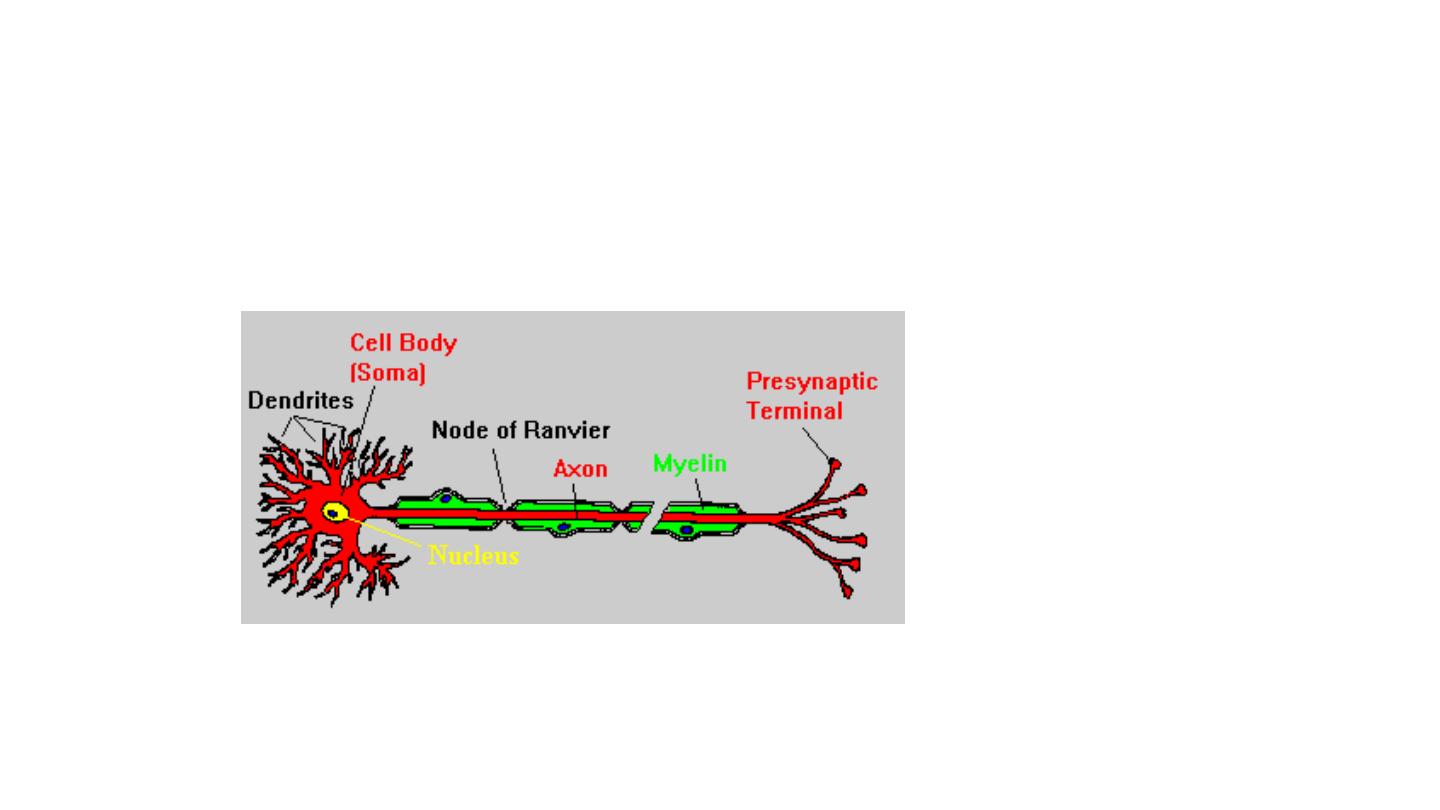
Peripheral
Nerve Injury

Neuropraxia:
Tinel’s Sign Negative
•
It is temporary physiological disruption of nerve impulse
conduction. The loss of function is incomplete.
•
Complete recovery takes place in 3–6
weeks
and
it
comes back like lightening, i.e. completely recovers
in
one go.
Neuropraxia:
•
No Wallerian degeneration
takes place and Tinel’s
sign is
negative.
–
Crutch
palsy—Pressure palsy (radial
nerve
or
part of
brachial
plexus
injured)
–
Saturday night palsy—Pressure palsy (radial
nerve)
–
Tourniquet palsy—Pressure palsy
•
Few traumatic nerve
injuries
are neuropraxia

