Primary amenorrhea
Presented by :Dr. Aseel Basim Al_taee
Definition
Amenorrhea is defined as the absence of menstrual bleeding and may be primary (never occurring) or secondary (cessation sometime after initiation).Cryptomenorrhea is another condition caused by anatomic disorders interfering with the outflow of menses, such as an imperforate hymen or transverse vaginal septum, although these women are actually menstruating.
primary amenorrhea
primary amenorrhea is lack of menstruation by age of 14 in the absence of secondary sexual characteristicsor
lack of menstruation by age of 16 in the presence of secondary sexual characteristics
(prevalence about 0.3%)
classification OF PRIMARY AMENORRHEA
Although numerous classifications have been used for the various causes of primary amenorrhea and all have their strengths and weaknesses.So The simple classification divides causes of amenorrhea into anatomic versus hormonal etiologies.
Other classification based on the presence or absence of secondary sexual characteristics.
Classification Scheme for Amenorrhea
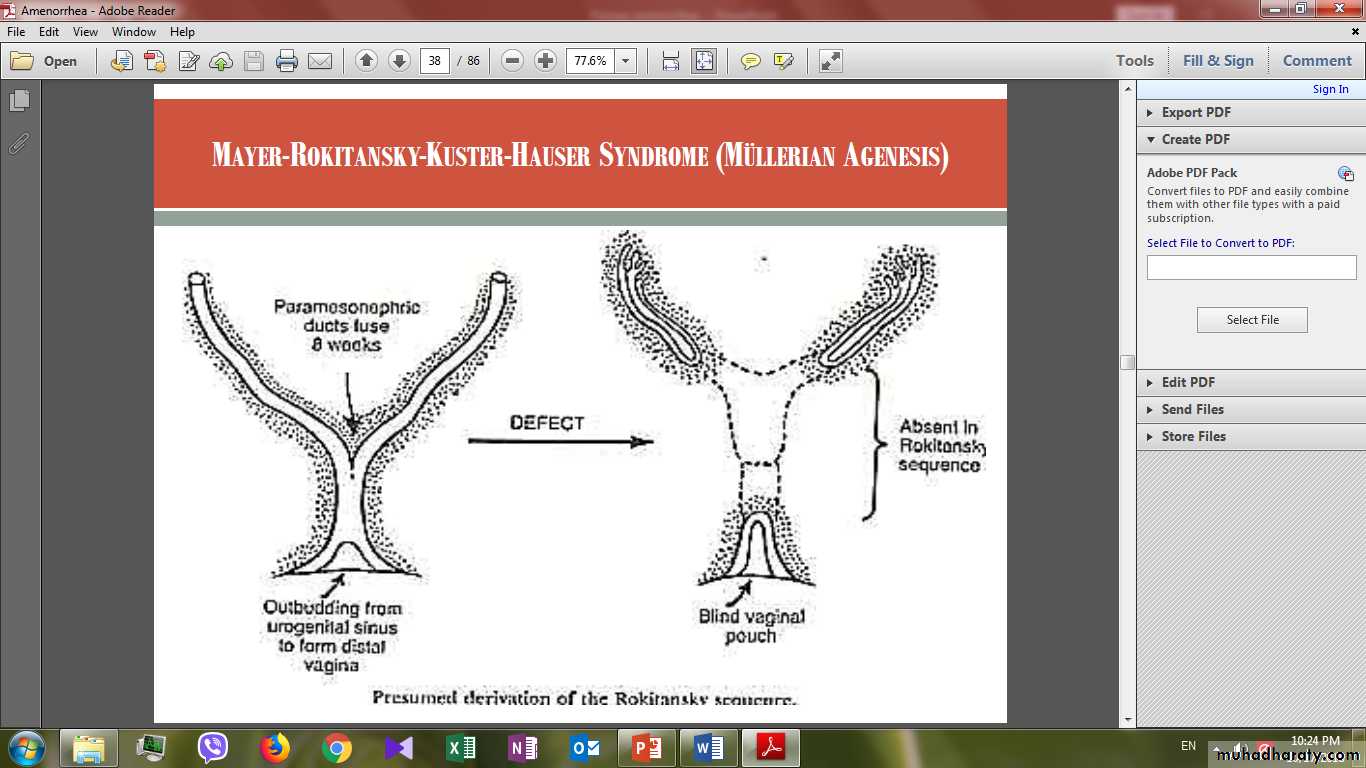
ANATOMICMüllerian agenesis (partial or complete) Mayer-Rokitansky-Kuster-Hauser (MRKH) syndrome
Cervical atresiaTransverse vaginal septum
Imperforate hymen
Complete androgen insensitivity. (Genetic male; mutation in androgen receptor).
