DEVELOPMENT OF OCCLUSION
Tooth development or odontogenesis is the complex process by which teeth form from embryonic cells, grow, and erupt into the mouth. For human teeth to have a healthy oral environment, all parts of the tooth must develop during appropriate stages of fetal development. Primary (baby) teeth start to form between the sixth and eighth week of prenatal development, and permanent teeth begin to form in the twentieth week.[1] If teeth do not start to develop at or near these times, they will not develop at all, resulting in hypodontia or anodontia.The tooth germ is an aggregation of cells that eventually forms a tooth. These cells are derived from the ectoderm of the first pharyngeal arch and the ectomesenchyme of the neural crest. The tooth germ is organized into three parts: the enamel organ, the dental papilla and the dental sac or follicle.
The enamel organ is composed of the outer enamel epithelium, inner enamel epithelium, stellate reticulum and stratum intermedium. These cells give rise to ameloblasts, which produce enamel and become a part of the reduced enamel epithelium (REE) after maturation of the enamel. The location where the outer enamel epithelium and inner enamel epithelium join is called the cervical loop.
The growth of cervical loop cells into the deeper tissues forms Hertwig Epithelial Root Sheath, which determines the root shape of the tooth. During tooth development there are strong similarities between keratinization and amelogenesis. Keratin is also present in epithelial cells of tooth germ and a thin film of keratin is present on a recently erupted tooth (Nasmyth's membrane or enamel cuticle).
The dental papilla contains cells that develop into odontoblasts, which are dentin-forming cells. Additionally, the junction between the dental papilla and inner enamel epithelium determines the crown shape of a tooth. Mesenchymal cells within the dental papilla are responsible for formation of tooth pulp.
The dental sac or follicle gives rise to three important entities: cementoblasts, osteoblasts, and fibroblasts. Cementoblasts form the cementum of a tooth. Osteoblasts give rise to the alveolar bone around the roots of teeth. Fibroblasts are involved developing the periodontal ligament which connect teeth to the alveolar bone through cementum.
All stages (bud, cap, bell, crown), growth and morphogenesis of the teeth are regulated by a certain protein.
Various phenotypic inputs modulate the size of the teeth.
Parathyroid hormone is required for tooth eruption.
Maxillary (upper) teeth
Primary teethCentralincisor
Lateralincisor
Canine
Firstmolar
Secondmolar
Initial calcification
14 wk I.U.
16 wk I.U.
17 wk I.U.
15.5 wk I.U.
19 wk I.U.
Crown completed
1.5 mo2.5 mo
9 mo
6 mo
11 mo
Root completed
1.5 yr2 yr
3.25 yr
2.5 yr
3 yr
Mandibular (lower) teeth
Initial calcification
14 wk I.U.16 wk I.U.
17 wk I.U.
15.5 wk I.U.
18 wk I.U.
Crown completed
2.5 mo3 mo
9 mo
5.5 mo
10 mo
Root completed
1.5 yr1.5 yr
3.25 yr
2.5 yr
3 yr
Human Tooth Development Timeline
The following tables present the development timeline of human teeth. Times for the initial calcification of primary teeth are for weeks in utero. Abbreviations: wk = weeks; mo = months; yr = years.
Maxillary (upper) teeth
Permanent teethCentralincisor
Lateralincisor
Canine
Firstpremolar
Secondpremolar
Firstmolar
Secondmolar
Thirdmolar
Initial calcification
3–4 mo
10–12 mo
4–5 mo
1.5–1.75 yr
2–2.25 yr
at birth
2.5–3 yr
7–9 yr
Crown completed
4–5 yr
4–5 yr
6–7 yr
5–6 yr
6–7 yr
2.5–3 yr
7–8 yr
12–16 yr
Root completed
10 yr
11 yr
13–15 yr
12–13 yr
12–14 yr
9–10 yr
14–16 yr
18–25 yr
Mandibular (lower) teeth
Initial calcification
3–4 mo3–4 mo
4–5 mo
1.5–2 yr
2.25–2.5 yr
at birth
2.5–3 yr
8–10 yr
Crown completed
4–5 yr
4–5 yr
6–7 yr
5–6 yr
6–7 yr
2.5–3 yr
7–8 yr
12–16 yr
Root completed
9 yr
10 yr
12–14 yr
12–13 yr
13–14 yr
9–10 yr
14–15 yr
18–25 yr
Stages Of Tooth Development
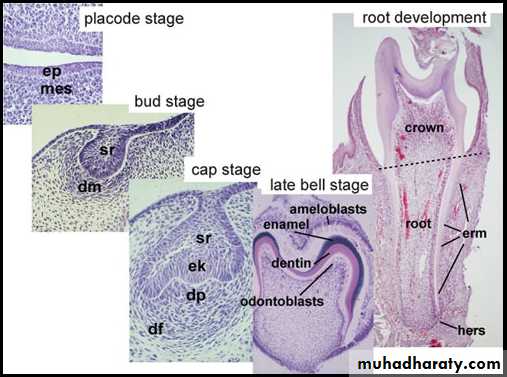
Tooth development is commonly divided into the following stages: the initiation stage, the bud stage, the cap stage, the bell stage, and finally maturation.
