TYPES OF EXODONTIA
1. Intra-alveolar extraction- also known as “Forceps Extraction”.
- Closed method technique of extraction
with the use of forceps and elevators.
2. Extra-alveolar extraction
– commonly called as “Surgical Extraction”or “ Transalveolar Extraction”.
- Open view technique.
Instrumentation for Basic Oral Surgery other than forceps and elevator
1-Artery forceps
Occasionally, pressure does not stop bleeding from a larger artery or vein. When this occurs, an instrument called a hemostat is useful
• The inner margins of the blades are serrated and on closure, the blades are tightly apposed without any gap in between.
• The blades are held together by means of a catchlock mechanism.
• The blades are conical and blunt. Based on the shape of the blades, artery forceps can be straight or curved.
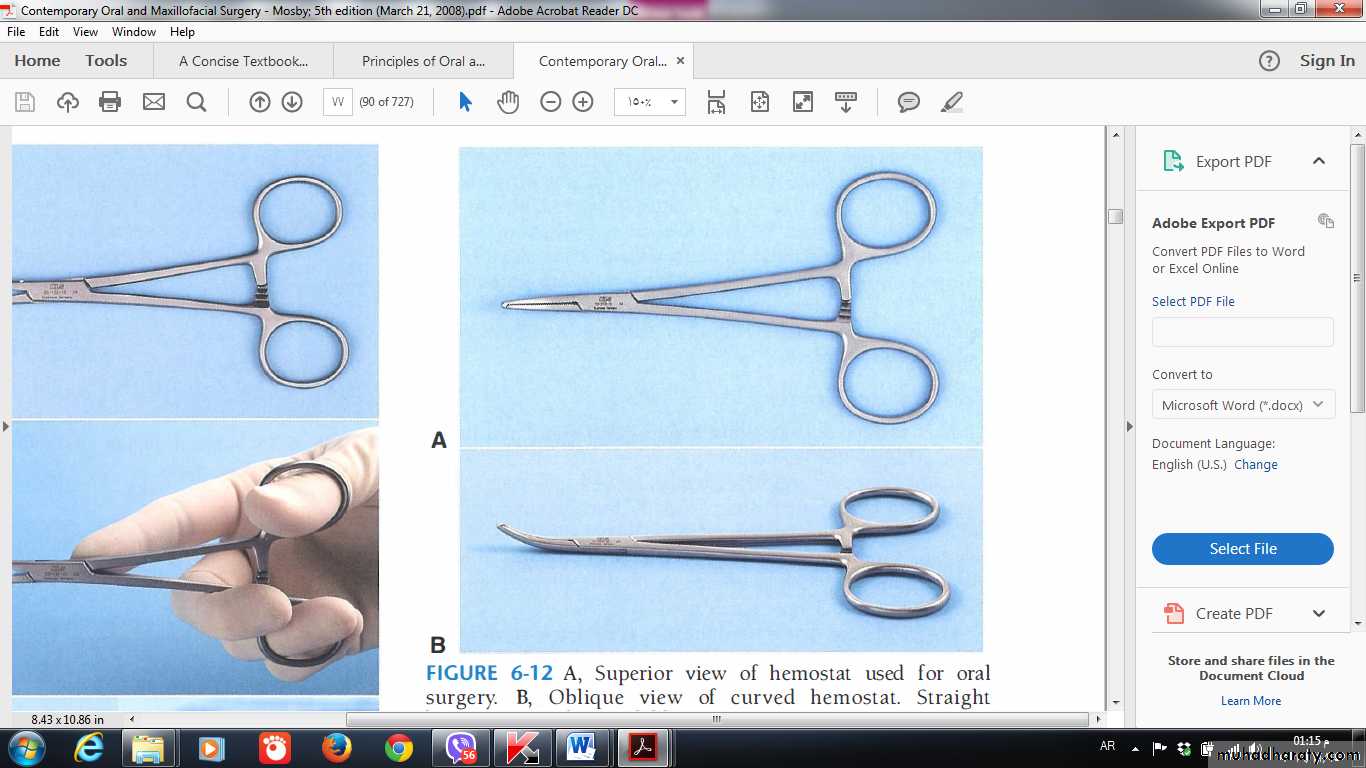
The artery forceps has following types:
Small or Mosquito Forceps (straight and curved)It is very small in size and has relatively pointed tips.
• It is used for holding small bleeding points.
• It is very useful in plastic surgical procedures, e.g. cleft lip, cleft palate.
Medium Artery Forceps
It is the most commonly used type of artery forceps. It can be straight or curved artery forceps
Large Artery Forceps
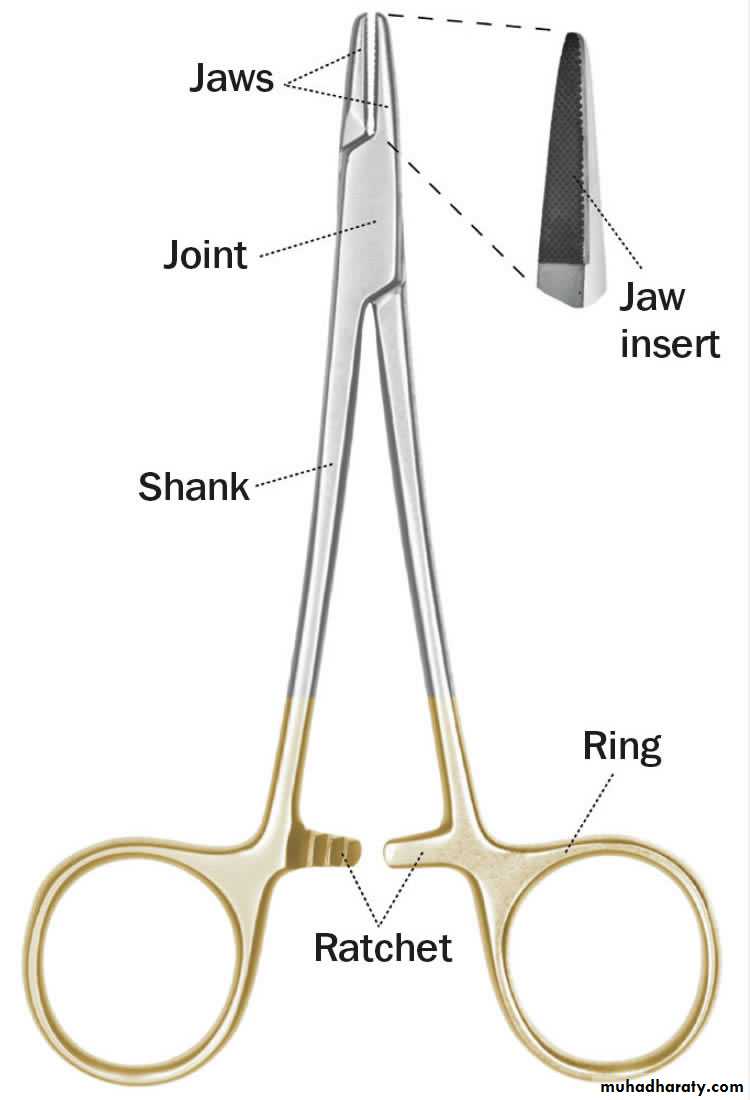
A needle holder
It has following features*The beaks of a needle holder are shorter and stronger than the beaks of a hemostat.
*The face of a beak of the needle holder is crosshatched to permit a positive grasp of the suture needle.
*Longitudinal groove is present on serrated surface
The hemostat has parallel grooves on the face of the beaks, thereby decreasing the control over needle and suture. Therefore the hemostat is a poor instrument for suturing.
2-A needle holder
The needle holder and artery forceps useful in oral surgery to remove granulation tissue from tooth sockets and to pick up small root tips, pieces of calculus, amalgam, fragments, and any other small particles that have dropped into the wound or adjacent areas.
3- scalpel and blade
A scalpel, or lancet, is a small and extremely sharp bladed instrument used for surgery.Scalpel blades are usually made of hardened steel
Scalpels are composed of handle and sharp, disposable blade. Scalpel No. 3 handle with N o . 15 blade is most commonly used
Scalpel blades used in oral surgery include No. 1 0 ,No. 1 1 , No. 1 2 , and No. 1 5 , going from left to right.
It is designed to fit into Bard parker handle
available in numbers and shapes
– No. 10- skin incision
– No. 11- drainage of an abscess: excision
of fistulous tract
– No. 12- incision in palatal aspect: distal
to last molars: incision of marginal
gingivae
– No. 15- incision in accessible area
(commonly used)
When loading scalpel blade, surgeon holds blade in needle holder and handle, with male portion of fitting pointing upward. Surgeon then slides blade into handle until it clicks into place. To remove blade, the surgeon uses needle holder to grasp end of blade next to the handle and lifts it to disengage it from the fitting. Surgeon then gently slides blade off the handle.
