
Orthopaedic surgery
فرع الجراحه
\
كلية طب الموصل
upper limbs trauma 1
د
.
ساهر حبيب
دكتوراه
(
بورد
)
اختصاص جراحة العظام والكسور

The great impact of upper limb injuries is
stiffness
– particularly of the
shoulder but sometimes of the elbow and hand as well.
Two points should be constantly borne in mind:
• Whatever the injury, and however it is treated, all the joints that
are not actually immobilized – and especially the finger joints – should
be exercised from the start.
• In elderly patients it is sometimes best to disregard the fracture and
concentrate on regaining movement.
UPPER LIMB INJURIES
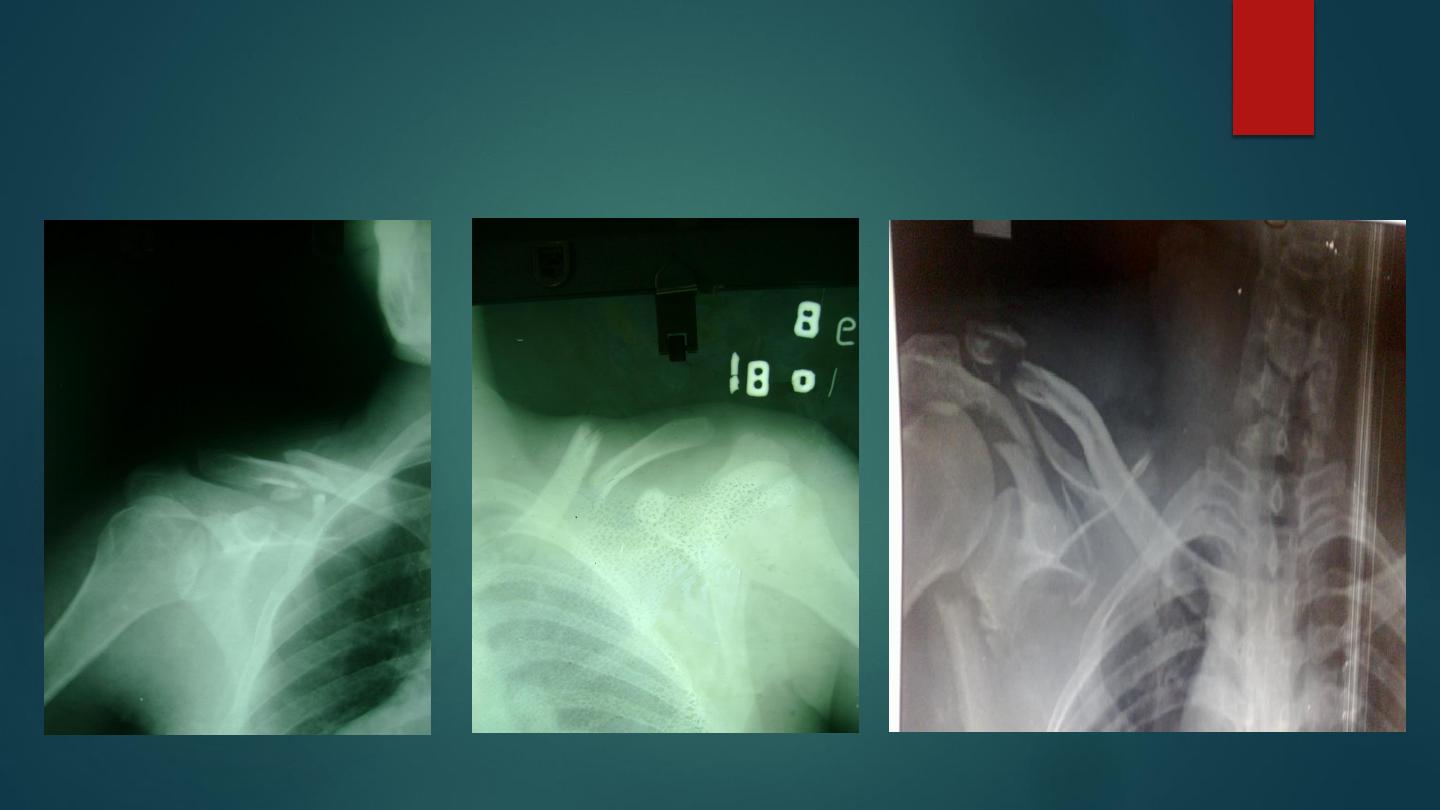
Fracture clavicle

Fracture clavicle is very common.
A fall on the shoulder or outstretched hand may break the clavicle in mid shaft, less
common outer end or medial end.
The arm is clasped to the chest to prevent movement, subcutaneous lump obvious,
occasionally sharp fragment threatens the skin.
Vascular complication is rare.
X-ray shows the site and displacement of the fractures, the lateral segment displaced
downward and medially.
Clavicle fractures are usually classified on the basis of their location: Group I )middle
third fractures), Group II (lateral third fractures) and Group III (medial third fractures).
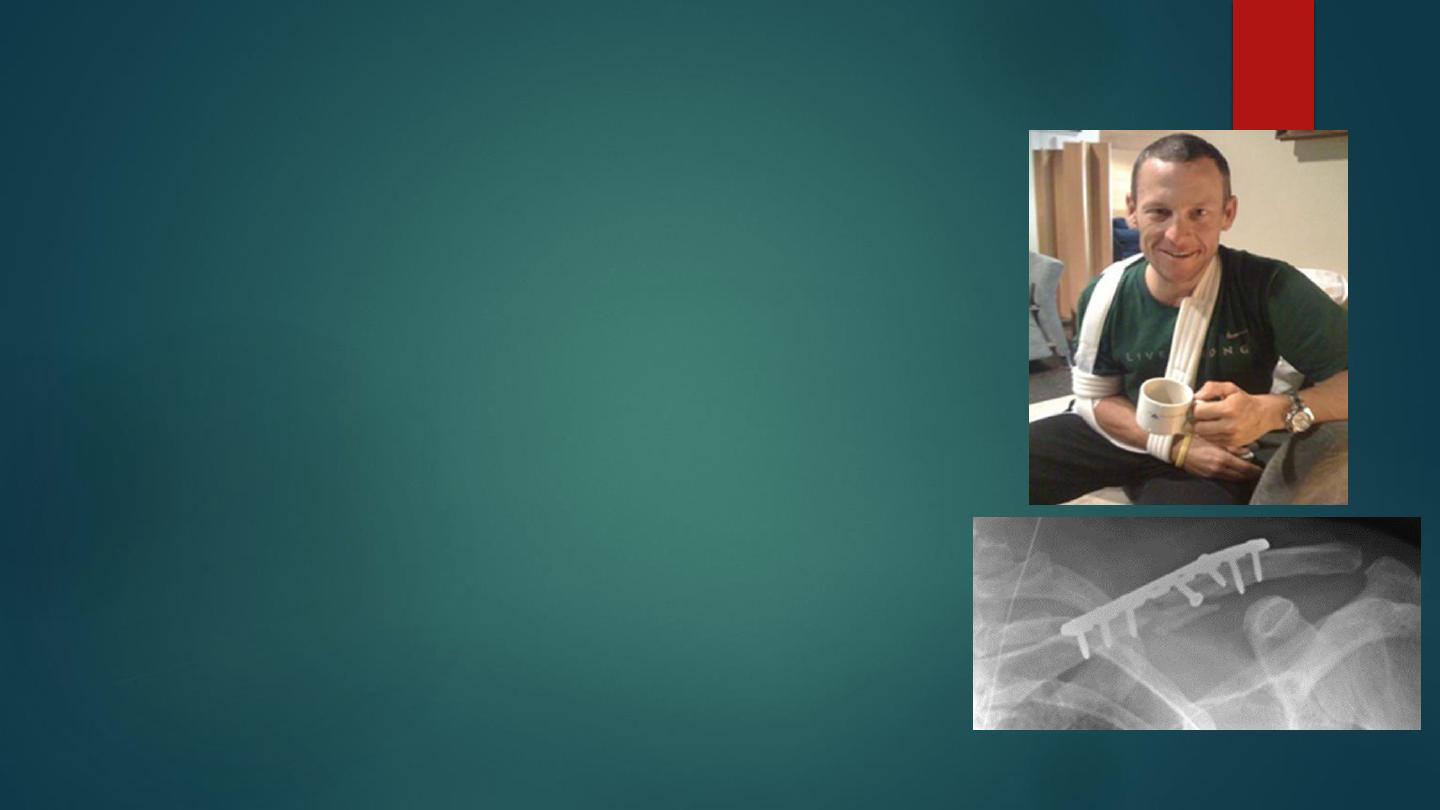
Treatment: Accurate closed reduction is neither possible
nor essential.
