STROKE
Dr.BASHAR SHAKER
30-10-2019
Stroke
Stroke is a common medical emergency.The incidence rises with age, and in many lower- and middle-income countries it is rising in association with less healthy lifestyles.
About 20% of stroke patients die within a month of the event and at least half of those who survive are left with physical disability.
85% sustain a cerebral infarction due to inadequate blood flow to part of the brain, and most of the remainder have an intracerebral haemorrhage
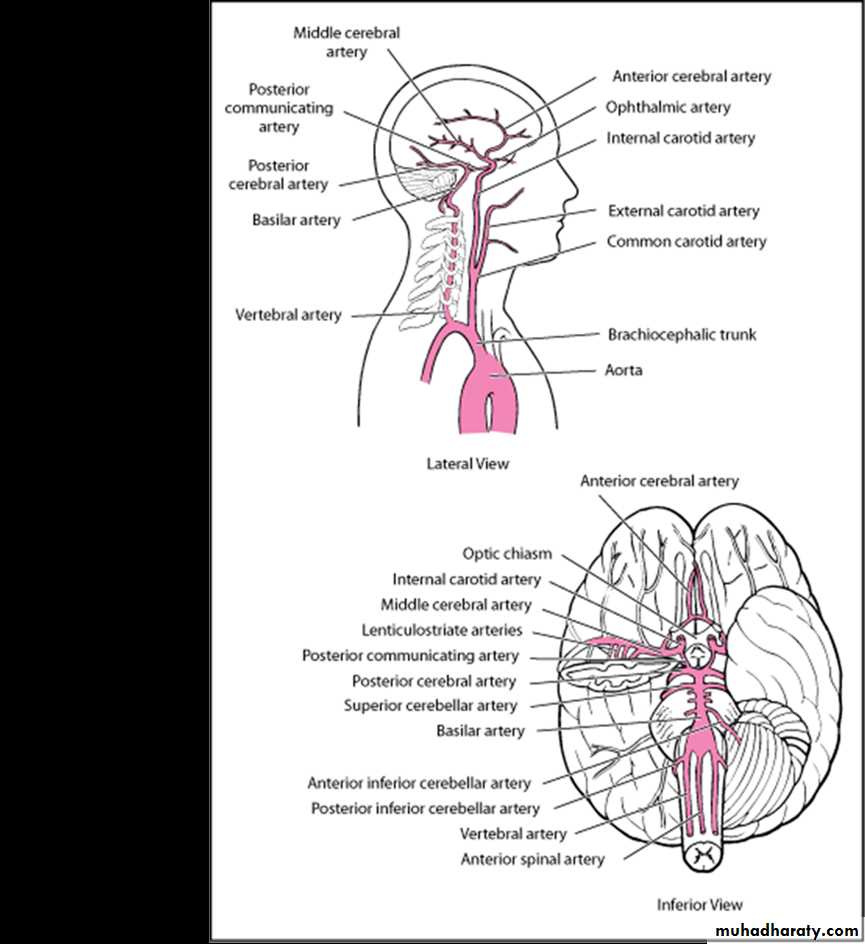
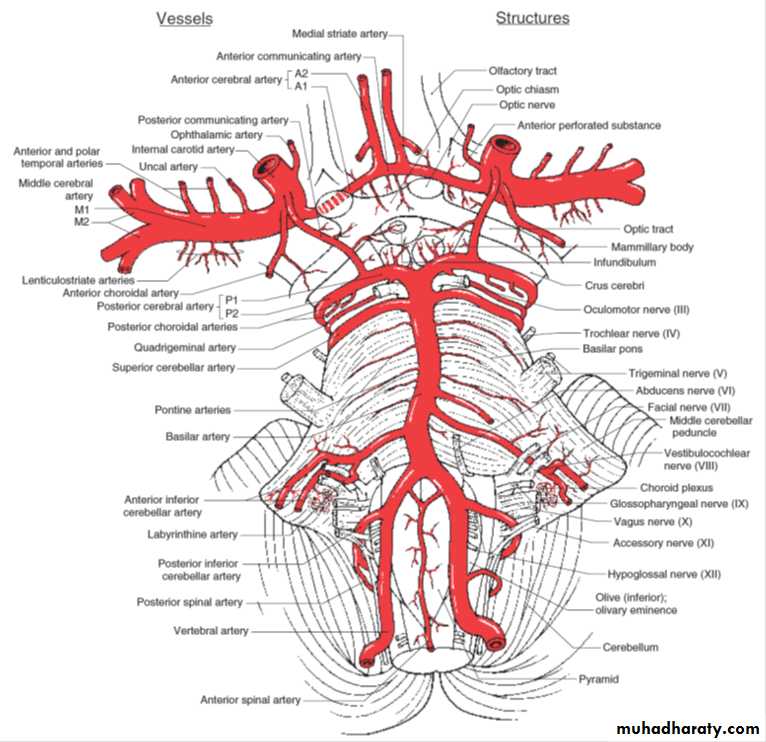
Cerebral infarction is mostly caused by thromboembolic disease secondary to atherosclerosis in the major extracranial arteries (carotid artery and aortic arch).