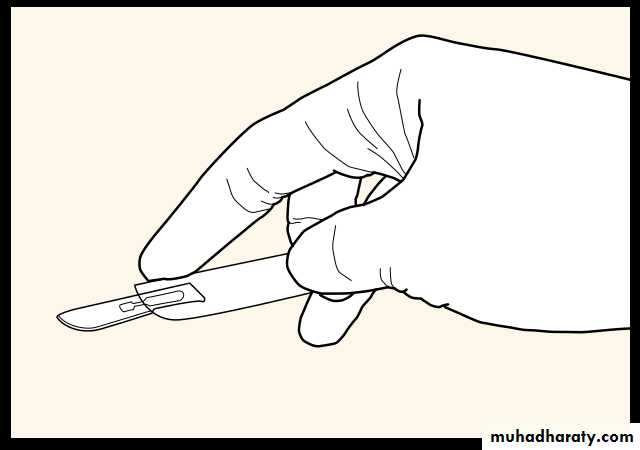

Palmar grip
Pencil grip4-Elevating Mucoperiosteum
When an incision through periosteum is made, ideally the periosteum should be reflected from the underlying cortical bone in a single layer with a periosteal elevator. The instrument that is most commonly used in oral surgery is the N o . 9 Molt periosteal elevator.5-Retractor
The two most popular cheek retractors are• The right angle Austin retractor
2- The broad offset Minnesota retractor .
These retractors can also be used to retract the cheek and a mucoperiosteal flap simultaneously.
6-Grasping Soft Tissue
• A-Adson forceps: - These are delicate forceps with or without small teeth at the tips, which can be used to hold tissue gently and thereby stabilize it.B-Allis tissue forceps
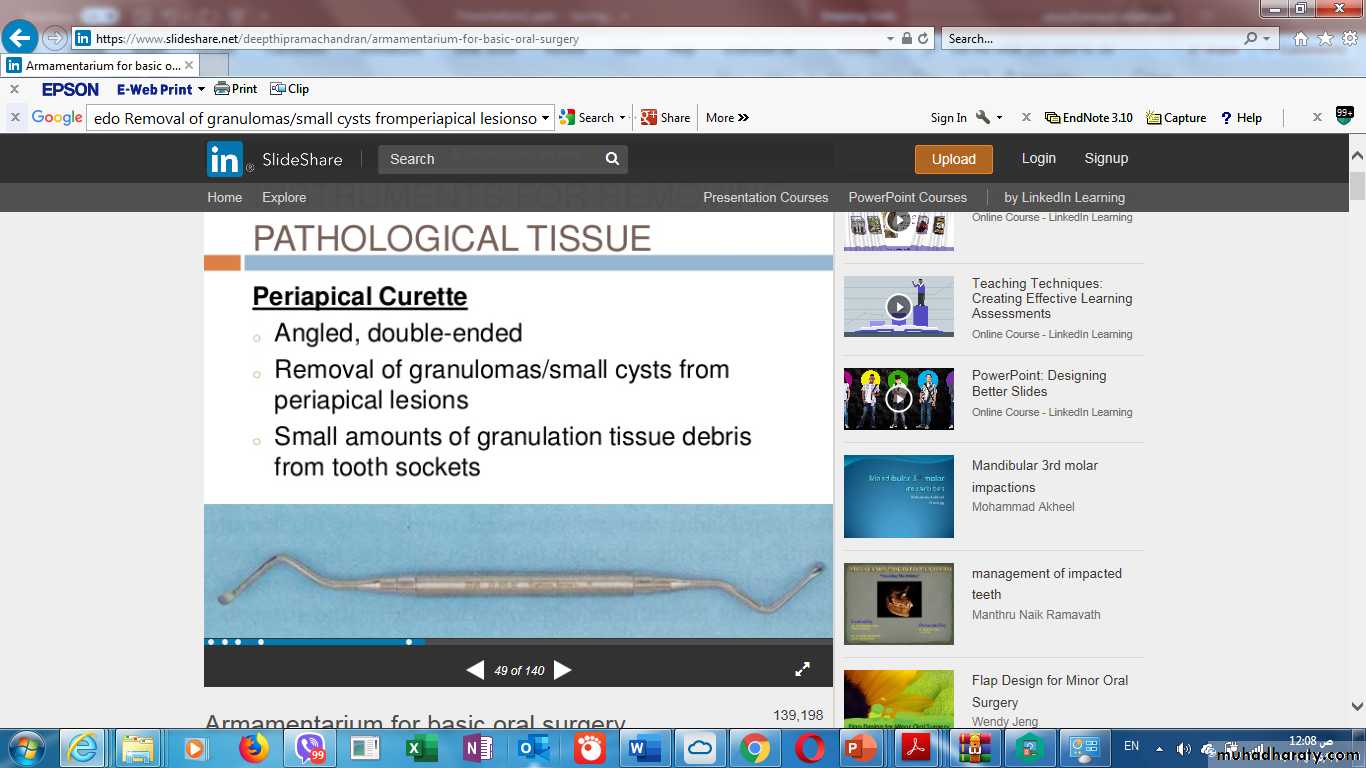
some types of surgery, especially when removing larger amounts of tissue or doing biopsies, forceps with locking handles and teeth that will grip the tissue firmly are necessary. In this situation the Allis tissue forceps are used.Periapical Curette
Angled, double-ended for Removal of granulomas/small cysts from periapical lesions o Small amounts of granulation tissue debris from tooth sockets
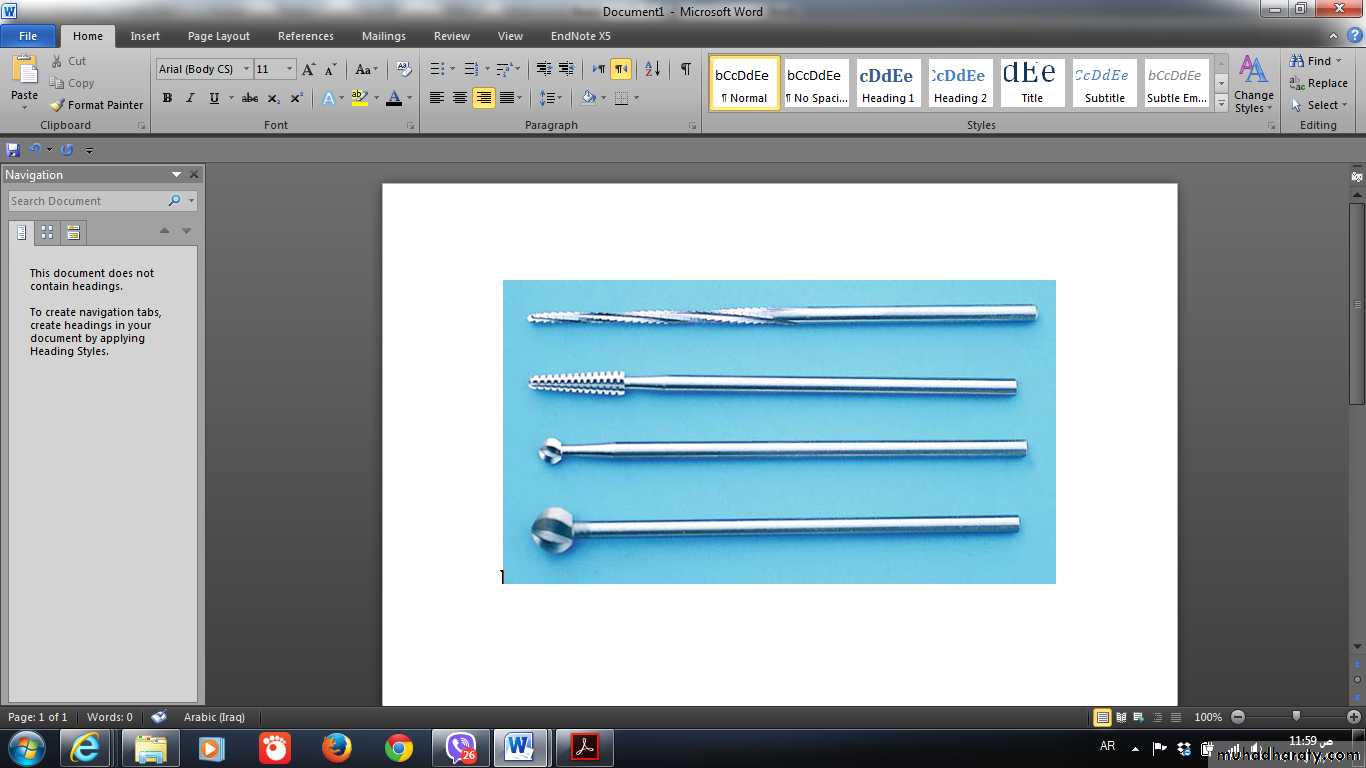
7-Removing bone instrument
A- RongeursThe instrument commonly used for removing bone in dentoalveolar surgery is the rongeur forceps. This instrument has sharp blades that are squeezed together by the handles, cutting or pinching through the bone. The surgeon should not use the rongeurs to remove large amounts of bone in single bites. Rather, smaller amounts of bone should be removed in multiple bites.