Initiation Stage
It occurs in the sixth to seventh week of the embryonic life. The dental lamina connects the developing tooth bud to the epithelial layer of the mouth for a significant time. This is regarded as the initiation stage.Bud stage
• The bud stage is characterized by the appearance of a tooth bud without a clear arrangement of cells. Typically, this occurs when the fetus is around 8 weeks old. The tooth bud itself is the group of cells at the periphery of the dental lamina.• Along with the formation of the dental lamina, 10 round epithelial structures, each referred to as a bud, develop at the distal aspect of the dental lamina of each arch. These correspond to the 10 primary teeth of each dental arch, and they signify the bud stage of tooth development.
Cap stage
The first signs of an arrangement of cells in the tooth bud occur in the cap stage. At this point, the tooth bud grows around the ectomesenchymal aggregation, taking on the appearance of a cap, and becomes the enamel (or dental) organ covering the dental papilla. A condensation of ectomesenchymal cells called the dental sac or follicle surrounds the enamel organ and limits the dental papilla. Eventually, the enamel organ will produce enamel, the dental papilla will produce dentin and pulp, and the dental sac will produce all the supporting structures of a tooth, the periodontium.Bell stage
The bell stage is known for the histodifferentiation and morphodifferentiation that takes place. The dental organ is bell-shaped during this stage.Then the dental lamina disintegrates, leaving the developing teeth completely separated from the epithelium of the oral cavity; the two will not join again until the final eruption of the tooth into the mouth.
The crown of the tooth, which is influenced by the shape of the inner enamel epithelium, also takes shape during this stage.
It is still uncertain why teeth form various crown shapes—for instance, incisors versus canines.
Advanced bell stage
Hard tissues, including enamel and dentin, develop during the next stage of tooth development. This stage is called the crown, or maturation stage, by some researchers. Important cellular changes occur at this time. Rapid dividing, called mitosis, stops during the crown stage at the location where the cusps of the teeth form. The first mineralized hard tissues form at this location.• The adjacent layer of cells in the dental papilla suddenly increases in size and differentiates into odontoblasts, which are the cells that form dentin.
