
Furcation
involvment and treatmentFurcation
The term refer to invasion of the furcation areas by the periodontal disease process , the reason for this event is that the progression of periodontal disease not occurs only in vertical direction along the root surface but also in horizontal direction involving the furcation areas found between the roots of multi – rooted teeth.Etiologic Factors
The primary etiologic factor in the development of furcation defects is bacterial plaque and the inflammatory consequences that result from its long-term presence.The extent of attachment loss required to produce a furcation defect is variable and related to local anatomic factors (e.g., root trunk length, root morphology) and local developmental anomalies (e.g., cervical enamel projections [CEPs]) and it also increase with age, and dental caries.
Etiologic Factors
prevalence and severity of furcation involvement increase with age.Dental caries and pulpal death may also affect a tooth with furcation involvement or even the area of the furcation.
Diagnosis of Furcation Defects
Careful probing is required to determine the presence and extent of furcation involvement, the position of the attachment relative to the furca.The Nabors probe may
• be helpful to enter and
• measure difficult to
• access furcal areas.

Local Anatomic Factors
Local factors may affect the rate of plaque deposition or complicate the performance of oral hygiene procedures.• Root Trunk Length
• Root Length
• Root Form
• Interradicular Dimension
• Anatomical Aetiological Factors
Cervical Enamel Projections
• Enamel Pearls
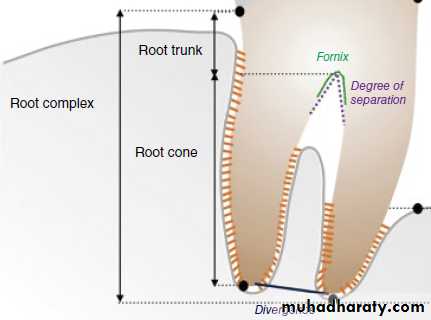
Root Trunk Length
A key factor in both the development and the treatment of furcation involvement.The distance from the cementoenamel junction to the entrance of the furcation can vary extensively.
• teeth with long root trunks may not be appropriate for treatment.
Root Length
Teeth with long root trunks and short roots may have lost a majority of their support by the time that the furcation becomes affected.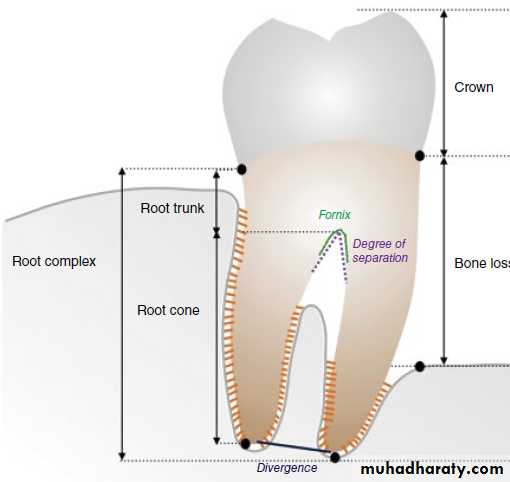
Root Form
The mesial root of most mandibular first and second molars and the mesiofacial root of the maxillary first molar are typically curved to the distal side in the apical third.the distal aspect of this root is usually heavily fluted.
The curvature and fluting may increase the potential for root perforation during endodontic therapy which lead to furcation problem.
Interradicular Dimension
Closely approximated or fused roots can preclude adequate instrumentation during scaling, root planing, and surgery.widely separated
roots present more
treatment options.