Classification Scheme for Amenorrhea
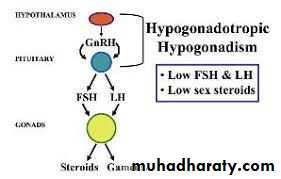
HORMONAL/ENDOCRINOLOGICHypogonadotropic hypogonadism
(Disorders of the hypothalamus )Constitutional delay.
Inherited/congenital (Kallmann syndrome )
Acquired (Eating disorders; Excessive exercise, Stress )
Destructive processes (Tumor, Radiation ,Trauma, Infection, Infiltrative disease).
Disorders of the anterior pituitary gland
Inherited/congenital (Pituitary hypoplasia)Acquired( Macroadenoma, Metastases ,Radiation, Trauma)
Other Causes
chronic diseases including end-stage kidney disease, liver disease.
Malignancies.
acquired immunodeficiency syndrome.
malabsorption syndromes.
Hypergonadotropic hypogonadism (POF)
Inherited/congenitalChromosomal (gonadal dysgenesis) Absence of two normal X chromosomes or mosaicism.( Turner syndrome).
Single gene disorders e.g. Fragile X
Acquired
Infectious
Autoimmune
Iatrogenic
Environmental
Idiopathic
EU gonadotropic amenorrhea
InheritedPolycystic ovarian syndrome
Adult-onset congenital adrenal hyperplasia
Acquired
Hyperprolactinemia
Thyroid disease
Cushing syndrome
Acromegaly
Ovarian tumors (steroid producing)
Surgical removal of the ovaries.
Exposure to radiation.
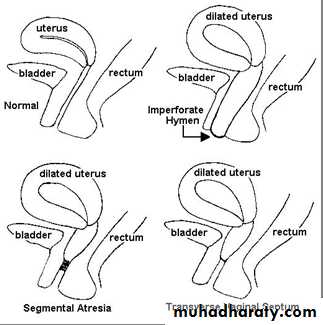
ANATOMIC DISORDERS
Lower Outflow Tract Obstruction
Amenorrhea is associated with imperforate hymen (1 in 2000 women), a complete transverse vaginal septum (1 in 70,000 women).
Patients with outflow obstruction have a 46,XX karyotype, female secondary sexual characteristics, and normal ovarian function Thus, the amount of uterine bleeding is normal, but its normal path is obstructed.
accumulation of blood behind the blockage results in cyclic abdominal pain.
Intrauterine trapping of fluid (hydrometra), pus (pyometra), or blood (hematometra) creates a soft, enlarged uterus.Similarly, the terms hydrocolpos, pyocolpos, and hematocolpos describe distention o the vagina and are seen with distal obstructions.
in women with outflow blockage, an increase in retrograde menstruation may lead to endometriosis development.
Müllerian Defects
During embryonic development, the müllerian ducts give rise to the upper vagina, cervix, uterine corpus, and fallopian tubes.Agenesis during these ducts’ development may be partial or complete.
In complete müllerian agenesis, often called Mayer-Rokitansky-Kuster-Hauser syndrome, patients fail to develop any müllerian structures, and examination reveals only a vaginal dimple
patients have a 46,XX karyotype and normal ovarian function. Renal abnormalities (34%) ,Skeletal abnormalities (12%)
however; In complete androgen insensitivity syndrome the patient has a 46,XY karyotype and functioning testes.
Hypogonadotropic hypogonadism
Here the primary abnormality lies in the hypothalamic-pituitary axis.Constitutional delayed puberty ,Common cause (20%)
There is no anatomical anomaly.