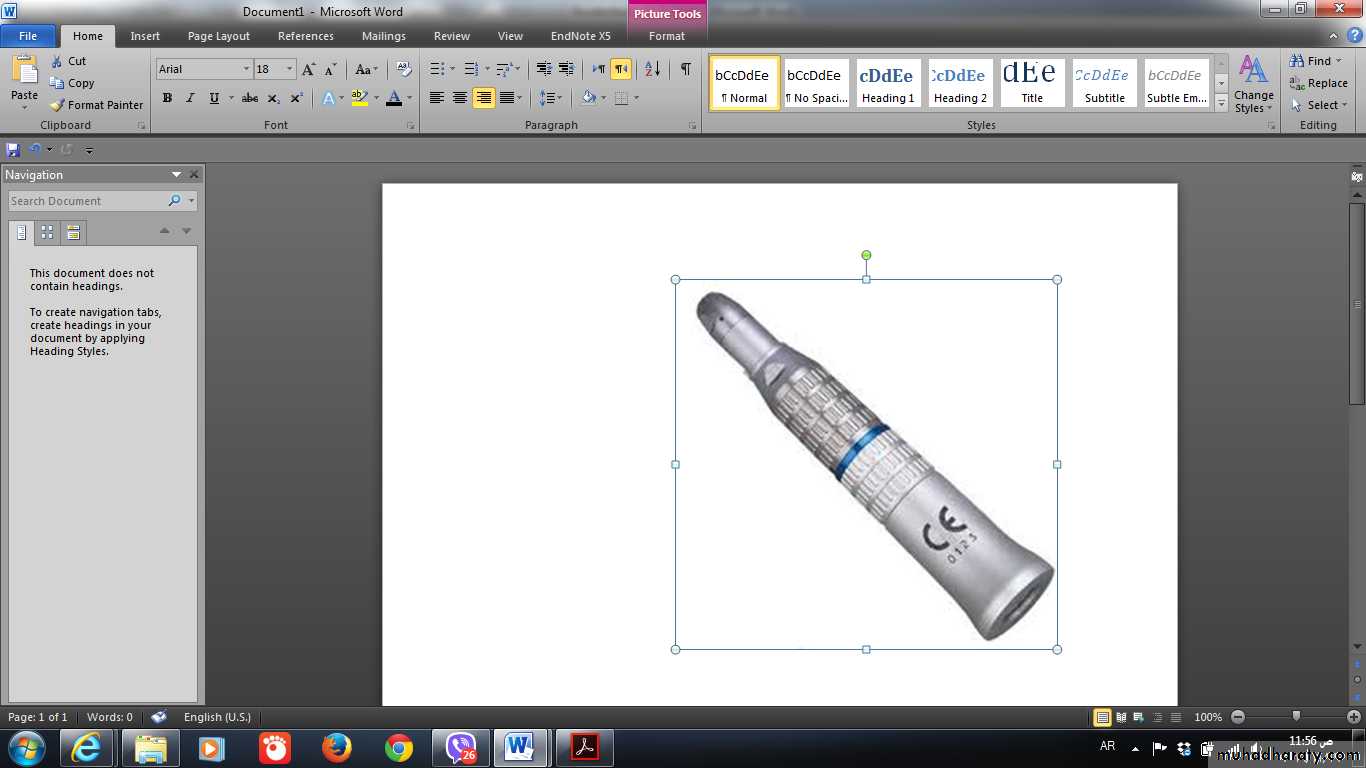
This is the technique that most surgeons use when removing bone for surgical removal of teeth. High-speed, high torque handpieces with sharp carbide burs remove cortical bone efficiently. The handpiece must not exhaust air into the operative field, making it unwise to use typical high-speed turbine drills for routine restorative dentistry. The reason is that the air exhausted into the wound may be forced into deeper tissue planes and produce tissue emphysema, a dangerous occurrence.
B-Bur and Hand piece
• C-Mallet and Chisel
Occasionally, bone removal is performed using a mallet and chiselD-Bone File
Final smoothing of bone before suturing a mucoperiosteal flap back into position is usually performed with a small bone file.The bone