Anatomical Aetiological Factors
• The anatomy of the furcation is complex, The presence of bifurcational ridges, a concavity in the dome, and possible accessory canals, Cervical Enamel Projections, Enamel Pearls complicates not only scaling, root planing, and surgical therapy, but also periodontal maintenance.Cervical Enamel Projections
Grade I: The enamel projection extends from the cementoenamel junction of the tooth toward the furcation entrance.Grade II : The enamel projection approaches the entrance to the furcation. It does not enter the furcation, and therefore no horizontal component is present.
Grade III : The enamel projection extends horizontally into the furcation.
Cervical Enamel Projections


Enamel Pearls

Classification
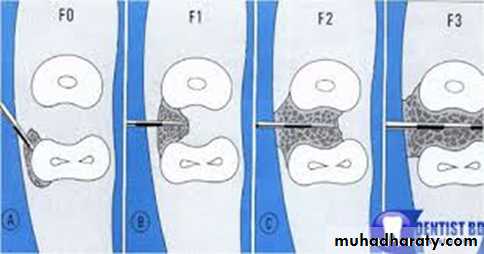
• GRAD I (initial): horizontal loss of periodontal tissue support not exceding 1/3 of the width of the tooth.
• GRAD II (partial): horizontal loss of periodontal tissue support exceeding 1/3 of the width of tooth.
• GRAD III(total): horizontal (through and through) destruction of the periodontal tissue support in the furcation.
Sometimes there is class IV when the furcation is covered by only gingiva.
Classification
Treatment
The objectives of furcation therapy• facilitate maintenance
• prevent further attachment loss
• obliterate the furcation defects as a periodontal maintenance problem.
Treatment
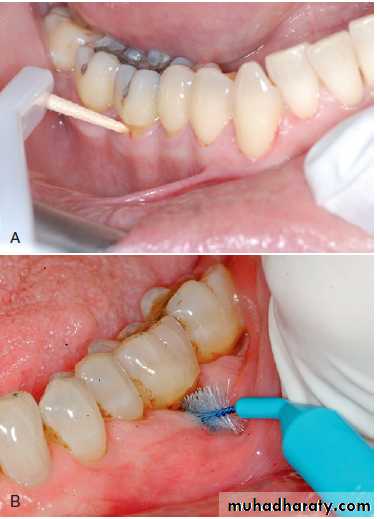
Nonsurgical TherapyOral Hygiene Procedures
Scaling and Root Planing
Surgical Therapy
Osseous Resection
Regeneration
Extraction
Dental Implants
(A) The utilization of a Perio-Aid into the furcation for plaque removal. (B) Proxy brush is used for plaque removal into the furcation lesion.
TREATMENT OF FURCATION INVOLVMENT
degree 1scaling & root planing
• furcationplasty
Degree II
furcationplasty
tunnel prepeation
root resection & hemi section
tooth extraction
DegreeIII
tunnel preperation
root resection & hemi section
tooth extraction
Note: scaling and root planing is made in any degree of furcation involvment not only in degree 1.
FURCATIONPLASTY: is the removal of all soft and hard inflammed and destructed tissues , and establishing a good area for the patient for self performed plaque control , recontouring the tooth by this procedures have some side effects: hypersensivity, root surface caries, more destruction .
FURCATIONPLASTY:
Procedures:1- reflection of mucoperiosteal flap to obtain proper access to the inter radicular area.
2- remove of hard and soft bacterial deposits and inflammatory soft tissues from the furcation area.
3-odontoplasty: removal of tooth substance in furcation area in order to widen the narrow enterance of the furca and to reduce the horizontal depth of the involvment.
4- osteoplasty : re contouring the bony defect in the furcation
5-repositioning and suturing the flap.
TUNNEL PREPERATION:
We remove all the infected tissue making tunnel by performing both odontoplasty and osteoplasty then the tunnel is either left exposed or covered by tissue depending on the patient where he can clean his teeth well or not.ROOT RESECTION & HEMI SECTION”
This is the procedures of choice in case of deep degree II and III furcation involvement , and includes removal of one or more roots from multi-rooted teeth, the tooth must endodontically treated before resection, in the selection of root to be retained following root seperation the following factors should be considred:ROOT RESECTION & HEMI SECTION
1- the amount of supporting structures around the root2-the staibility of individual root
3-the periapical condition of the roots
4-the root and root canal anatomy with respect to endodontic and restorative treatment.
5-the position of various tooth roots in the alveolar process in relation to adjacent and opposing teeth.
6-the O.H of the patient.
7-neighboring teeth should be healthy.
Root Resection
Root resection may be indicated in multirooted teeth with grades II to IV furcation involvement.
may be performed on vital teeth or endodontically treated teeth.
Resection of a root with advanced bone loss. (A) Facial osseous contours. An early grade II furcation is present on the facial aspect of the mandibular first molar, and a class III furcation is present on the mandibular second molar. (B) Resection of the mesial root. The mesial portion of the crown was retained to prevent mesial drift of the distal root during healing. The grade II furcations were treated by osteoplasty. (C) Buccal flaps adapted and sutured. (D) Lingual flaps adapted and sutured. (E) Three-month postoperative view of the buccal aspect of this resection. New restorations were subsequently placed. (F) Three-month postoperative view of the lingual aspect of this resection.
Teeth planned for root resection include
• Teeth that are critically important to the overall dental treatment plan. (teeth serving as abutments for fixed or removable restorations for which loss of the tooth would result in loss of the prosthesis and entail major prosthetic retreatment.• Teeth that have sufficient attachment remaining for function.
• Furcation defects that have been treated successfully with endodontics but now have a vertical root fracture.
• Teeth in patients with good oral hygiene and low activity for caries are suitable for root resection
HEMISECTION
Hemisection is the splitting of a two-rooted tooth into two separate portions, also called (Bicuspidization) or separation as it changes the molar into two separate roots.It is most likely to be performed on mandibular molars with buccal and lingual class II or III furcation involvements.
As with root resection, molars with advanced bone loss in the interproximal and interradicular zones are not good candidates for hemisection.
After sectioning of the teeth, one or both roots can be retained.orthodontic separation of the roots is commonly required to allow restoration with adequate embrasure form
HEMISECTION
The anatomy of the mesial roots of mandibular molars often leads to their extraction.The interradicular dimension between the two roots of a tooth to be hemisected is also important.
Orthodontic separation of the roots with narrow interradicular dimension is often required to allow restoration with adequate embrasure form.
HEMISECTION