Under stature and delayed bone age, Positive family history
Endocrine investigations are all normal.
Diagnosis by exclusion and follow up
Prognosis is good ,No drug therapy is required, Reassurance.
In some circumstances it may be useful to promote a menstruation using the oral contraceptive pill for one cycle to prove that menstruation can occur and this can be extremely reassuring.
Hypothalamic Disorders (Inherited Hypothalamic Abnormalities)
Kallmann syndrome This syndrome can be inherited as an X-linked, autosomal dominant, or autosomal recessive disorder, associated with defects in the ability to smell (hyposmia or anosmia)
Kallmann patients have a normal complement of GnRH neurons, however, these neurons fail to migrate and instead remain near the nasal epithelium As a result, locally secreted GnRH is unable to stimulate gonadotropes in the anterior pituitary gland to release LH and FSH. In turn, marked decreases in ovarian estrogen production result in absence of breast development and menstrual cycles.
Acquired Hypothalamic Dysfunction(Also called “hypothalamic amenorrhea”)
Acquired hypothalamic abnormalities are much more frequent than inherited deficienciesthis diagnosis include three main categories:
eating disorders,
Excessive exercise,
and stress.
Eating Disorders
Anorexia nervosa and bulimia, both can lead to amenorrhea.
Hypothalamic dysfunction is severe in anorexia and may affect other hypothalamic-pituitary axes in addition to the reproductive axis.
Amenorrhea in anorexia nervosa can precede, follow, or appear coincidentally with weight loss.
Patients with premenarchal onset of anorexia are at particular risk or protracted amenorrhea
Exercise induced Amenorrhea
This is most common in women whose exercise regime is associated with significant loss of fat, including ballet, gymnastics, and long-distance running.In those women who continue to menstruate, cycles are notable for their variability in cycle interval and length due to reduced hormonal function