file cannot be used efficiently for removal of large amounts of bone; therefore, it is used only for final smoothingScissors
It is used for placing sutures . The scissors are held in the same way as the needle holder.
Soft tissue scissors are of two designs: Iris scissors(top) are small, sharp-pointed scissors. Metzenbaum scissors(bottom) are longer, delicate scissors. Metzenbaum scissors areavailable as either sharp tipped (shown here) or blunt-tipped.
THE TRANSALVEOLAR APPROACH


INDICATIONS OF THE TRANSALVEOLAR APPROACH
.
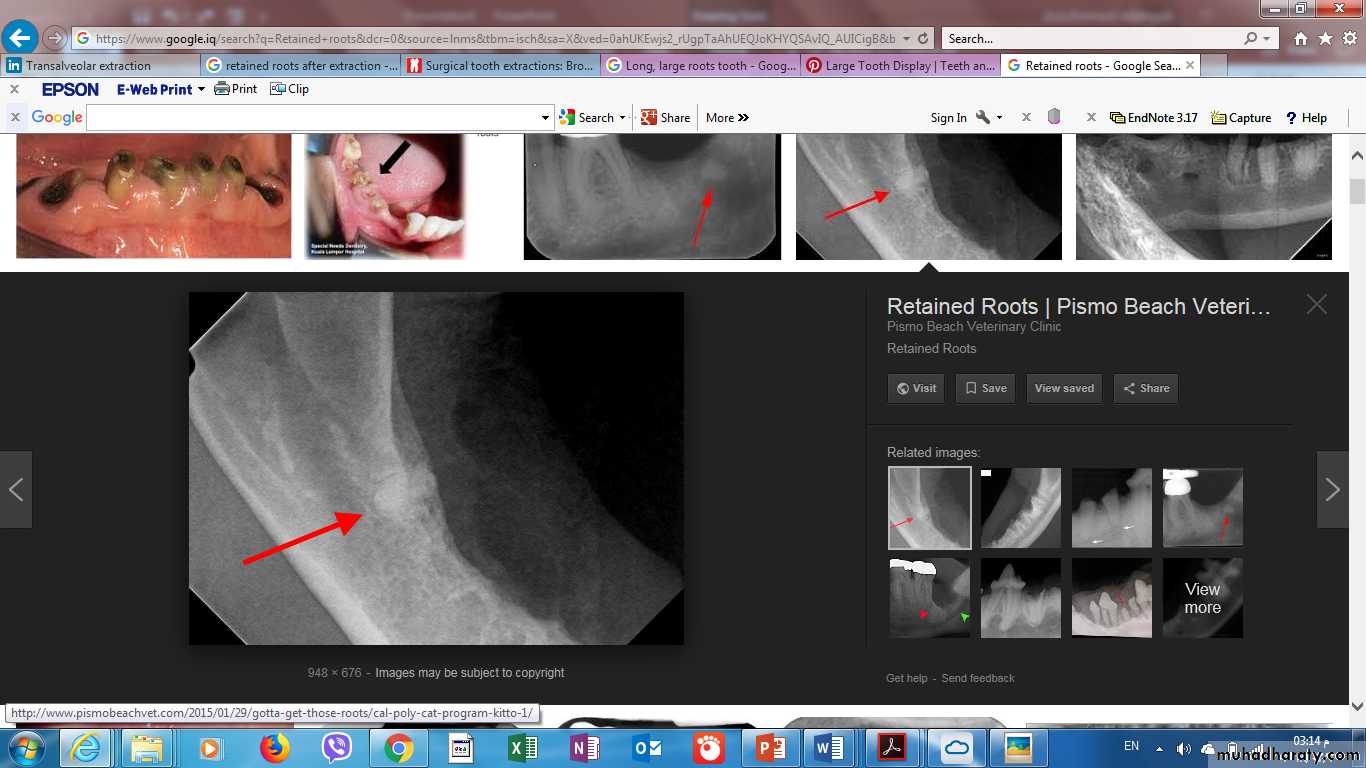
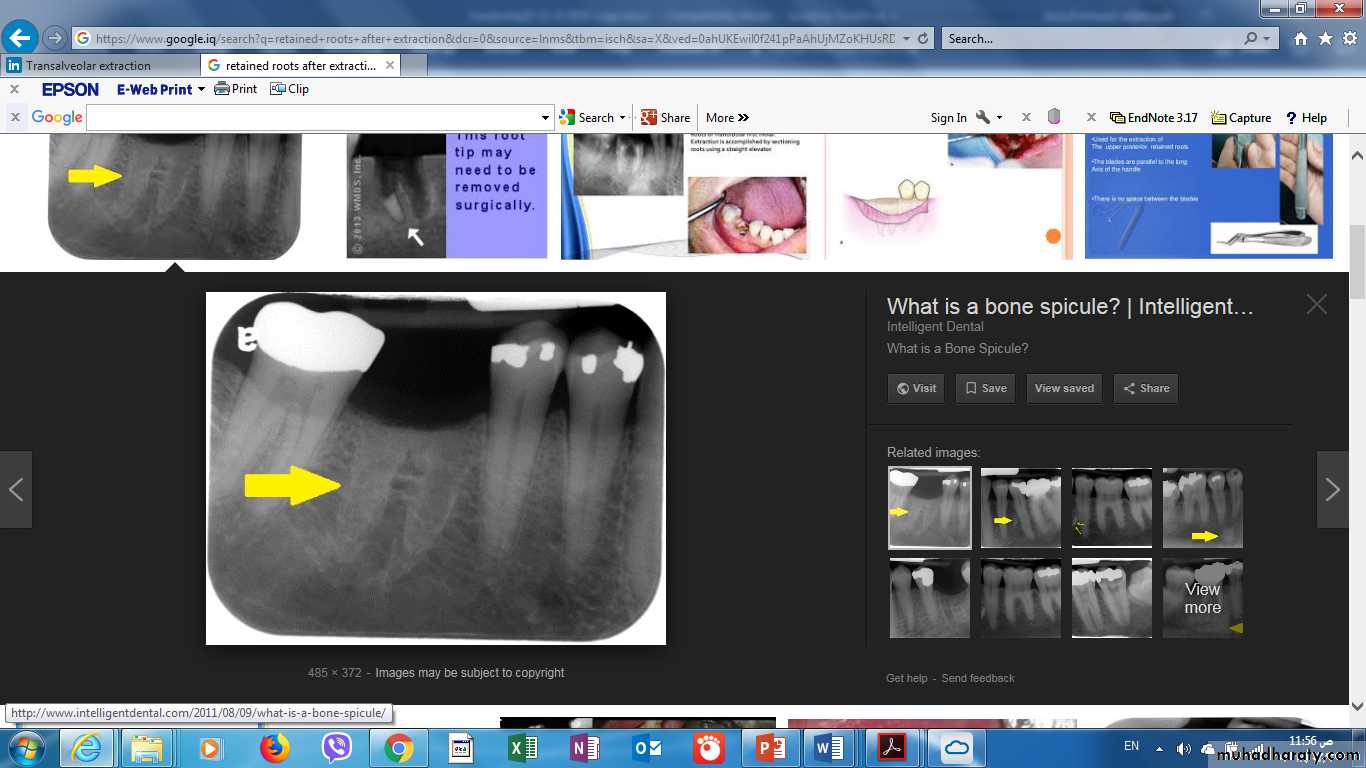
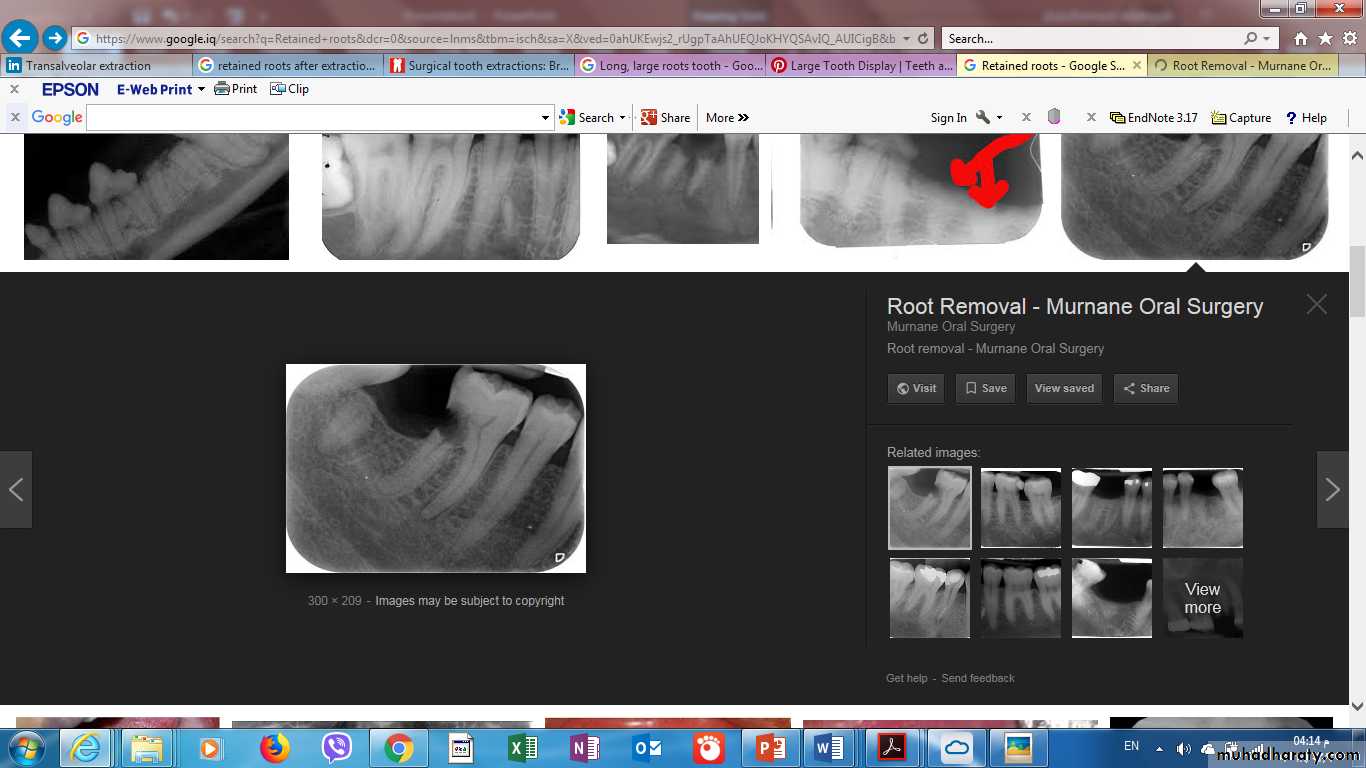
1-Retained roots, which can’t be grasped by the root forceps.
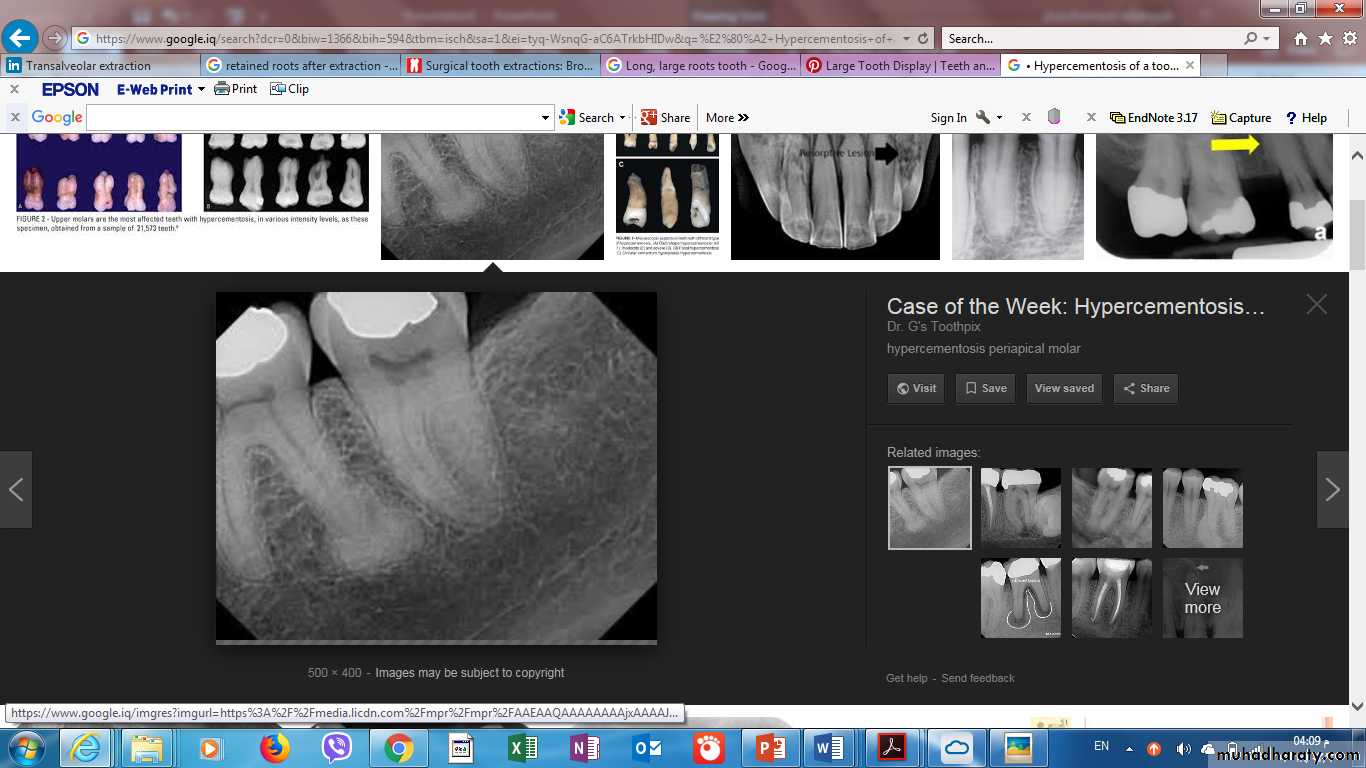
2• Hypercementosis of a tooth.