About 20% of infarctions are due to embolism from the heart, and a further 20% are due to thrombosis in situ caused by intrinsic disease of small
Perforating vessels (lenticulostriate arteries), producing lacunar infarctions.
Proximal arterial stenosis with hypotension that decreases cerebral blood flow in arterial watershed zones (hemodynamic stroke).
Etiology
Modifiable risk factorsHypertension
Cigarette smoking
Dyslipidemia
Diabetes
Abdominal obesity
Alcoholism
Lack of physical activity
High-risk diet (eg, high in saturated fats, trans fats, and calories)
Psychosocial stress (eg, depression)
Heart disorders (particularly disorders that predispose to emboli, such as acute MI, infective endocarditis, and atrial fibrillation)
Use of certain drugs (eg, cocaine, amphetamines)
Hypercoagulability
Vasculitis
Unmodifiable risk factors
Prior stroke
Older age
Family history of stroke
Male sex
Thrombosis
Atherothrombotic occlusion of large arteries (thrombus superimposed on an atherosclerotic artery) is the most common cause of ischemic stroke.Atheromas, particularly if ulcerated, predispose to thrombi. Atheromas can occur in any major cerebral artery and are common at areas of turbulent flow, particularly at the carotid bifurcation.
Less common causes of thrombosis include vascular inflammation secondary to disorders such as acute or chronic meningitis, vasculitic disorders, and syphilis; dissection of intracranial arteries or the aorta; hypercoagulability disorders (eg, antiphospholipid syndrome, hyperhomocysteinemia); hyperviscosity disorders (eg, polycythemia, thrombocytosis, hemoglobinopathies, plasma cell disorders); and rare disorders (eg, fibromuscular dysplasia, moyamoya disease).Older oral contraceptive formulations increase risk of thrombosis. In children, sickle cell disease is a common cause of ischemic stroke.
Emboli may originate as cardiac thrombi, especially in the following conditions
Atrial fibrillationRheumatic heart disease (usually mitral stenosis)
Post-MI
Vegetations on heart valves in bacterial or marantic endocarditis
Prosthetic heart valves
Atrial Fibrillation
Atrial fibrillation increases stroke risk 2- to 7-fold and, when valvular heart disease is also present, about 17-fold.Additional risk factors include age greater than 75 years, hypertension or diabetes, and heart failure. Atrial fibrillation predisposes to embolic stroke from thrombi that form in the left atrial appendage due to stasis of blood.
Other sources include clots that form after open-heart surgery and atheromas in neck arteries or in the aortic arch. Rarely, emboli consist of fat (from fractured long bones), air (in decompression sickness), or venous clots that pass from the right to the left side of the heart through a patent foramen ovale with shunt (paradoxical emboli). Emboli may dislodge spontaneously or after invasive cardiovascular procedures (eg, catheterization).