All that is needed is to support the arm in a simple sling
(2-3 weeks) to relieve pain, followed by active exercises.
Fracture of clavicle unite readily, with no disability.
In assessing clinical progress, remember that ‘clinical’
union usually precedes ‘radiological’ union by several
weeks.
Internal fixation rarely used if there neurovascular injury
or skin penetration, or severely displaced fracture in outer
third of clavicle.
The early complication include injuries to subclavian
artery , brachial plexus , pneumothorax , all are rare .
late complication are malunion, stiffness of the shoulder
and nonunion .

Sternoclavicular dislocation.
The medial end of clavicle may displaced
forwards, this injury is uncommon, very
rarely the displacement posteriorly press
on trachea and vessels.
Anterior displacement treated easily by
reduction by direct pressure followed by
local plaster pad and sling for two weeks,
but recurrence is common and need no
treatment.
The posterior type need urgent operative
treatment and medial end pulled foreword
with towel clip in operating room with
assistant of thoracic surgeon.

Acromio-clavicular dislocation
and subluxation
It is common injury ,A fall on the shoulder with the arm
adducted may strain or tear the acromioclavicular ligaments
and upward subluxation of the clavicle may occur; if the force
is severe enough, the coracoclavicular ligaments will also be
torn, resulting in complete dislocation of the joint.
Type I is an acute sprain of the acromioclavicular ligaments; the joint is
undisplaced. In Type II the acromioclavicular ligaments are torn and the joint
is subluxated with slight elevation of the clavicle. In Type III the
acromioclavicular and coracoclavicular ligaments are torn and the joint is