3.Broken teeth
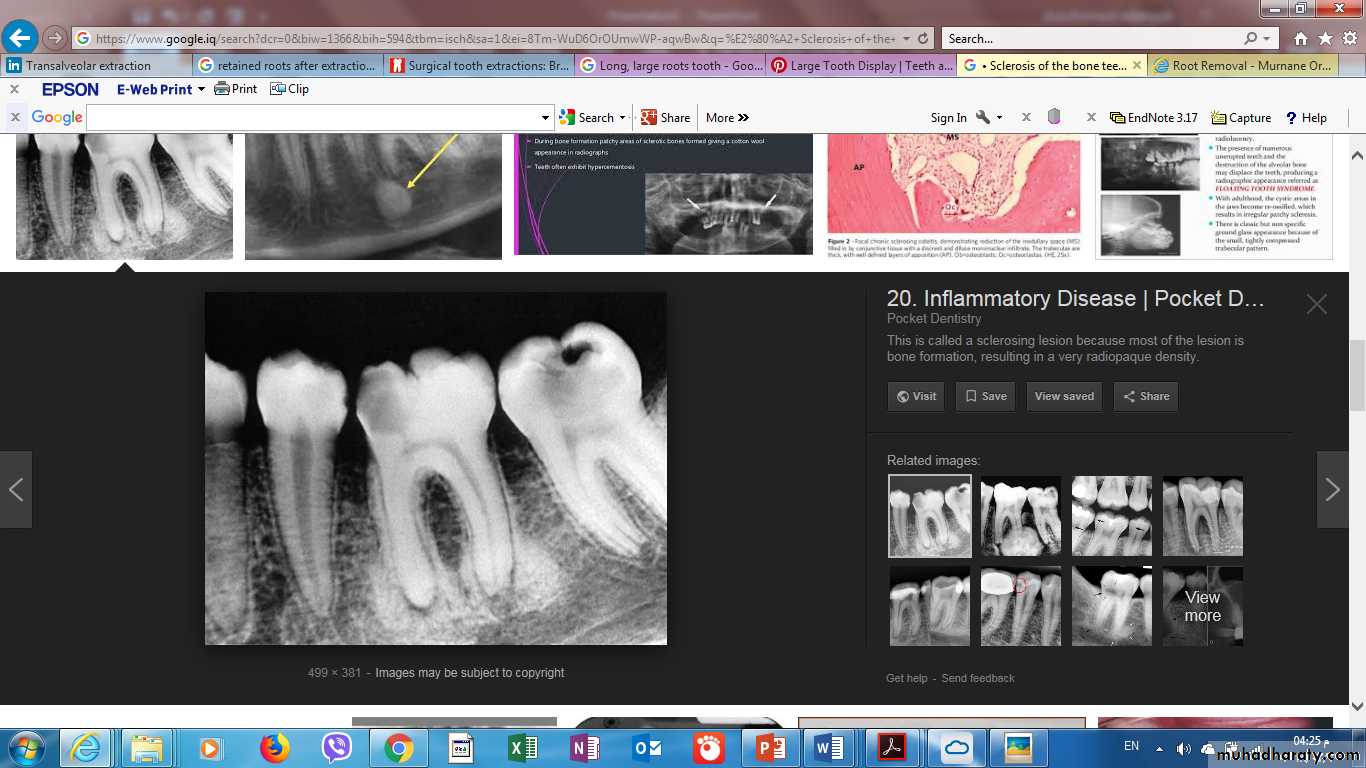
4.Sclerosis of the bone

5.Teeth associated with pathology –
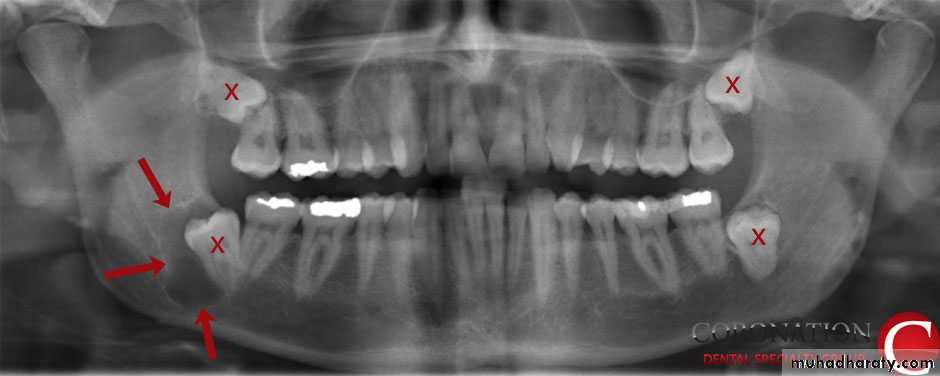
periapical granuloma, cyst, tumor etc6• Impacted teeth, embedded teeth
7.Any tooth, which offers a lot of resistance in forceps extraction.

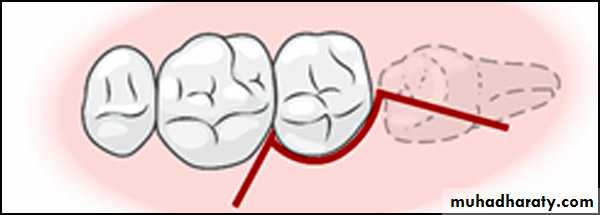
8.Curved roots - Multi-rooted teeth (like molars) that have especially curved, hooked or crooked roots can be stubborn extractions. Beyond just being difficult, the act of pulling these teeth may require the use of excessive forces that may result in bone or tooth breakage
Advantages
• Gives good visibility.• Easy Access.
• Prevents laceration of gingiva.
• Prevents traumatization of bone &fracture of tooth.
• Reduce post operative complications.
Procedure
• Local Anaesthesia
• Incisions and flap design
• Bone removal
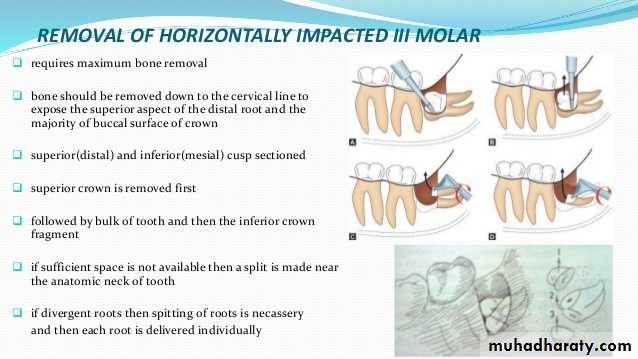
• Sectioning of teeth
• Elevation of the tooth
• Smoothening of sharp edges of bone
• Debridement of socket
• Suturing of the flap
Incisions and flap design
Incision is defined as a cut or wound intentionally made by an operator in the skin or the mucosa using a sharp instrument such as a surgical blade so that the underlying structures can be exposed adequately for surgical access.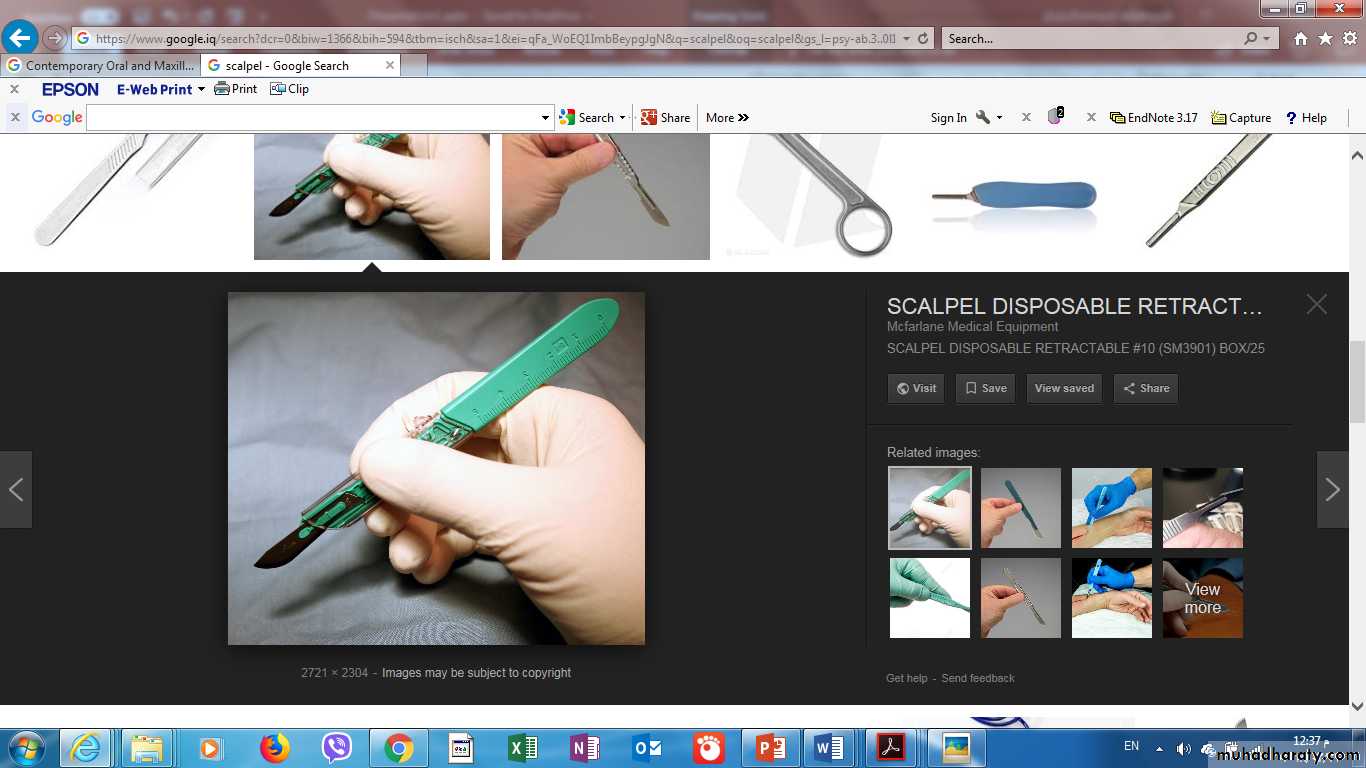
The term flap, as used, indicates a section of soft tissue that
(1) is outlined by a surgical incision,(2) carries its own blood supply,
(3) allows surgical access to underlying tissues,
(4) can be replaced in the original position,
(5) maintained with sutures.