Axonotmesis:
• Tinel’s Sign Positive and Progressive
• • It
is
Axon breakdown,
Tinel’s
sign is
positive, Motor
March
is
seen (recovery
of
muscles
takes place in
the order of
their
nerve
supply
from proximal to
distal
direction).
• • Recovery is
usually
not complete.
• • Seen in
closed
fractures and dislocations

Neurotmesis:
•
Tinel’s sign is positive and nonprogressive
• • Complete anatomic section
of
the nerve.
Tinel’s
sign is
positive
and nonprogressive.
• • No recovery without
surgical
intervention.
Even
with intervention
may not have complete recovery.
• • Degeneration
distal to
injuries
(Secondary or
Wallerian degeneration)
• • Degeneration
in
proximal
segment
(Primary
or
retrograde degeneration)
• • At
proximal
end forms—
Neuroma
• • At
distal end forms—
Glioma

• Order of Nerve Injuries
Neuropraxia
• Axonotmesis
• Neurotmesis
N AN

Autonomous Zone of Nerves:
• Exclusively Supplied by that Particular Nerve
• • Median
Nerve—Tip
of
index finger,
middle
finger.
• • Ulnar Nerve—Tip
of
little finger
• • Radial
Nerve—1st
web space
on dorsum
of
hand
• • Deep peroneal nerve—Dorsum of
1st web space
on foot

Tinel’s Sign:
•
(Records regeneration
rate) by
tapping
on the
nerve
course
from distal to
proximal direction
tingling
is
felt at
the sprouting nerve
ends
till
the distal course
of
the nerve
and it
disappears as
myelinization
takes place (Rate of
Recovery of
Nerve
is
1mm/day)

Diagnostic Tests for Nerve Injuries:
• • EMG: Denervation
fibrillation potentials. Appears at
2–
3 weeks
then spontaneous
fibrillation.
• • EMG is the earliest indicator of nerve recovery.
• • Nerve conduction study:
• 1. reduced
in
axonotmesis
and neurotmesis
but
cannot
differentiate
between the two.
• 2. Normal nerve
conduction
velocity on day 10
goes toward
neuropraxia.
• 3. No
conduction
will indicate
neurotmesis.

• • Sweat Test:
In
autonomous
area, presence of
sweat
rules out complete injury
as
sweat
fibers
are most resistant to
compression.
• • MRI: Value only in
nerve
root lesions
(e.g.
Brachial
plexus
injuries).

Management:
• 1. In
closed
Injury
(Neuropraxia
or
axonotmesis
or
:
• – Axillary
N
–
Shoulder abduction splint
• – Radial
N
–
Cock-up splint
• – Median
N/Ulnar
N
–
Knuckle
bender
splint
• – Common peroneal N
–
foot drop splint
• – Brachial plexus
injury
–
Aeroplane splint

• 2. In open injuries
• – Primary repair: Within
6–8 hrs
• – Delayed primary repair:
7–18 days
• – Secondary repair:
After 18
days

• 3. Nerve
that may be used as
nerve
donors: –
Sural nerve
• – Saphenous nerve
• 4. Neurotization that is
transfer
of
fibers
of
an
intact
nerve
to
a
damaged nerve
to
augment its
functions.
• 5. If
nerve
recovery does not take place tendon
transfer
can be carried
out, e.g. modified jones
transfer
for radial
nerve
palsy and tibialis
posterior transfer
for foot drop. Most common tendon
for transfer
is Palmaris Longus.