dislocated; the clavicle is elevated (or the acromion depressed) creating a
visible and palpable ‘step’. Other types of displacement are less common, but
occasionally the clavicle is displaced posteriorly (Type IV), very markedly
upwards (Type V) or inferiorly beneath the coracoid process (Type VI).

Treatment:
depends on degree of displacement ( type 1,2,3): subluxation and
mild dislocation treated by analgesia and sling for 2 weeks,
while severely displaced (4,5,6) dislocation treated by surgical
reduction and fixation.
Complications : rotator cuff syndrome, secondary osteoarthritis
,unreduced dislocation and ossifications of ligaments.
Fractures of the scapula
Fractures of the scapula are
uncommon.
Result from direct severe trauma,
might affect neck of the scapula ,
glenoid, coracoid, acromion
process or body .
might associated with chest injury
and rib fractures.
Usually treated by sling for 2-3
weeks followed by active
exercises,
operative treatment rarely used.

Dislocation of the shoulder
Dislocation of the shoulder is common in
adults, it might be anterior ( common) or
rarely posterior.
Of the large joints the shoulder is the one
that most commonly dislocate it is due to
the following :
shallowness of the glenoid, extraordinary
range of movement, ligament laxity, or
glenoid dysplasia.
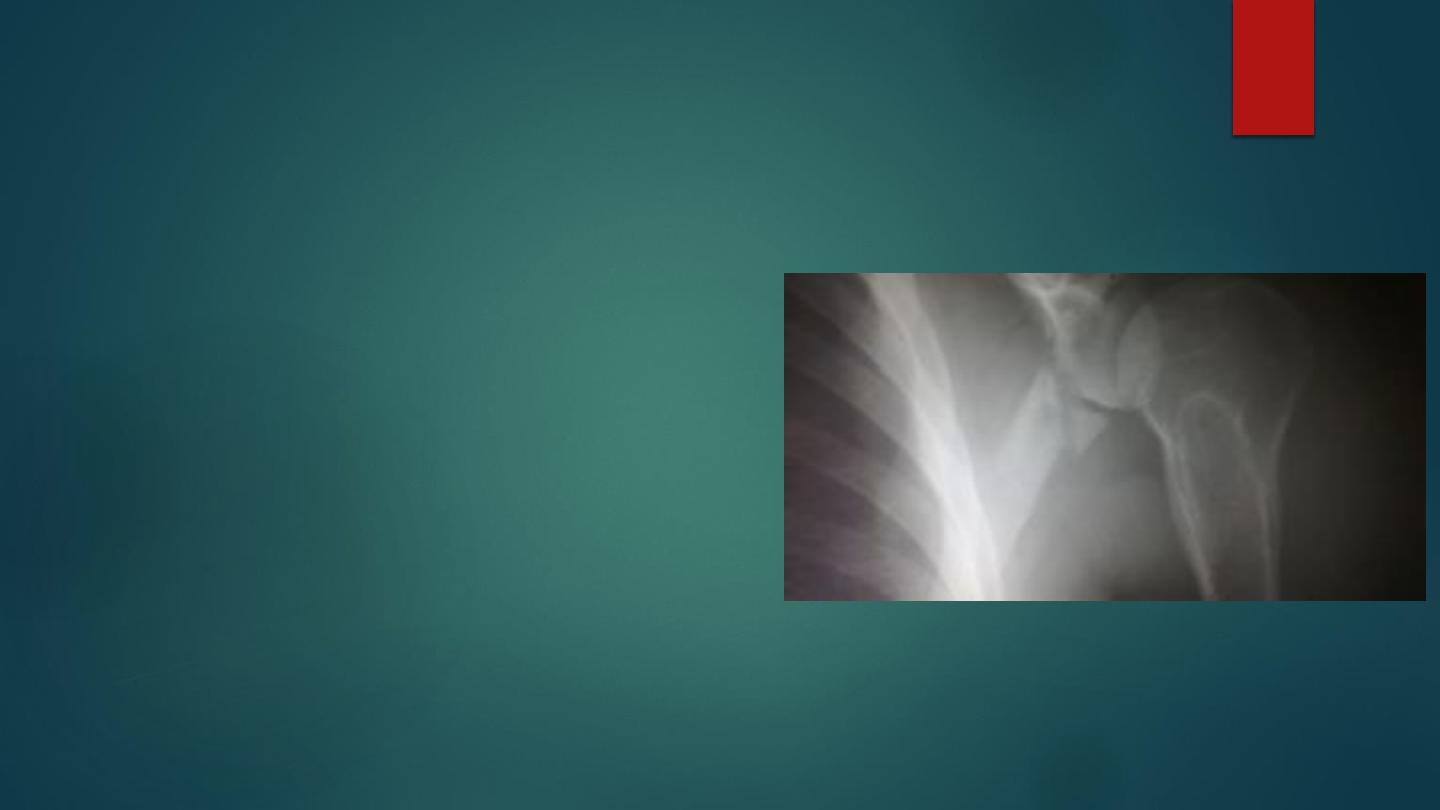
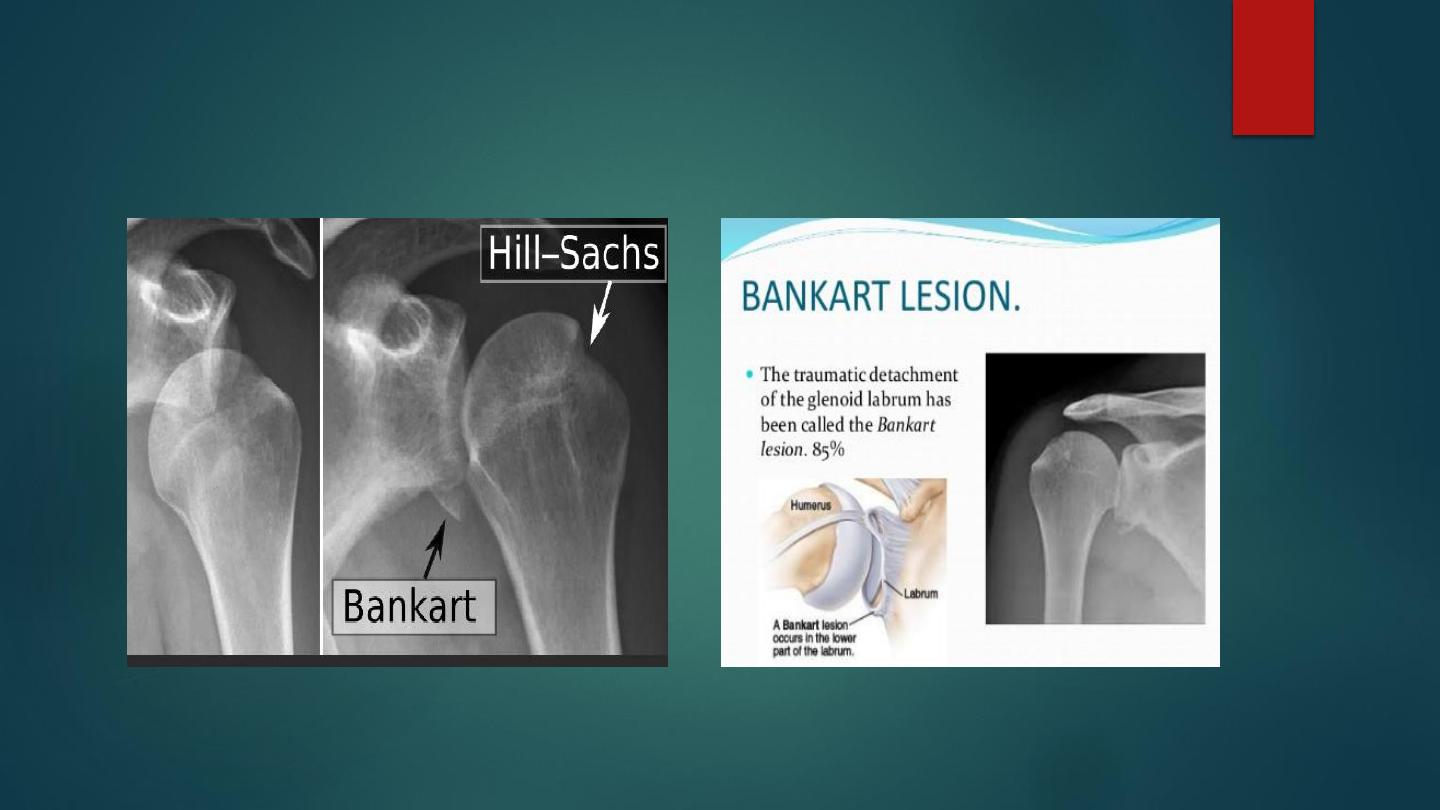
Anterior dislocation
Dislocation is usually caused by a fall on the outstretched hand. The
head of the humerus is driven forward, tearing the capsule and producing
avulsion of the glenoid labrum (the Bankart lesion). Occasionally the
posterolateral part of the head is crushed (Hill sach lesion ).