Lacunar infarcts
These small (≤ 1.5 cm) infarcts result from nonatherothrombotic obstruction of small, perforating arteries that supply deep cortical structures; the usual cause is lipohyalinosis (degeneration of the media of small arteries and replacement by lipids and collagen). Whether emboli cause lacunar infarcts is controversial. Lacunar infarcts tend to occur in elderly patients with diabetes or poorly controlled hypertension.Symptoms and Signs
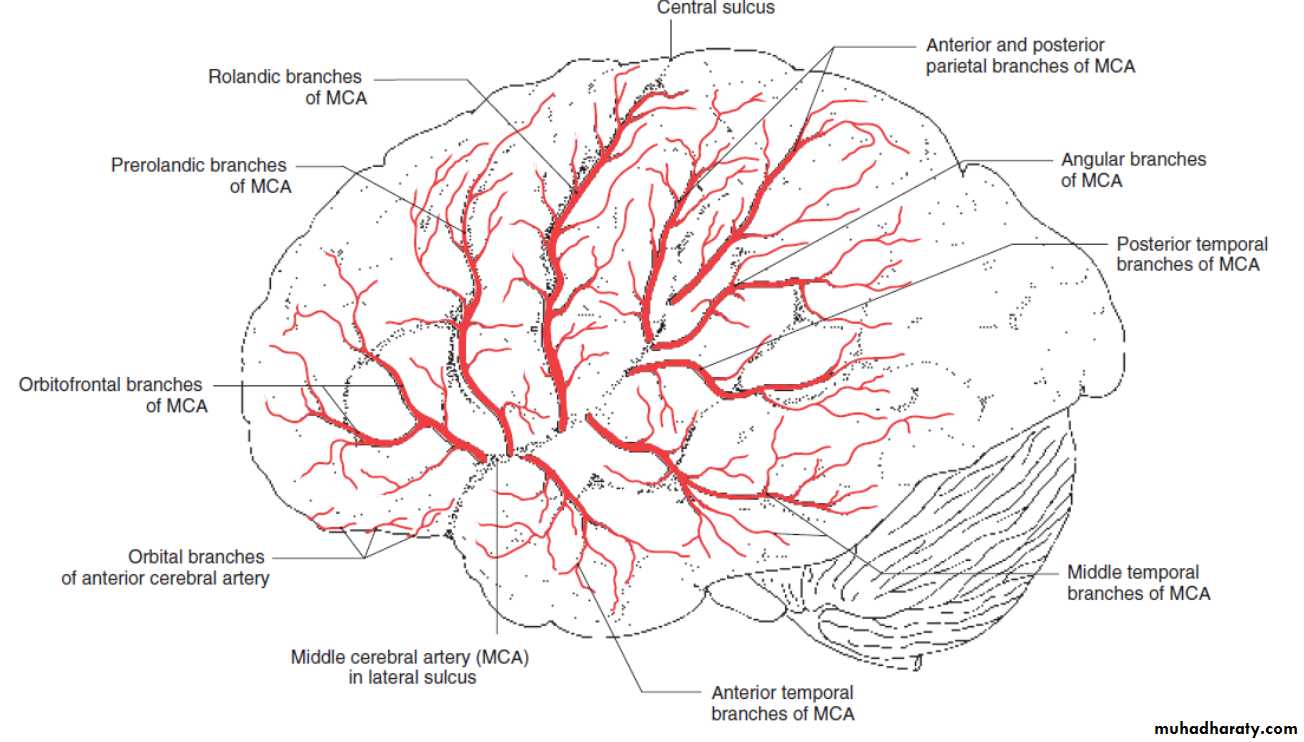
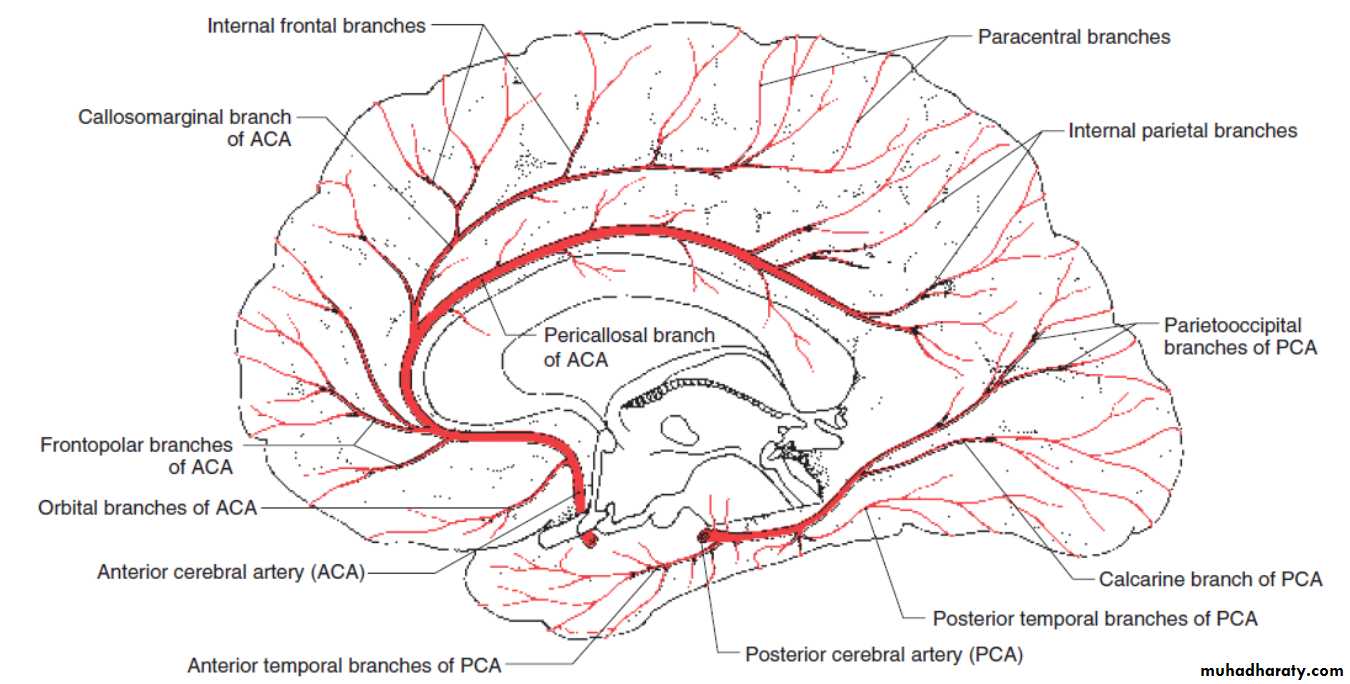
Symptoms and signs depend on the part of brain affected.Patterns of neurologic deficits often suggest the affected artery.