Good Prognostic Factors
• Growing age/Good repair
• Only motor
• Only sensory
• Distal Lesion
• Neuropraxia
Early repair
Radial
Vascularity maintained
End to end repair
GOOD NERVE

PERSENTATION
• PAIN
• LOSS OF SENSATION
• LOSS OF MOTION
• LOSS OF POWER
• LOSS OF REFLEXES
• WASTING
• TROPHIC CHANGES
(skin,sc,neurovascular,bones,muscles)
• CONTRACTURES

CLINICAL EXAMPLES
• ERB’ PALSY
• CARPAL TUNNEL SYNDROME(MEDIAN NV)
• RADIAL NERVE INJURY
• ULNAR NERVE INJURY
• SCIATIC NERVE INJURY
• LATERAL POPLITEAL NERVE INJURY

ERB’S PALSY
• BIRTH INJURY (DIFFICULT LABOUR)
• TRACTION ON NERVE ROOTS C5-6
• STRETCH-RUPTURE-AVULSION
• UPPER LIMB IN EXTENSION
• MOTHER NOTICE NO MOTION
• 90% GOOD RECOVERY
• ROLE OF SURGERY AFTER 3 MONTHS
• REMEMBER PROPER REHABILITATION
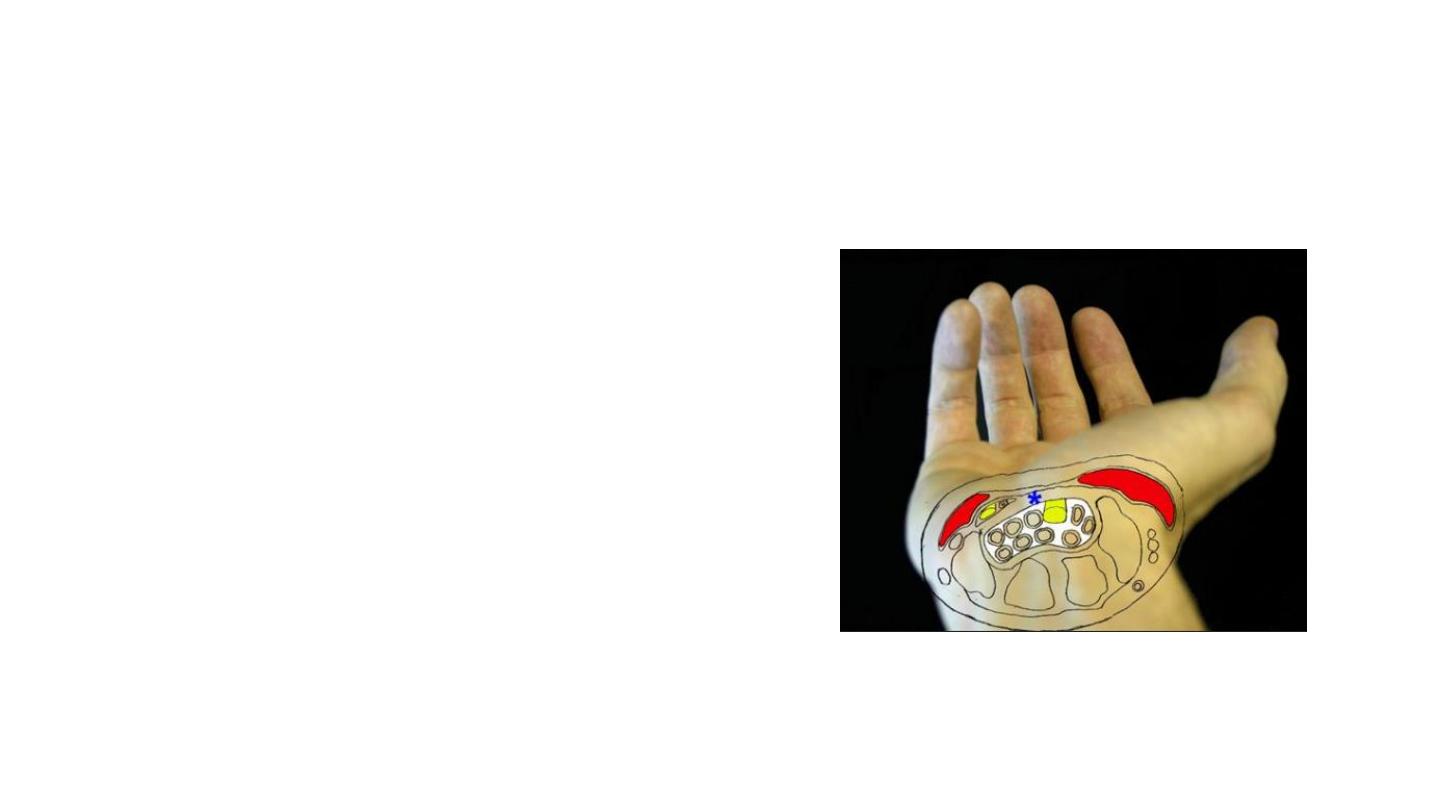
CARPAL TUNNEL SYNDROME
• MEDIAN NERVE ENTRAPMENT BY
FLEXOR RETINACULUM (TVS CARPAL
LIGAMENT)
• PAIN,NUMBNESS,NIGHT
• MANUAL WORKERS
• DIAGNOSIS
• CONS Rx
• SURGERY