Puberty may be delayed in girls who begin training before menarche.

Stress induced Amenorrhea
This may be associated with clearly traumatic life events and even positive events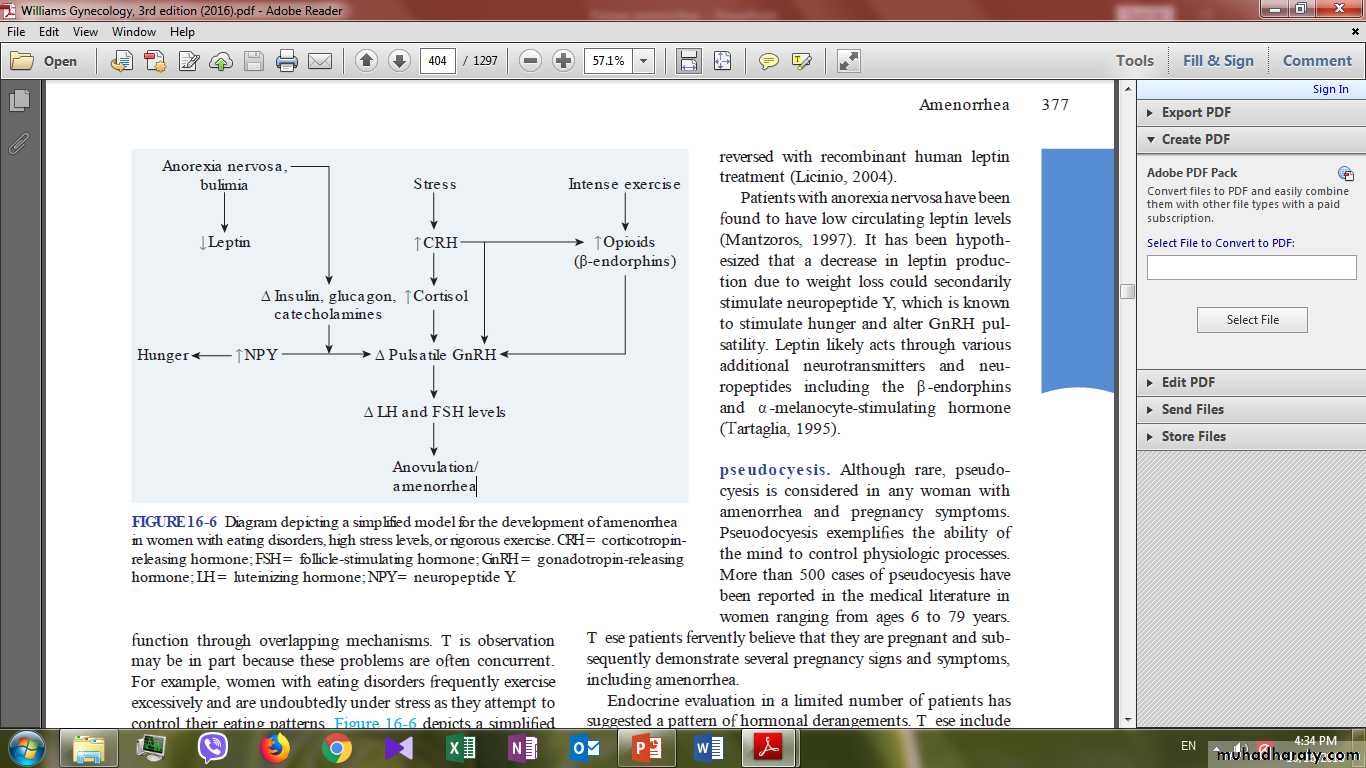
Hypothalamic Disorders (Anatomic Destruction)
Any process that destroys the hypothalamus can impair GnRH secretion and lead to hypogonadotropic hypogonadism and amenorrheaThe tumors most often associated with amenorrhea include craniopharyngiomas, germinomas ,gliomas, and metastatic lesions.
The most common of these tumors, craniopharyngiomas.
Alternatively, impaired GnRH secretion may follow trauma, radiation, infections such as tuberculosis, or infiltrative diseases such as sarcoidosis.
Anterior pituitary Gland Disorders
Most pituitary dysfunction is acquired after menarche and therefore presents with normal pubertal development followed by secondary amenorrhea.
In rare cases, these disorders may begin prior to puberty, resulting in delayed puberty and primary amenorrhea.
Pituitary adenomas are the most frequent cause of acquired pituitary dysfunction.
These most commonly secrete prolactin, but excessive secretion of any pituitary-derived hormone can result in amenorrhea.
Pituitary tumors also may indirectly alter gonadotrope function by a mass effect. First, tumor growth may compress neighboring gonadotropes. Second, damage to the pituitary stalk can disrupt dopamine’s pathway to inhibit prolactin secretion
As in the hypothalamus, pituitary function may also be diminished by inflammation, infiltrative disease, metastatic lesions, surgery, or radiation treatment
Other Causes of Hypogonadotroic Hypogonadism
The mechanisms by which these disorders result in menstrual dysfunction are poorly understood.End-stage kidney disease is associated with increased serum prolactin and altered leptin levels, both of which may disrupt normal GnRH pulsatility.
Chronic diseases may produce amenorrhea through common mechanisms, such as stress and nutritional deficiencies.