Severity
Collateral circulation
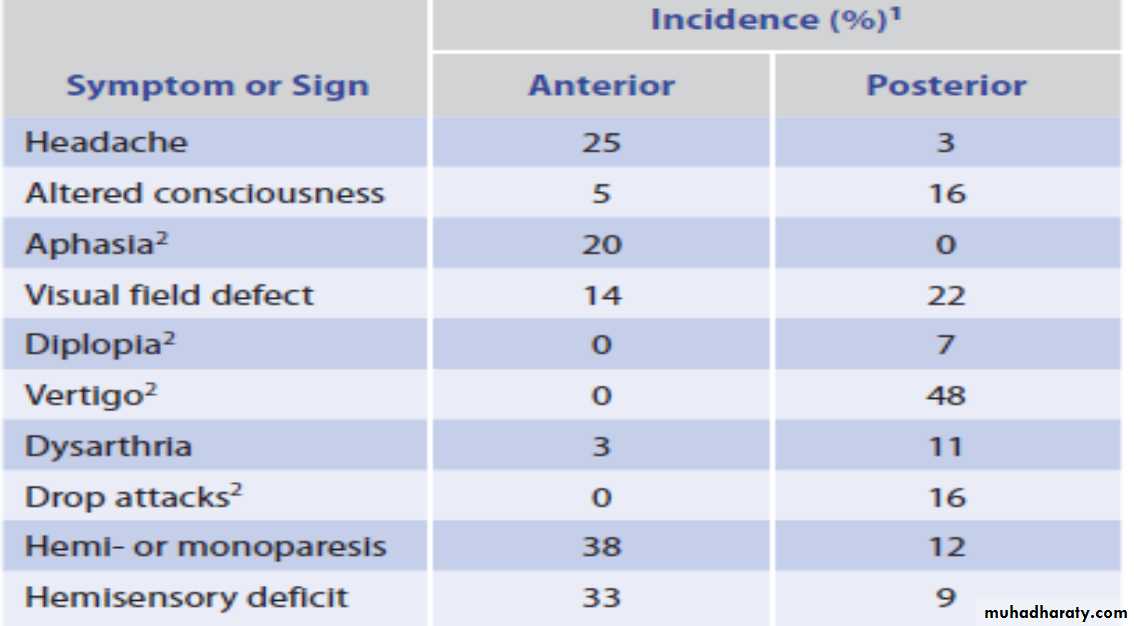
Symptoms and Signs of Anterior andPosterior Circulation Ischemia
Deficits may become maximal within several minutes of onset, typically in embolic stroke. Less often, deficits evolve slowly, usually over 24 to 48 h (called evolving stroke or stroke in evolution), typically in atherothrombotic stroke. In most evolving strokes, unilateral neurologic dysfunction (often beginning in one arm, then spreading ipsilaterally) extends without causing headache, pain, or fever.Progression is usually stepwise, interrupted by periods of stability.
