Secret Lectures
(11)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
1
Spleen
• Imaging modalities :US, CT, MRI
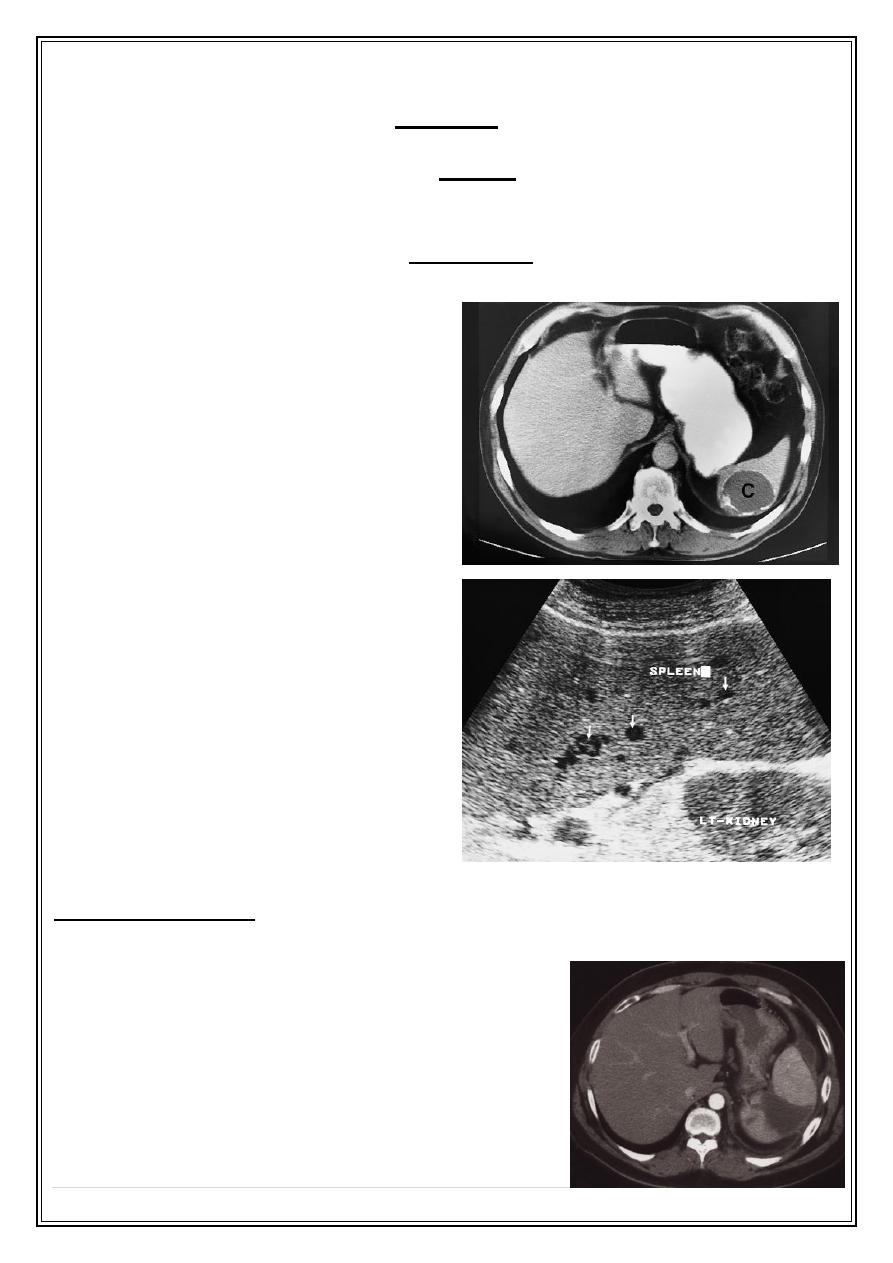
• The commonly encountered splenic masses are : cysts including H.cysts,
abscesses and tumors including lymphoma is much commoner than
metastases
which
are rare in the spleen.
• Many conditions causing splenic enlargement but cause no change in splenic
texture on US and CT eg. Lymphoma , portal HT,chronic infection , various
blood disorders.
Hydatid cyst. CT showing a cyst (C) in the
spleen withcalcification in its walls.
Lymphoma. Ultrasound showing an enlarged
spleen with several hypoechoic areas within it
.
, may occur secondary to severe pancreatitis, pancreatic
Splenic infarction
carcinoma, sickle cell or trauma, is well demonstrated on CT as either focal or
complete loss of normal enhancement following
intravenous contrast
Splenic infarction. CT with contrast demonstrates a
wedge-shaped non-enhancing segment of spleen
Secret Lectures
(11)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
2
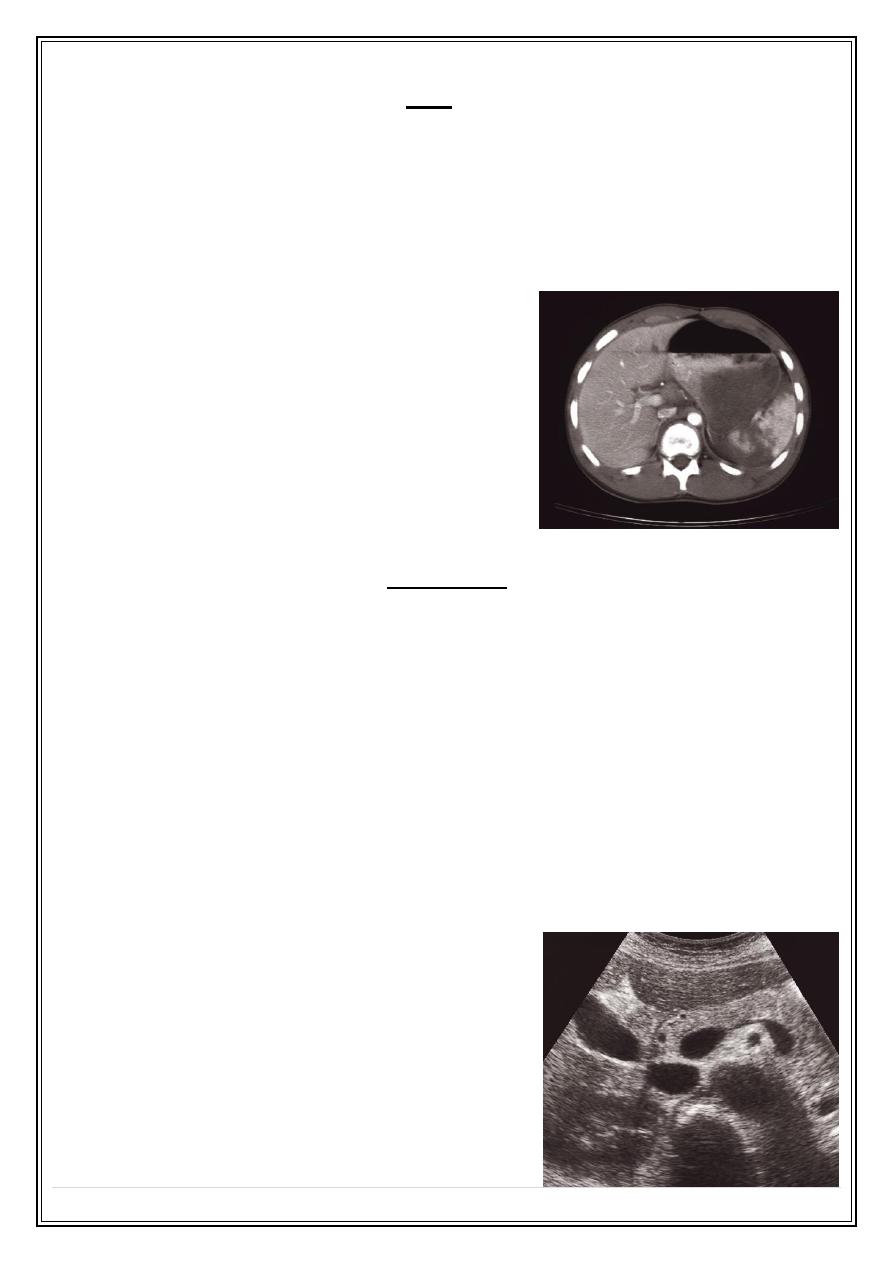
• The spleen is the most commonly injured organ in blunt abdominal trauma and
laceration , contusion or haematoma may results .rupture may be delayed until
sometime after the injury. Splenic injury may be detected by US , but CT is
superior. Changes of splenic rupture may be seen on plain film , as haematoma
form amass may be seen in the upper abdomen displacing adjacent structures ,
there may be paralytic ileus and fracture of lower ribs. However these signs
often not seen even with significant injury to the spleen.
Ruptured spleen on CT. The spleen is shattered with
low-density blood (arrows) adjacent to the fragments.
Pancreas
Method of investigation
:
• CT :
- is the mainstay imaging modality.
- superior to US : no interference of adjacent bowel gas
• Abdominal Ultrasound.
• Endoscopic US:
- is routinely used in the diagnosis (including biopsy) of pancreatic disease and
staging in patients with pancreatic cancer (e.g. involvement of the superior
mesenteric artery precludes a surgical cure
• MRI and MRCP.
• ERCP
• Arteriography
Ultrasound of normal pancreas (transverse scan).
Secret Lectures
(11)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
3
CT of normal pancreas
Pancreatic masses:
•
The usual causes of masses in , or immediately adjacent to pancreas are
:
carcinoma of pancreas , neoplasm of adjacent LN, focal pancreatitis m
pancreatic abscess and pseudocysts. Occasionally congenital cysts may be
seen.
•
Most neoplasms of pancreas are adenocarcinoma
, two 3
rd
occur at the head ,
and these can diagnosed even when are small (obstructing the common bile
duct and causing jaundice . while those arise in the body and tail have to be
fairly large to give rise to signs or symptoms (pain being the cardinal symptom).
•
The important sign of carcinoma both on CT and US:
= a focal mass within or deforming the outline of the gland.
= on an enhanced CT scan the tumor appears of lower density compared to the
normal pancreatic tissue.
= obstructive dilatation of pancreatic duct +/- common duct on CT , US or MRCP.
• Staging attempts to identify potentially resectable tumors. Most are irresectable :
the presence of liver metastases , adenopathy ,retroperitoneal invasion, tumor
encasement of arteries and veins are contraindications to surgery.
• The presence of endocrine secreting tumors, of which insulinoma is the
commonest example, is suggested by clinical presentation and biochemical
investigation. These are usually small and difficult to detected, may be seen on
US, CT or MRI as small rounded masses, sometimes selective angiography is
required- hypervascular tumor. Special somatostatin receptor radionuclide scans
(octreoscan) may also demonstrate the tumor and any metastases.
Secret Lectures
(11)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
4
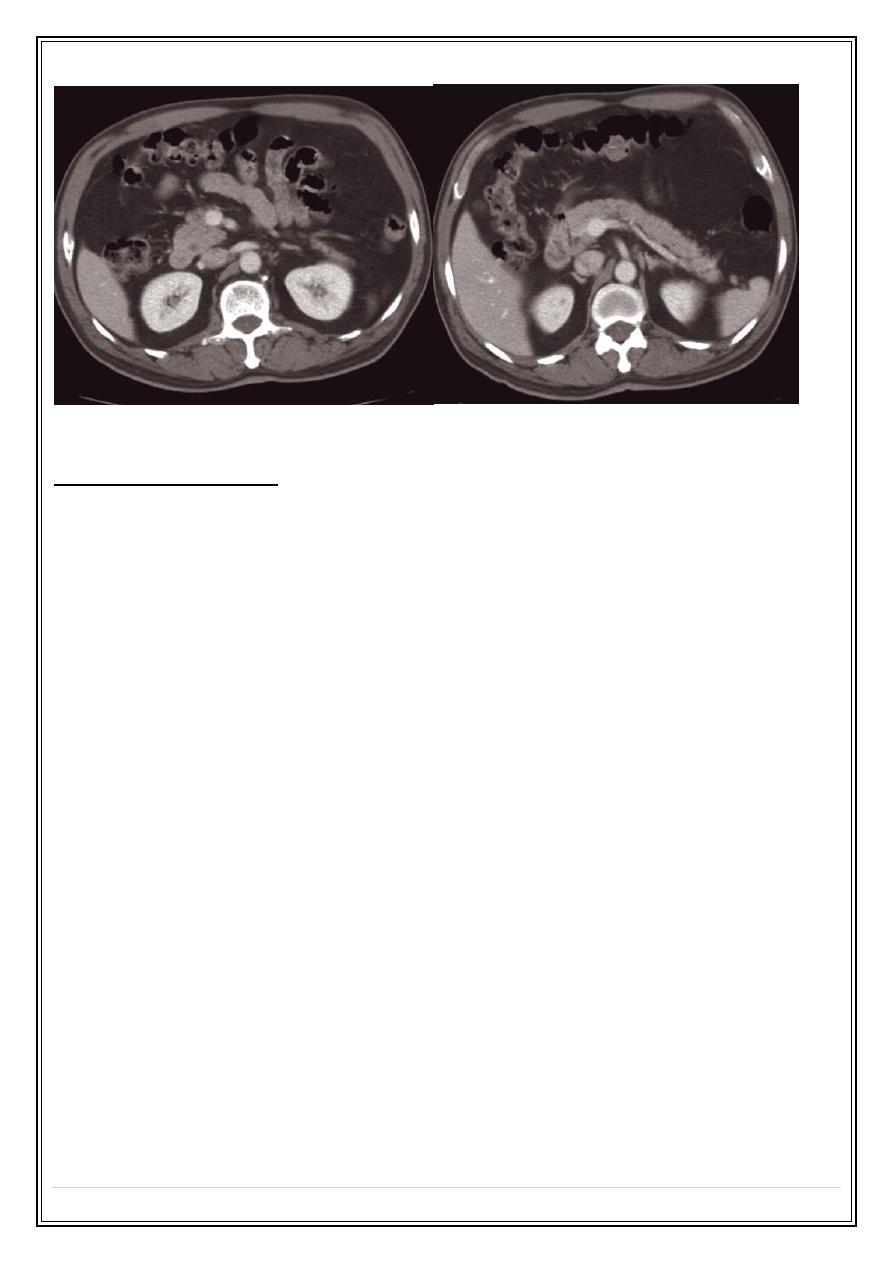
Carcinoma of the pancreas (a) head of the pancreas (b) the body of the pancreas
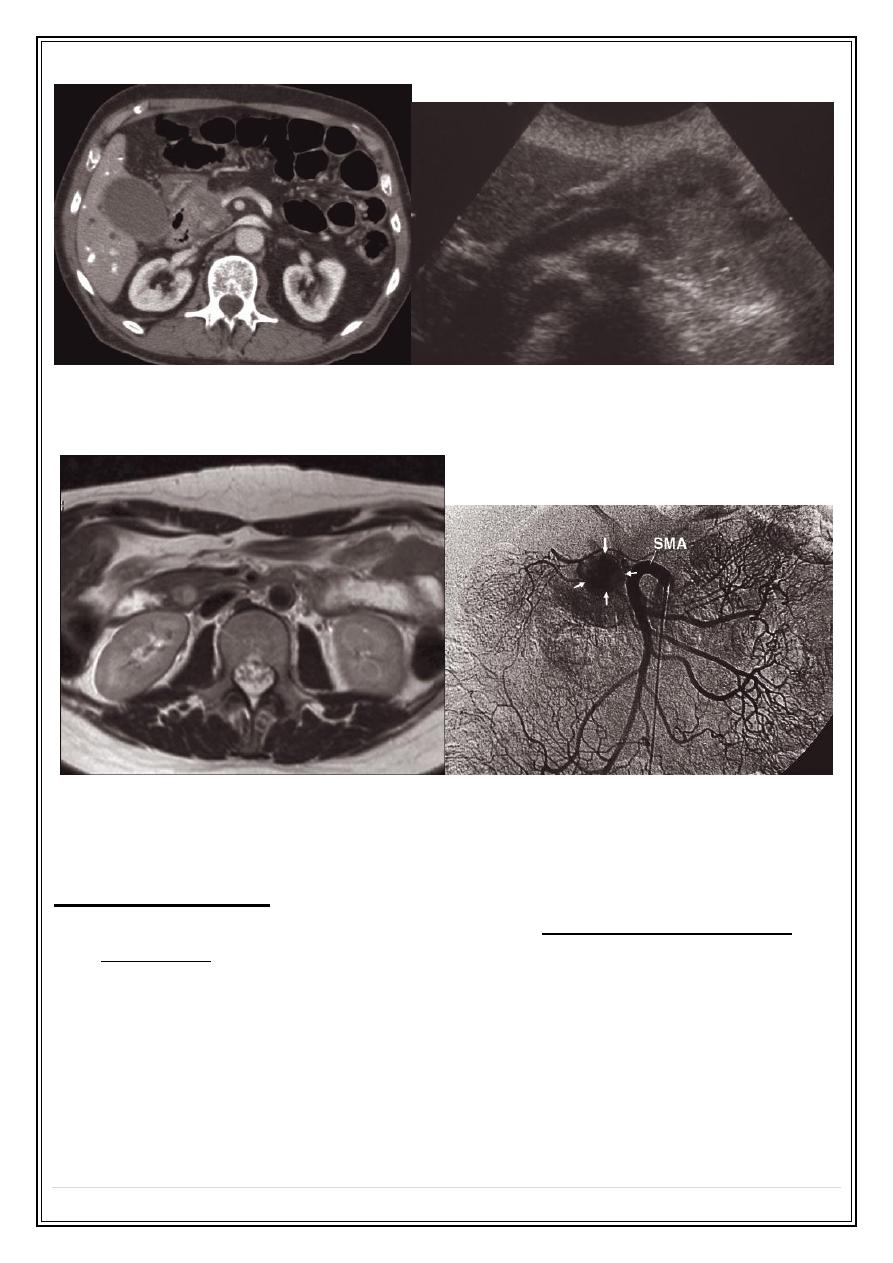
Insulinoma. (a) Axial T2-weighted MRI demonstrating a 1.5 cm insulinoma in the uncinate
process of the pancreas . (b) Selective superior mesenteric angiogram in another patient
showing the tumour as a vascular blush (arrows)
Acute pancreatitis:
• The findings at CT and US vary with amount of necrosis, hemorrhage, and
suppuration.
• The pancreas is usually
enlarged
, often diffusely and may shows
irregularit
y of
its outline , caused by extension of inflammatory process into surrounding fat:
features that are well recognized at CT.
•
The diagnosis of pancreatitis is usually made on clinical and biochemical
grounds
, the purpose of imaging, with contrast –enhanced CT, is to assess the
severity of the disease and to demonstrate
complications
:
Secret Lectures
(11)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
5
1.
Necrotic or nonviable tissue
( not enhanced after IV contrast)
2.
An
abscess
formation .
3.
Vascular complications are serious
and include splenic vein thrombosis
, arterial erosion and formation of a pseudoaneurysem
.
4.
Pseudocysts
: tissue necrosis leads to a leak of pancreatic secretions
contained in a cyst-like manner within or adjacent to pancreas, well
seen on CT or US as a thin or thick walled cysts containing fluid vary in
size from very small to many centimeters in diameter, may resolve
spontaneously or may needs surgery
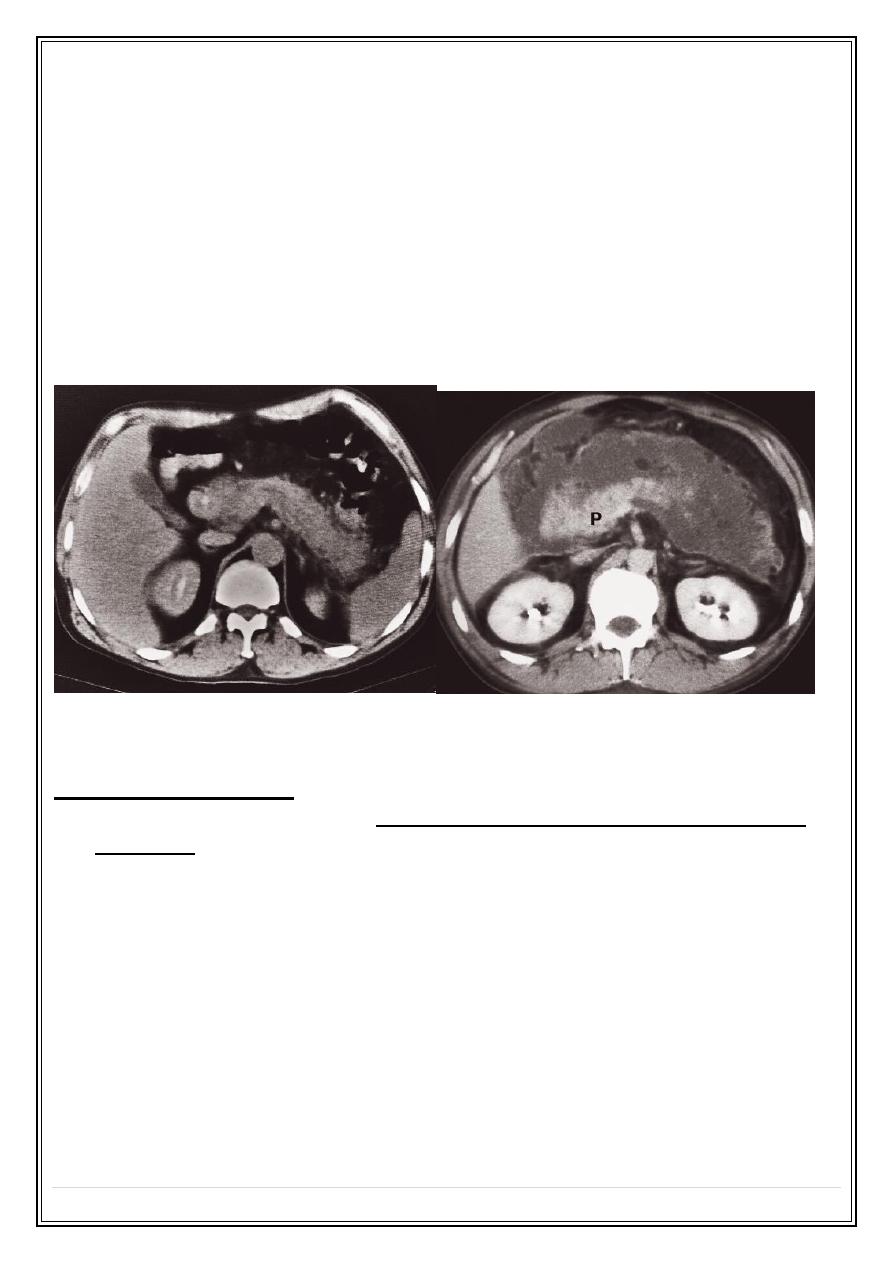
Acute pancreatitis. (a) CT scan showing diffuse enlargement of the pancreas with ill-
defined edges. (b) CT scan showing considerable inflammation around the pancreas (P).
Chronic pancreatitis:
• Chronic pancreatitis results in fibrosis, calcifications, and ductal stenosis and
dilatations.
•
Pseudocysts
are seen with chronic pancreatitis just are in the acute form.
• The
calcification
is mainly due to small calculi within the pancreas, often
recognizable on plain films, US, and particularly on CT.
• The
gland may enlarged focally or generally
, focal enlargement is rare and is
then often indistinguishable from carcinoma.
• Conversely, the pancreas
may atrophy focally or generally.
Atrophy is anon-
specific sign, its frequently seen in normal elderly people and also occurs distal
to carcinoma.
•
The pancreatic duct may enlarged and irregular.
• ERCP occasionally used to try and document chronic pancreatitis and exclude
carcinoma. MRCP can be used as alternative non-invasive method.
Secret Lectures
(11)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
6
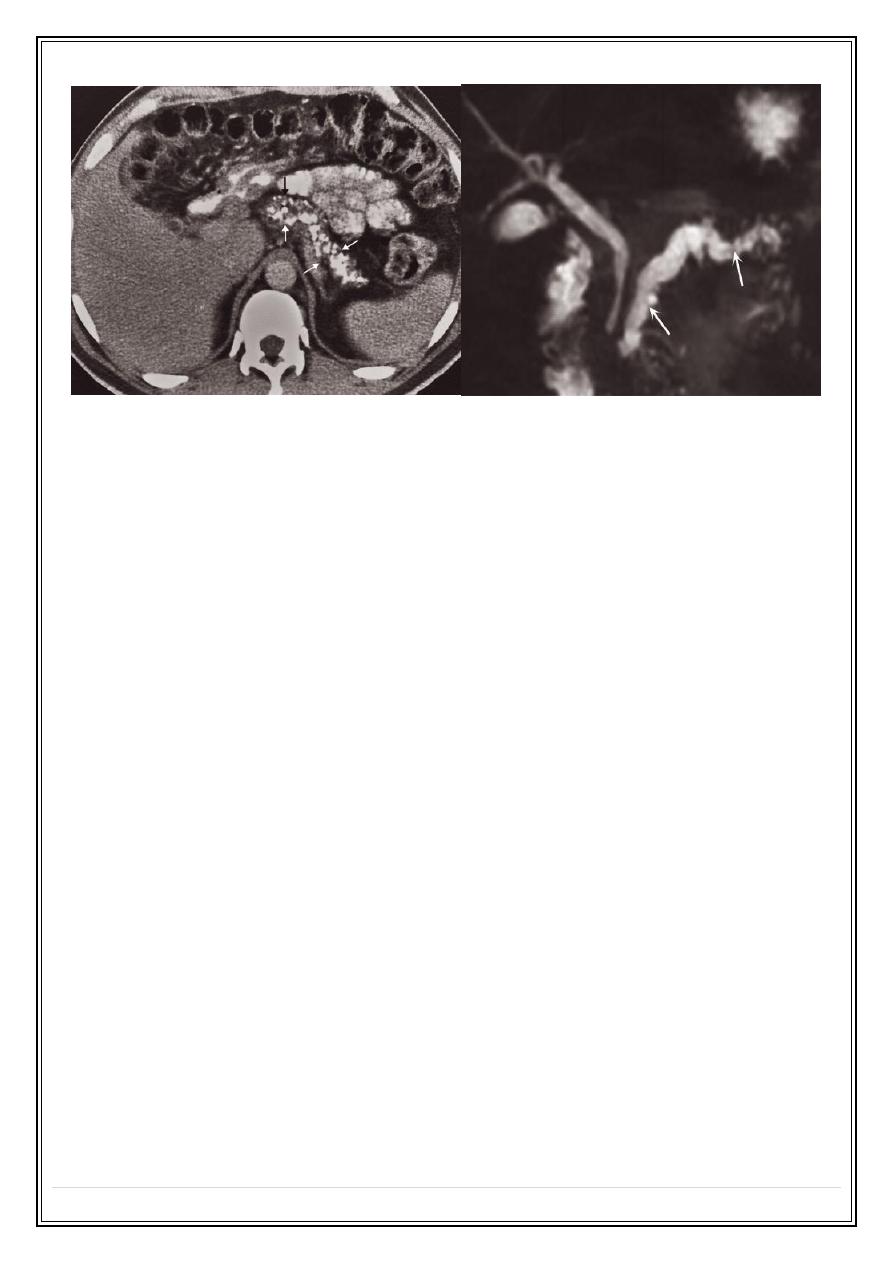
Chronic pancreatitis. (a) CT scan showing numerous small areas of calcification within the
pancreas (arrows) (b) Magnetic resonance cholangiopancreatography (MRCP) showing a
normal biliary duct system but irregular dilatation of the pancreatic duct (arrows)
Thank you,,,