Rarely, the acromion process levers the head downwards and the joint
dislocates with the arm pointing upwards (luxatio erecta); nearly always
the arm then drops, bringing the head to its subcoracoid position
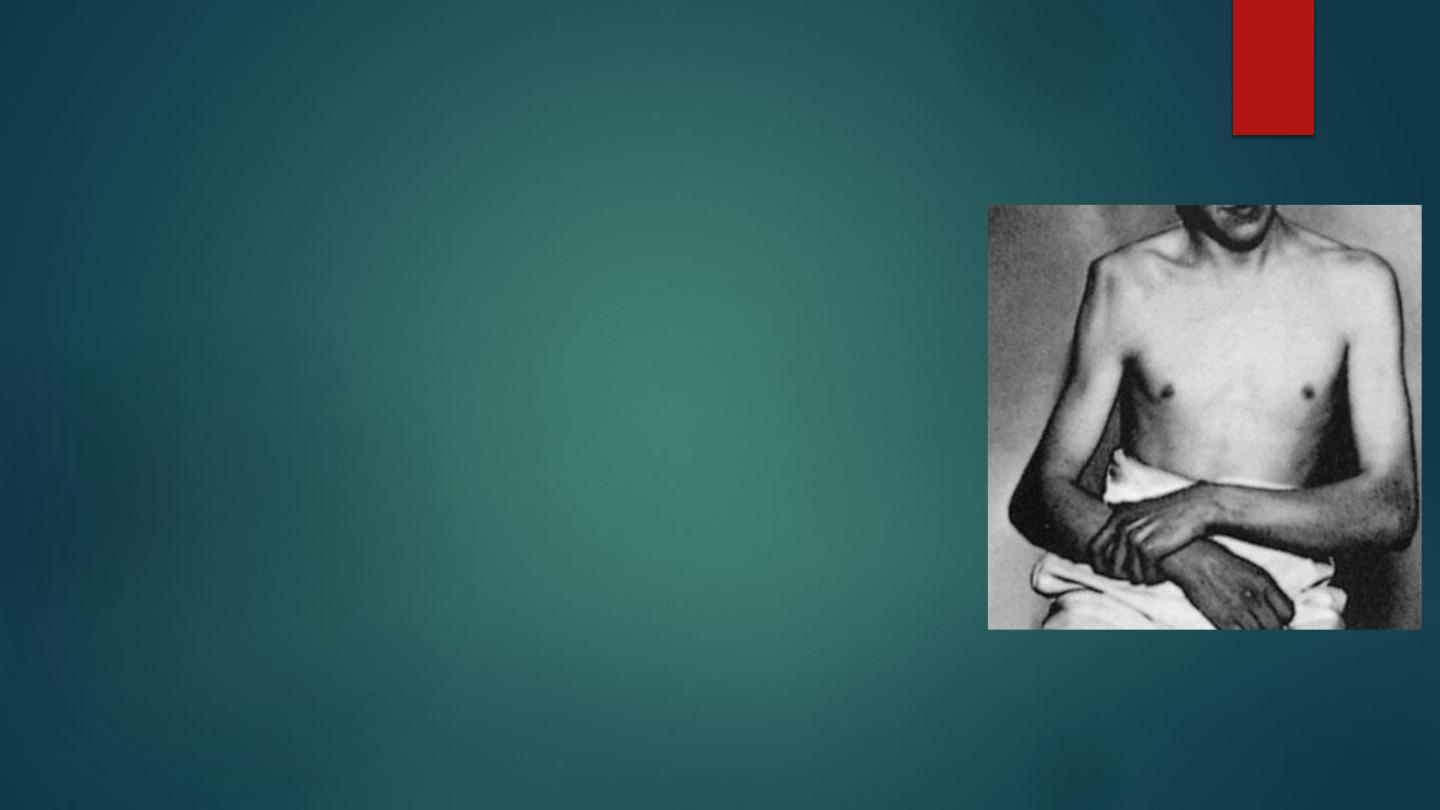
Clinical features: Pain is sever. Patient support the arm with the opposite
hand and prevent any kind of movement . Flattened lateral outline of
shoulder and prominent tip of shoulder, bulge below the clavicle are
other features. Examination for axillary nerve and nearby blood vessels
is important.
Radiological examination in anteroposterior views , Head usually lying
below and medial to the glenoid.

Treatment
reduction should be done as soon as possible, with sedation and possibly GA
three techniques used:
1.
Stimsons’ technique: Patient is left prone with the arm hanging over the side of the
bed. after 15-20 min the shoulder may reduce spontaneously, or with some traction .
2.
Hippocratic method: Gently increasing traction is applied to the arm with the shoulder
is slight abduction, Counter traction either by assistant with towel slung or the foot of
the examiner.
3.
