Fifth Stage
Orthopedics
Dr. Haider – Lecture 8
1
Osteomyelitis
Bone infection
Types ( classification )
According to mechanism of infection
exogenous
open fracture
Surgery
Penetrating injuries
Endogenous ( hematogenous)
bacteremia in blood
According to duration of the disease
Acute ( less than 2 weeks)
Subacute (2-3 weeks )
Chronic ( more than 3 weeks )
Acute hematogenous osteomyelitis
Incidence:
88% occurs in children
(Because the children is more subjected to trauma and the developed hematoma
may acts as a media for bacterial growth)
12% occurs in adults
(especially common in immune compromised adult patients )
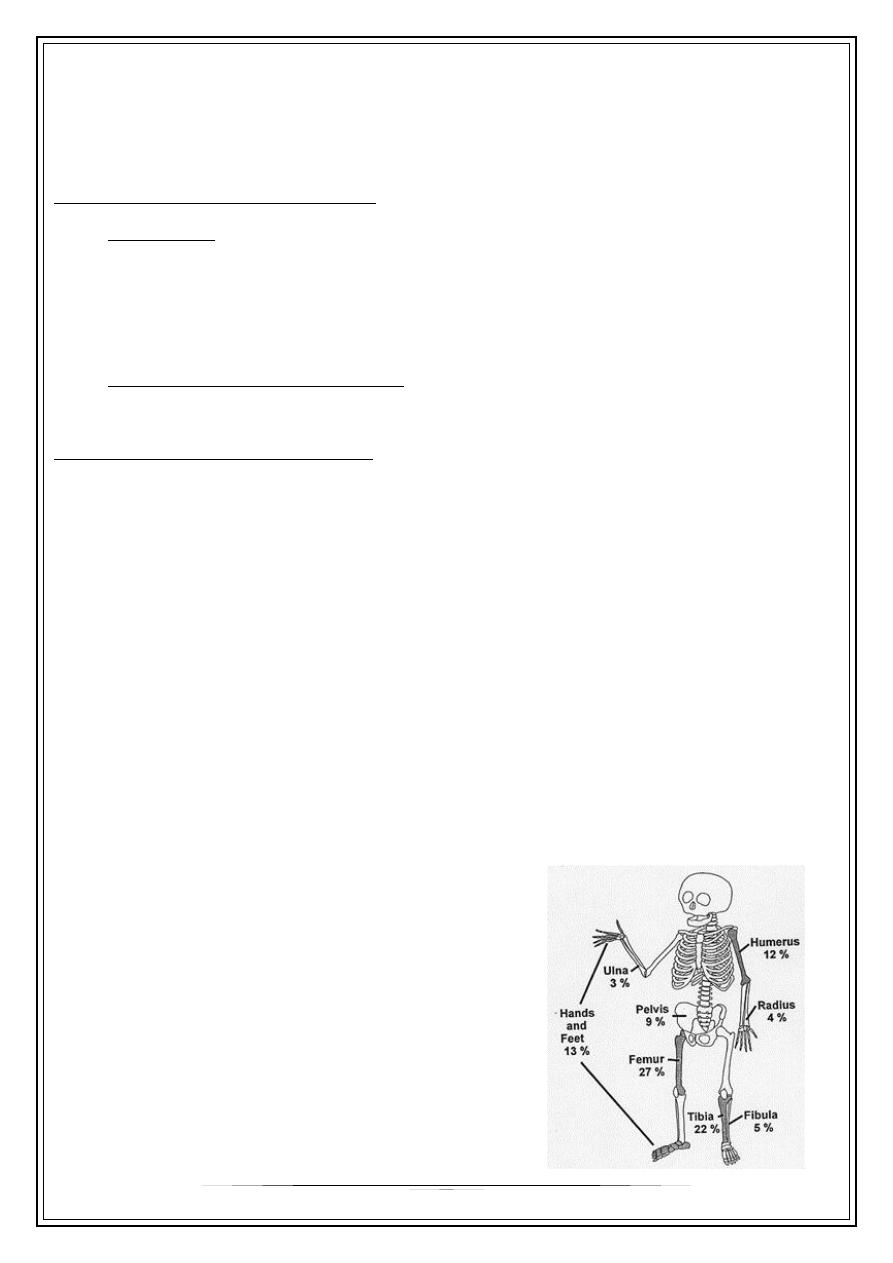
It is common around the knee joint
Proximal tibia and lower femur
50% around knee
2
It is common in the metaphysis of long bones.