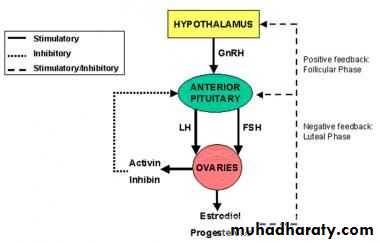
Hypergonadotropic Hypogonadism
The term hypergonadotropic hypogonadism describes any process in which:(1) ovarian function is decreased or absent (hypogonadism) and
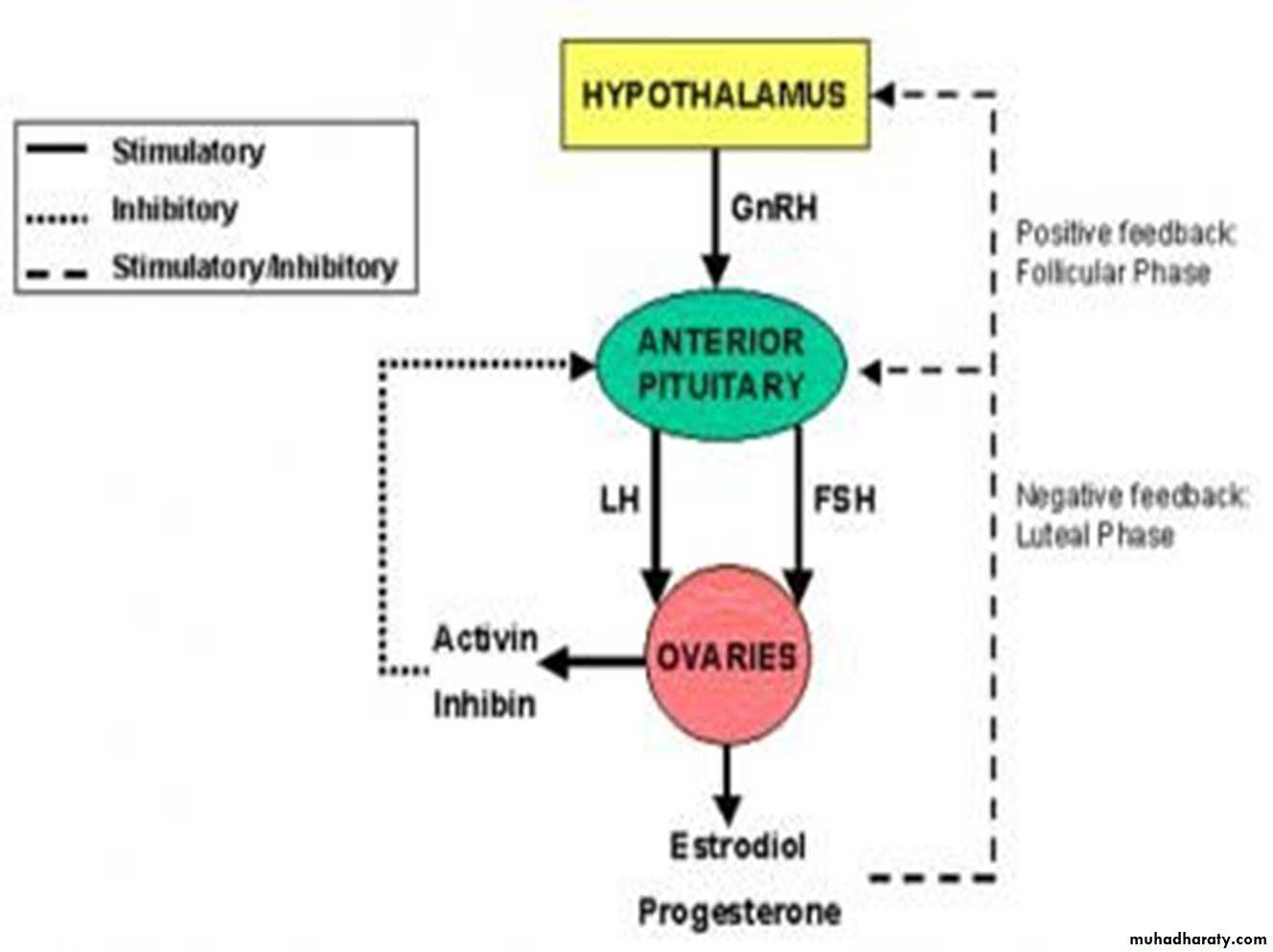
(2) due to absent negative sex-steroid feedback, the gonadotropins, LH and FSH, have increased serum levels (hypergonadotropic).
This category of disorders implies primary dysfunction within the ovary. (premature ovarian failure (POF)or (premature ovarian insufficiency)
Heritable Disorders (Gonadal Dysgenesis)
Turner syndrome is caused by de novo loss or severe structural abnormality of one X chromosome in a phenotypic female.( 45 Xo)more than half of the girls with this syndrome have chromosomal mosaicism such as 45,X/46,XX.
in girls with turner syndrome ,phenotype varies widely, but nearly all affected patients have short stature.
Associated problems include cardiac anomalies (especially coarctation o the aorta), renal anomalies, hearing impairment, otitis media and an increased incidence of hypertension, diabetes mellitus, and Hashimoto thyroiditis.
