Surgical management of
Fibro-osseous and granulomatous lesionsOral tumors may be classified into those of dental origin and those of non-dental origin. those of dental origin arise from epithelial inclusions remaining within the jaw bones after tooth formation is completed. This occur around the teeth and within suture lines of the developing maxillae and mandible, epithelial tumors may be secreting or non-secreting depending on the presence of secretory epithelium.
Odontogenic tumors:-
1- odantomacalcified odontomas, (simple enamel pearls and cementomas) usually consist of one or more kinds of tooth elements, enamel pearls consist of enamel. odontomas consist of dentine, cementomas are consist of cementum, odontomas may be composite by manifesting two or more tooth tissue elements. These simple tooth tumors arise from some aberration of the tooth germ early in life.
Surgical intervention is instituted at an early age to prevent derangement of the permanent dentition. In later years multiple cementomas and ossifying fibroma appear frequently near the roots of
teeth. The teeth remain vital with absence of subjective symptoms

Surgical intervention is usually unnecessary since they frequently reach stage of inactivity and became calcified within the jaw bones without disturbing function but if they become locally aggressive causing destruction of anatomical surroundings or when these tumors occurring in maxilla which may can invade the sinuses so extensive surgical intervention is necessary.


Complication after removal may include paresthesia of the lower lip and mandible. Hemorrhage form the cavitation's. And secondary infection with breakdown of sutures. recurrence of these benign tumors has not been reported.
Ameloblastoma:-
It is a tumor arising from embryonal cells of developing teeth. Although most forms of this tumor simulate other slow-growing benign tumors some can develop malignant tendencies.Patient may have few subjective symptoms during tumor growth. Enlargement of the tumor may expand the buccal, lingual or palatal bone plates. Tooth may be loosen and pressure symptoms may occur.
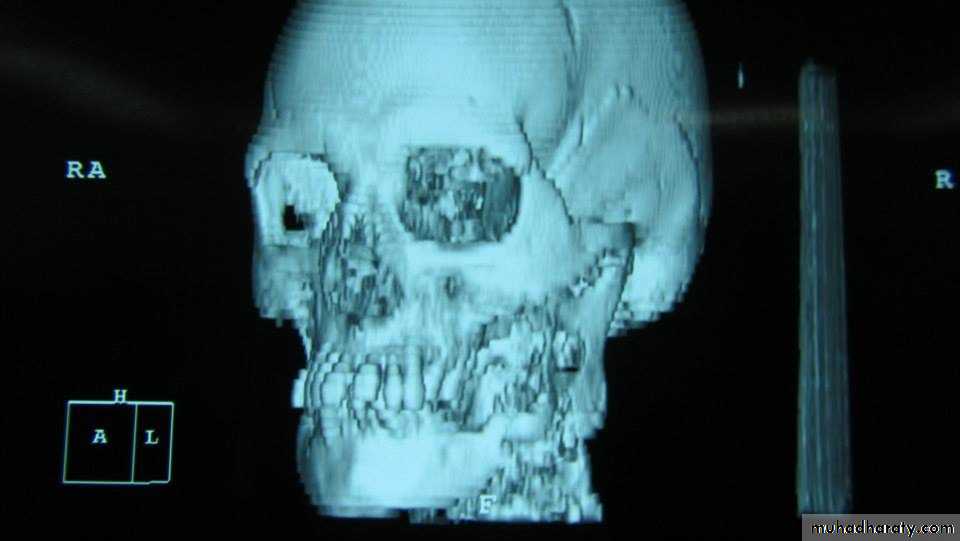
Raioraghical examination may demonstrate unlocular or multilocular types. Unilocular ameloblastomas may be confused with benign cysts. The tumors frequently absorbs the alveolus surrounding ,the roots of teeth and may absorb root ends.
Ameloblastoma grow by extension into adjacent tissues and may perforate the investing bone. A biopsy should precede treatment since
these tumors frequently present with individual characteristics.