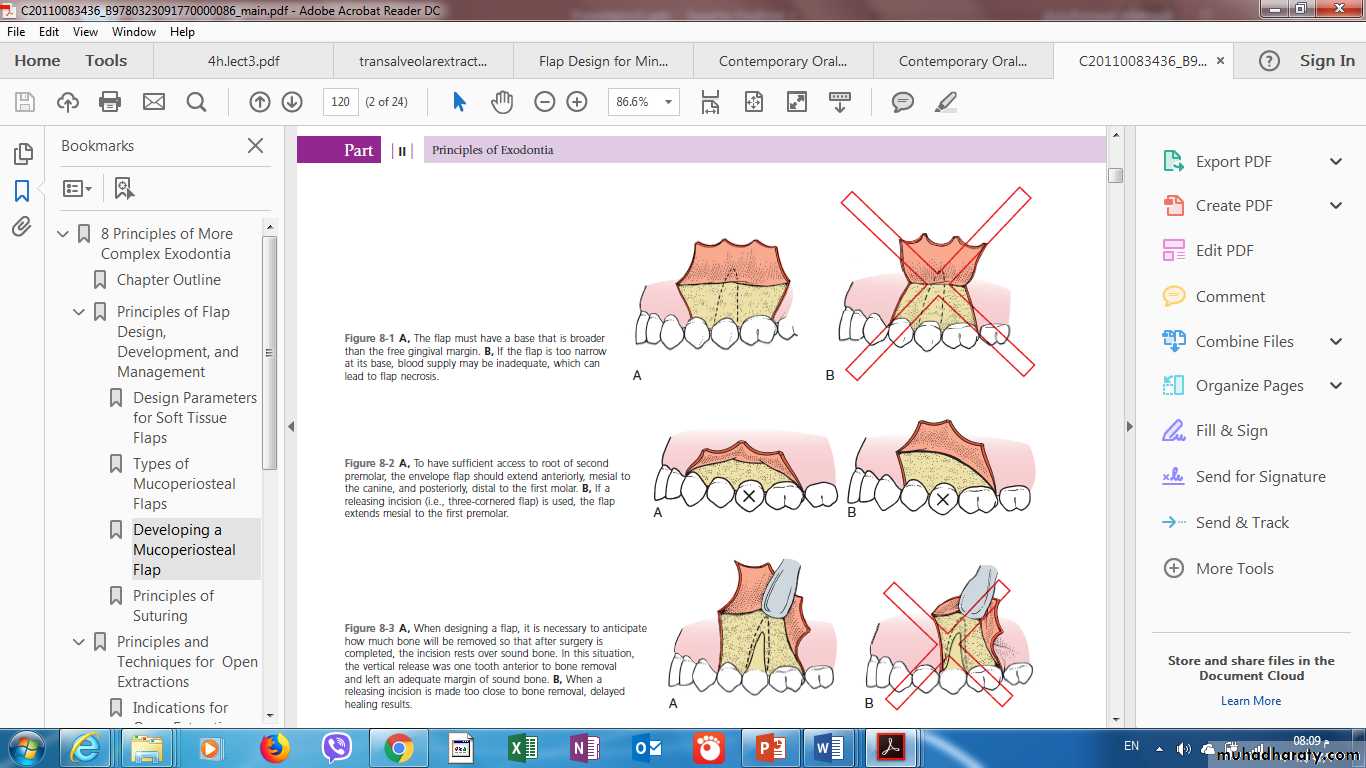
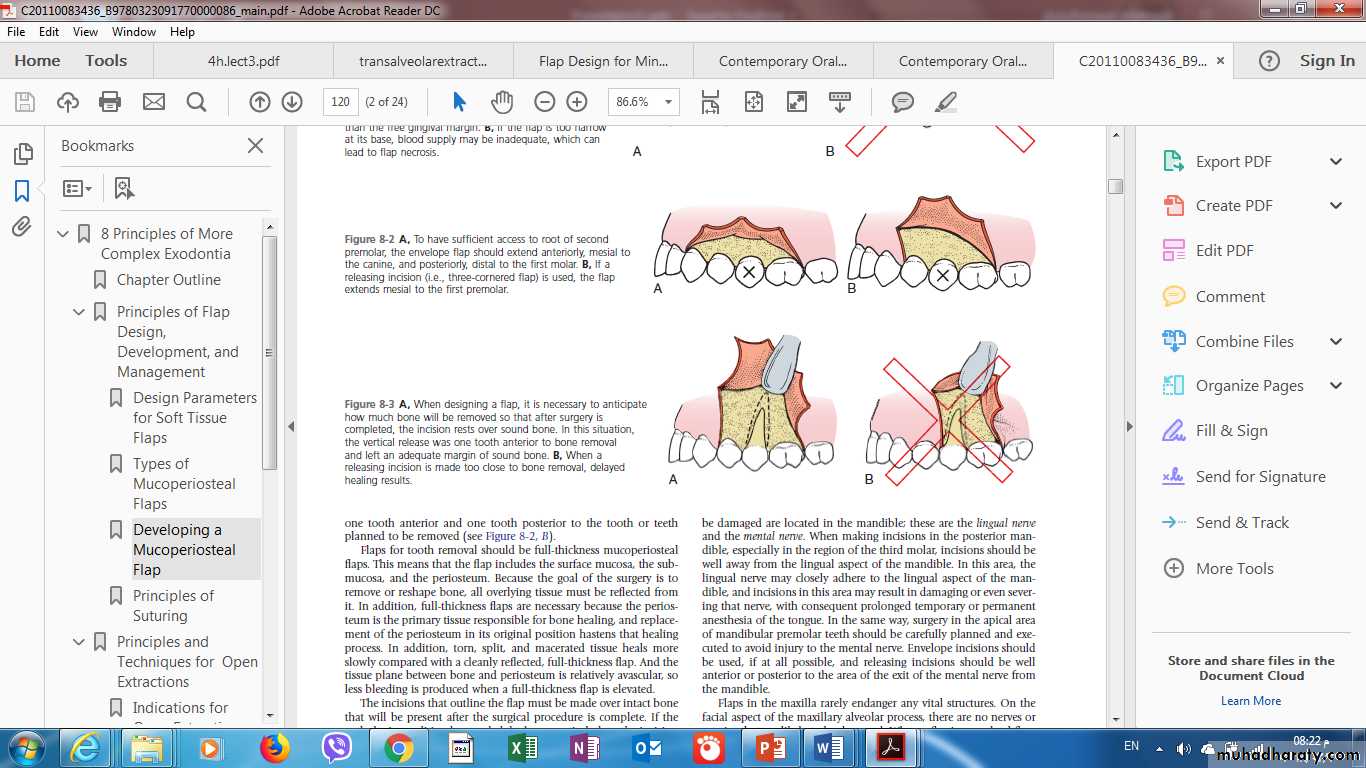
1-When the flap is outlined, the base of the flap must usually be broader than the free margin to preserve an adequate blood supply
PRINCIPLES OF FLAP DESIGN
2-Flaps for tooth removal should be full-thickness mucoperiosteal flaps. This means that the flap includes the surface mucosa, the submucosa, and the periosteum.( why)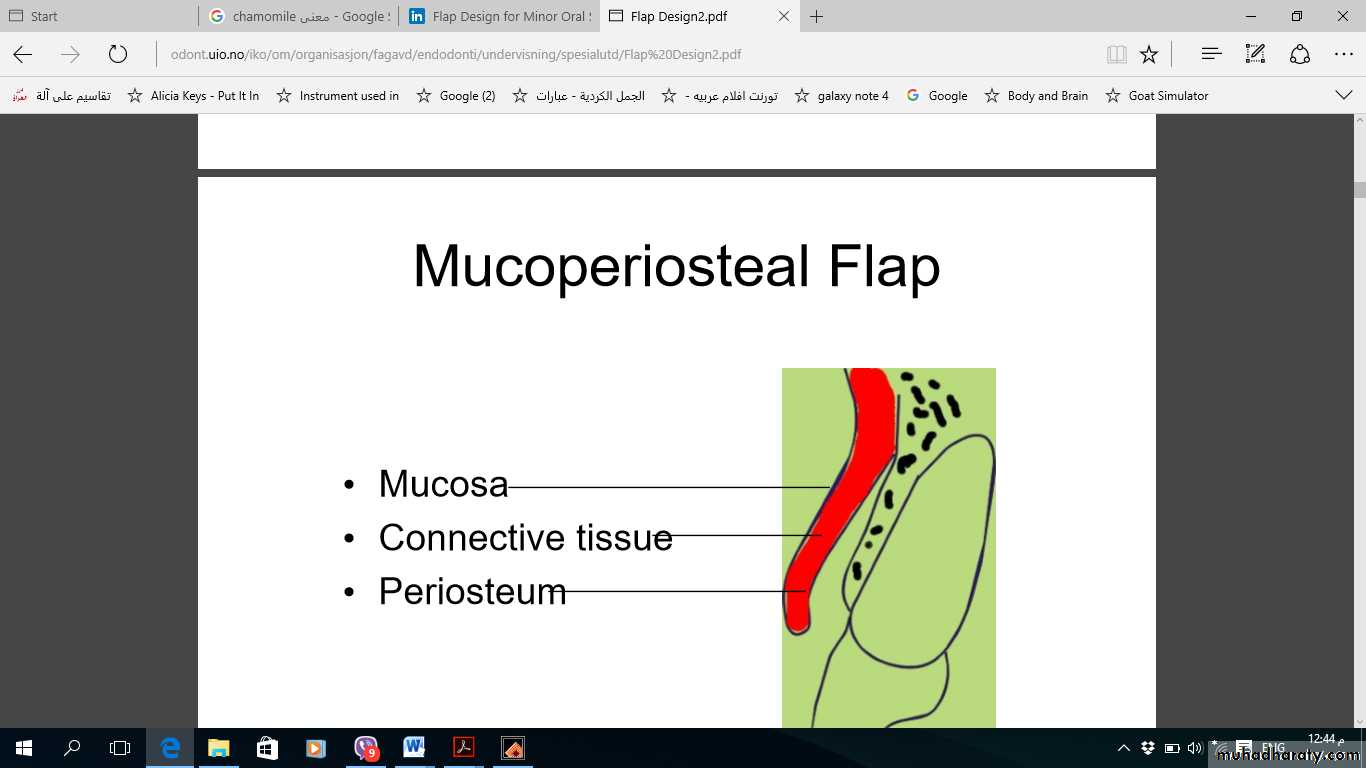
3-The incisions that outline the flap must be made over intact bone that will be present after the surgical procedure is complete
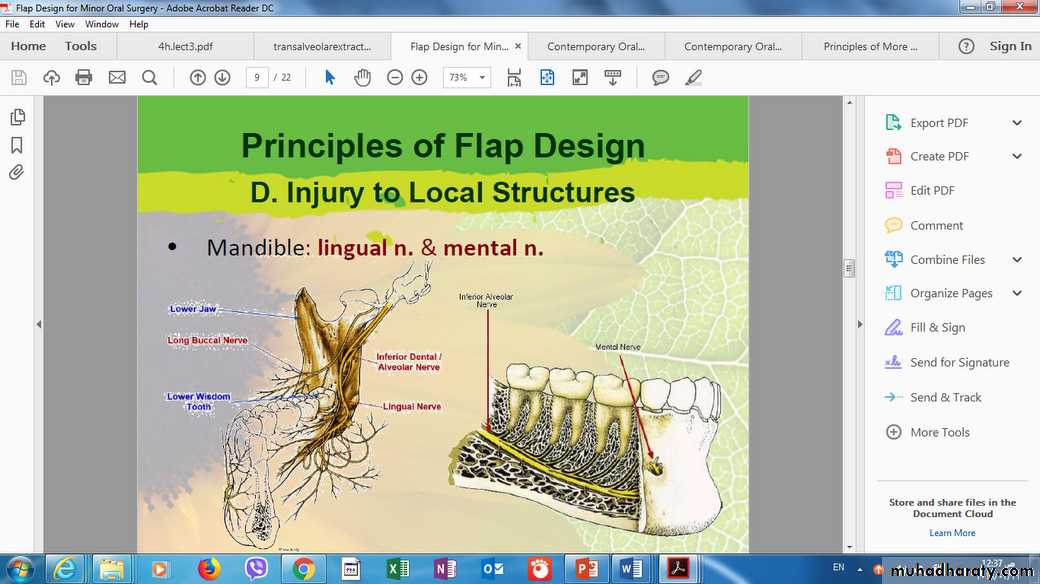
4-The flap should be designed to avoid injury to local vital structures in the area of the surgery
The two most important structures that can be damaged are located in the mandible;
