Fifth Stage
E.N.T
Dr. Mushtaq – Lecture 15
1
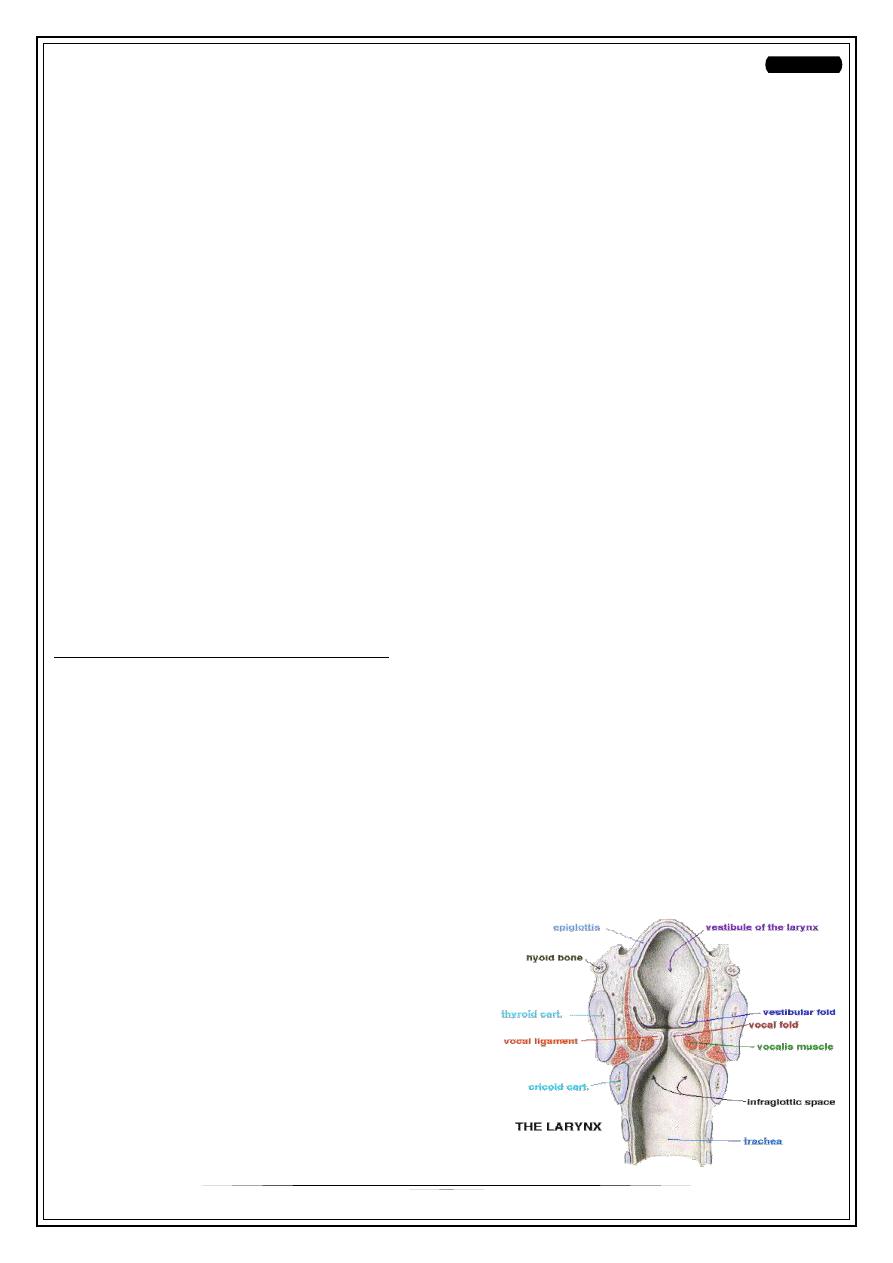
Neoplasms Of The Larynx
Benign neoplasms of the larynx
Epithelial tumours
Single papilloma of the larynx
Multiple papillomas of the larynx
Connective-tissue tumours
Fibroma of the vocal cord
Chondroma
Angioma
Others : lipoma. rhabdomyoma and leiomyoma.