CTS diagnosis
• History:
–Numbness and pain
–Often at night
–Volar aspect → thumb - index - long - radial half of ring
–Risk factors

Risk Factors
• obesity
• pregnancy
• diabetes
• thyroid disease
• chronic renal failure
• Others RA, storage diseases, alcoholism, acromegaly,
advanced age.
• Repetitive strain injury
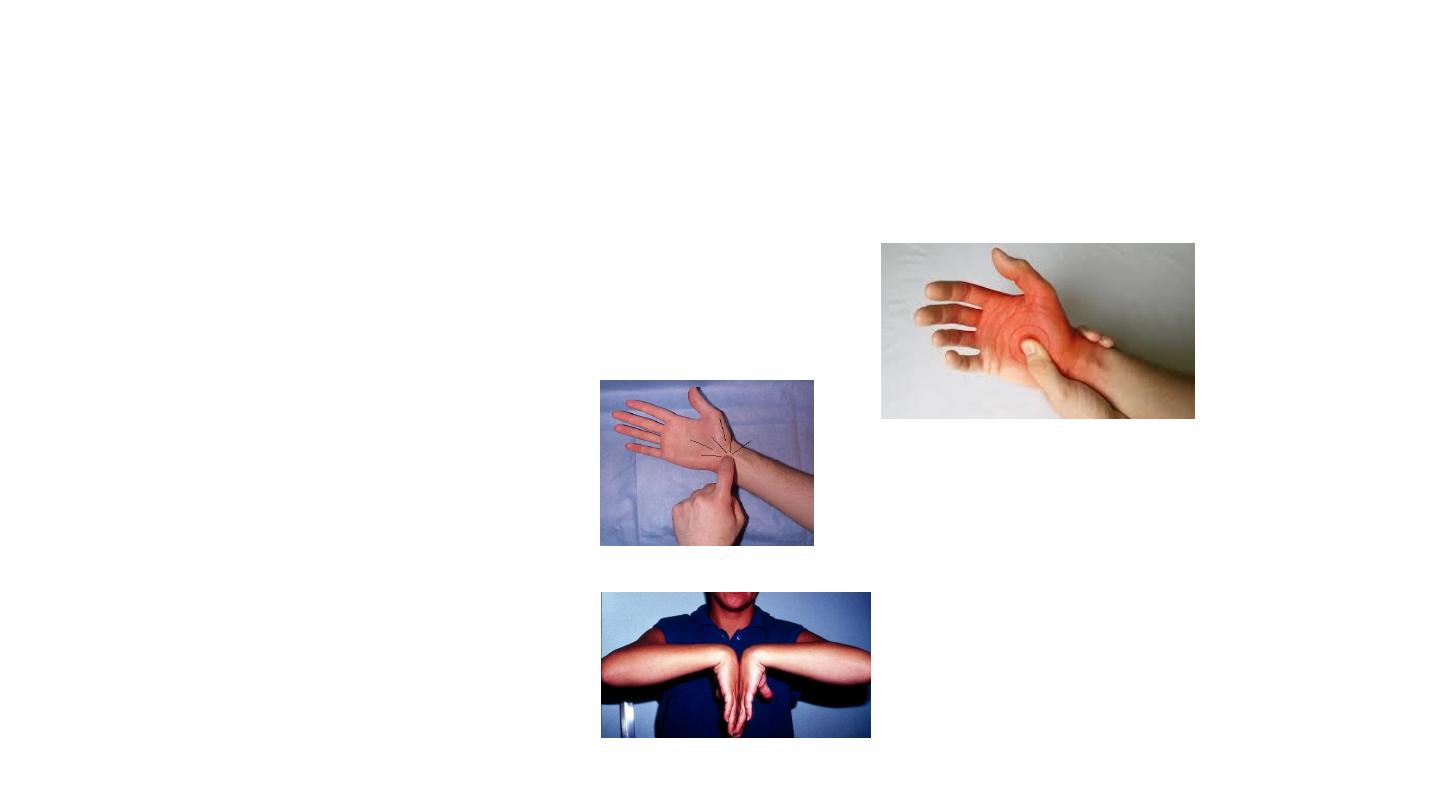
CTS diagnosis
• Physical examination:
– Durkan’s test → Most sensitive
– Tinel’s test
– Phalen’s test