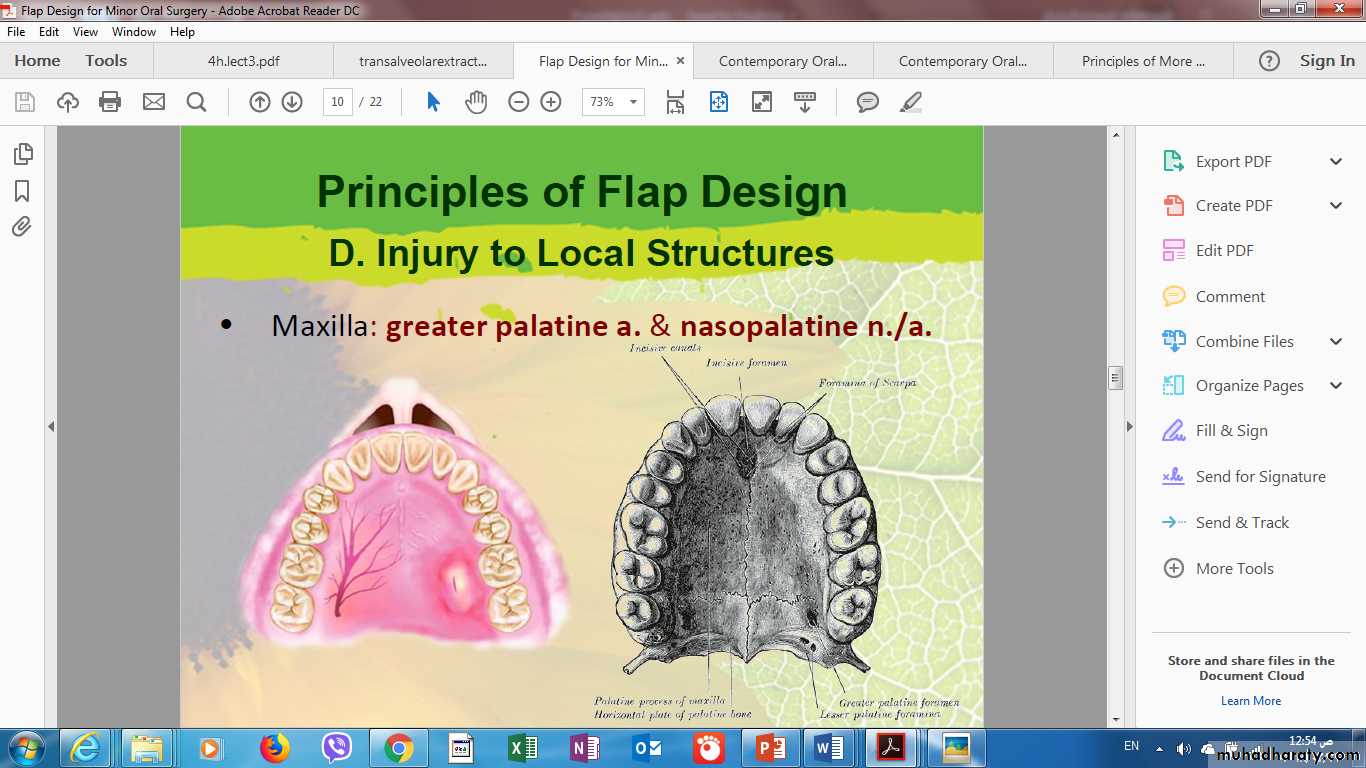
these are the lingual nerve and the mental nerve.When reflecting a palatal flap, the surgeon must remember that the major blood supply to the palatal soft tissue comes through the greater palatine artery, which emerges from the greater palatine foramen at the posterior lateral aspect of the hard palate
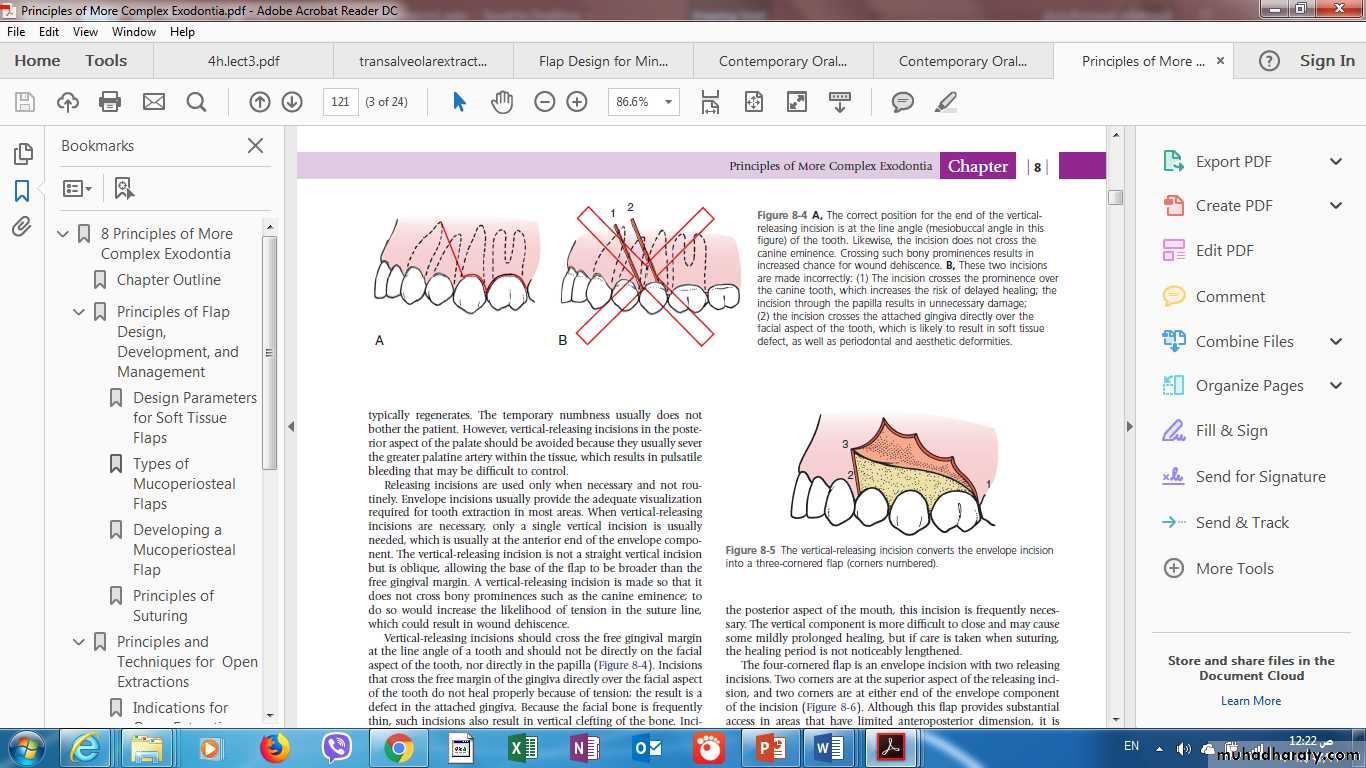
5-Vertical-releasing incisions should cross the free gingival margin at the line angle of a tooth and should not be directly on the facial aspect of the tooth, nor directly in the papilla
6.The flap must be of adequate size for several reasons
1-Sufficient soft tissue reflection is required to provide necessary visualization of the area.2- For the insertion of instruments required to perform the surgery.