Methods of treatment:
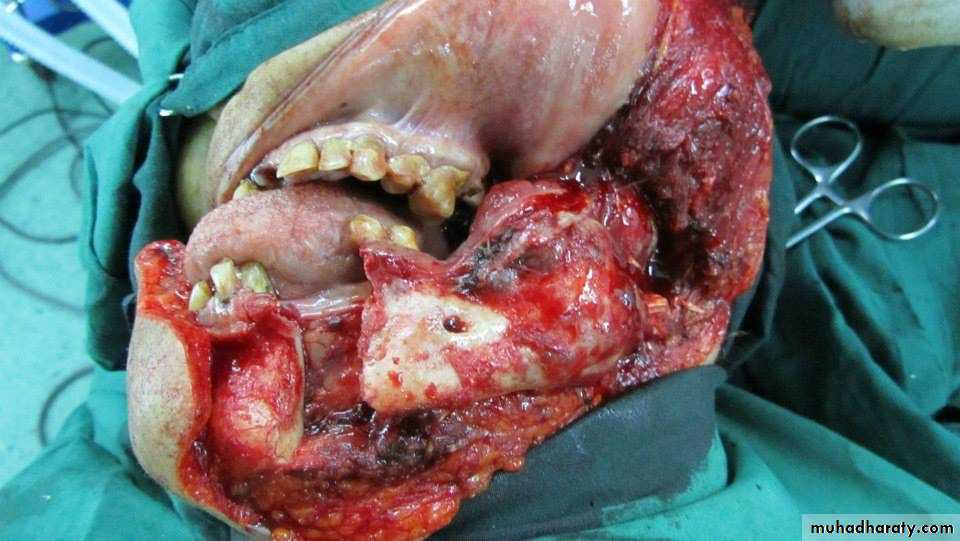
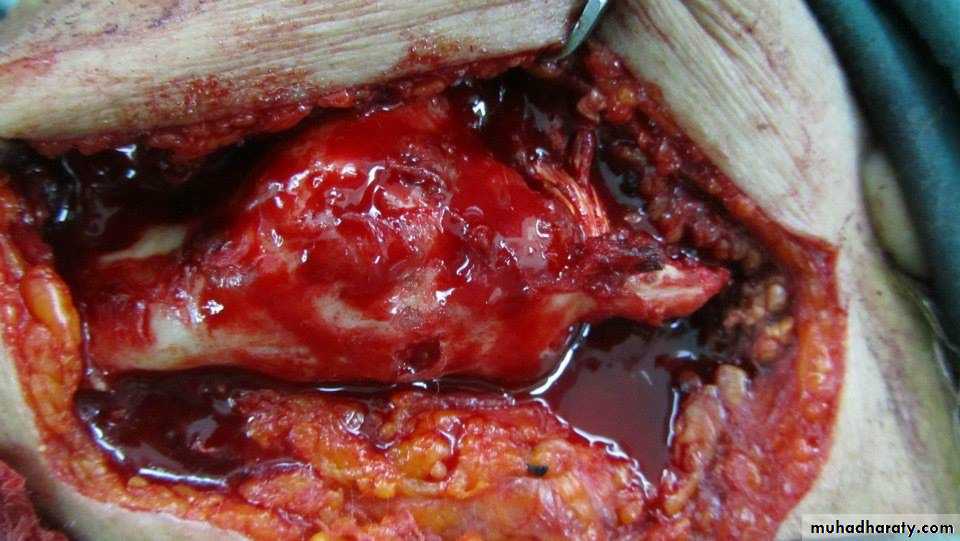
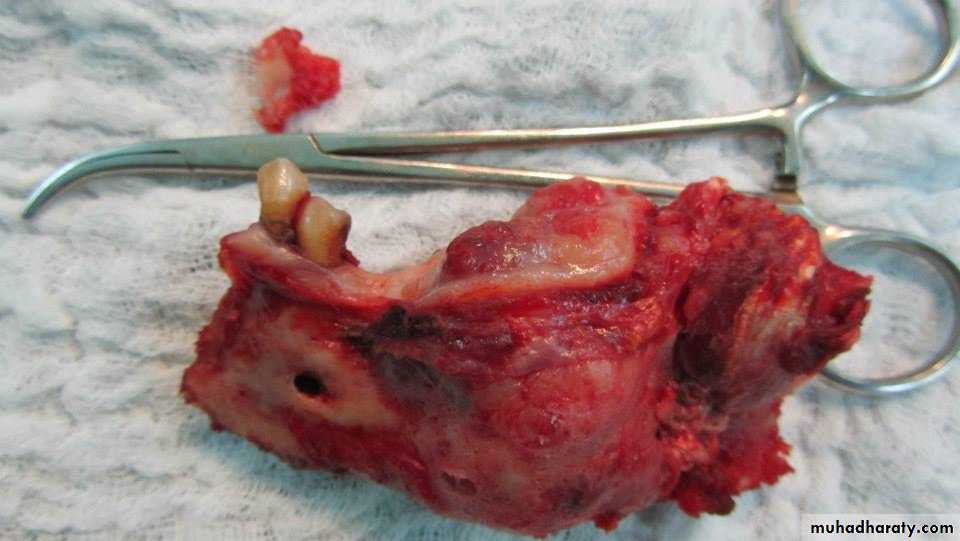
include extirpation, radical resection of the jaw. selective block excision and electro cauterization. Local excision of usually accessible tumor is indicated in the young.Provided, that they agree to regular follow - up and a radical resection when recurrence occurs. Recurrences are not unusual after curettage incomplete surgical treatment may stimulate tumor cell growth.