CTS - Differential diagnoses
• cervical radiculopathy
• brachial plexopathy
• pronator syndrome
• ulnar neuropathy
• peripheral neuropathy of multiple etiologies
CTS Treatment
• Nonoperative
–Activity modification
–Night splints
–NSAIDs
–Steroid injection
• Operative
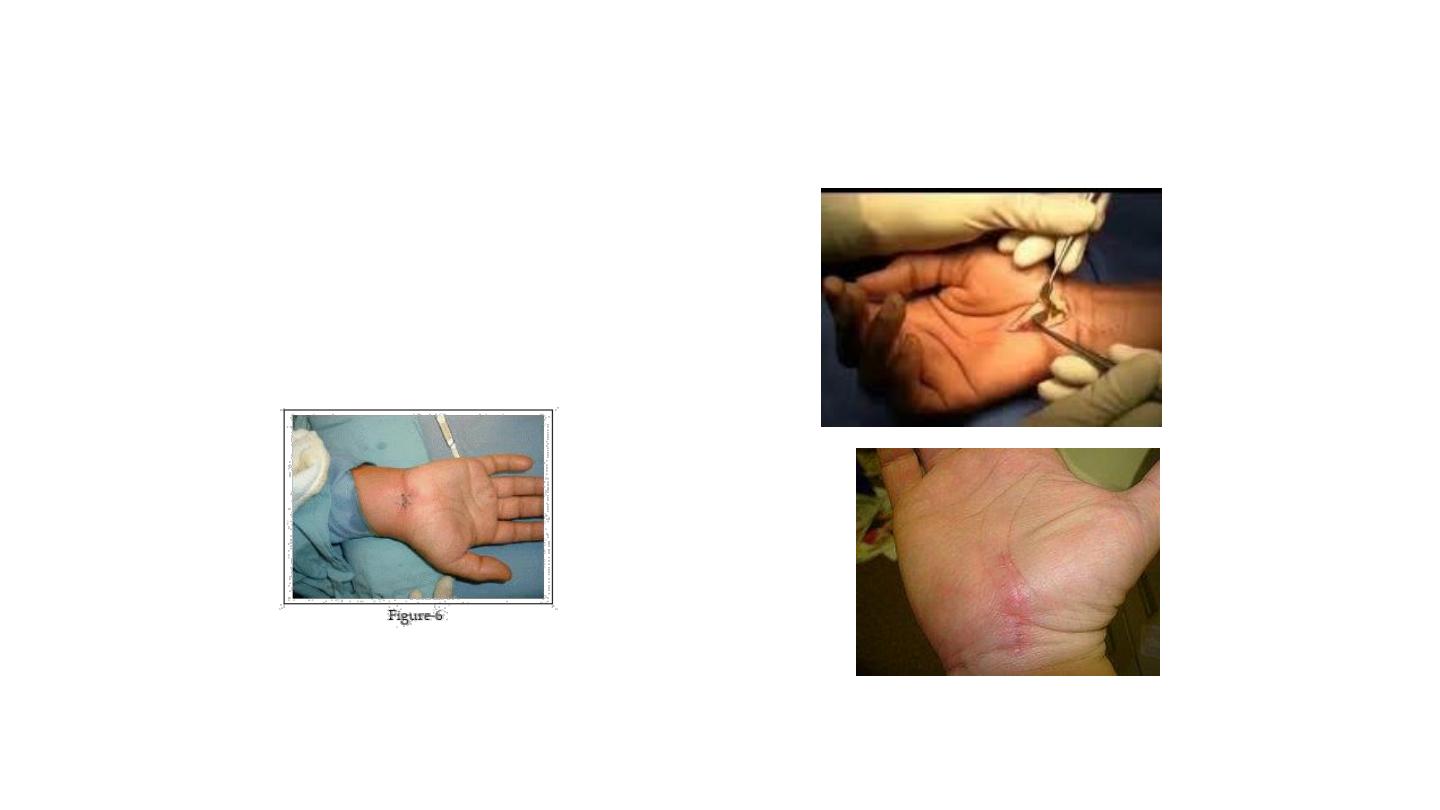
CTS – Operative