Malignant neoplasms of the larynx
Epithelial tumours
Squamous-cell carcinoma
Others: Adenocarcinoma, Cylindroma,
Basal-cell carcinoma
Connective-tissue tumours
Squamous Cell Carcinoma
5th-6th decades
M/F:3/1,
Smoker/Non:6/1
Pathologically range from highly keratinized to anaplastic types.
Biopsy is always necessary, both for diagnosis and to determine the degree of
differentiation , which assists in the choice of treatment.
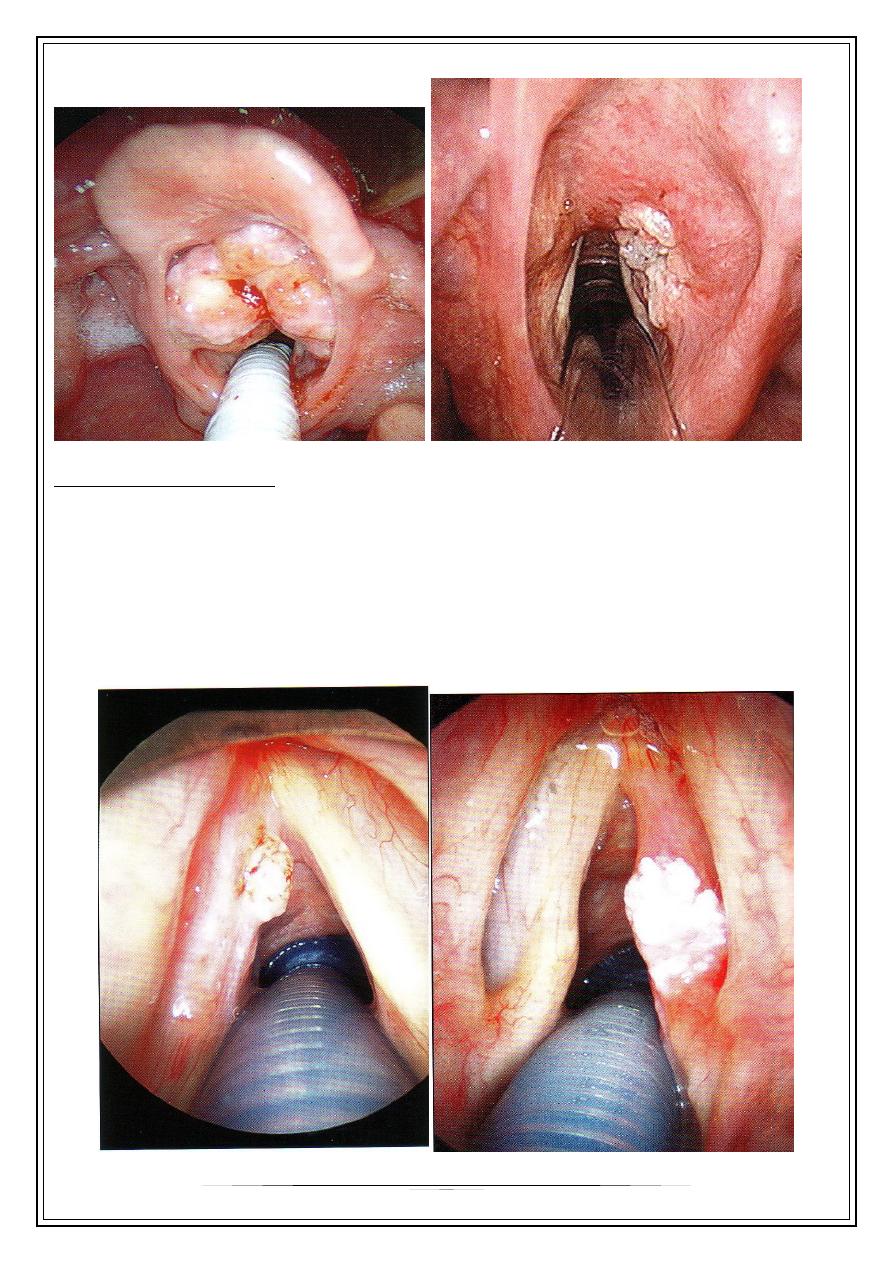
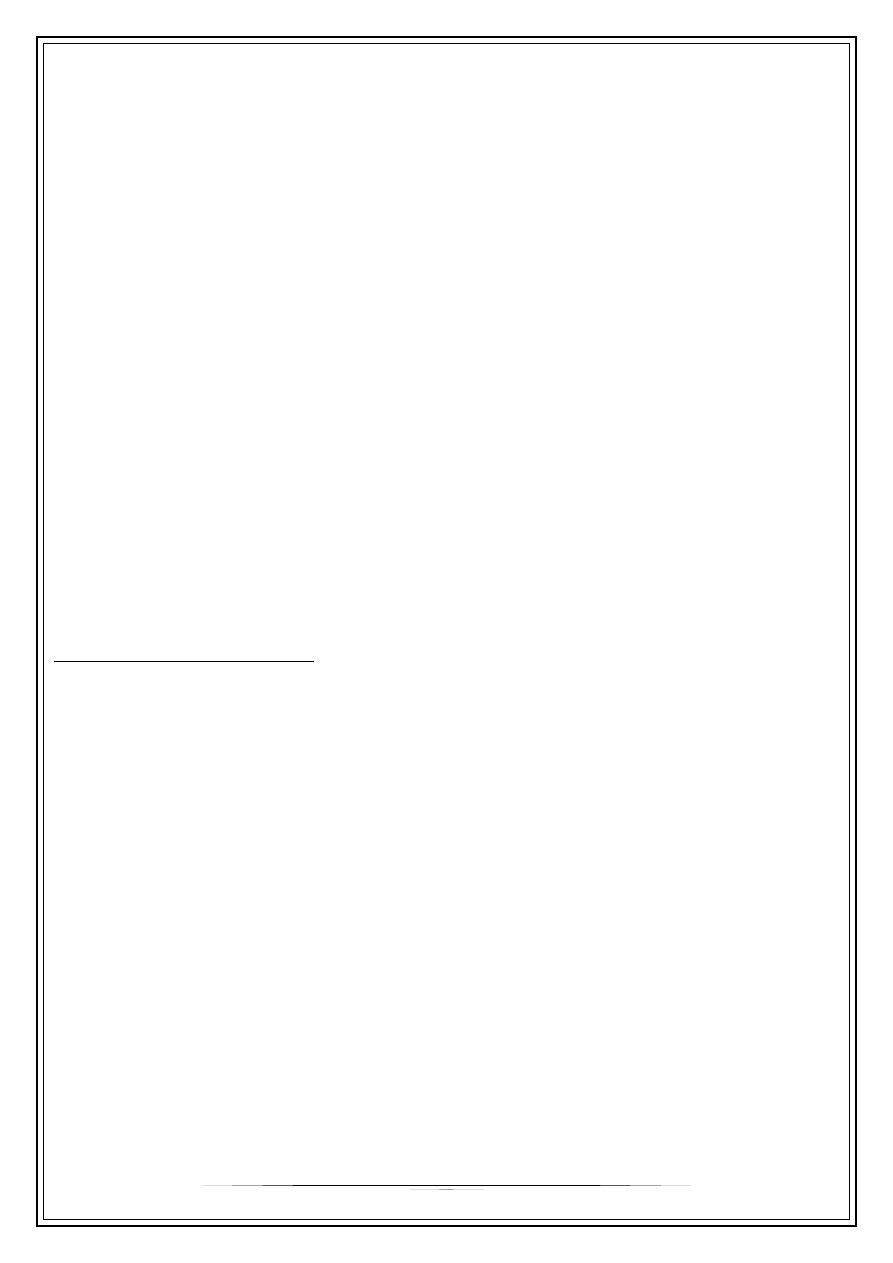
Clinically the growth may be ulcerative or proliferative.