Ameloblastic fibroma and the ameloblstic adenoma are also tumors related to dental epithelium. These benign neoplasm grow slowly and expand the cortical plates of the jaws these tumors occur most frequently in the second and third decade of life and are painless in the early stages of growth. Surgical treatment is accomplished by complete local excision and cauterization



Osteogenic tumors:
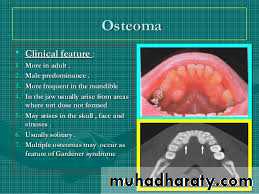
These tumors araise from the jaw bones which include:-1- Osteoma :
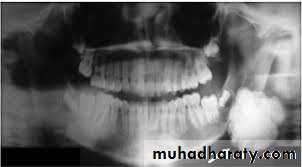
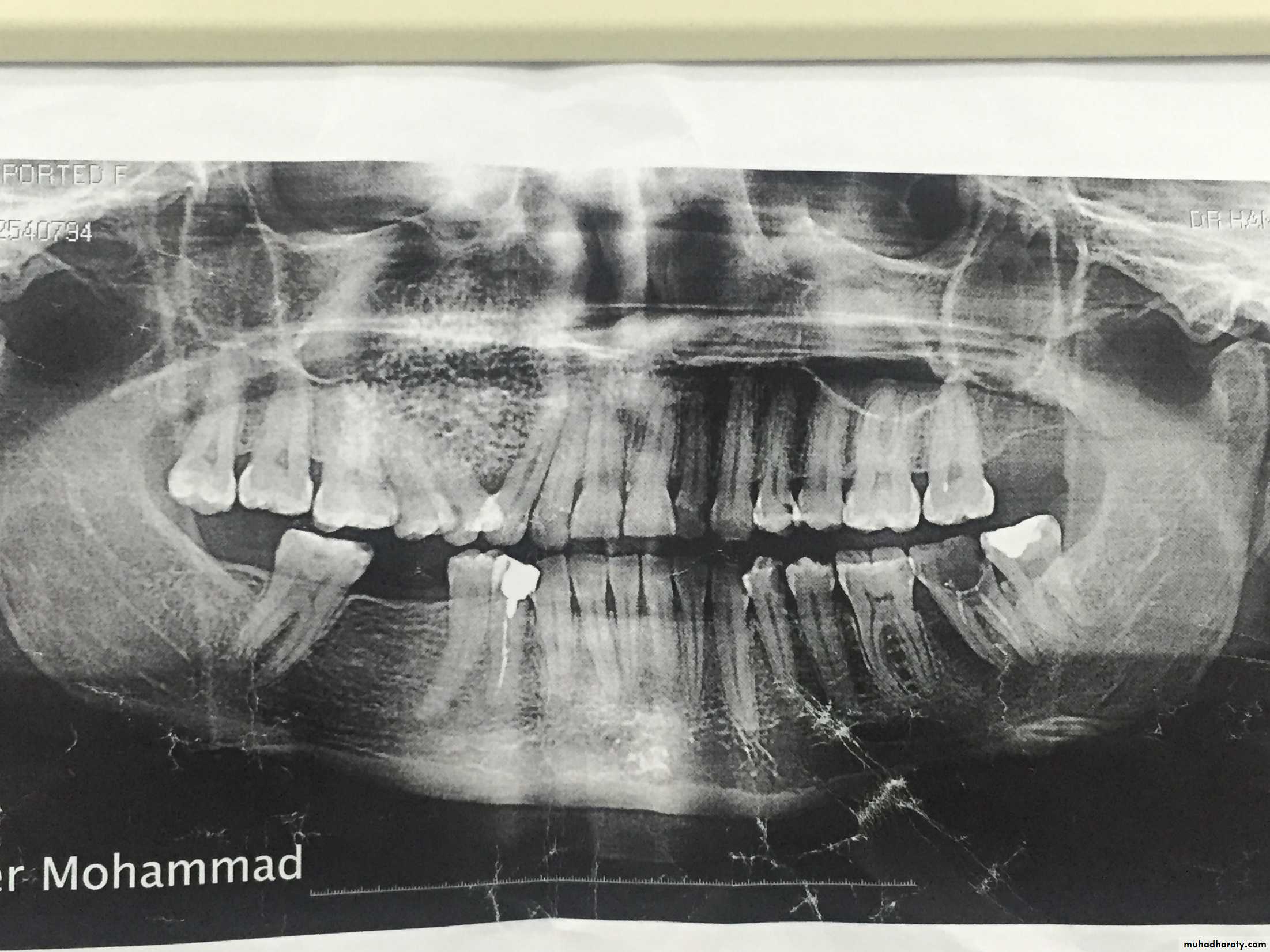
which appears as an areas of circumscribed being bony new growth. osteomas arising from the inner surface of bone cortex. Tumor of this kind consist of dense cortical bone extending into the spongiosa of The jaw. They can be seen in the X-Ray as circumscribed dense bony tumors .which appears as a radiopaque shadow.
Treatment may be unnecessary unless symptom of pain resulting from pressure on nerve fibers are manifested or superficial ulceration occurs in overlying tissues.