Characteristic Findings of Turner Syndrome
Height 142–147 cm Micrognathia
Hearing loss Webbed neck
Absent breast development Widely spaced areolae
Short fourth metacarpal Autoimmune disorders
Autoimmune thyroiditis Epicanthal folds
Low-set ears Shield-like chest
Cubitus valgus Renal abnormalities
Aorta coarctation Diabetes mellitus
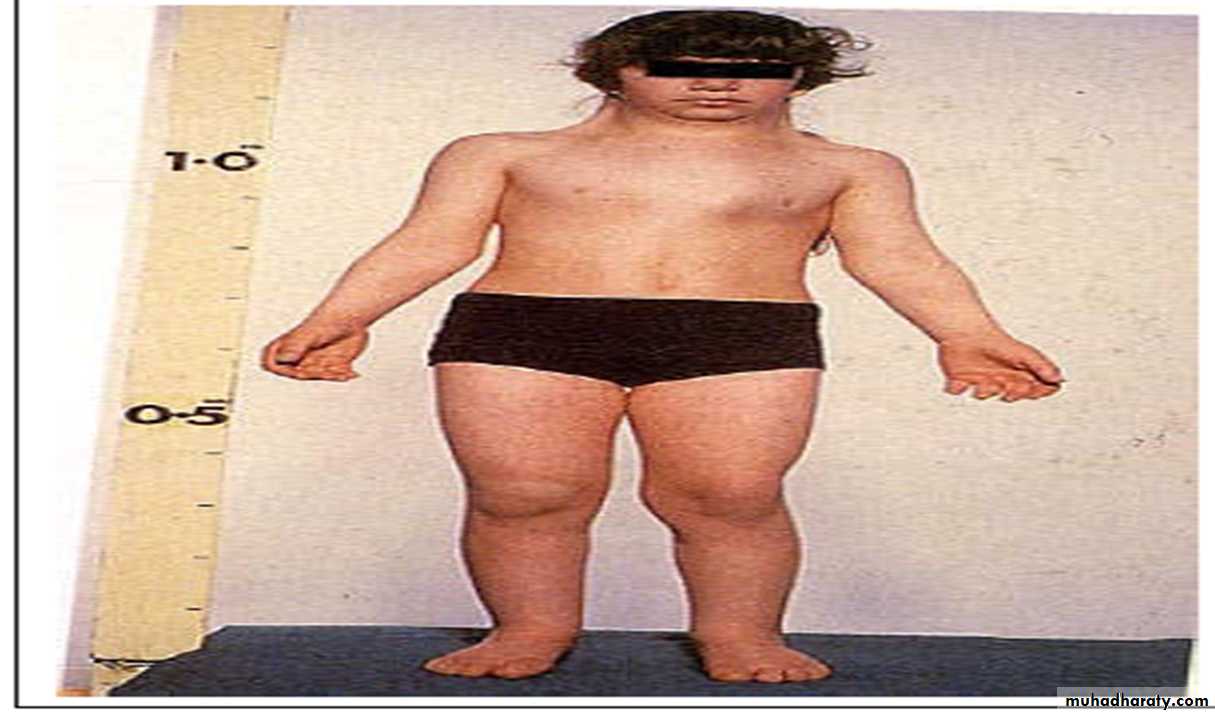
This syndrome may be recognized in childhood.
However, some patients are not diagnosed until adolescence, when they present with prepubertal female genitalia and primary amenorrhea and with short stature.The uterus and vagina are normal and capable of responding to exogenous hormones.
EVALUATION /Clinical features:
Initial questions investigate whether pubertal tanner stages have been reached and whether menses have begun,Childhood growth and development.Excessive exercise and any change in weight should be elicited.
An imperforate hymen or vaginal septum may present with a history of amenorrhea and cyclical abdominal pain difficulties in urination and even urinary retention, difficulties in defecation.
Chronic illnesses or medications (such as antipsychotics that increase prolactin levels). should be asked about.
A review of symptoms can also be helpful. For example, new-onset headaches or visual changes may suggest a tumor of the CNS or pituitary gland.
Thyroid disease can be associated with heat or cold intolerance, weight changes, and sleep or bowel motility abnormalities.
Surgical history focuses on prior pelvic surgery, especially intrauterine or ovarian surgery.
A family history of female relatives with late onset of periods is suggestive of constitutional delay. Anosmia, Autoimmune disease or androgen insensitivity syndrome may also be suggested in the family history.
A sexual history should be obtained if married.
physical Examination
Should be done in presence of girl's mother.(don't forget this)The weight and height should be checked for calculation of body mass index.
The important examination feature is the presence or absence of secondary sex characteristics such as breast development, pubic and axillary hair.
Absence of such features by 14 years suggests ovarian dysgenesis (e.g. Turner’s), a hypothalamic cause or hypothyroidism.
Other features to note are signs of Turner’s syndrome (such as webbed neck and short stature), hypothyroidism ( can present with an abnormally enlarged thyroid gland, delayed reflexes, and bradycardia.)
During breast examination, bilateral spontaneous galactorrhea implies hyperprolactinemia or abnormal visual fields from a possible prolactinoma.
Fundoscopy examination, visual filed examination and neurological examination if pituitary tumour is suspected.
Acne or hirsutism suggests androgen excess and clitoromegaly may suggest virilization or may represent ambiguous genitalia of congenital adrenal hyperplasia or an androgen-secreting tumor.
Pelvic examination Should be undertaken in the presence of the patient’s mother.
Inspect vulva to see opening of introitus (opened, closed by bluish membrane, closed)A bimanual examination is inappropriate (contraindicated) in unmarried girl. In most cases information taken from transabdominal ultrasound examination of the pelvis.
Rectal examination may help identify a uterus above an obstruction (at the level of the introitus or in the vagina.)
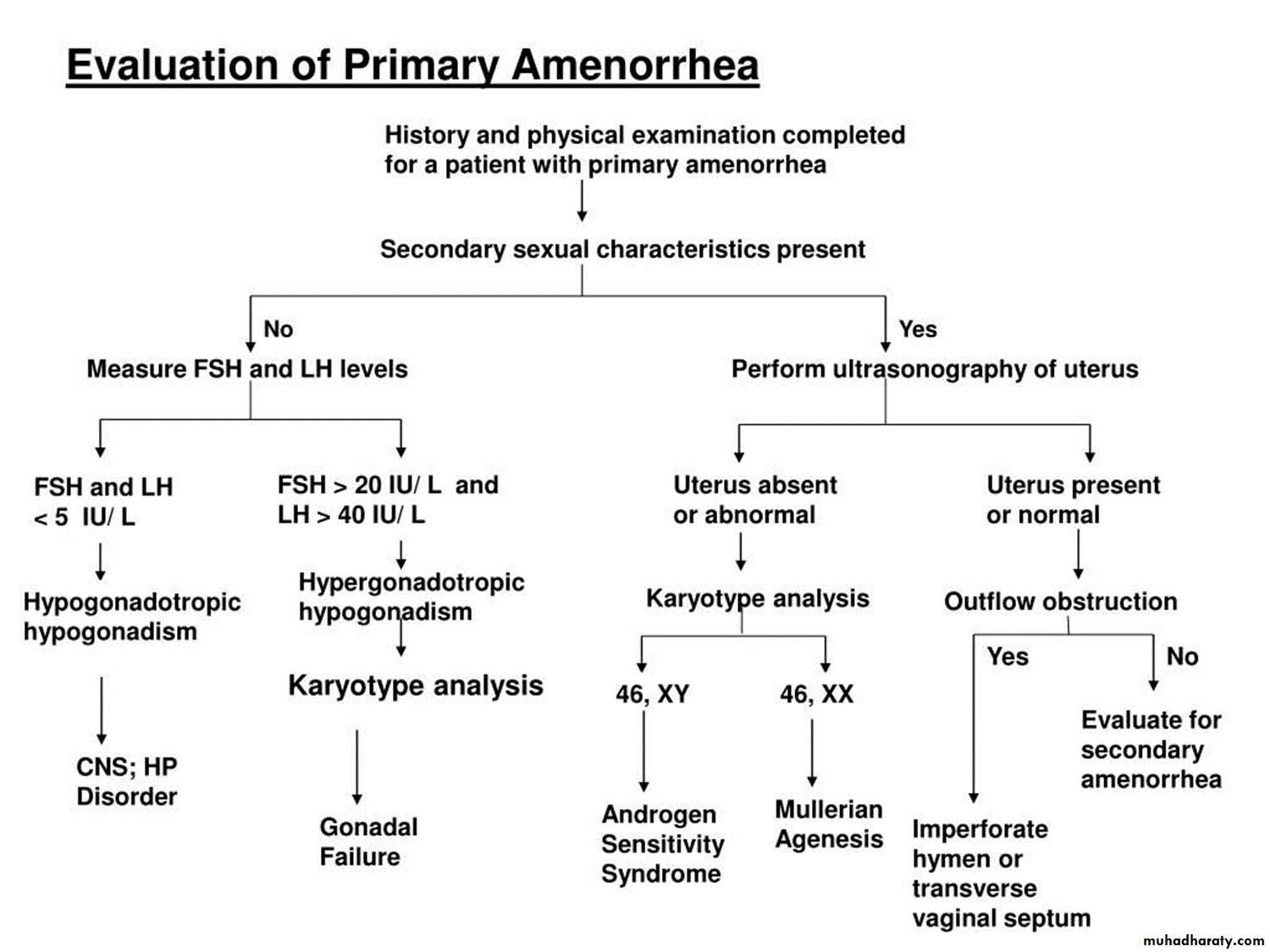
Investigations:
Start investigation in cases with primary amenorrhoea at:
a) 14 years in the absence of secondary sexual characteristic.
b) 16 years in presence of secondary sexual characteristic.
c) in some circumstances, it is reasonable to initiate an evaluation despite the absence of the above strict criteria as:
1) in patient with the stigmata of Turner syndrome.