(A) Grade III furcation lesion. (B) Hemisection to divide the tooth into mesial and distal portions. (C) Postoperative view of a hemisected mandibular molar with new crowns for both roots.
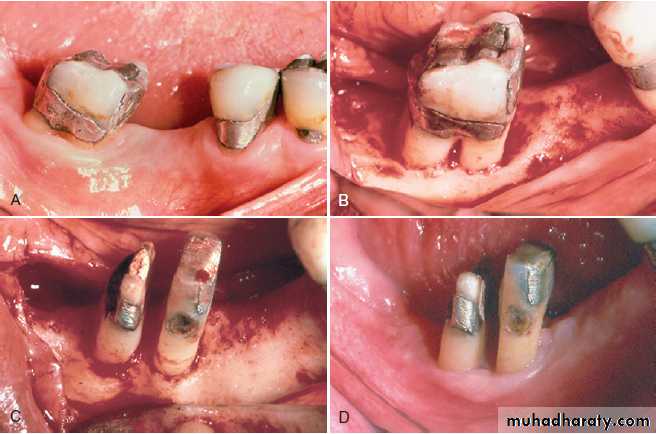
Hemisection and interradicular dimension. (A) Buccal preoperative view of a mandibular right second molar with a deep grade II buccal furcation and root approximation. (B) Buccal view of bony lesions with flaps. Note the mesial and distal one-wall bony defects. The lingual furcation was similarly affected. (C) The molar has been hemisected and partially prepared for temporary crowns. Observe the minimal dimension between the two roots. (D) Buccal view 3 weeks postoperatively. Because the embrasure space is minimal, these roots will be separated with orthodontic therapy to facilitate restoration.