The topographical types
1. Supraglottic carcinoma :
arising in the upper part of the larynx above
the vocal cord. Hoarseness may be relatively
late and is preceded by a sense of discomfort
in the larynx.
2
2. Glottic carcinoma.
Commonest , majority show keratinization.
Carcinoma-in-situ the change is confined to the surface epithelium without
invasion of the supporting connective tissue .
Site : free edge or the flat upper surface of the cord, usually in its central portion
or its anterior half.
C/F: hoarseness
LN. Negative
3
:
Direct spread
Forwards to the anterior commissure ,may spread across the midline to the
anterior end of the opposite cord .
Laterally to pre-epiglottic space.
Backwards to the vocal process, is usual and may occur early.
Upwards into the ventricular band ,is late .
Downwards into the subglottic space on the same side or below the anterior
commissure. It may reach the trachea.
Lymphatic spread: rare < 4%.
Clinical features.
Hoarseness, gradually increasing
Pain (often referred to the ear),
Dyspnoea, and dysphagia are caused by perichondritis as the disease advances.
Indirect laryngoscopy :
* A nodular or generalized swelling of the cord
* White papilliferous excrescence or an ulcer- ated area or a plaque.
* Impaired movement of the affected cord
Metastasis in the lymphatic glands of the neck appears as a hard painless mass
beneath the sternomastoid.
3. Subglottic carcinoma.
The incidence is midway between that of glottic and supraglottic cancer.
Site: is usually the subglottic surface of the cord, but sometimes it is immediately
below the anterior commissure
Direct spread:
•
Upwards to the cord edge. This may be late.
•
Downwards to the trachea.
•
Circumferential spread. The posterior wall is attacked last.
Lymphatic spread. in the lower deep cervical, cricothyroid, paratracheal and
mediastinal lymph nodes.
Clinical features.
Hoarseness results from infiltration of the cord and may therefore be late in
appearing.
Stridor presents as the growth increases in size.
4
Diagnosis
a.History & Clinical ex.
b.Radiography, particularly CT or MR scanning.
c.Endoscopy with biopsy.
Summary of UICC classification
Tumour:
Glottis
TI Limited/mobile.
•
One cord.
•
Both cords.
T2 Extension to supra- or sub- glottis/mobile.
T3 Fixation of cord(s).
T4 Extension beyond the larynx.
Supra- and sub-gloltis
TI Limited/mobile. T2 Extension to glottis/mobile.
T3 Fixation of cord(s). T4 Extension beyond the larynx.
Regional Lymph Nodes:
All regions
NI Homolateral movable.
N2 Contra- or bilateraJ movable.
N3 Fixed.
Treatment
1.Laser :
esp. in Ca.in situ,but today become wider uses
2.Radiotherapy
is indicated in:
•
Anaplastic tumours.
•
Early cordal growths
•
Tumours which only slightly exceed the limitations demanded by partial
laryngectomy.
. In general growths in the posterior half of the larynx and those involving
cartilage are less suitable for radiotherapy .
In some centres radiotherapy combined with hyperbaric oxygen to increase the
cancericidal effects is proving successful with some of the more extensive
growths.
3.Chemotherapy
5
4. Surgery
failure of radiotherapy,
primary curative treatment,
in advanced cases
•
Total laryngectomy.
•
Partial laryngectomy
Management of cervical lymph-node metastases
1. Observation. In cancers limited to one vocal cord. Continued strict and regular
observation, however, is essential if metastases are to be detected early.
2. Presentation. Palpable nodes in the neck at presentation should be treated by
block neck dissection unless the patient is unfit, or in advanced cases.
3. Prophylactic treatment. Radiotherapy of the more advanced cancers of the
larynx should include the lymphatic areas.
4. Treatment of postoperative and post-irradiational lymph-node metastases.
Metastases after radiotherapy or surgery should be treated by block neck
dissection.
Thank you,,,