2) in patient with obvious virilization.
3) in a patient or her parents are concerned.
A pregnancy test should be performed if there is a possibility of pregnancy.
Hormonal investigations:Thyroid function and prolactin levels should be checked.
Serum gonadotrophin levels are high with low estrogens in ovarian causes, such as Turner’s syndrome, previous chemotherapy or premature ovarian failure.
Low gonadotrophins are found in hypothalamic causes such as weight-related and exercise-induced amenorrhea.
Serum testosterone levels are measured in women with suspected PCOS or with clinical signs of androgen excess.
Karyotype confirms the presence of Turner’s syndrome or other rare abnormalities, such as fragile X syndrome, and aids the diagnosis of androgen insensitivity.
Imaging studies: Ultrasound scan should be arranged to confirm
the presence of a uterus and exclude hematometra or haematocolpos,Determine the presence, state and size of ovaries and any follicular activity.
Congenital anatomic abnormalities of uterus or vagina or both are often associated with renal abnormalities such as unilateral solitary kidney so these patients should have intravenous pyelogram.
MRI of the pituitary is indicated.
Bone age X ray to determine bone age which is important in differentiating pubertal delays as a cause.
TREATMENT
Girls with constitutional delay will menstruate spontaneously and reassurance should be given.Other causes of primary amenorrhea should be treated where possible;
for example, thyroxine for hypothyroidism,
bromocriptine or surgery for prolactinoma,
hymenal division for haematocolpos.
Exercise should be limited in those with exercise-induced amenorrhea and weight gain encouraged if the body mass index is less than 19.
In causes such as Turner’s syndrome, androgen insensitivity and premature ovarian failure, extensive counselling is required for both the girl and her parents. Support groups exist for all these disorders and cover issues of self-image, sexuality and fertility.
Osteoporosis should be prevented by long-term hormone replacement, usually in the form of the COCP.
Remove gonadal streaks if xy as in androgen insensitivity syndrome.
( Increased risk (up to 52%) of gonodoblastomas)
Questions
Amenorrhea
All are causes of primary amenorrhea except:
a.Kallman‘s syndromeb.Sheehan’s syndrome
c.Rokitansky’s syndrome
d. Turner’s syndrome
e. Constitutional delay .