Kochers’ method: Under general anesthesia with assistant, elbow is flexed 90 degree
and held close to the body, the arm slowly rotated 75 degree externally, the elbow is
lifted forwards, finally the arm is rotated medially.
The arm rest in sling for one week if age more than 30 years and 3 weeks if age less than
30 years, Then movement started with avoidance abduction and lateral rotation.
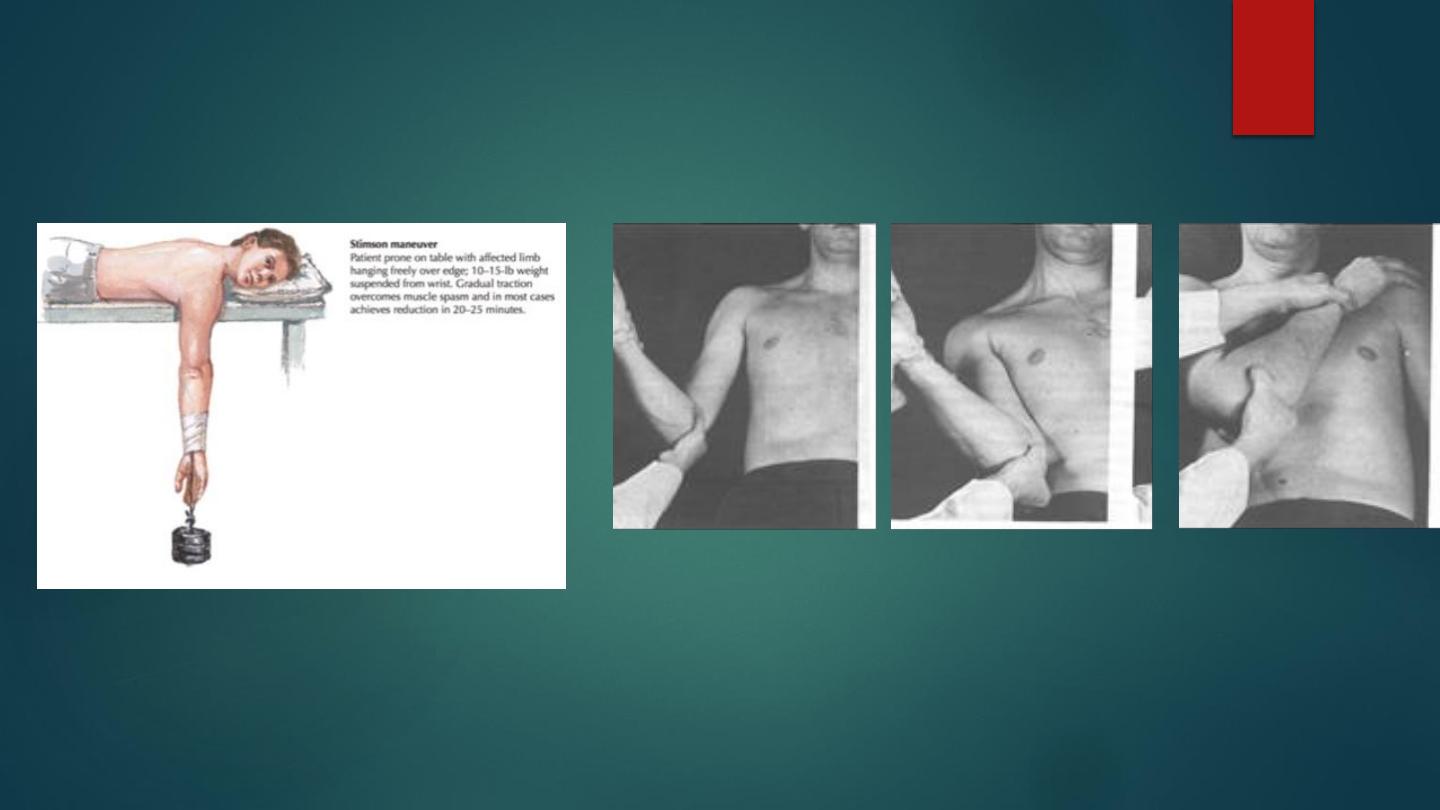
Sitmsons
kocher method
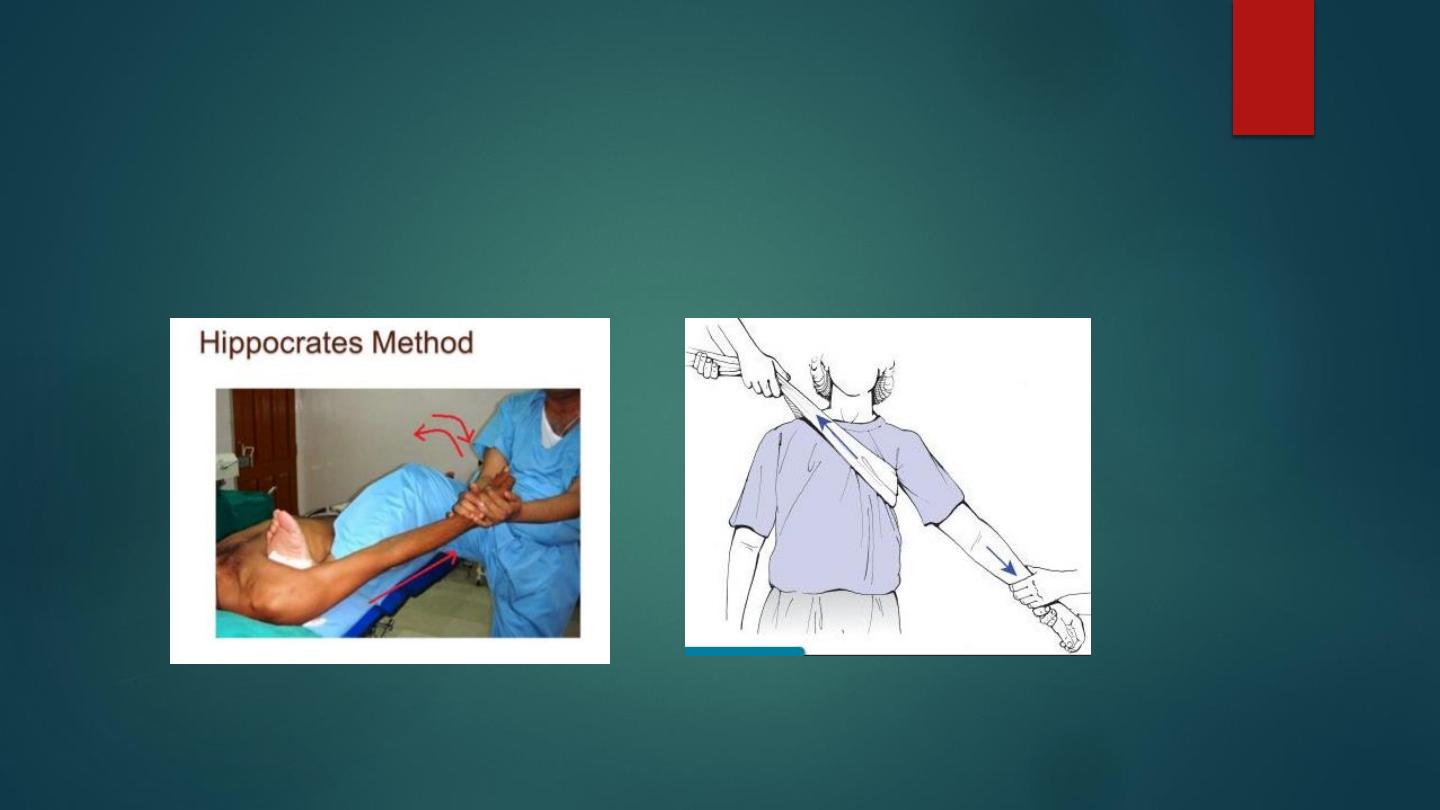
Hippocratic method
Hippocratic method

Complications
Early:
1- Rotator cuff tear.
2- Axillary Nerve injury.
3- Vascular injury
4- Fracture dislocations of the proximal humerus and associated fractures.
Late:
1- Recurrent dislocation, more common in young patients, diagnosis depend on
history. MRI, CT , and arthroscopy might demonstrate clearly the cause of recurrence.
If shoulder recurred more than 3 times and cause significant symptoms the treatment is
surgical, many surgical technique used including Putti-Platt, Bankart, and arthroscopic
reconstruction .
2- Shoulder stiffness in patients older than 40 years.
3- Unreduced dislocation.