2.Fiber osteoma or (ossifying fiberoma ) :
which is a benign slow growing tumor of bone that tends to have its greatest growth in the second decade of life. it is a diffuse poorly differentiated endosteal tumor. replacing the normal spongiosa with fibrous tissues. The enlargement neoplasm may displace teeth and expand cortical plates of the jaw bones.
Fibro-osteoma tends to occur more frequently in women than in man and is seen more often in the maxilla than in the mandible. The active fibro-osteoma or ossifying fibroma frequently recurs when surgical excision dose not include . 10 to 12mm margin or when treatment has been instituted at an early age. radical treatment is less likely to lead to a later recurrence. These tumors do not respond favorably to radiation therapy.



Myxoma and chondroma:
These tumors of embryonic tissue origin developing from immature primitive bone or cartilage cells. the myxoma may simulate a cystic lesion because of its honeycomb appearance in the x-rays, Expansion of the bone cortex occurs with the appearance of mucoid material replacing bone architecture.

The chondroma arises from aberrant fetal cartilage in specific regions of the mandible such as the symphysis and coronid and condyloid process. Myxoma and chondroma may be detected clinically by pain swelling and limitation of motion. these tumors grow slowly they are extripated surgically.


Ewing's tumor :
Is of obscure etiology it is believed to arise from the endothelial lining of the blood or lymph vessels or both. trauma is the common important factor in it's etiology this neoplasm is seen during the first two decades of life subjective symptoms include elevation of bony temperature, pain swelling and interference with jaw function.X-ray reveal expansion of bone cortex with apparent areas of increased density the periosteum is thickened and pushed away from the bone-areas and new bone are formed over areas of bone destruction.
Treatment is primarily by irradiation since the tumor is extremely radiosensitive. this may be followed by radical surgical treatment.
Central giant ell tumor:-
The central giant cell tumor is a benign neoplasm developing in the bone of cartilaginous origin the symphysis and the angles of the mandible and the canin fossa of the maxilla are typical locations . these tumors occur in the second or third decade of life with trauma as the suspected factor. pain and swelling of the mandible with occasional fractures. Occurs whenever the tumor reaches a large size,


X-Rays show no uniform clear-cut picture of central giant cell tumor since the growth appears as multicystic areas with irregularly outlined , fine trabeculations . the teeth are frequently loosened these tumors destroy spongy bone and tend to thin out the cortical bone to a frail shell thus lead to ultimate perforation . the tumor tissue is soft and highly vascular and tends to undergo free hemorrhage when traumatized.

Treatment consist of enculation of the growth after complete exposures the walls and bed of the resulting cavitation's are thoroughly electro cauterized to destroy possible residual areas leading to re growth since this tumor is benign and show slow growing conservative treatment is carried out for ultimate preservation of the bone continuity of the jaw bone.