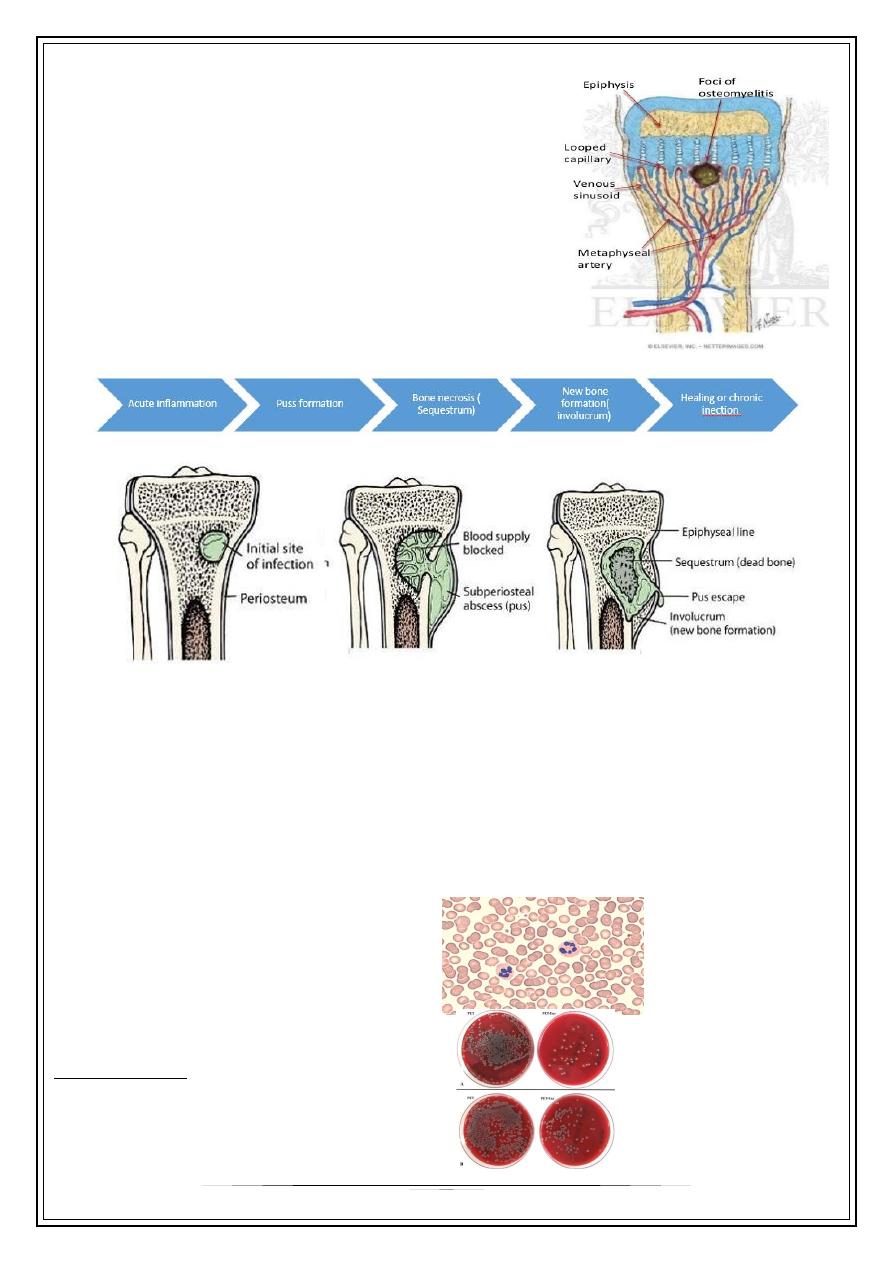
Pathogenesis :
1.Due to vascular stasis. The metaphysial blood vessels
twist back in sharp hairpin loops pattern before it enter
large sinusoidal veins, it gives time for the bacteria to
escape from the vessels to the bone.
2. Relative decrease in phagocytes number in
metaphysis.