Embolic strokes often occur during the day; headache may precede neurologic deficits. Thrombi tend to occur during the night and thus are first noticed on awakening
A seizure may occur at stroke onset, more often with embolic than thrombotic stroke. Seizures may also occur months to years later; late seizures result from scarring or hemosiderin deposition at the site of ischemia
Deterioration during the first 48 to 72 h after onset of symptoms, particularly progressively impaired consciousness, results more often from cerebral edema than from extension of the infarct.
Unless the infarct is large or extensive, function commonly improves within the first few days; further improvement occurs gradually for up to 1 yr.
Diagnosis
Primarily clinical evaluationNeuroimaging and bedside glucose testing
Evaluation to identify the cause
Sudden neurologic deficits referable to a specific arterial territory
Headache, coma or stupor, and vomiting are more likely with hemorrhagic strokeSeveral terms have been used to classify strokes, often based on the duration and evolution of symptoms
Transient ischaemic attack (TIA) describes a stroke in which symptoms resolve within 24 hours – an arbitrary cut-off that has little value in practice, apart from perhaps indicating that underlying cerebral haemorrhage or extensive cerebral infarction is extremely unlikely. The term TIA traditionally also includes patients with amaurosis fugax, usually due to a vascular occlusion in the retina.
Several terms have been used to classify strokes, often based on the duration and evolution of symptoms
Stroke describes those events in which symptoms last more than 24 hours.
The differential diagnosis of patients with symptoms lasting a few minutes or hours is similar to those with persisting symptoms.
The term ‘minor stroke’ is sometimes used to refer to symptoms lasting over 24 hours but not causing significant disability.
Progressing stroke (or stroke in evolution) describes a stroke in which the focal neurological deficit worsens after the patient first presents. Such worsening may be due to increasing volume of infarction, haemorrhagic
transformation or increasing cerebral oedema.
Completed stroke describes a stroke in which the focal deficit persists and is not progressing.
Differential diagnosis of stroke and transientischaemic attack
Differential diagnosis of stroke and transientischaemic attackCharacteristic features of stroke and non-strokesyndromes (‘stroke mimics’)
Investigation of a patient with an acute strokeInvestigation of acute stroke aims to
Confirm the vascular nature of a lesion Distinguish infarction from haemorrhage Identify the underlying vascular disease and risk factors
Investigation of a patient with an acute stroke
Prognosis
Stroke severity and progression are often assessed using standardized measures such as the National Institutes of Health (NIH) Stroke Scale (the score on this scale correlates with extent of functional impairment and prognosis.
During the first days, progression and outcome can be difficult to predict
Older age, impaired consciousness, aphasia, and brain stem signs suggest a poor prognosis.Early improvement and younger age suggest a favorable prognosis.
Complete neurologic recovery occurs in about 10%
About 50% of patients with moderate or severe hemiplegia and most with milder deficits have a clear sensorium and eventually can take care of their basic needs and walk adequatelyUse of the affected limb is usually limited, and most deficits that remain after 12 mo are permanent
Subsequent strokes often occur, and each tends to worsen neurologic function
About 20% of patients die in the hospital; mortality rate increases with age
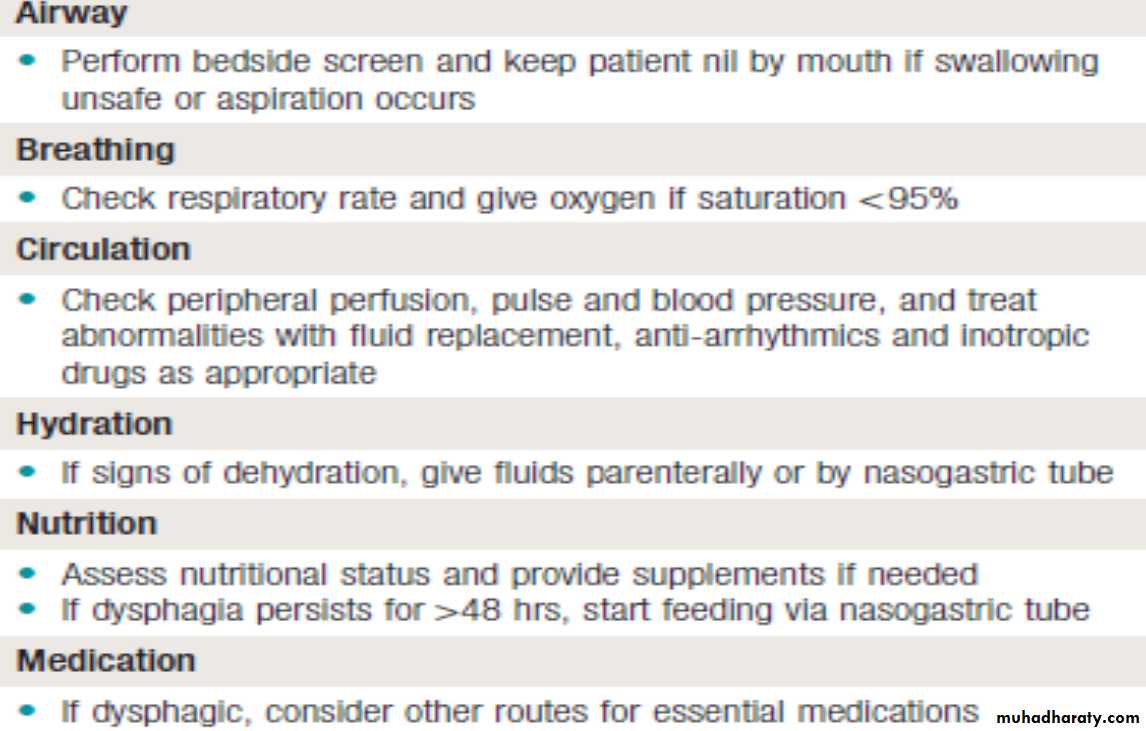
Treatment
General stroke treatmentsAcute antihypertensive therapy only in certain circumstances
Antiplatelet therapy
Occasionally for acute treatment, reperfusion (eg, recombinant tissue plasminogen activator [tPA] or thrombolysis-in-situ)
Sometimes anticoagulation
Long-term control of risk factors
Sometimes carotid endarterectomy or stenting
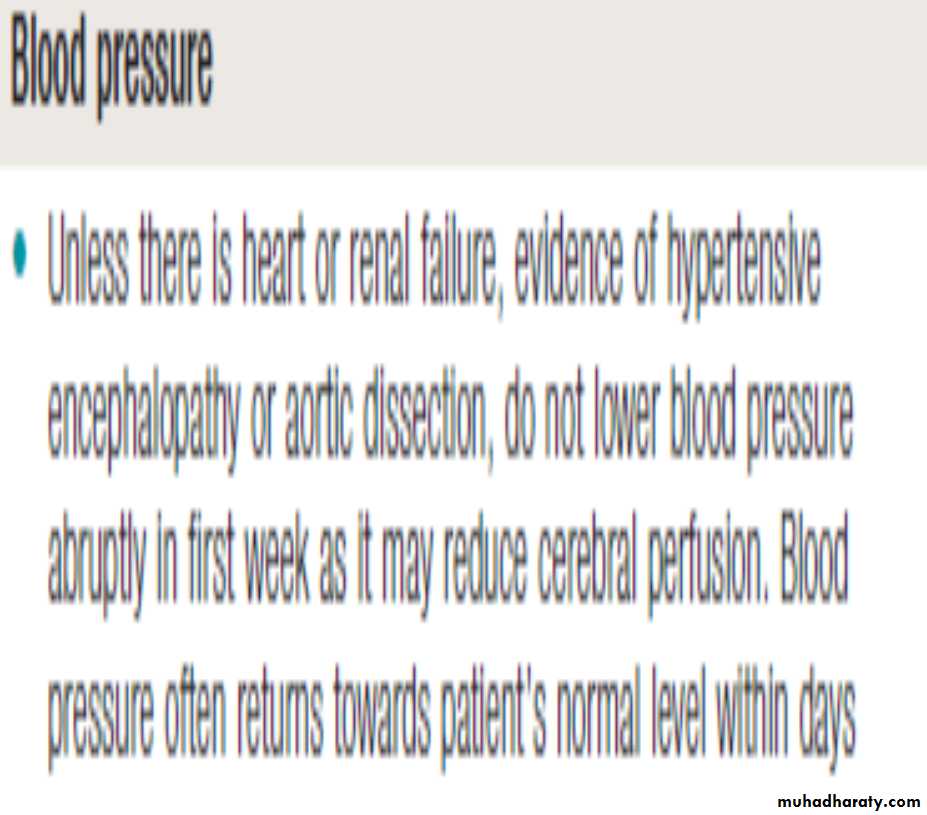
Perfusion of an ischemic brain area may require a high BP because autoregulation is lost; thus, BP should not be decreased except in the following cases
BP is > 220 mm Hg systolic or > 120 mm Hg diastolic on 2 successive readings >15 min apart.