3- In addition, the flap must be held out of the operative field by a retractor that must rest on intact bone.
4-There must be enough flap reflection to permit the retractor to hold The flap without tension.
Incision that should be avoided
1. Incision over boney prominences?
2. Incision through papillae
3. Incision over facial aspect midcrwon
4. Incision not placed over sound bone
5. Vertical incision on area of mental foramen
6. Lingual incision in the posterior mandible
7. Vertical releasing incision in the posterior palate
1-Envelope Flap
This type of flap is the result of an extended horizontal incision along the cervical lines of the teeth. The incision is made in the gingival sulcus and extends along four or five teeth .it is usually indicated when the surgical procedure involves the cervical lines of the teeth labially (or buccally) and palatally (or lingually), apicoectomy (palatal root), removal of impacted teeth, cysts.Types of Flaps
Advantages. Avoidance of vertical incision and easy reapproximation to original position.
Disadvantages.Difficult reflection (mainly palatally), great tension with a risk of the ends tearing,
limited visualization in apicoectomies, limited access,
possibility of injury of palatal vessels and nerves,
defect of attached gingiva.
2. Triangular Flap
This flap is the result of an L-shaped incision with a horizontal incision made along the gingival sulcus and a vertical or oblique incision.
The vertical incision begins approximately at the vestibular fold and extends to the interdental papilla of the gingiva. The triangular flap is performed labially or buccally on both jaws and is indicated in the surgical removal of root tips, small cysts, and apicoectomies.
Advantages. Ensures an adequate blood supply, satisfactory visualization, very good stability and reapproximation; it is easily modified with a small releasing incision, or an additional vertical incision, or even lengthening of the horizontal incision.
Disadvantages. Limited access to long roots, tensions created when the flap is held with a retractor, and it causes a defect in the attached gingiva
3.Trapezoidal Flap(THREE SIDED FLAP)
It is formed by a horizontal incision along the gingivae, and two oblique vertical releasing incisions extending to the buccal vestibule.Advantages.
1.Provides excellent access,2.allows surgery to be performed on more than one or two teeth,
3.produces no tension in the tissues,
4. allows easy reapproximation of the flap to its original position and hastens the healing process.
Disadvantages. Produces a defect in the attached gingiva (recession of gingiva).
4.Semilunar Flap
This flap is the result of a curved incision, which begins just beneath the vestibular fold and has a bows haped course with the convex part towards the attached gingiva. The lowest point of the incision must be at least 0.5 cm from the gingival margin, so that the blood supply is not compromised. Each end of the incision must extend at least one tooth over on each side of the area of bone removal. The semilunar flap is used in apicoectomies and removal of small cysts and root tips.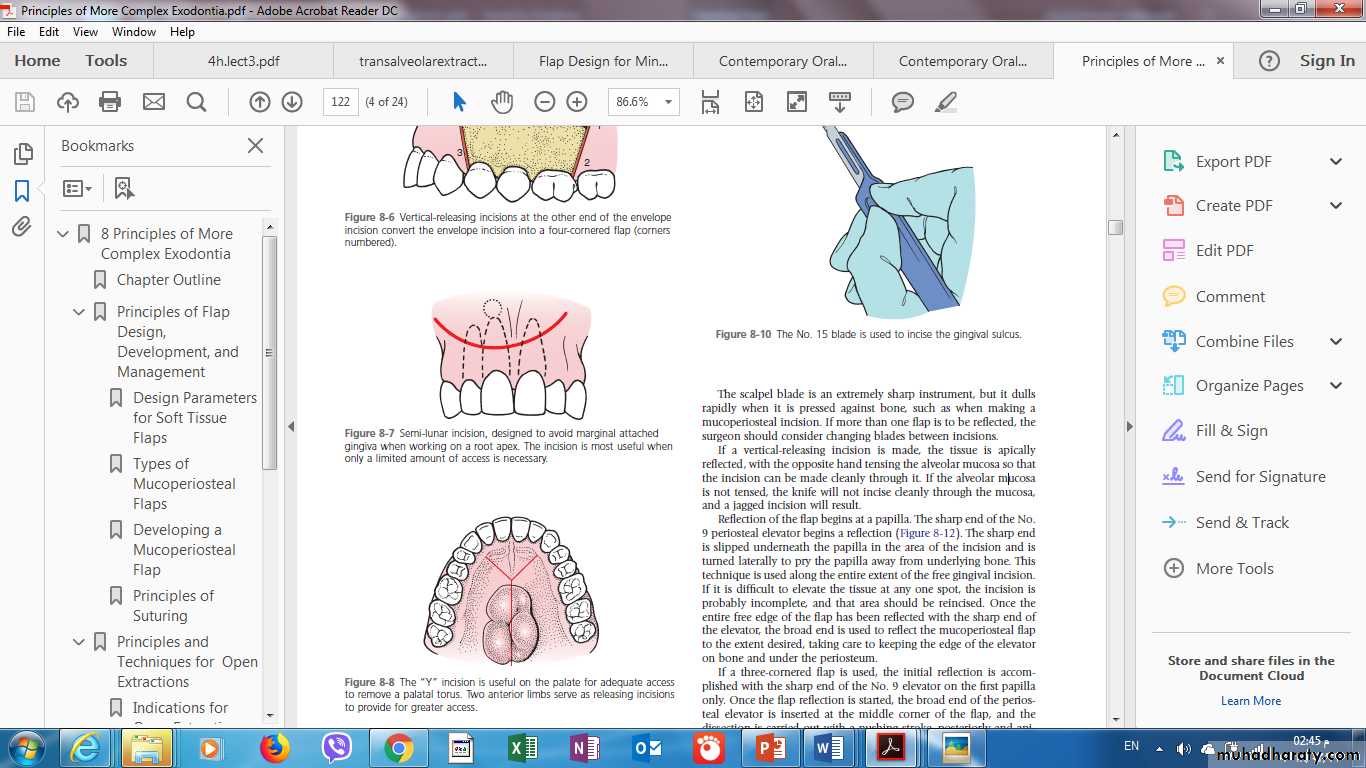
Advantages. Avoidance of vertical incision and easy reapproximation to original position.
Disadvantages. Difficult reflection (mainly palatally),great tension with a risk of the ends tearing,
limited visualization in apicoectomies,
limited access,
possibility of injury of palatal vessels and nerves,
defect of attached gingiva
Suturing
Suturing is defined as sewing together two structures or tissues using suture threaded on a needle.
Suturing of the surgical wound is necessary, aiming at holding a flap over the wound, reapproximating the wound edges, If the space between the two wound edges is minimal, wound healing will be rapid and complete. If tears or excessive trauma to the wound edges occur, wound healing will be by secondary intention.
, protecting underlying tissues from infection or other irritating factors, and preventing postoperative hemorrhage. Suturing may also aid in the following: