TYPES OF FLAPS
SOFT TISSUE MANAGEMENT
A: CONSIDERATIONS IN FLAP DESIGN1. Number of teeth involved
2. Length and shape of roots involved
3. Presence or absence of periradicular pathosis
4. Extent of periradicular lesion
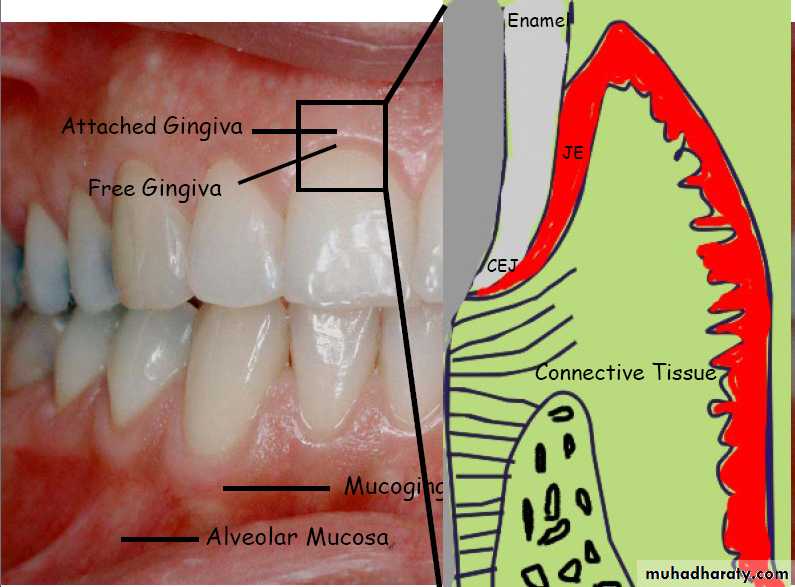
5. Sulcular depth
6. Location and size of frenum and muscle attachments
7. Approximating anatomic structures.
8. Access needed.
9. Types of restorations in surgical area.
10. Width of attached gingiva.
B: (Principles of flap design)
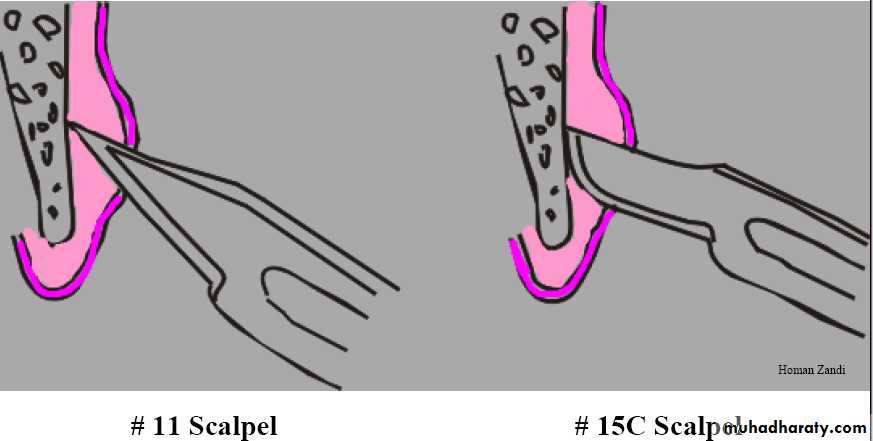
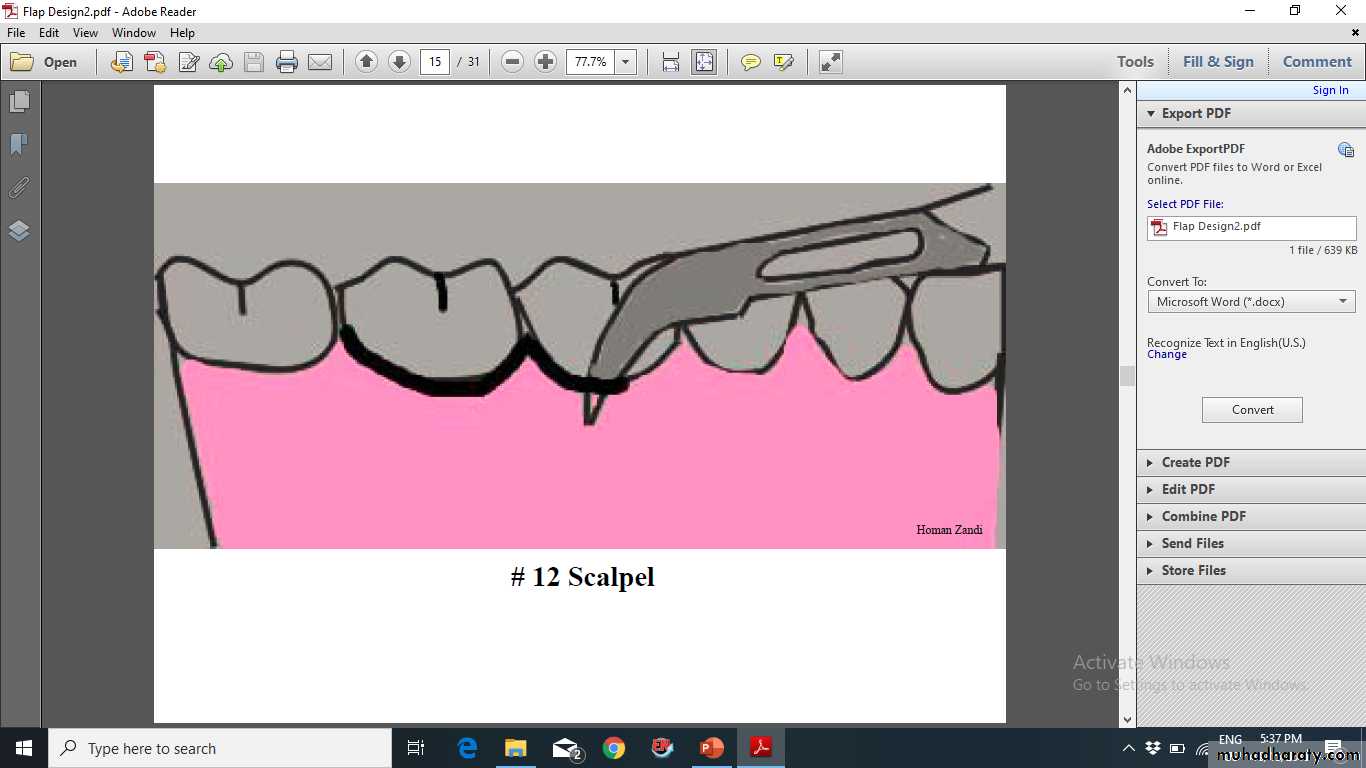
1. Incision is made with a firm, continuous stroke.
2. Incision should not cross underlying bony defect that existed prior to surgery, or is produced by surgery…….
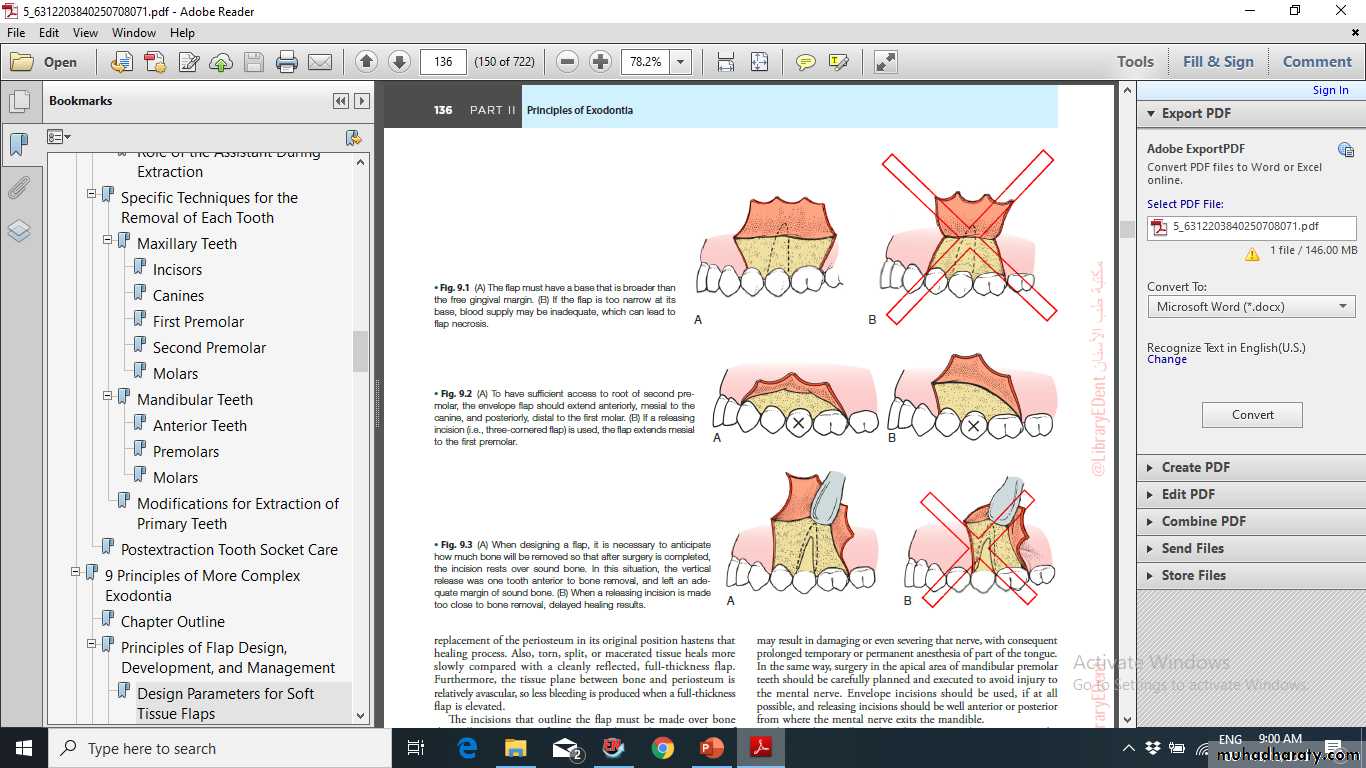
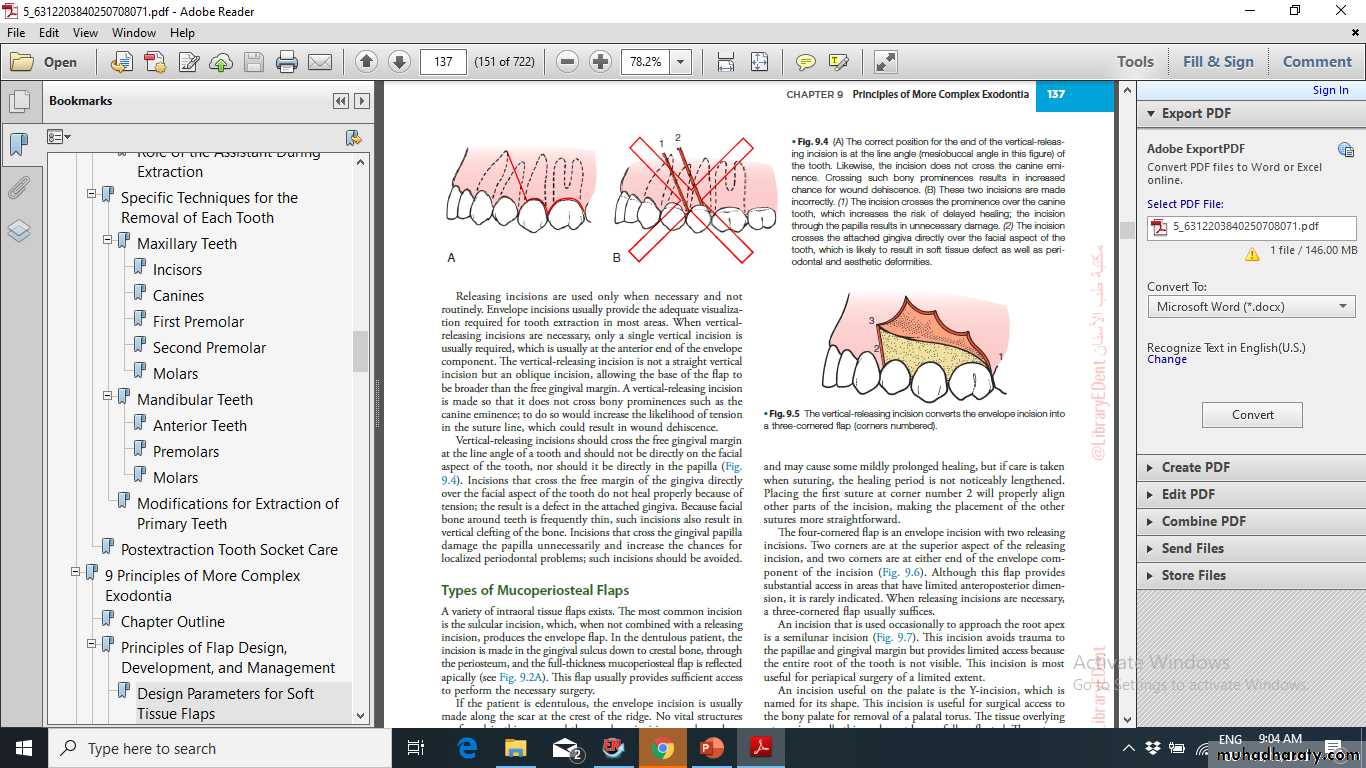
• Vertical incisions are made in the concavities between bony eminences.
• Termination of the vertical incision at the gingival crest must be at the line angle of the tooth, dental papilla should be included or excluded.
5. Do not extend the vertical incision beyond the depth of the muco-buccal fold
6. Base of the flap must be broader than free edge (Supraperiosteal blood vessels run vertically, try not to transect them)
• 7. Periosteum must be reflected as an integral part of the flap.
8. Retractor must rest on bone and not impinge on soft tissue
9. Any tissue removed must be submitted for biopsy
10. Suture from unattached to attached tissue.
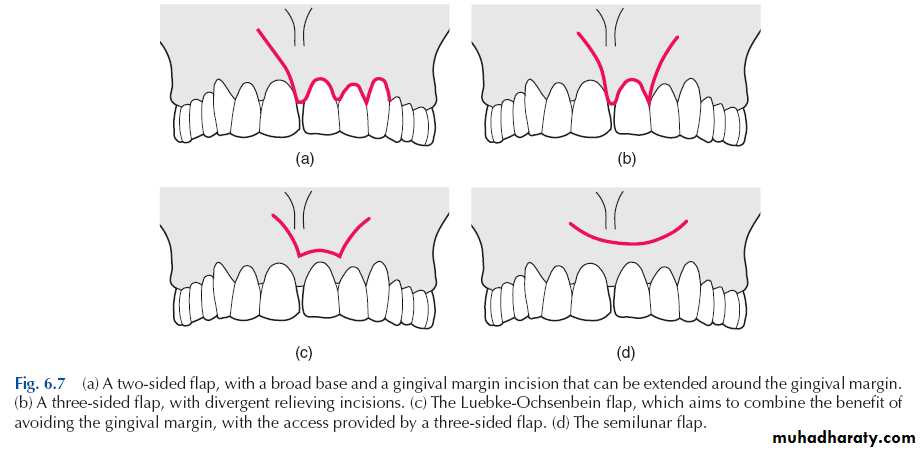
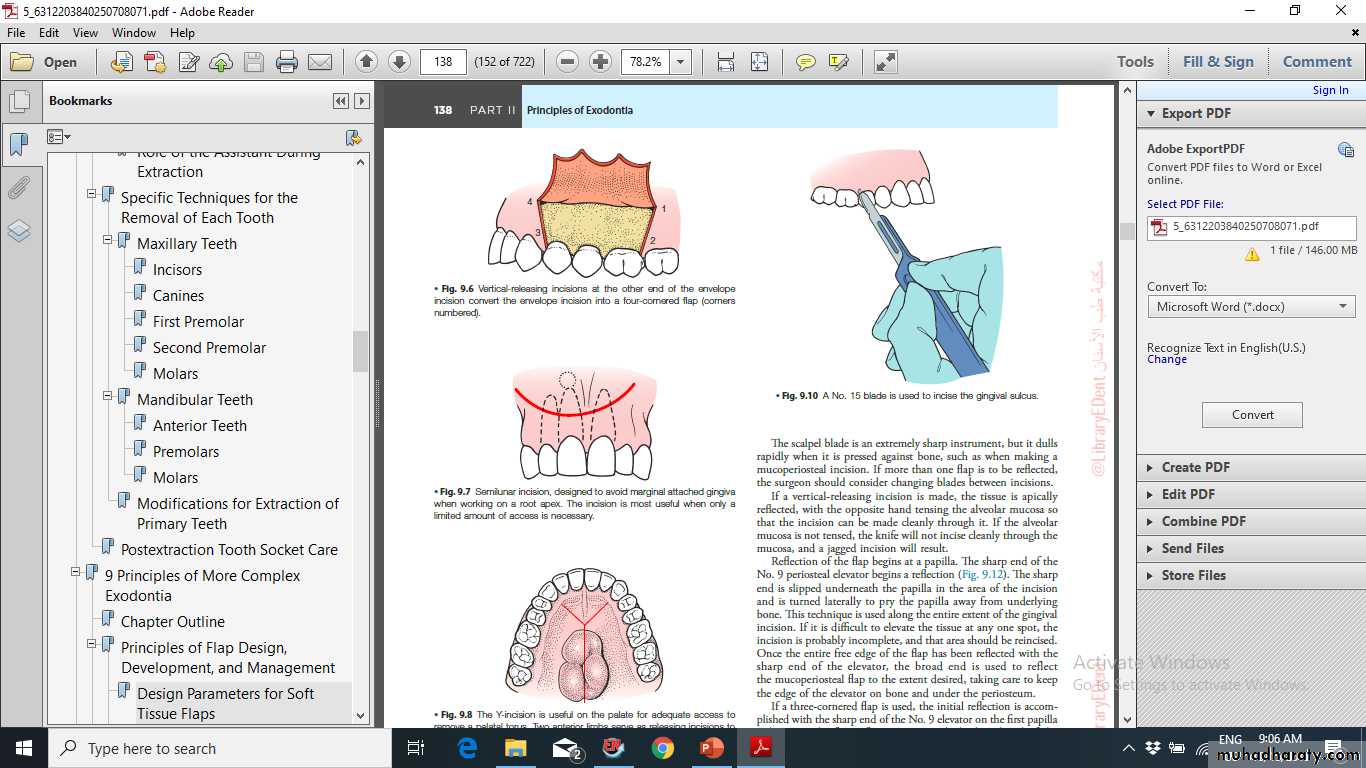
1-Semilunar flap
Advantages- Fast, easy to reflect
- Marginal and interdental gingiva are not involved
- Unaltered soft tissue attachment level
- Crestal bone is not exposed
- May be used for an extremely long root in certain situations (long maxillary canine)
Disadvantages:-
• Excessive scarring• Disruption of blood supply to unflapped tissues
• Flap shrinkage
• Difficult flap re-approximation and wound closure
• Delayed, secondary intention healing with more postsurgical sequelae
• Limited apical orientation (cannot visualize root eminences and other landmarks)
• Limited use in mandibular surgery
• May cross bony cavity
• Cannot extend flap
• Least amount of access and convenience
1-Semilunar flap
2-Triangular (intrasulcular) - One vertical releasing incision
Advantages
- Excellent wound healing potential
- Minimal disruption of vascular supply to flapped tissues
- Excellent visibility
- Can view the entire root and overlying cortical and crestal bone; good for viewing and treating periodontal defects and root fractures
- Easy to extend, if needed
- Good flap re-approximation
- Easy to suture
Disadvantages
More difficult to incise and reflectSurgical access slightly limited due to the single releasing incision
Possibility of slight gingival recession
2-Triangular (intrasulcular) - One vertical releasing incision
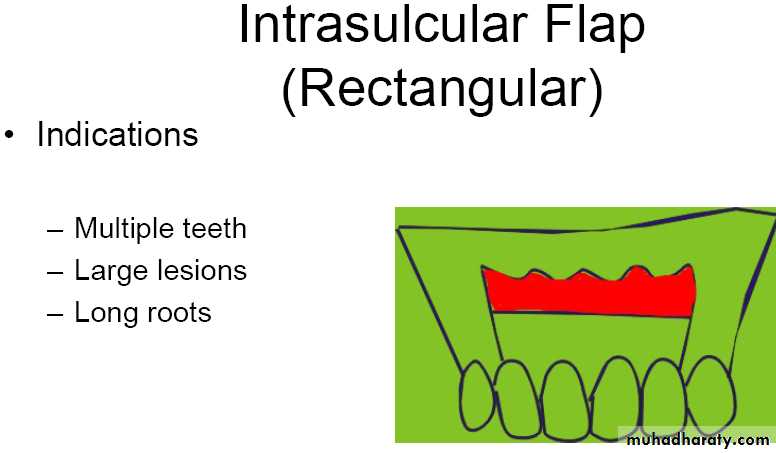
3. Rectangular or Trapezoidal (intrasulcular) - Two vertical releasing incisions, horizontal intrasulcular incision
Disadvantages
- More difficult to incise and reflect- Possibility of gingival recession
- Flap re-approximation, wound closure, suturing, and post-surgical stabilization is more difficult than with the triangular flap
3. Rectangular or Trapezoidal (intrasulcular) - Two vertical releasing incisions,
