1
Suppurative otitis media.
1.Acute suppurative otitis media.
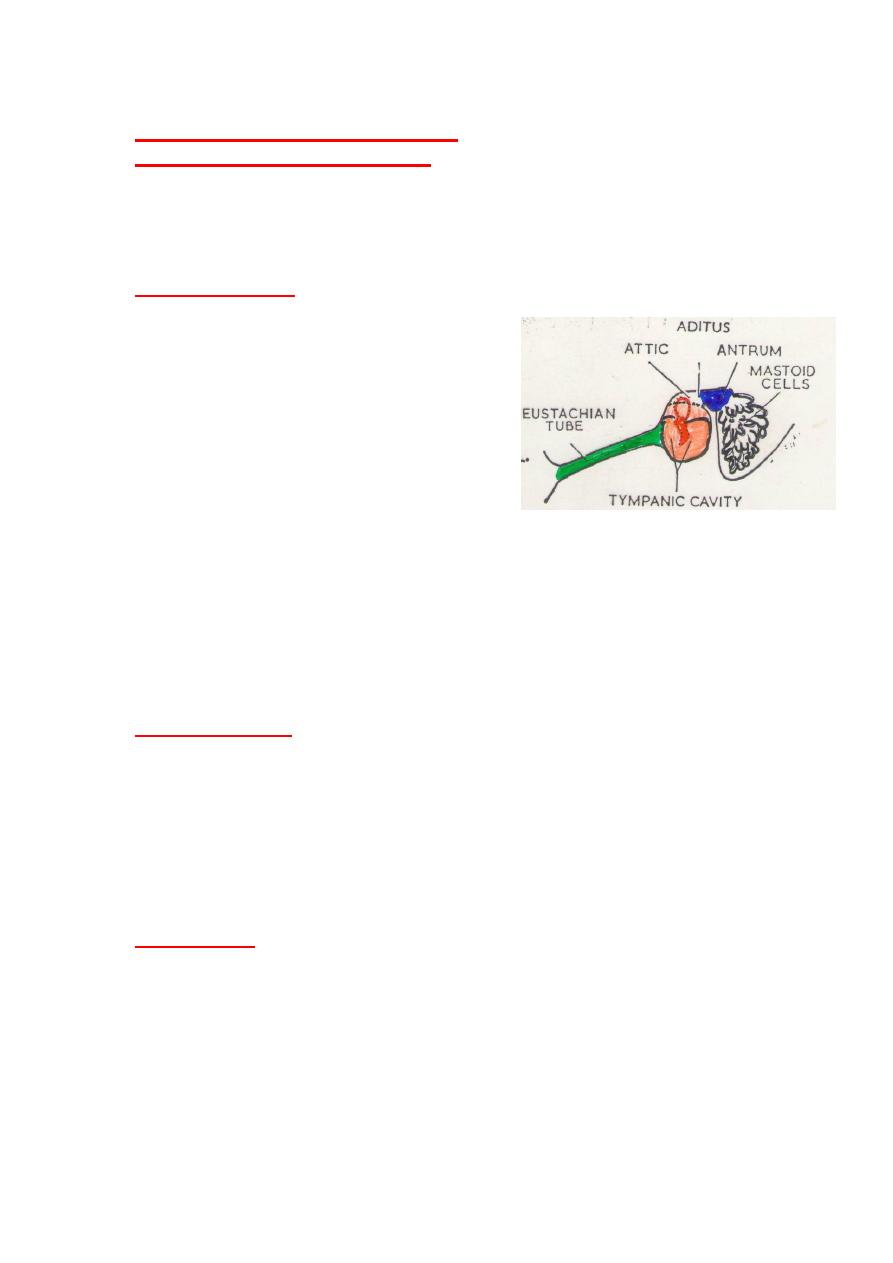
Inflammation of the mucous membrane lining the middle ear cleft produced
by pus forming organism. (middle ear cleft consisting the tympanic cavity,
Eustachian tube, mastoid antrum,and mastoid cavity).
It is a disease of childhood and very common in infants
.
Route of infection
:
1. The Eustachian tube:
*Ascending infection (Upper respiratory tract infection, and lower
respiratory tract infection).
*Excessive nasal blowing.
* Swimming and diving..
2.External auditory meatus.
* Perforated tympanic membrane.
* Through ventilation tube.
3. Blood borne infection. rare.
*In exanthemata as measles and whooping cough.
Predisposing factors
:
1. Nasopharyngeal mass ,commonly adenoid in children ands nasopharyngeal
tumor in adults.
2. Upper respiratory tract infection;Rhinitis,sinusitis,tonsillitis,…
3. Lower respiratory tract infection; pneumonia, bronchiectasis.
4.Allergy.