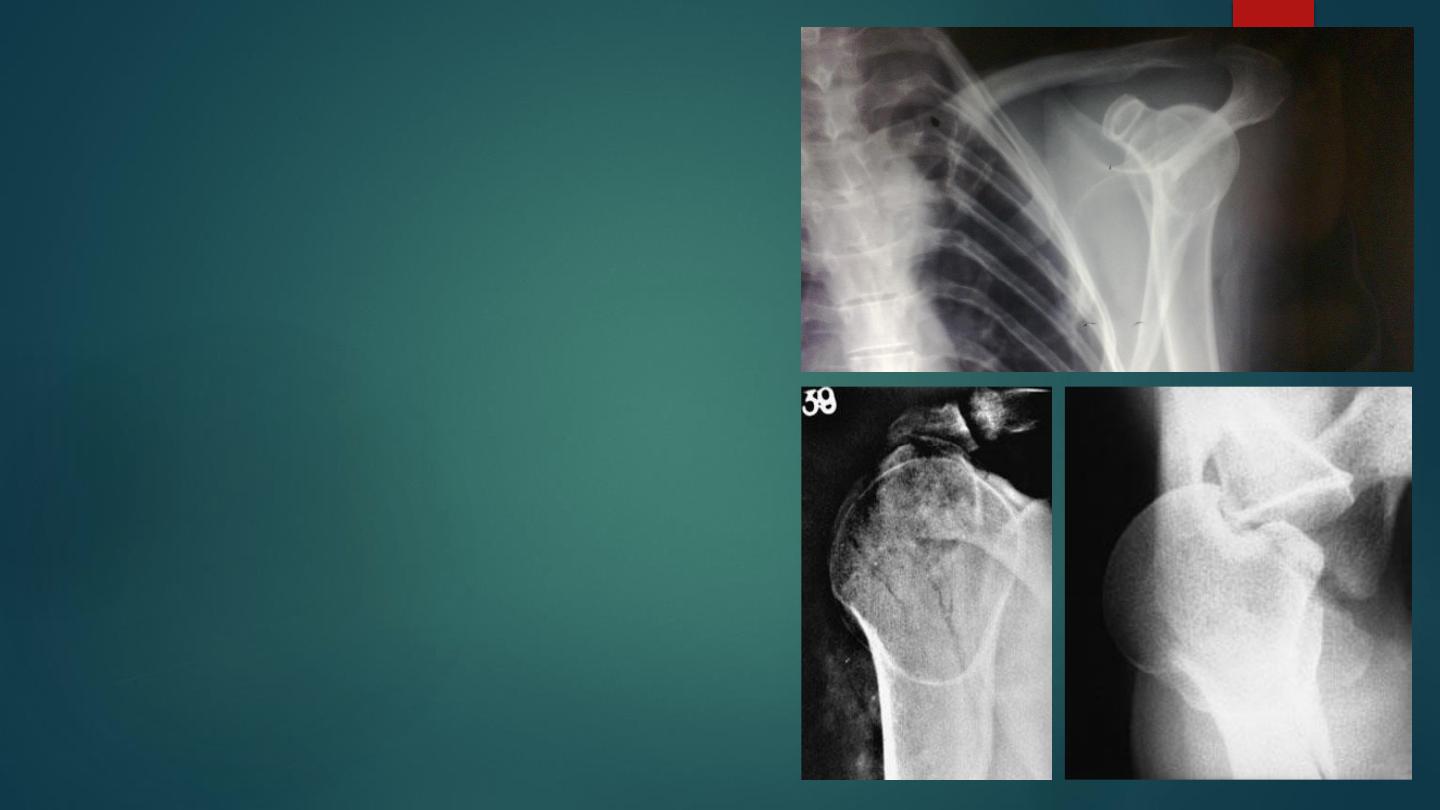
Posterior dislocation of the
shoulder
It is rare type , result from direct blow to anterior
of the shoulder or by forceful internal rotation
like epileptic fit or electroconvulsive therapy.
It is easily missed, there is fixed internal rotation.
X-ray in anteroposterior view easily misleading
and give feature of electrical pulp sign, the
diagnostic view is the axillary view .
Reduction achieved by rotating the arm laterally
with longitudinal traction , sometime direct
forward pressure applied to displaced the humeral
head.

Fractures of proximal humerus
Fractures of the proximal humerus usually occur after middle age
and most of the patients are osteoporotic, postmenopausal women.
Fracture displacement is usually not marked and treatment presents
few problems. However, in about 20 per cent of cases there is
considerable displacement of one or more fragments and a
significant risk of complications due to bone fragility, damage to the
rotator cuff and the prevailing co-morbidities. Deciding between
operative and nonoperative treatment can be very difficult.

The most widely accepted classification is that of Neer (1970)
who drew attention to the four major segments involved in these
injuries:
the head of the humerus, the lesser tuberosity, the greater
tuberosity and the shaft
. Neer’s classification distinguishes
between the number of displaced fragments, with displacement