Pathology
Clinical features
High grade fever
Swelling( signs of inflammation)
Limitation of movement ( pseudoparalyasis )
Investigation
Increase WBC count (neutrophil series)
Increase ESR
Increase C-reactive protein level
Blood culture
Positive only in 60%
3
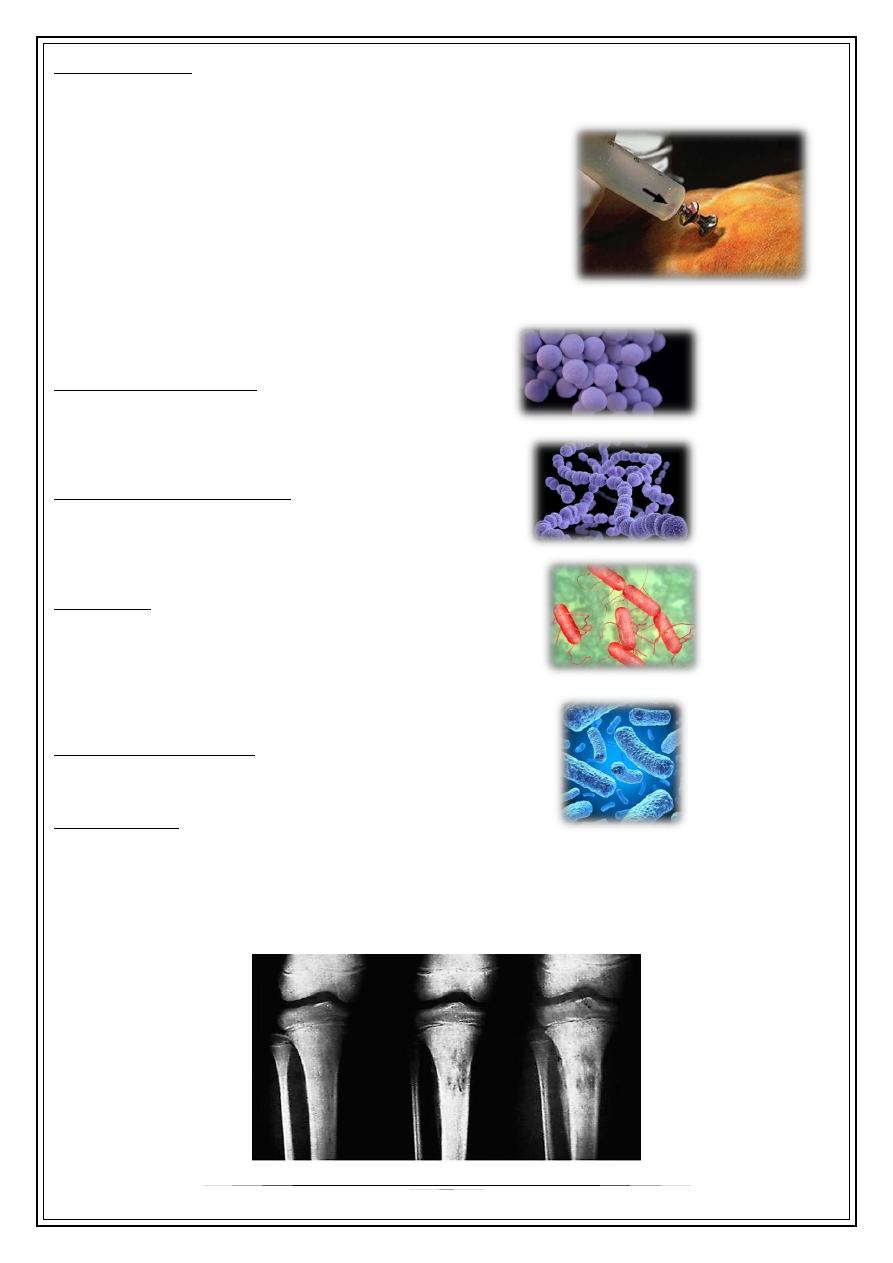
Bone aspirate
If purulent material is aspirated , this will confirm the diagnosis and necessitate surgical
drainage and clearance .
The aspirate should be sent for :
*White cell count
*Gram stain
*Culture and sensitivity
Staphylococcus aureus : 80% of cases
Streptococcus hemolyticus : 10%
Salmonella : common in patients with sickle
cell anemia.
Hemophilus influenzae : common in patients
below 5 years
Radiography
* Early is negative only soft tissue swelling.
* After 2 weeks will shows rarefaction of the bone
* After 3 weeks new bone formation ( periosteal new bone formation )( involucrum)
4
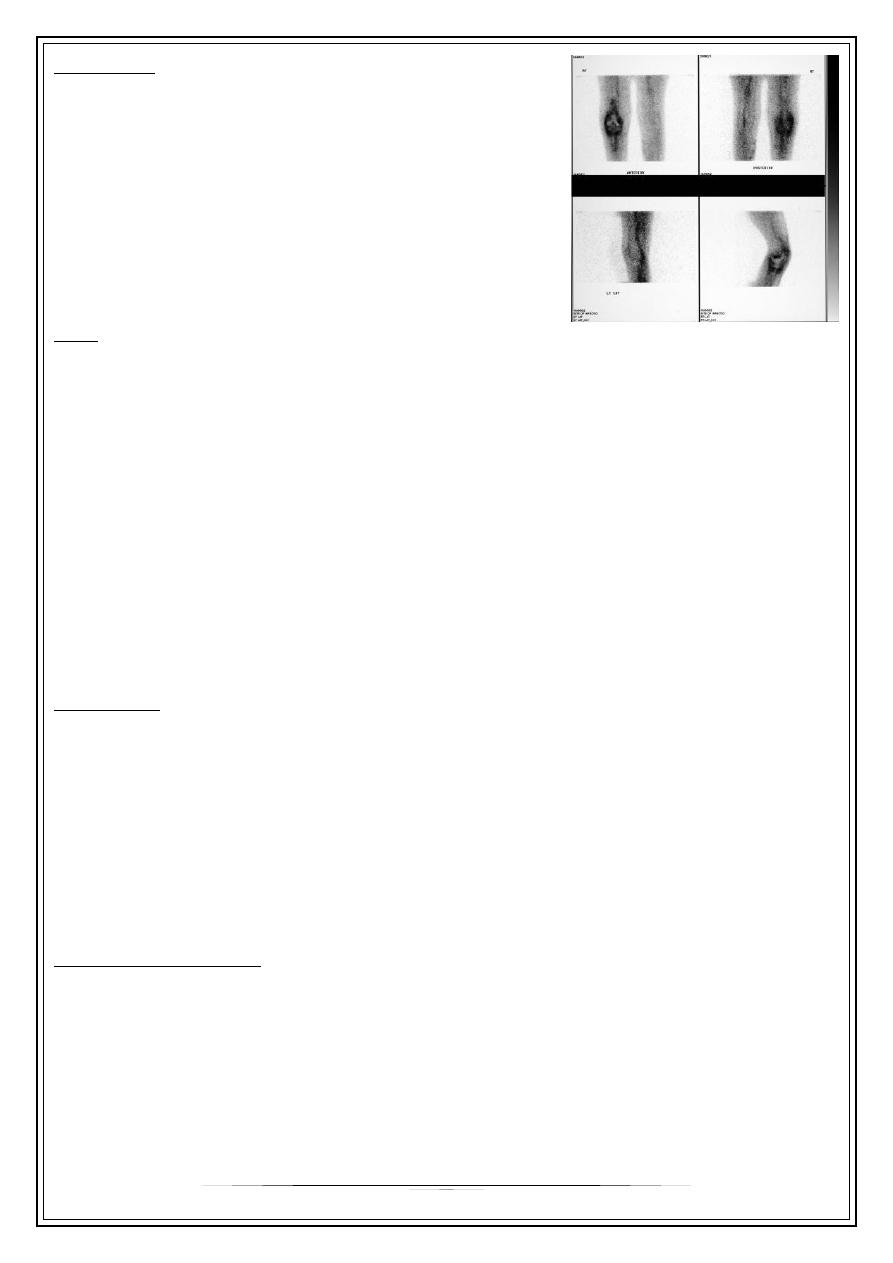
Bone scan
Will shows Increase uptake of radioactive material ( hot
spot).
it is 90% - 95% diagnostic and positive in the first 24-
48 hours.
low specificity
Can not differentiates Between infection and tumor.
MRI: better than x-ray, good in early stages.
Management
'RESTS'
R : rest in bed and splint to alleviate pain and prevent pathological fracture.
E : elevation of the limb.
S : systemic ( fluid and blood transfusion).
T : treatment ( antibiotics).
S : surgery
Antibiotics
* should be started according to the results of bone aspirate or blood culture
* empirical treatment should be started as early as possible according to the best guess
(the most probable organism ) and modified then according to the result of culture and
sensitivity test.
* The principle of treatment is initial 2-4 weeks of intravenous antibiotics , followed by
4-6 weeks of oral antibiotics.
