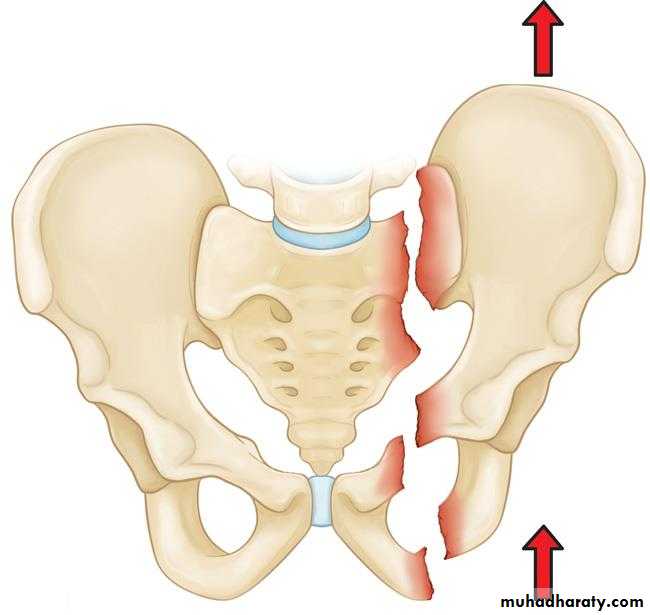
Vertical shear – an axial shear force with disruption sacroiliac junction, combined with cephalic displacement of the fracture.
Combined mechanism – a combination of two of the above mechanisms , which leads to a pattern of pelvic fracture that is a combination of one or more of the above fracture types
Physical Examination ( ATLS )
Primary survey :-Begins with the ABCs (airway, breathing, and circulation)
hemorrhagic shock is common with pelvic injuries
Secondary survey :-
PELVIC COMPRESSION/DISTRACTION test
Examination of perineum ( for hematoma or bleeding )
Rectal and vaginal examination.
Examination of lower limbs.
imaging
Plain radiography :
AP ,
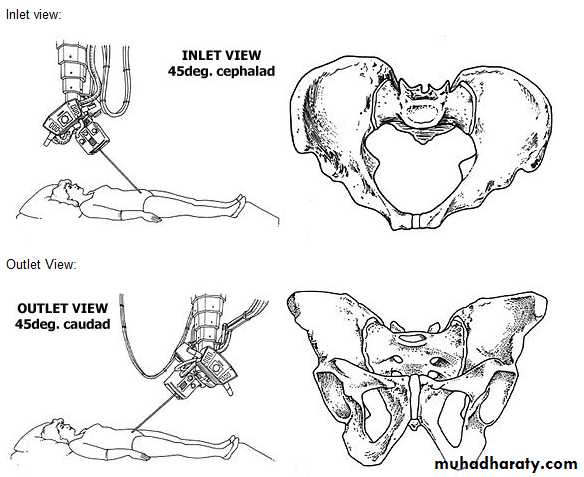
inlet and outlet views
iliac oblique and obturator oblique views for acetabulum fracture assessment
CT SCAN :
CT is the modality of choice for accurately showing acetabular or pelvic ring fractures

Other investigations :
• BLOOD GROUPING AND CROSSMATCHING
• FAST ( for associated visceral injuries )• DIAGNOSTIC PERITONEAL LAVAGE ( for intraperitoneal bleeding )• CT ANGIO ( for persistant shock )
• RETROGRADE URETHROGRAM ( fro associated urethral injuries )
CLASSIFICATION of pelvic fractures
Young and Burgess Classification is the Most common classification used and Based on the mechanism of injury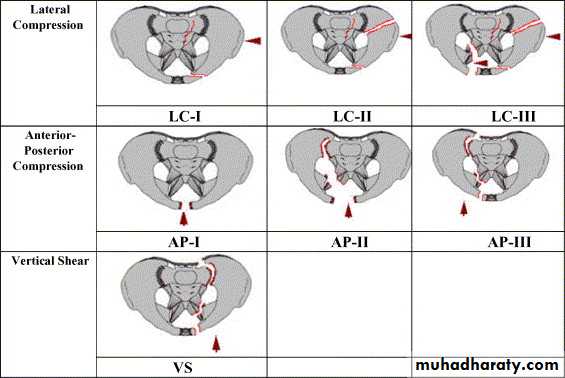
Management
EARLY MANAGEMENtshould follow the ATLS protocol
primary survey ,
secondary survey
and definitive management
Definitive management :
non operative treatment :
Isolated non pelvic ring fractures
minimally displaced fractures
pubic diastasis of less than 2 cm
Treatment by bed rest, and may be combined with lower limb traction for 4–6 weeks
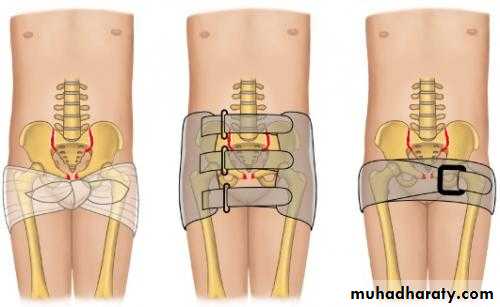
Operative :Plevic binder can be used initially to control the intrapelvic hemorrhage .
External fixation : with pins in both iliac blades connected by an anterior bar.
Internal fixation by attaching a plate across the symphysis or for post sacroiliac fixation.


Complications :
Thromboembolism : deep vein thrombosis or pulmonary embolism. Prophylactic anticoagulants .Neurological injury
Urogenital injuries
Persistent sacroiliac pain