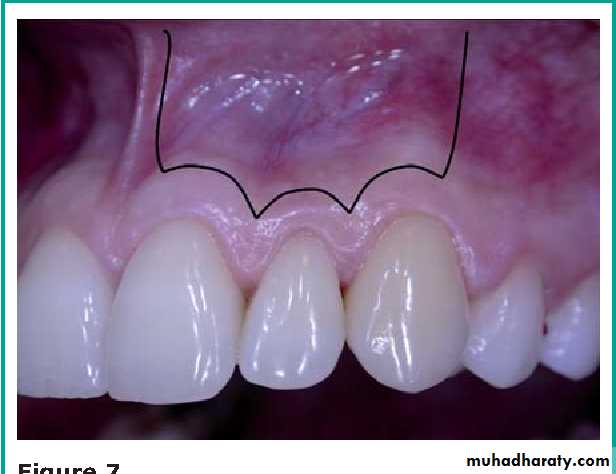
4. Submarginal (Ochsenbein-Luebke)
Formed by scalloped horizontal incision in attached gingiva and two vertical releasing incisions.Scalloped incision corresponds to the contour of the marginal gingiva.
There must be an adequate band of attached gingiva present (4-5mm).
This requires a very careful analysis of attachment level along the entire length of the horizontal incision.
Advantages
- Does not involve marginal or interdental gingiva.- Does not expose crestal bone
- Minimizes gingival recession where crowns are in place and esthetics is a concern.
- Minimizes crestal bone loss.
- Easy to reapproximate flap.
4. Submarginal (Ochsenbein-Luebke)
Disadvantages
• -Unable to extend flap, if needed
• - Disruption of blood supply to marginal gingival tissues, must rely on collateral circulation (which may not exist resulting in sloughing of marginal gingiva)
• - Limited use in mandibular surgery
• - Possible delayed healing- Possible scarring-Possible flap shrinkage
• - Full root and crestal bone are not exposed, so periodontal defects and root fractures are difficult to visualize and treat
4. Submarginal (Ochsenbein-Luebke)
5- Gingival (envelope)
Intrasulcular horizontal incision without vertical releasingincisions.
Generally not used for surgery in the apical area except occasionally for palatal roots of maxillary molars.
Used for root resections, root amputations, hemisections, and repair of cervical perforations or resorptive defects.
Palatal flap:1.palatal torus2.canine impaction3. palatal lesion\cyst.The anterolateral extensions of the midline incision are anterior to the region of the canine teeth???