There are signs of other end-organ damage (eg, aortic dissection, acute MI, pulmonary edema, hypertensive encephalopathy, retinal hemorrhages, acute renal failure).
Use of recombinant tPA is likely.
Recombinant tPA
Used for patients with acute ischemic stroke up to 4.5 h after symptom onset if they have no contraindications to tPA.Although tPA can cause fatal or other symptomatic brain hemorrhage, patients treated with tPA strictly according to protocols still have a higher likelihood of functional neurologic recovery
Before treatment with tPA, brain hemorrhage must be excluded by CT, systolic BP must be < 185 mm Hg, and diastolic BP must be < 110 mm Hg
Dose of tPA is 0.9 mg/kg IV (maximum dose 90 mg); 10% is given by rapid IV injection, and the remainder by constant infusion over 60 min. Vital signs are closely monitored for 24 h after treatment, and BP is maintained below 185 mm Hg systolic and 110 mm Hg diastolic.
Any bleeding complications are aggressively managed.
Anticoagulants and antiplatelet drugs are not used within 24 h of treatment with tPA.
Thrombolysis-in-situ (angiographically directed intra-arterial thrombolysis)
Sometimes used for major strokes if symptoms began >3 h but < 6 h ago, particularly for strokes due to large occlusions in the middle cerebral artery.Clots in the basilar artery may be intra-arterially lysed up to 12 h after stroke onset, sometimes even later depending on the clinical circumstances
Often used as rescue treatment for patients who have had a severe stroke and have an NIH stroke score ≥ 8 when IV and/or intra-arterial thrombolysis has been ineffective; it must be done within 8 h of symptom onset
Anticoagulation
Used for stroke caused by cerebral venous thrombosis and is sometimes used for emboli due to atrial fibrillation and for stroke due to presumed progressive thrombosis if it continues to evolve despite use of antiplatelet drugs and cannot be treated any other way (eg, with tPA or invasive methods).Warfarin is begun simultaneously with heparin. Before anticoagulation, hemorrhage must be excluded by CT.