• Can be:
– Open
– Endoscopic
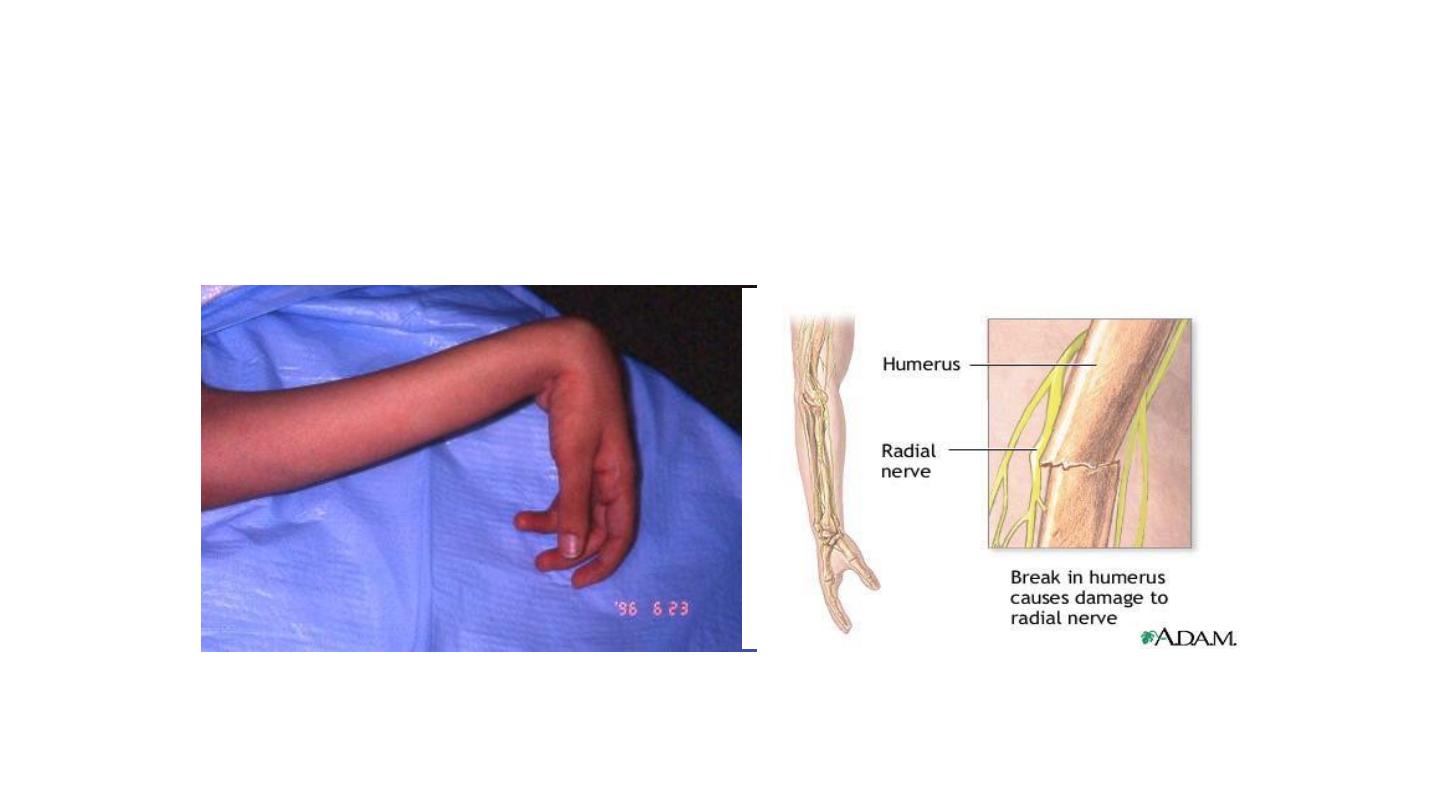
RADIAL NERVE INJURY
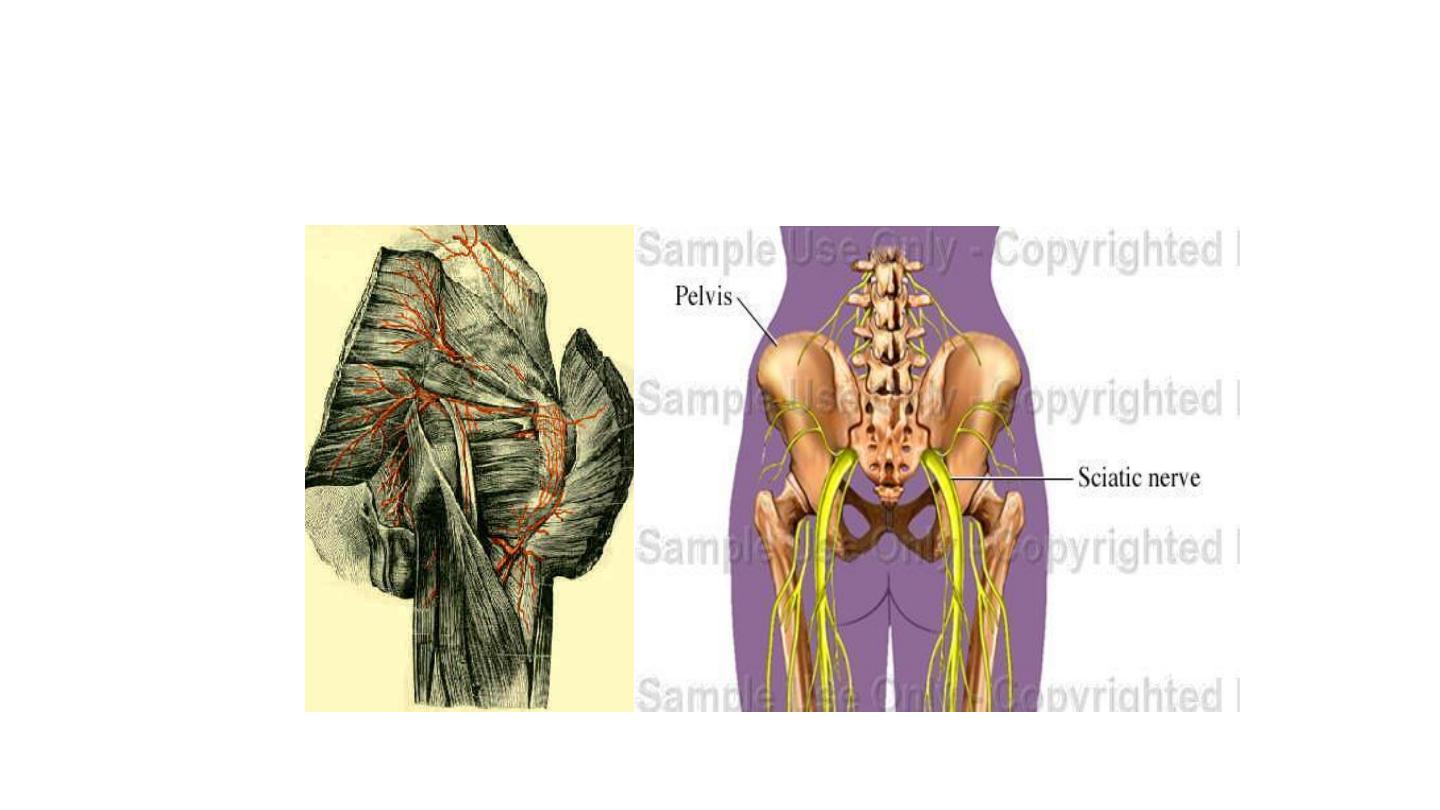
SCIATIC NERVE INJURY
The End