5. pre existing middle ear effusion.
6. Cleft palate and palatal paralysis >Eustachian tube dysfunction.
7. Systemic disease (Diabetes, leukemia,cystic fibrosis,..)and immunodeficiency
syndromes(Hypo gammaglobulinemia).
Bacteriology:
It considered as bacterial disease ,but viral infection precede bacterial infection
in some cases (20%).
Common pathogens in order of frequency are.
1.Streptococcus pneumonia.
2. Haemophilus influenza.
3.Branihamella(Moraxella) catarrhalis.
4. Streptococcal pyogenes
*Less G-ve Bacilli. Pseudomonas, proteus, E.coli, and Klebsella pneumonia.
They commonly affect babies under 3 months.
2
Clinical features
.
1.Fever.
2-Earache.(throbbing otalgia).
3-Hearing loss (conductive).tinnitus, and autophony.
4-Ear discharge.(after rupture of the tympanic membrane (T.M), early
serosangeuous then frank pus).
There are 4 clinical phases by otoscopic examination
1. phase of tubal obstruction. The T.M is retracted.
2. phase of pre suppuration. Congestion of the T.M along
the handle of malleus and periphery..
3. phase of suppuration. Bulging tense T.M.,Conductive hearing loss.
4. phase of resolution. * When the tympanic membrane perforated (usually