defined as greater than 45 degrees of angulation or 1cm of
separation. Thus, however many fracture lines there are, if the
fragments are undisplaced it is regarded as a one-part fracture; if
one segment is separated from the others, it is a two-part fracture;
if two fragments are displaced, that is a three-part fracture; if all
the major parts are displaced, it is a four-part fracture.
Furthermore, a fracture-dislocation exists when the head is
dislocated and there are two, three or four parts. This grading is
based on x-ray appearances, although observers do not always
agree with each other on which class a particular fracture falls
into.
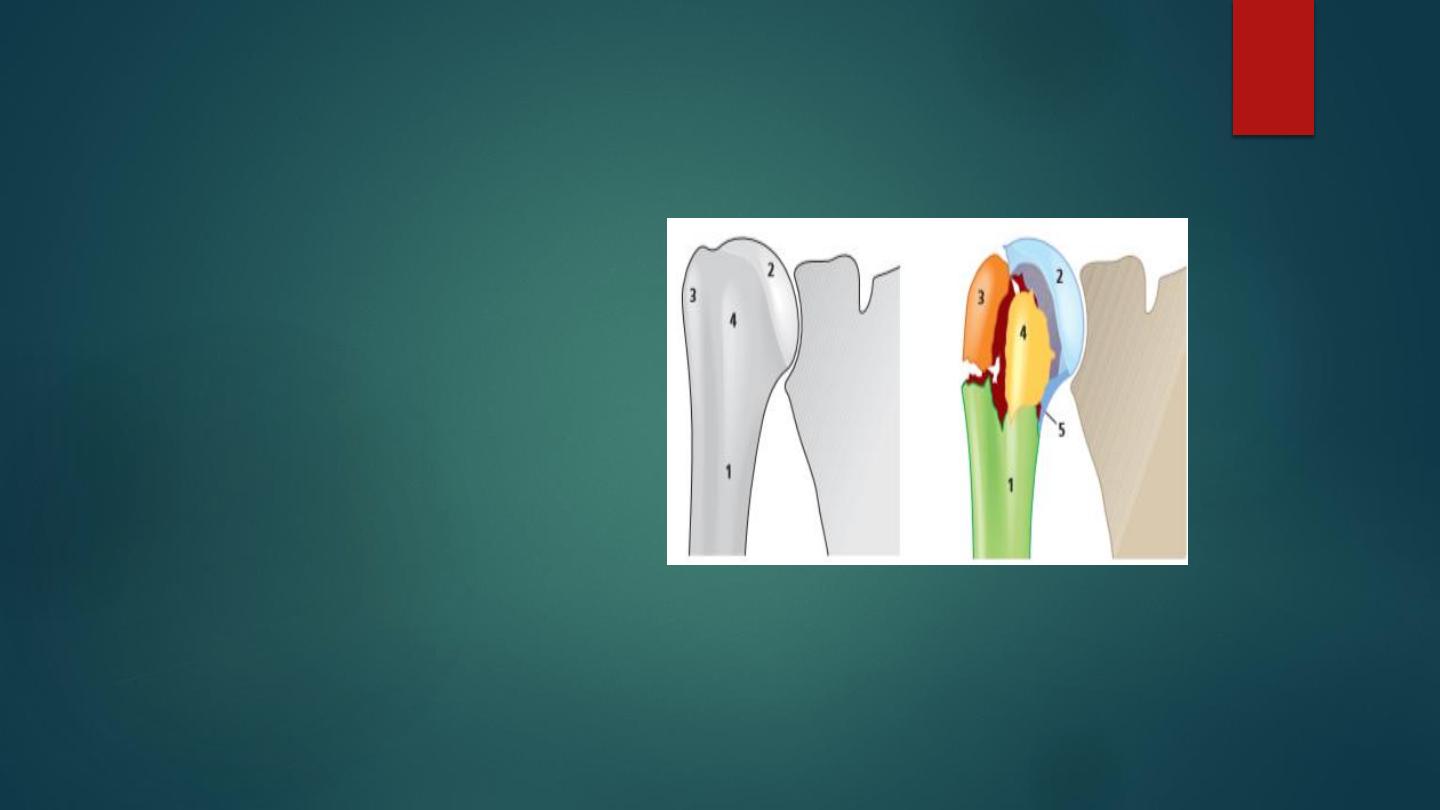
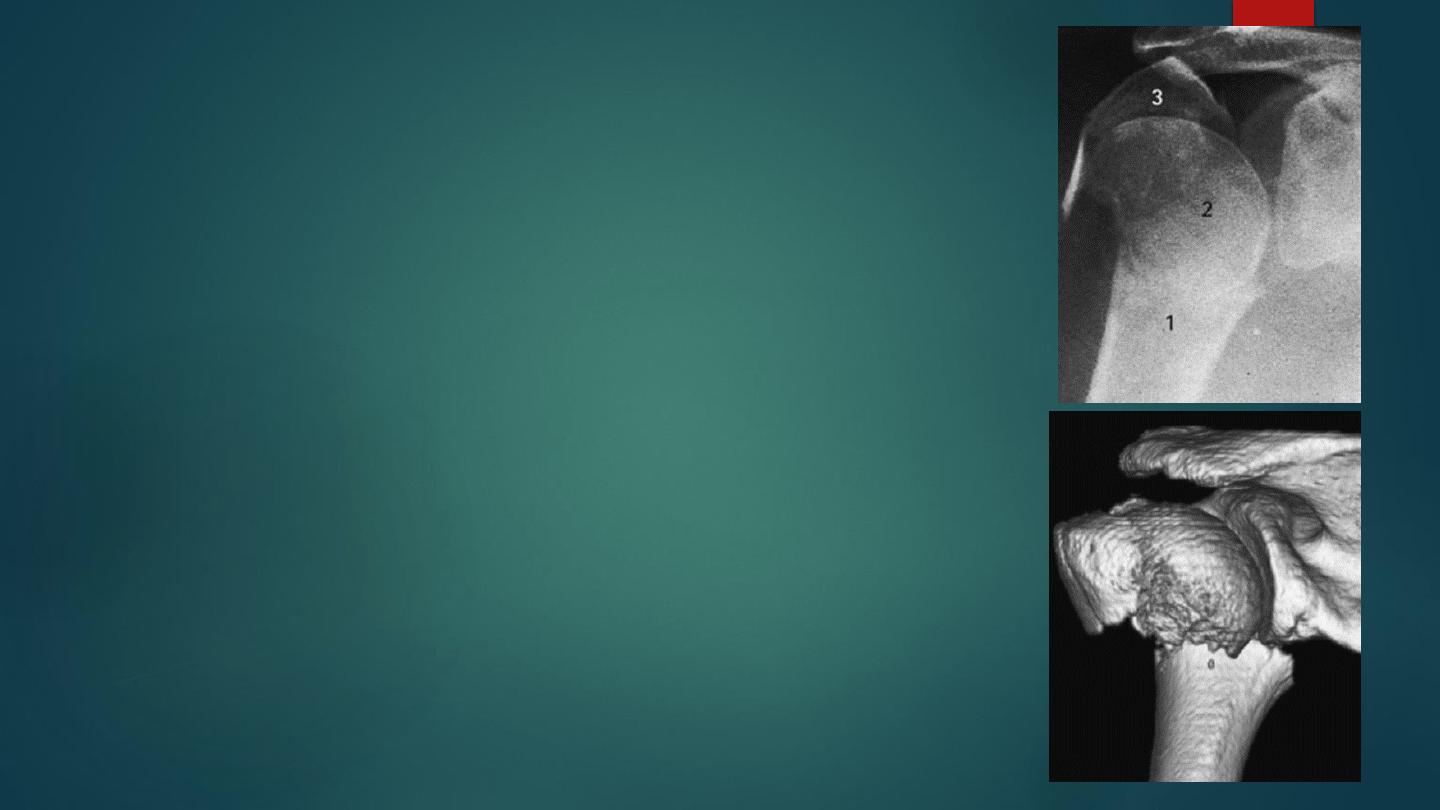
Fractures of the proximal
humerus Diagram of (a) the
normal and (b) a fractured
proximal humerus, showing the
four main fragments, two or
more of which are seen in
almost all proximal humeral
fractures. 1=shaft of humerus;
2=head of humerus; 3=greater
tuberosity; 4=lesser tuberosity.

Fractures of the greater tuberosity of the
humerus.
May result from fall on shoulder in
elderly, or associated with shoulder
dislocation.
Treatment depend on displacement,
undisplaced fracture treated by sling
for 3 weeks and active exercises.
If fragment is separated more than
5mm and angulated more than 45
degrees so it should be treated by
open reduction and internal fixation
by screw , to avoid impairment of
shoulder abduction.