Indication of surgery
1. If there is no improvement after 36 hours from starting the conservative
treatment.
2 . If pus comes out during aspiration.
5
Surgery
Drain any subperiostial pus collection.
If you don’t fined pus: open the bone either by multiple drills
or by making bone window.
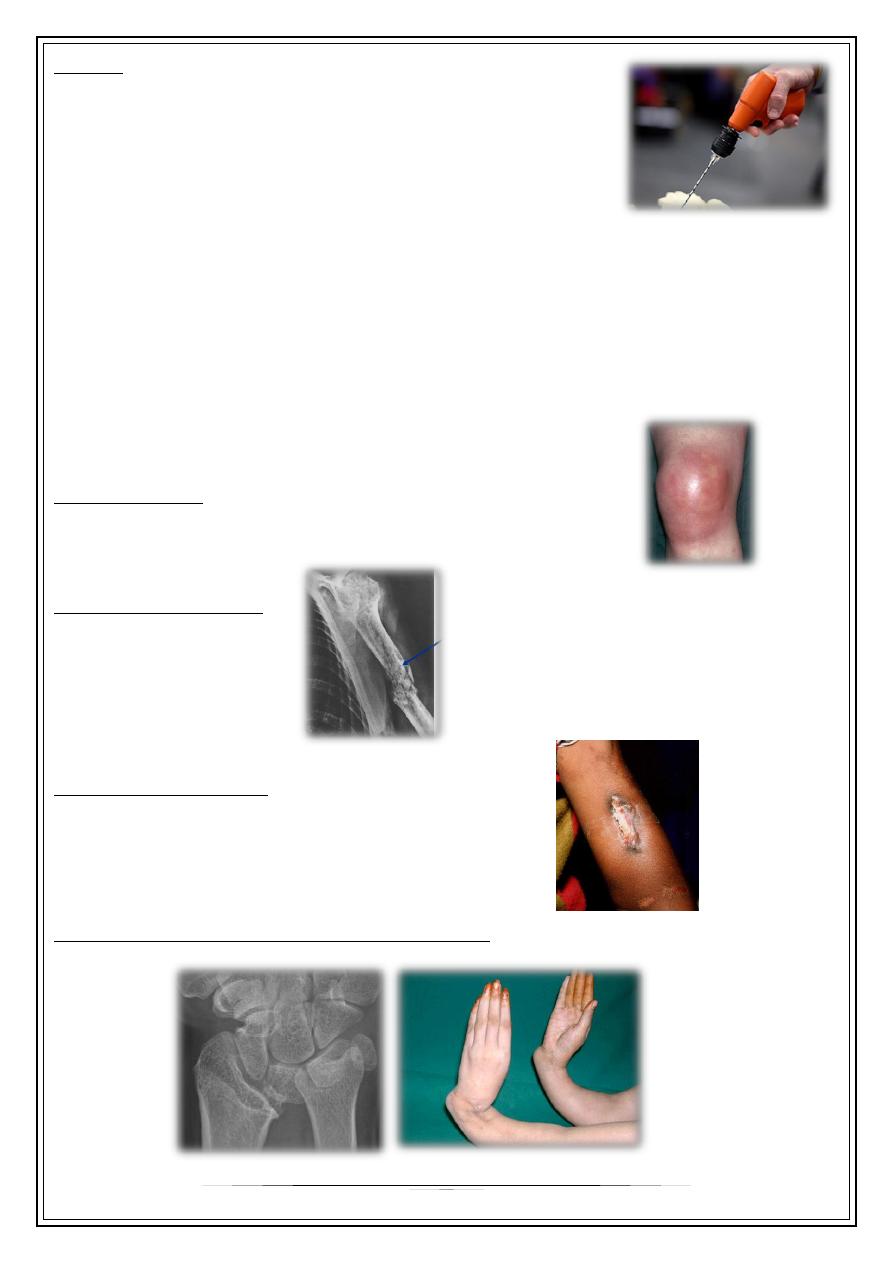
Complications
1. Septic arthritis
2. Chronic osteomyelitis.
3. Pathological fracture.
4. Epiphyseal damage and growth disturbance.
Septic arthritis
especially in intraarticular metaphyses ( sholder , elbow , hip)
Pathological fracture
Chronic osteomyelitis
( persistant discharging sinus and bone sequestra )
Epiphyseal damage and growth disturbance, common in infants and neonates
Thank You,,,