Hemodynamic Disorders 2
د.بنان برهان محمدماجستير/هستوباثولوجي
Continue ------congestion
Morphological changes in venous congestion***Pulmonary congestion:
In case of left sided heart failure → raised pressure in the pulmonary veins → alveolar capillaries become distended, engorged with blood, alveolar septal edema and minute intra alveolar hemorrhage → break down of RBCs & phagocytosis of intra-alveolar red cell debris by macrophages leading to accumulation of (hemosidrin –laden macrophages) (heart failure cells) with a transudate in the alveolar spaces.In chronic pulmonary congestion, the septa become thickened and fibrotic.
Pulmonary congestion with dilated capillaries and leakage of blood into alveolar spaces leads to an increase in hemosiderin-laden macrophages,
Usually follows right sided heart failure →liver moderately enlarged & tender.
Micro:- the central vein and sinusoids are distended with blood and may be central hepatocyte degeneration; the periportal hepatocytes are better oxygenated because of their proximity to hepatic arterioles, so they are less hypoxic & may develop only fatty changes.Grossly:- central regions of hepatic lobules red-brown surrounding by uncongested tan, some time fatty liver giving it an appearance called "nut meg liver".
In sever long standing hepatic congestion, hepatic fibrosis can develop, termed ”cardiac cirrhosis”
***Congestion of the liver
Microscopically, the nutmeg pattern results from congestion around the central veins, as seen here. This is usually due to a "right sided" heart failure
"

venous congestion of the liver ”nutmeg liver”.