central perforation), the pain relieved(child go to sleep), reduced temperature,
and otorrhea.
* When no perforation. gradually fade of tympanic
membrane hyperemia, with relief of otalgia and deafness
.
*In infants
:
The fever is high (may reach 40-41 0C),
-Ear ache(infant is irritable, sleepless, and catch his ear with his hands),
-there are vomiting and diarrhea..
otoscopy. May show only loss the cone of light or slight congestion of the
tympanic membrane. as it is thicker than adults.
Treatment of acute suppurative otitis media.
1. Bed rest and warmth and analgesia;(warm room with adequate humidity to
improve cillary function.).
2. Systemic antibiotics: Broad spectrum antibiotics for 10 days.
Amoxicillin is drug of choice (orally).
In allergy >Erythromycin or septrin.
*When no response,B-lactamase-resistant antibiotics should be choice, like .
Coamoxyclav (amoxicillin+Glavulinic acid).
Parental injection given in severe infection.
*Ceftriaxone 50 mg/kg. I.M,or I.V/single dose daily/for three days.
3. Nasal decongestant, to improve patency of Eustachian tube
-Local .Xylometazoline (drops or spray)/4 times daily.
-Systemic decongestant is controversy.
4. Local treatment.
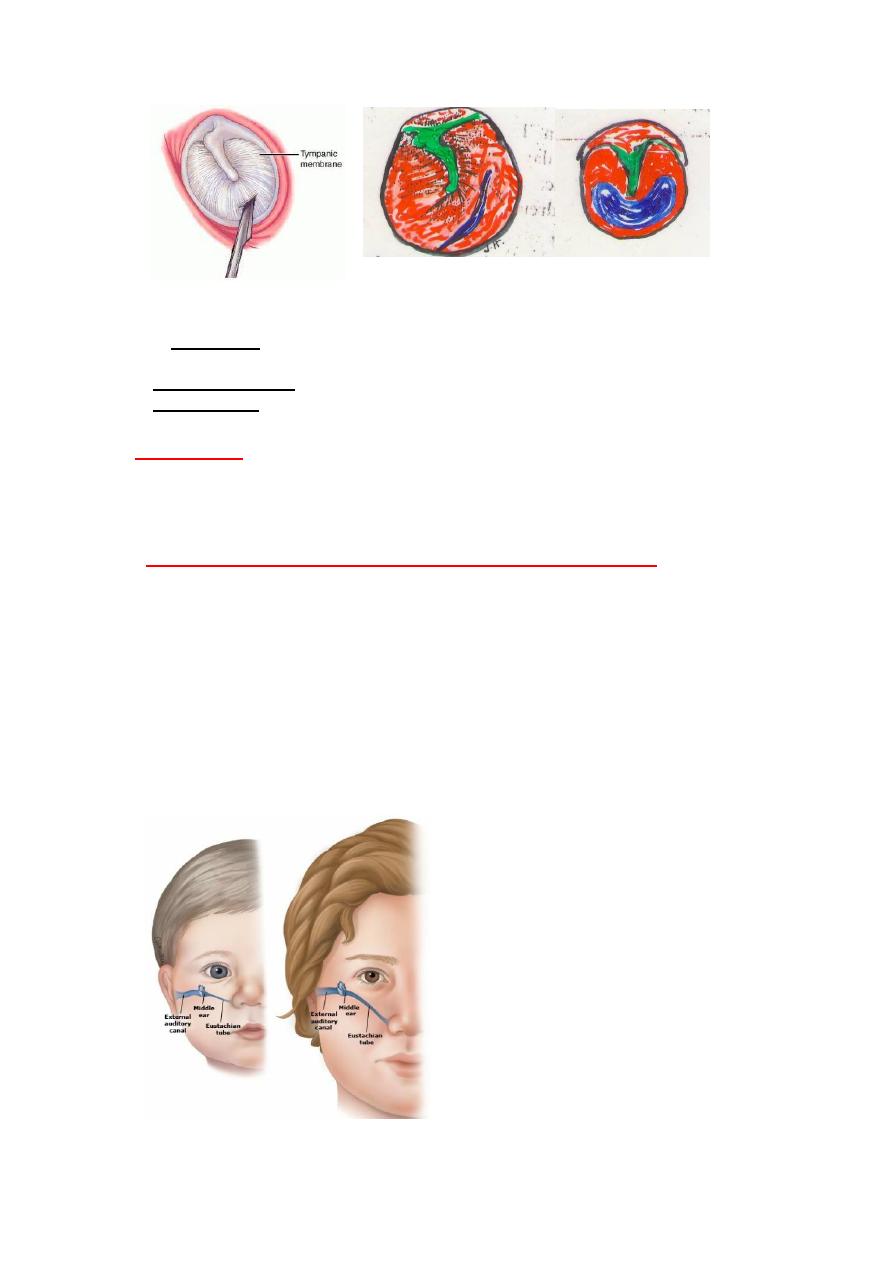
A* Myringotomy: Incision in the tympanic membrane to drain pus or fluid
present in the middle ear.
Pus taken for culture and sensitivity test.
The myringotomy incision heals better than pathological opening as there is no
tissue loss.
Indications for myringotomy in A SOM.
1-Intense pain with bulging tympanic membrane.
2-Failure of resolution ,persistent pain and fever despite of medical treatment.
3- With complications ;acute mastoiditis,Facial palsy.
4-Small or high perforation, to ensure good drainage.
3
myringotomy incision spontaneous perforation
* Aural toilet .After rupture of the tympanic membrane. By dry mopping
(cotton wool),or frequent suction clearance.
5. Topical antibiotics. is unnecessary as it unlikely to reach the infected area.
6. Keep ear dry. (prevent water entering the ear)using cotton immersed with
Vaseline.
Prognosis:
85% get complete recovery with full resolution of auditory function.
*Failure of resolution causes.
1.Persistent perforation.
2.Otitis media with effusion.
ASOM is common in infants and childhood, than adults;
Because
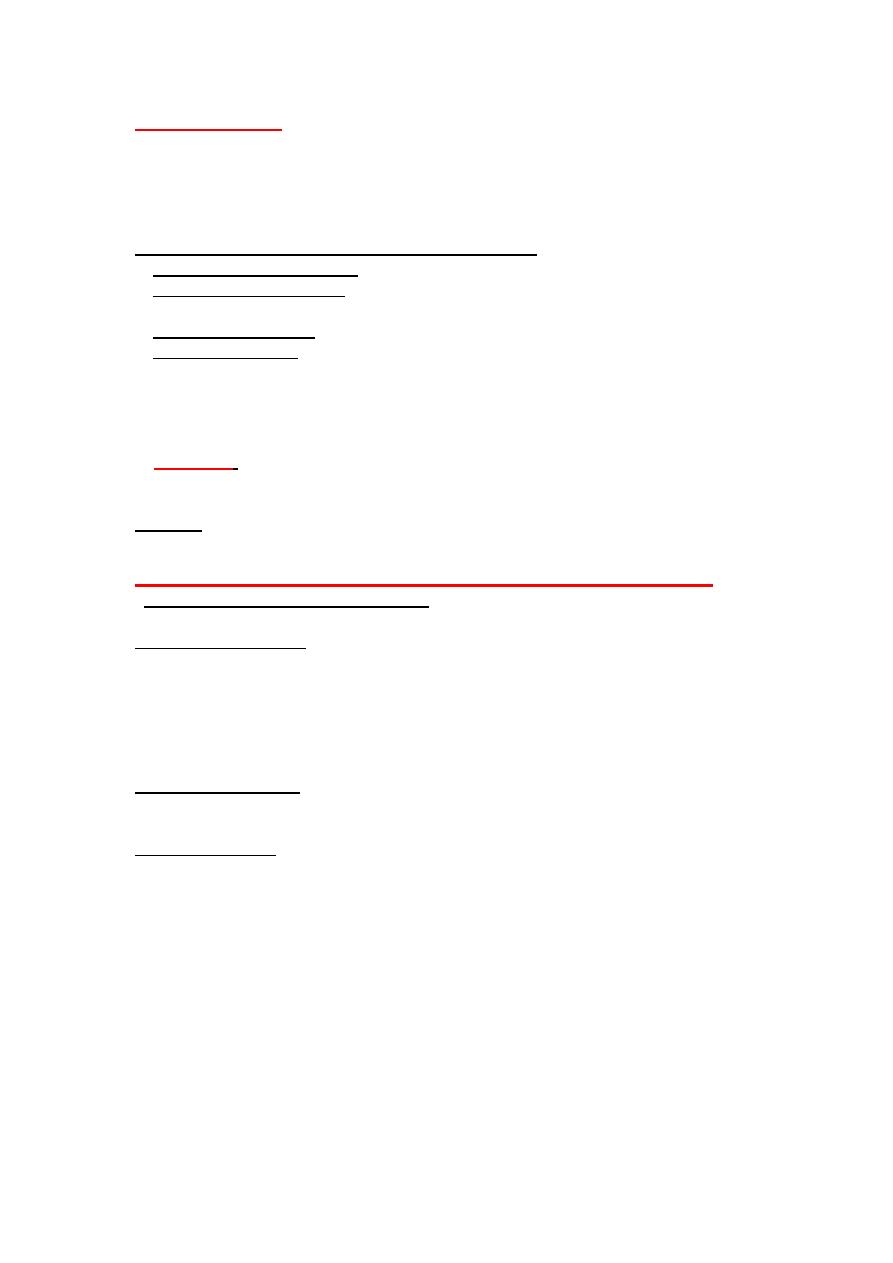
1.The Eustachian tube is relatively wider ,shorter and more horizontal, and
opens at lower level.
2.Frequency of upper respiratory tract infections(Measles, chicken pox and
whooping cough),tonsillitis and adenoiditis.
3. Gastroenteritis(vomits may be forced through the Eustachian tube.
4.Teething lower the resistance.
5. Bottle feeding make infant more liable than breast feeding because
a.Recumbent position during during bottle feeding causes regurgitation of
milk in to nasopharynx and Eustachian tube.
b. Milk less sterile.
c. The bottle-fed infants less resistant to infection.
4
CHRONIC SUPPURATVE OTITIS MEDIA(CSOM)
Is a persistent disease of middle ear cleft of insidious onset capable to causes
destruction and irreversible sequalae.Clinically presented with otorrhea and
hearing loss.
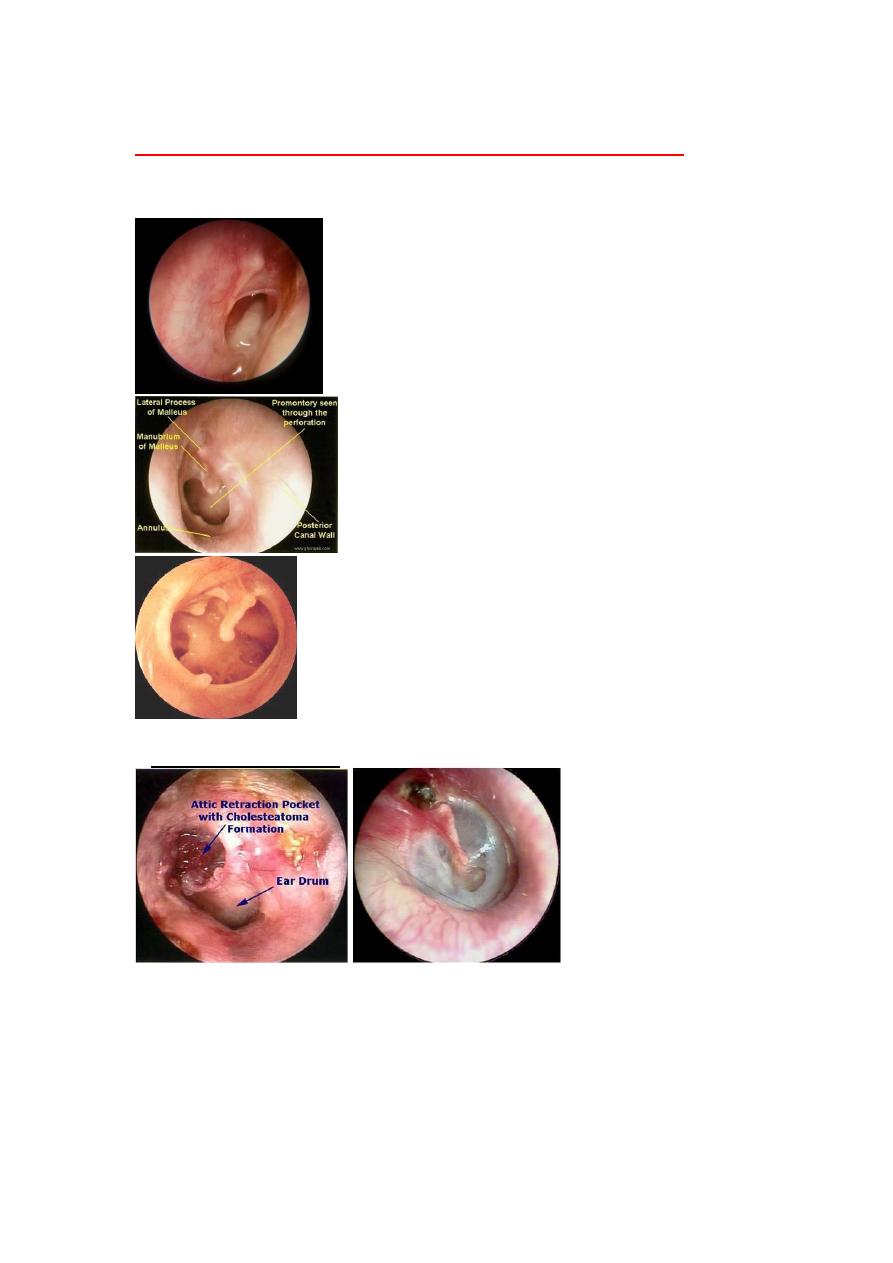
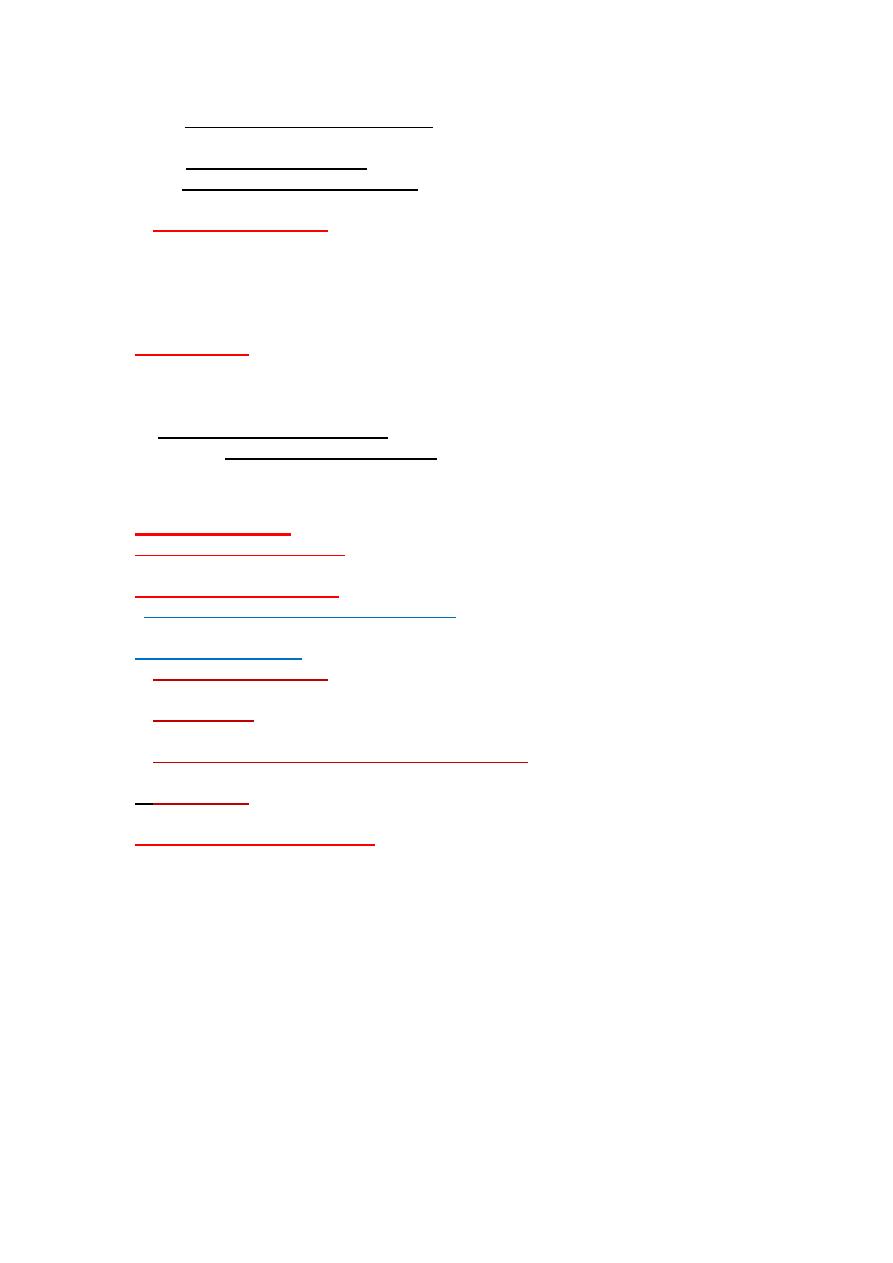
Active Tubo-Tympanic disease(discharge from the perforation)
In active Tubo-Tympanic disease (dry central perforation
)
In active Tubo- Tympanic disease.( dry subtotal perforation
.
2.Attico-Antral disease.(AA).
Attic Retraction pocket.
5
According to anatomical classification
it of two types.
1.Tubo-Tympanic disaes .(TT)
II.Attico-Antral disease.(AA)
Regarded "safe" from complications
Regarded "unsafe "dangerous from risk of
complications.
The perforation is always central
perforation in parse tensa.
*The perforation is in the attic, marginal,
or postero-superior perforation.
The discharge is
*mucoid or mucopurulent. *profuse.
* intermittent for short duration,
commonly preceded by URTI or
swimming.
*not offensive.
The discharge :
* purulent.
* scanty.
* continuous.
*offensive.
*Rarely found cholesteatoma
Commonly found cholesteatoma.
*Active
phase
,there is discharge
(otorrhea),granulation tissue or polyps
).
*Inactive
(Dry perforation)
*Active phase,
there is cholesteatoma,
granulation tissue, polyp).
*Inactive
no cholesteatoma,dry
perforation.
According to pathological classification
Called
mucosal chronic otitis media.
According to pathological classification
called
( Sequaumous epithelial COM.)
Treatment
usually conservative medical
treatment.
Treatment
Surgical when there is
cholesteatoma.
Investigations for CSOM
1. Ear swab
. for both aerobic G-ve and G+ve organism, and culture and
sensitivity test. and anaerobic organisms.
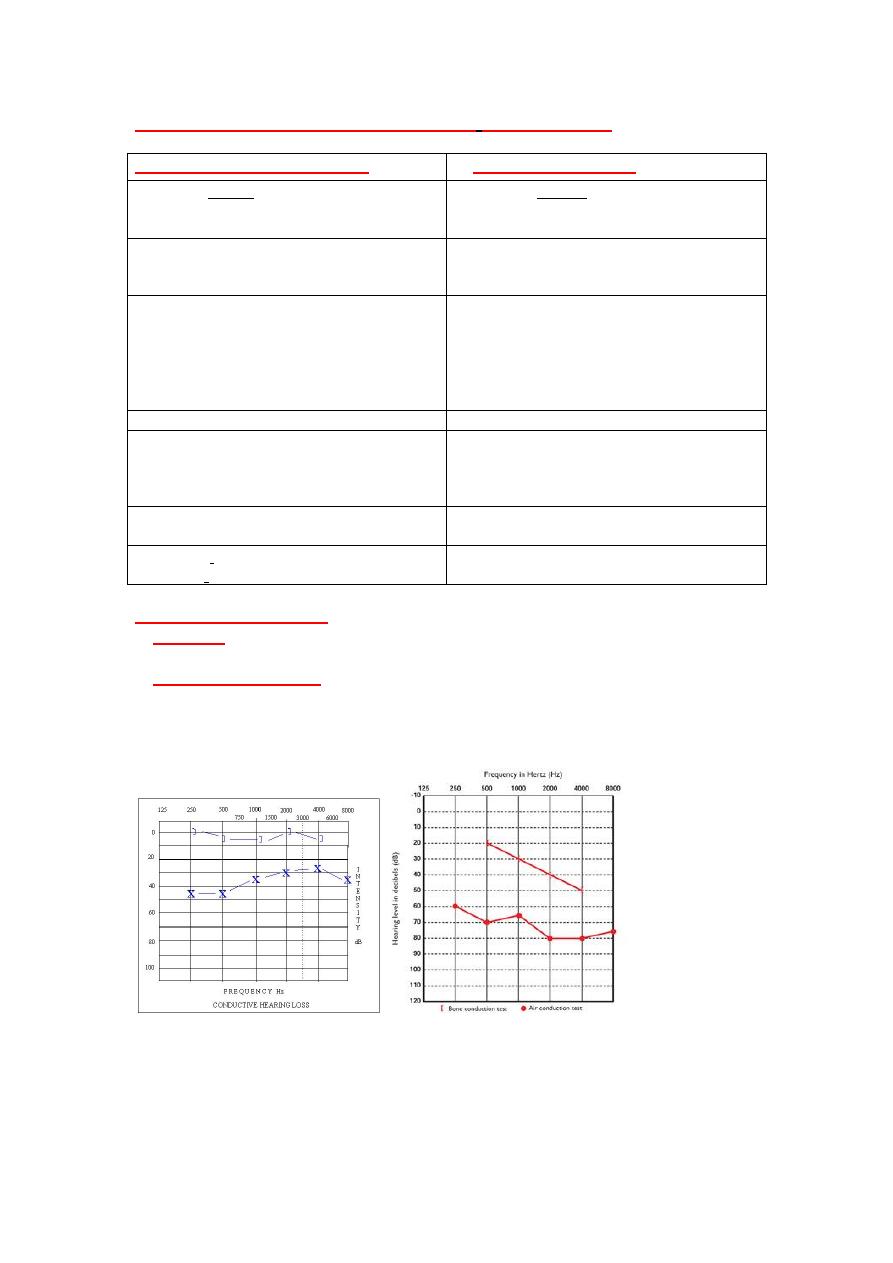
2. Pure tone audiometry.for
Type of hearing loss; expected conductive hearing loss, in advanced cases
mixed hearing loss.
*Severity of hearing loss.
*Base line of treatment
Pure tone audiometry.
(A)Conductive hearing loss (B)Mixed hearing loss.
6
3. Imaging study
1.Plain mastoid X-Ray:
Commonly do Lateral oblique view for both mastoid.
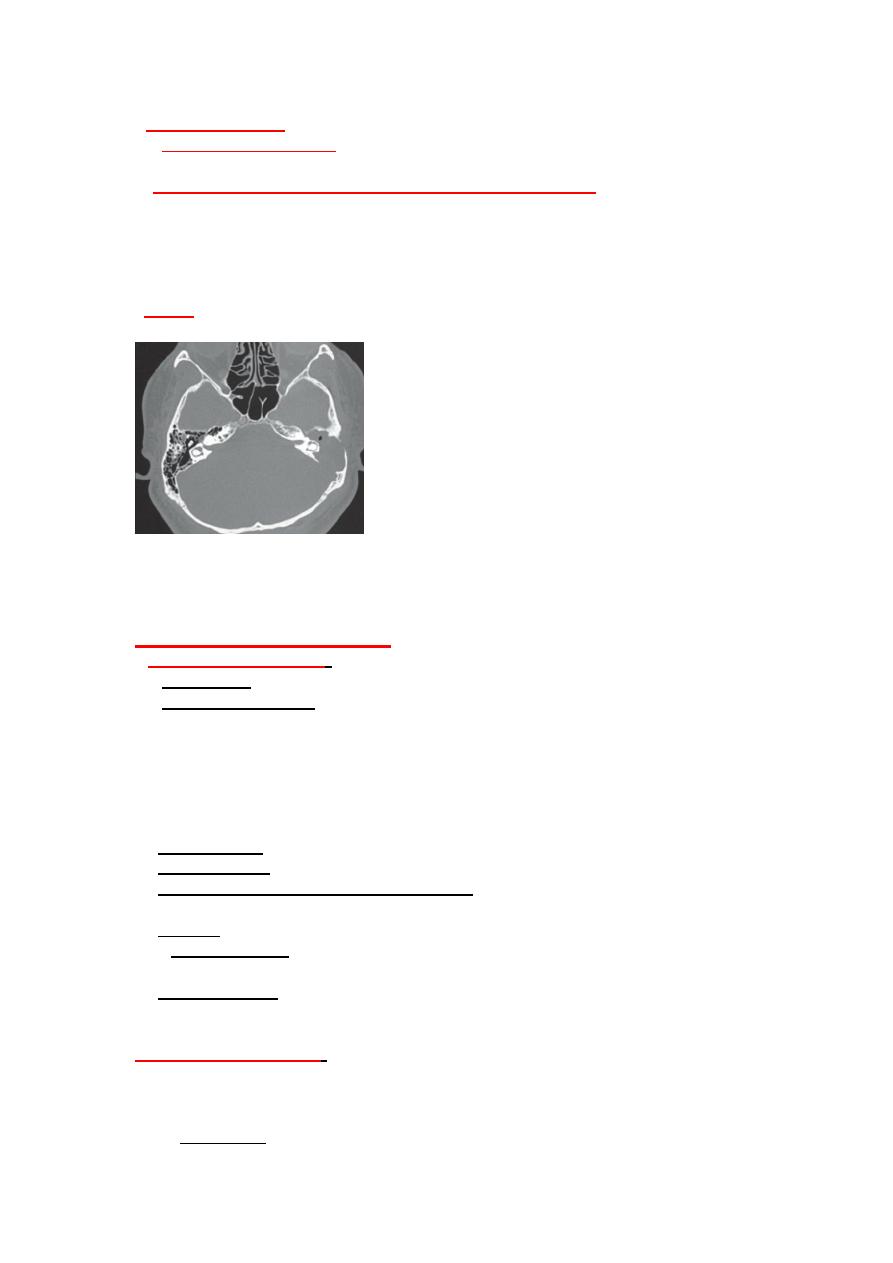
2.High resolution CT scan of temporal bone..best imaging
For* a.pathology (sclerosis,cholesteatoma ,ossicular condition,labyrinthin
fistula,..).
*b. Anatomy: Degree of pneumatization, Level of dural plate, sinus
plate,facial nerve. landmarks for surgery
*c. Inner ear and intracranial complications.
3.MRI..
High resolution CT scan of temporal bone, For patient with left
CSOM, AA disease ;showing chlolesteatoma of left temporal bone causing destruction and absence of
ossicular chain and erosion of tegmen increasing risk of intracranial complications
Mastoiditis
Treatment of CSOM:
I:Tubo-tympanic disease
:
1*Aural toilet: by dry mopping, or suction clearance(frequently)
2*Systemic antibiotics .according to C/S test for 10-14 days.
Common G-ve is pseudomonas ,and G+ve staph aureus so use Fluroquinolone
(ciprofloxacine), or aminoglycosides
.Systemic and locally(ear drops).
Ciprodar orally ,or local drops is safe (non-ototoxic drug) like
aminoglycosides.
3*Ear drops ??Topical Ab-Steroid ear drops.(ciprocort drop)
4*Keep ear dry.
5*Minor surgery. Remove aural polyp or granulation tissue.
6*Eliminate and correct any abnormalities in the nose ,tonsil,sinuses,and lower
respiratory tract.
7*Surgery
*_Myringoplasty.(grafting of the tympanic membrane) when get dry
perforation(Inactive mucosal COM).
*Tympanoplasty. when failure to get dry ear.(There is eradication of the
disease(Mastoid exploration) with reconstruction of hearing mechanisms include
Myringoplasty, ossiculoplasty(reconstruction of ossicular chain.)
II: Attico_antral disease
:
*When no cholesteatoma. might think of medical treatment.
*When there is cholesteatoma. need mastoid exploration, and the type of
operation depends on extension of the disease and preoperative finding.
1_Atticotomy.for small cholesteatoma confined to the attic.
7
2_Modified radical mastoidectomy.
Indications.Large cholesteatoma with good inner ear function.
3- Radical Mastoidectomy: rarely done.
4- Canal wall up mastoidectomy. To eradicate cholesteatoma throught facial
recess approach.
**The aim of the surgery
:
1.Remove bone disease and change the ear to safe ear.(Reduce complications.
2.Improve hearing do myringoplasty, ossicloplasty.
3.Prevent recurrence.
4. Get dry ear (about 70%)
Cholesteatoma
:
Is presence of keratinized squamous epithelium in the middle ear cleft, with
ability to destruction of the ossicles,tegmen tympani and tegmen antri to the
subdural space and sinus plate causing
*temporal bone complications like( facial palsy,labyrinthitis and labyrithin
fistula ,and *intracranial complications. (like menigitis,extradural , sub dural
abscess and brain abscess,lateral sinus thrombosis and thrombophlebitis,and
otitic hydrocephalus
)
Classification
:
I;Congenital cholesteatoma
;Congenital nest of epithelial tissue(epidermoid
cyst).occurs in the middle ear cleft,petrous apex,and cerebellopontine angle.
II.Acquired cholesteatoma
.
1.Primary acquired.(invagination theory);
as squale of negative middle ear
pressure causes retraction pocket then cholesteatoma.
2.Secondary acquired
. Due to CSOM.the pathogenesis are
A. Immigration theory
.in marginal and postero-superior perforation.because
absence of annulus..
B.Metaplasia
of middle ear mucosa. Due to chronic irritation in CSOM, the
mucosa converted to squamous epithelium.
C.Papillary proliferation of stratum germinatum
.the basal layer of epidermis
of shrapnel membrane.
D.Iatrogenic
. keratinizing epithelium introduced in to the middle ear by
surgical procedure, perforation.
Clinical features and treatment
.
Same Attico-Antral CSOM.
=============================