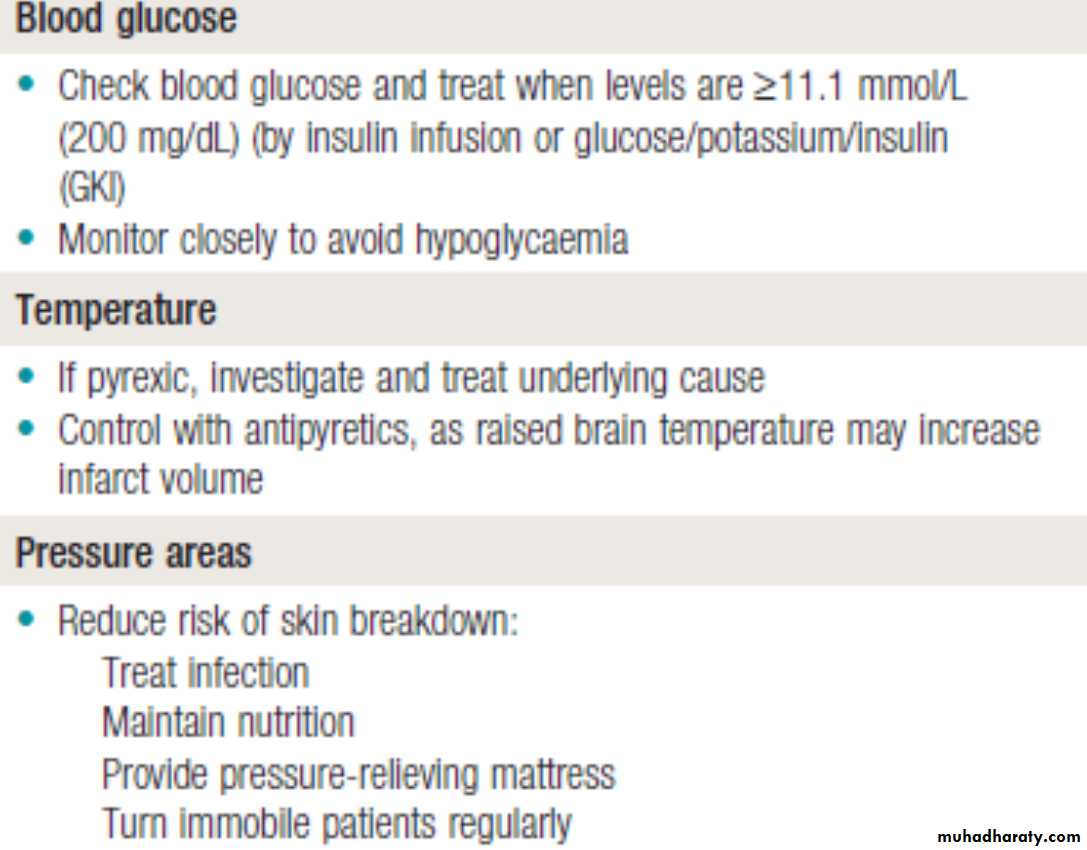
Long term
Supportive care is continued during convalescence.Controlling hyperglycemia and fever can limit brain damage after stroke, leading to better functional outcomes.
Long-term management also focuses on prevention of recurrent stroke (secondary prevention)
Modifiable risk factors (eg, hypertension, diabetes, smoking, alcoholism, dyslipidemia, obesity) are treated.
Reducing systolic BP may be more effective when the target BP is < 120 mm Hg rather than the typical level (< 140 mm Hg).
Extracranial carotid endarterectomy or stenting
Extracranial vertebral angioplasty and/or stentingIntracranial major artery angioplasty and/or stenting
Oral antiplatelet drugs
Used to prevent subsequent noncardioembolic (atherothrombotic, lacunar, cryptogenic) strokes (secondary prevention).Aspirin 81 or 325 mg once/day, clopidogrel 75 mg once/day, or the combination product aspirin 25 mg/extended-release dipyridamole 200 mg bid may be used.
Ticlopidine 250 mg bid
Oral anticoagulants
For secondary prevention of cardioembolic strokes (as well as primary prevention). Adjusted-dose warfarin (a vitamin K antagonist) with a target INR of 2 to 3 is used for certain patients with nonvalvular or valvular atrial fibrillation.A target INR of 2.5 to 3.5 is used if patients have a mechanical prosthetic cardiac valve.
Statins
Used to prevent recurrent strokes; lipid levels must be decreased by substantial amounts.Atorvastatin 80 mg once/day is recommended for patients with evidence of atherosclerotic stroke and LDL (low-density lipoprotein) cholesterol ≥ 100 mg/dL.
A reasonable LDL cholesterol target is a 50% reduction or a level of < 70 mg/dL.
Other statins (eg, simvastatin, pravastatin) may be also used.
Transient Ischemic Attack (TIA)
Focal brain ischemia that causes sudden, transient neurologic deficits and is not accompanied by permanent brain infarction (eg, negative results on diffusion-weighted MRI).
TIA is similar to ischemic stroke except that symptoms usually last < 1 h; most TIAs last < 5 min. Infarction is very unlikely if deficits resolve within 1 h
As shown by diffusion-weighted MRI and other studies, deficits that resolve spontaneously within 1 to 24 h are often accompanied by infarction and are thus no longer considered TIAs