the natural nutmeg
Hemostasis and thrombosisNormal hemostasis: is the Maintaining blood in a fluid, clot-free state in normal vessels while inducing the rapid formation of a localized plug at a site of vascular injury.
Thrombosis: is the pathologic form of hemostasis , it means the formation of blood clot (thrombus) in uninjured vessels or thrombotic occlusion of vessel after relatively minor injury.
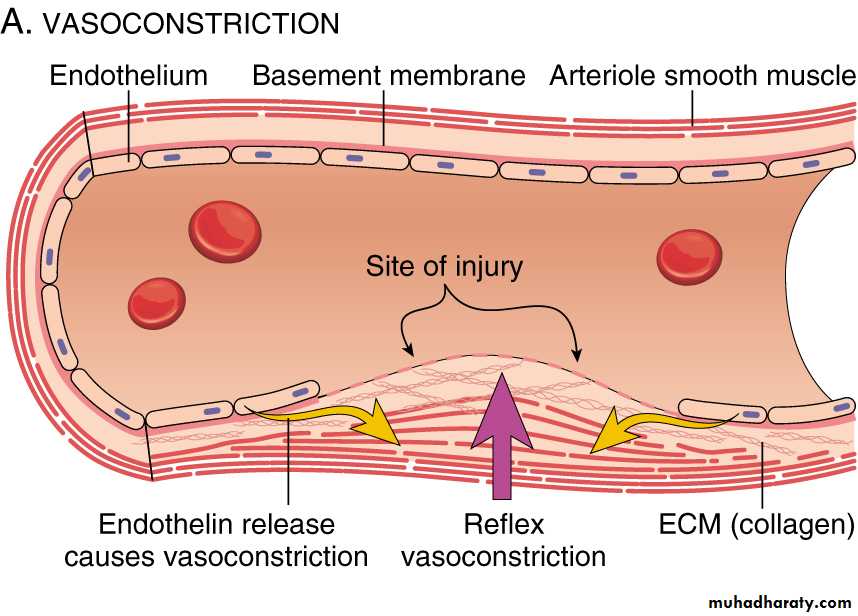
The sequence of events in hemostasis at a sit of vascular injury include:
Transient period of arteriolar vasoconstriction.
Endothelial injury expose highly thrombogenic
subendothelial extracellular matrix (ECM), then platelets adhere to ECM by VonWillebrand factor and become activated. Activation of platelets results in change of its shape (increase surface expression of phospholipid complex) and release secretory granules (adenosine diphosphate (ADP) and thromboxane A2 (TXA2)) which will lead to the further platelets aggregation, and to form primary hemostatic plug.
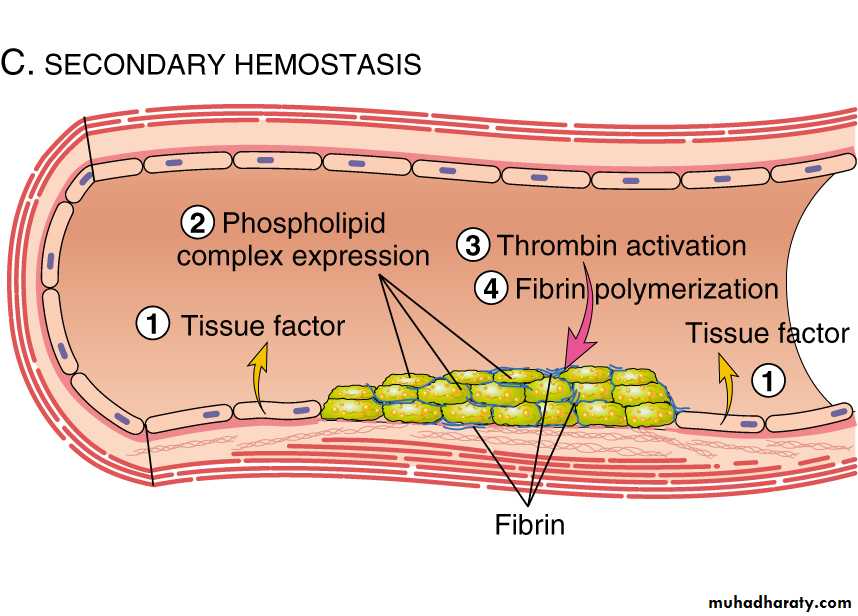
Tissue factor (factor III or thromboplastin) which also exposed at the site of injury, this factor activates the coagulation cascade which creating a fibrin meshwork deposition (secondary plug).
Polymerized fibrin and platelet aggregates form a solid permanent plug.
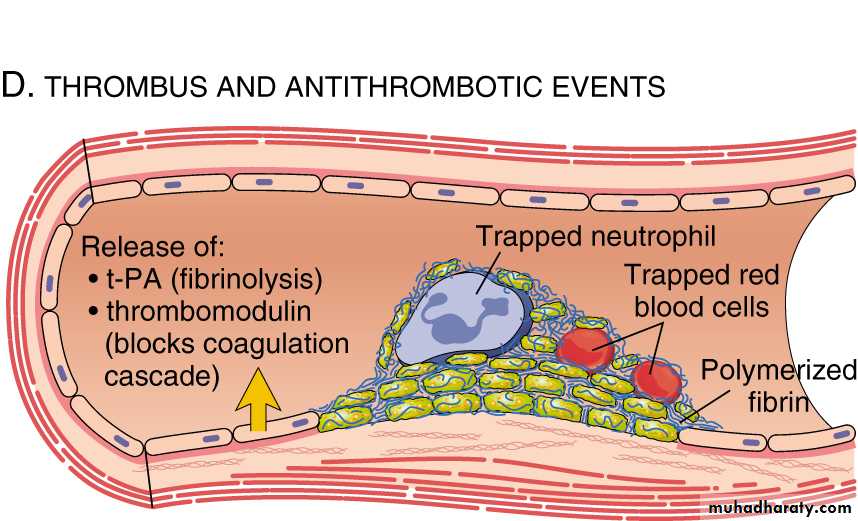
At this stage counter-regulatory mechanisms (tissue plasminogen activator(t-PA) & thrombomodulin) are set into motion to limit the hemostatic plug to the site of injury.
Slide 5.5
(from Robbins Basic Pathology,2003, a litter be changed)