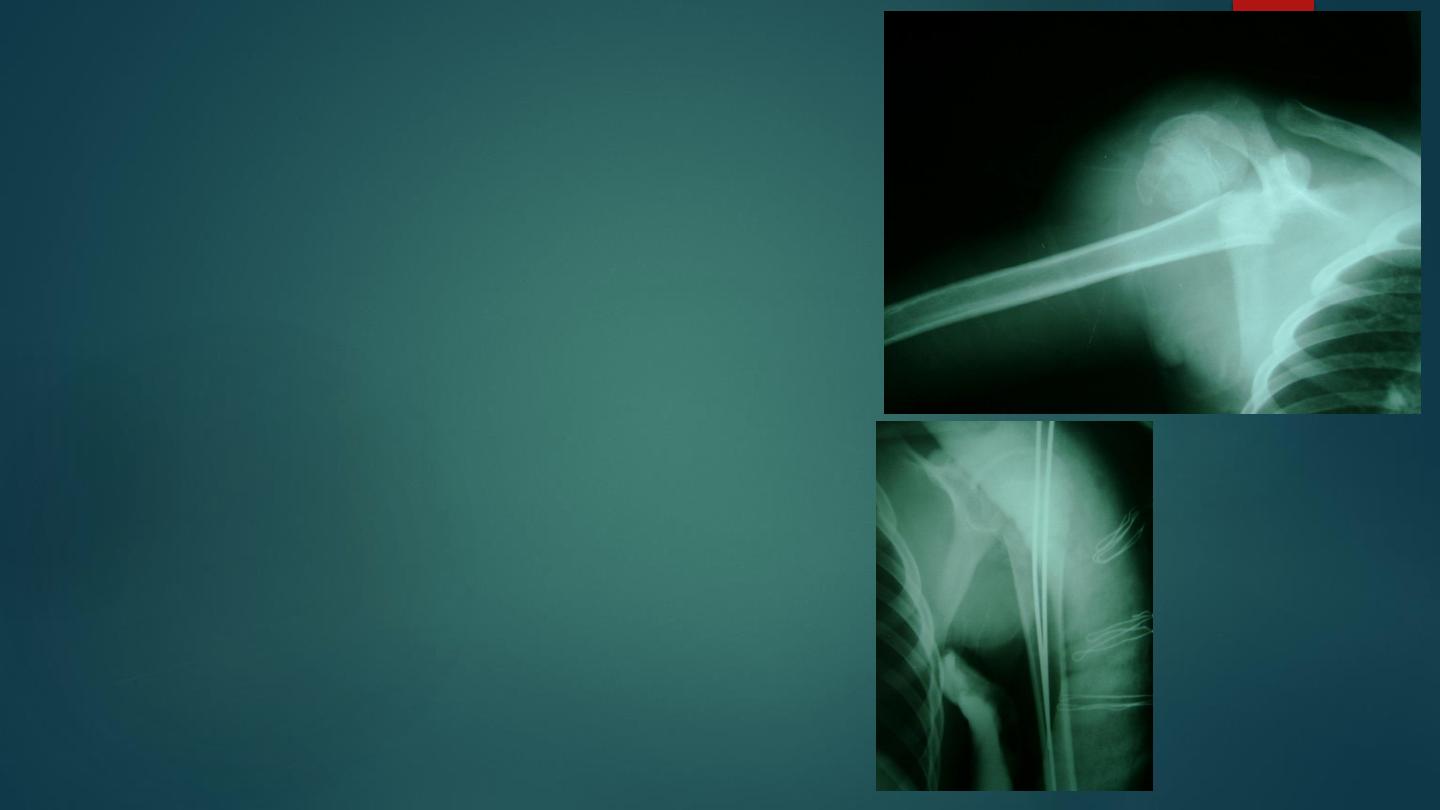
Fractures of the neck of the humerus
It occur commonly in elderly, as result of fall onto the
limb, in young patients result from severe trauma.
The displacement is variable, or may impacted. There is
history of trauma, pain, swelling , bruises , tenderness
and inability to move arm, distal blood vessels and
nerves must be examined .
X-ray shows the fracture , the pattern of displacement ,
and to exclude associated dislocation .
Treatment of proximal
humerus fractures
Minimally displaced or impacted fracture (majority) need
only sling of the arm for 3 weeks until the pain subside and
then gentle active movement is encouraged .
If there is considerable displacement of fragments ,
manipulation is advised followed by sling of the arm for 4
weeks and assisted active exercises.
If the fracture is severely displaced or unstable open
reduction and internal fixation used and even prosthetic
replacement in elderly patients with comminuted fractures
and avascular necrosis .
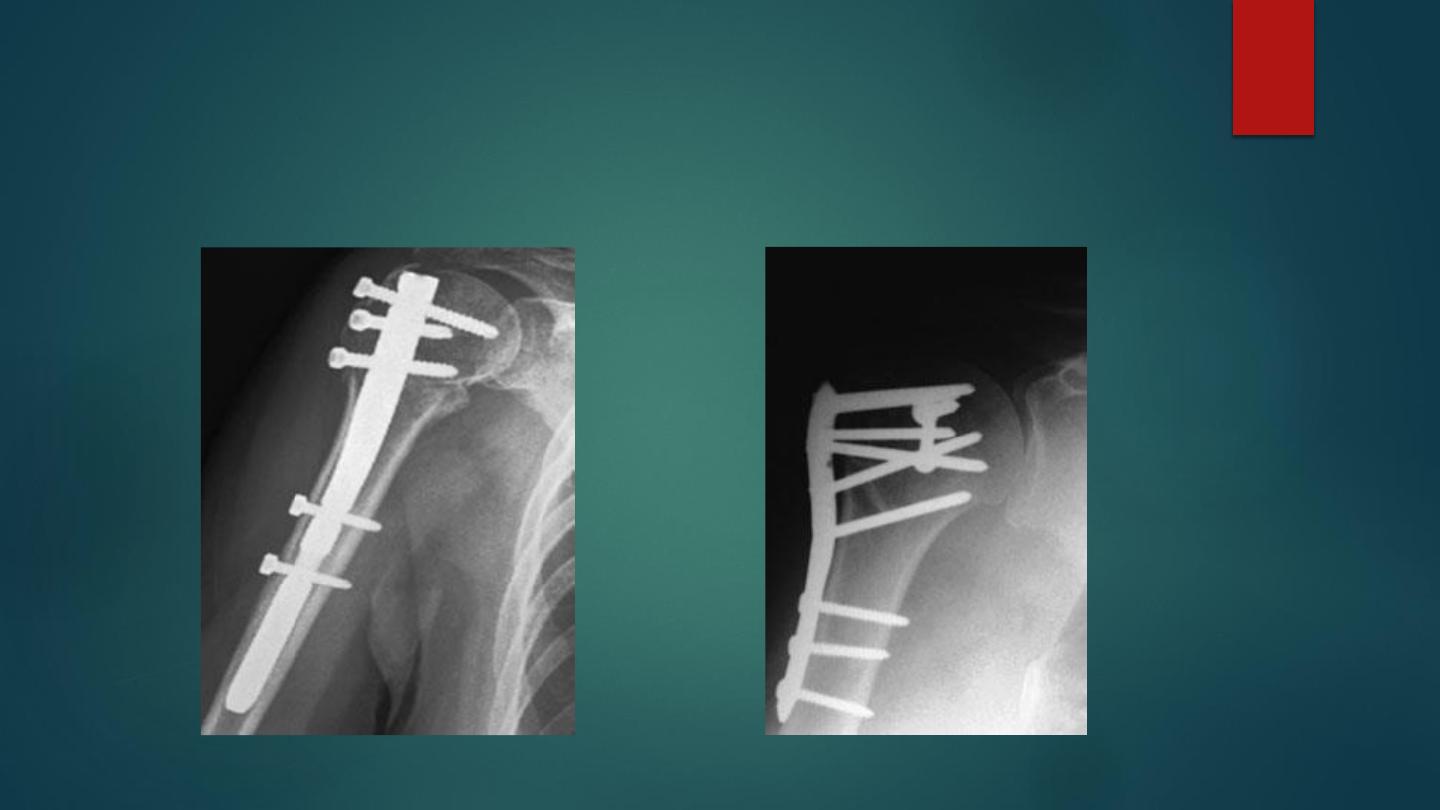
Humerus nail plate and screws
Complication
:
Early :
1- neurovascular injuries (axillary n. ,
a.).
2- Associated dislocation of
shoulder.
Late :
1- stiffness of the shoulder ; this can
minimized by early mobilization .
2- avascular necrosis of the head of the
humerus .