Permanent plug
Both hemostasis and thrombosis involve three components:1. Vascular wall.
2. Platelets.
3. Coagulation cascade.
Endothelial cells on the one hand at baseline exhibit anti thrombotic (anti-platelet, anti-coagulant, and fibrinolytic) effect; on the other hand , they capable (after injury or activation) of exerting prothrombotic functions.
Endothelium:
• Antiplatelet effects:
**An intact endothelium prevents platelets and plasma coagulation factors from meeting the highly thrombogenic subendothelial ECM.**The endothelium secret PGI2 & nitric oxide (vasodilators & inhibitor of platelet aggregation).
**also elaborate ADPase which degrade ADP & inhibits platelet aggregation.
1-Anti thrombotic Effect:
2. Anticoagulant effects: These effects are mediated by Membrane-associated heparin-like molecules and by thrombomodulin → activation of anticoagulant protein (protein C).
3.Fibrinolytic effects: endothelium synthesize tissue plasminogen activator (t-PA), promoting fibrinolytic activity to clear any fibrin deposits.
2. Pro-thrombotic activities
• endothelial injury results in platelet adhesion to subendothelial ECM by binding to von Willebrand factor (synthesized by normal endothelium).• cytokines such as TNF or IL-1 as well as bacterial endotoxin induce endothelial cell production of tissue factor (factor III) which activates clotting pathway.
• inhibition of fibrinolysis by plasminogen activator inhibitors (PAIs).
Platelets play a central role in hemostasis
AdhesionActivation and shape change with markedly increased surface area.
Secretion, upon activation, platelets secrete granule products (calcium, ADP, TXA2).
Aggregation: ADP & TXA2 are a potent mediators of platelets aggregation.
Coagulation cascade
Coagulation cascade: is essentially a series of enzymatic conversions, turning inactive pro-enzymes into active enzymes and culminating in thrombin formation. Thrombin converts soluble fibrinogen into insoluble fibrin.Beside inducing coagulation, activation of the clotting cascade also sets into motion a fibrinolytic cascade that limits the size of the final clot.
Three primary influences predispose to thrombus formation (Virchow triad);

Virchow triad:
• Endothelial injury : (by it self can lead to thrombosis) e.g. in MI, valvulitis, ulcerative atherosclerosis plaques, vasculitis.Endothelial dysfunction in the absence of endothelial cell loss can influence clotting events (may elaborate greater amounts of procoagulant factors or may synthesize fewer anticoagulant effectors). Endothelial dysfunction may occur with hypertension, bacterial endotoxins, radiation and products absorbed from cigarette smoke .
2. Stasis or turbulence of blood flow, causing;
• Disruption of laminar flow and bring platelets into contact with endothelium• Preventing dilution of activated clotting factors by fresh-flowing blood.
• Retarding the inflow of clotting factor inhibitors.
• Promote endothelial cell activation.
• e.g. aortic aneurysms, acute MI, atrial fibrillation and hyperviscosity syndromes as in polycythemia.
3. Blood hypercoagulability:
can be divided into:Primary as in mutation of factor V gene and prothrombin gene (most common), antithrombin III dificiency or protein C or S deficiency
Secondary as in prolonged bedrest, MI, tissue damage( surgery, burn, trauma, fracture), cancer, late pregnancy, ocp use, polycythemia, Nephrotic syndrome, smoking ……ect.
Morphology: thrombi may develop anywhere in the cardiovascular system.
Grossly and microscopically have apparent laminations (lines of Zahn), produced by alternating pale layers of platelets admixed with some fibrin and darker layers containing more red blood cells.
Right atrial mural thrombus with lines of Zahn

Mural thrombus with lines of Zahn

Venous thrombus leg muscle

Microscopic appearance of thrombus' the line of Zahn’.

• Types of thrombus:
• Arterial thrombi:(pale thrombus) are gray white in color, firmly attached to the wall , begin at site of injury or turbulence, usually occlusive, Occur in coronary, cerebral or femoral arteries.• Venous thrombi:(red thrombus) red in color, are less firmly attached to the wall, begin at site of stasis, invariably occlusive, occur in lower extremities (90%).
• Thrombophlebitis: (initiated by inflammation)
• Philebothrombosis:(initiated by factors other than inflammation)
Mural thrombi : are thrombi arise in heart chambers or aortic lumen.
Vegetations: are thrombi formed on heart valves as in infective endocarditisPost mortem clot: it is gelatinous with dark red dependent portion and yellow ”chicken fat” supernatant , lack lines of Zahn and not attached to blood vessel ,in contrast thrombi almost always have point of attachment.
Venous thrombosis
Occur in 90% in the veins of lower extremitiesSuperficial venous thromboses
_occur in saphenous veins ( with Varicosities)
_symptomatic
_rarely embolize
Deep vein thromboses
_rapidly offset by collateral channels (50%
asymptomatic)
_embolize to lungs
Fate of the thrombus:
1. Propagation to obstruct a critical vessel or branch.
2. Embolization in part or in whole.
3. Dissolution (removal by fibrinolytic action).
4. Organization and re-canalization.
Thrombi are significant because:
• They cause obstruction of vessels.• Artery → infarction, vein → congestion
2. They are possible sources of emboli.


organization
recanalizationFates of thrombus