• Outside the dentin are the newly formed ameloblasts in response to the formation of dentin, which are cells that continue the process of enamel formation; therefore, enamel formation moves outwards, adding new material to the outer surface of the developing tooth.
•
Postnatal development of the dentition
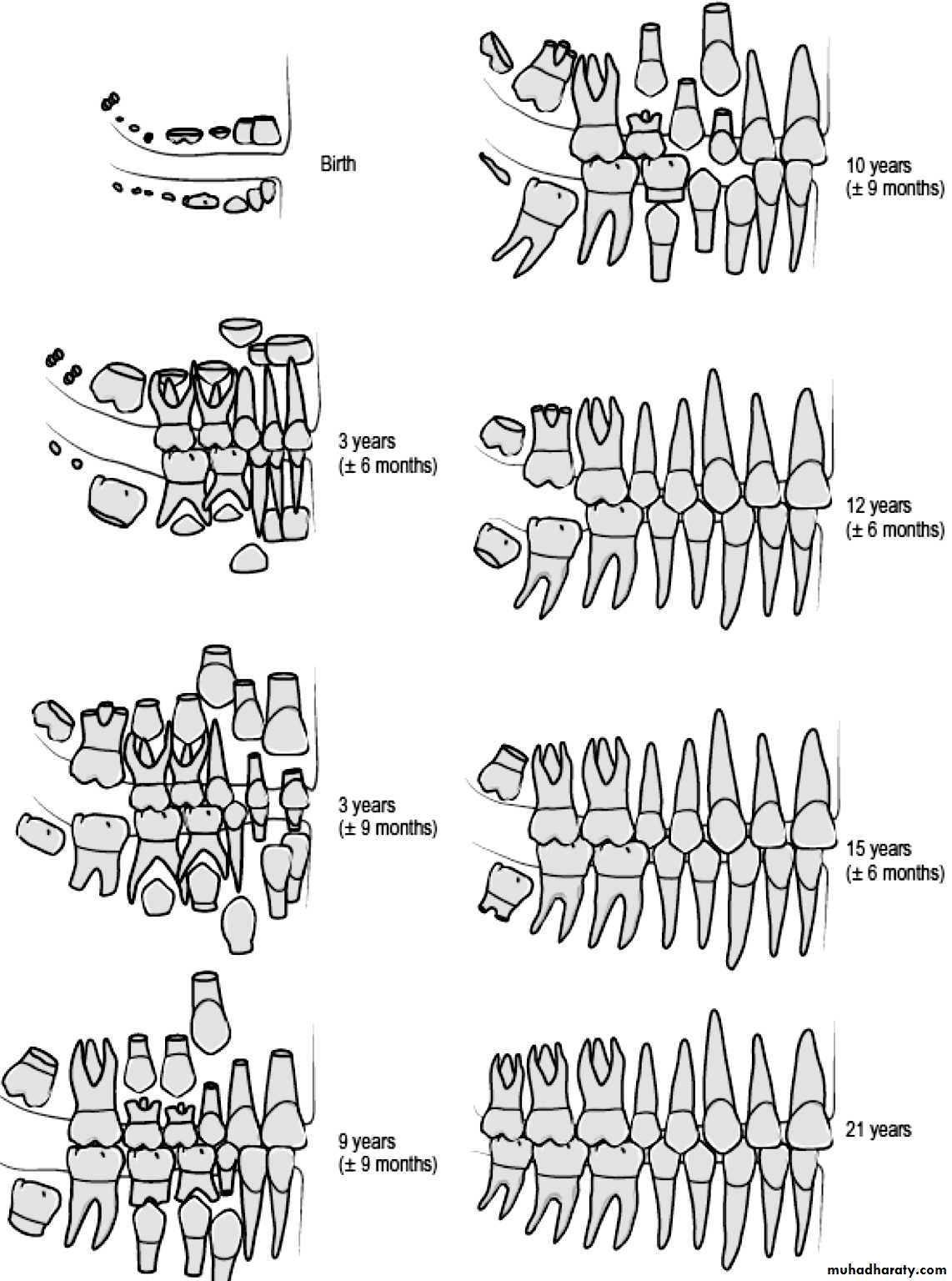
When a child is born, mineralization of all the primary tooth crowns is well happening, with this process also beginning in the first permanent molars. The primary dentition will start to erupt in the first year of life and will be established by the end of the third. The permanent dentition is heralded by eruption of the first molars at around 6 years of age and is completed in most cases, by the appearance of the third molars in the late teenage years.The jaws at birth
At birth, the maxillary dental arch is characteristically horseshoe-shaped whereas the mandibular arch assumes a wider U-shape. The mucous membrane of both the maxilla and mandible is thickened in the newborn infant to produce gum pads, which cover the alveolar processes containing the developing primary teeth.

Usually the upper jaw overlaps the lower jaw in antero-posterior and in transverse direction, in other ward: the upper jaw is wider than the lower jaw and at the same time,the lower jaw is in a retrognathic position in relation to the upper. On the upper jaw, we can see the lateral sulcus, which express to the distal margin of the upper deciduous canine and the gum pads, which is separated from the masticatory mucosa by a long and continuous groove called gingival groove.
The upper lip at this stage is usually short, and the anterior oral seal of the mouth occurs due to the contact between the lower lip and the tongue. At this age the anterior gum pads is averted anteriorly and when the child closes his mouth there is a space between the anterior gum pads and the only part that is in contact are the future growing E(s) (Es region).
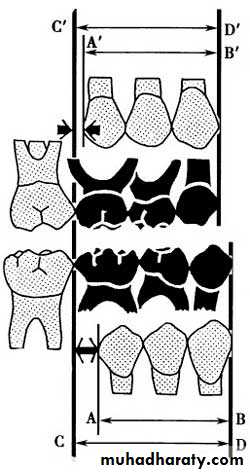
The maxillary (left) and mandibular (middle) gum pads in isolation and occlusion (right). Note the prominent lateral sulci (LS) present in both arches. A, C, external arch width; B, D, internal arch width; E, F, anterior arch length; G, overjet; H, anteroposterior relationship; I, overbite.
The elevations of the Es cannot be seen clearly, until the age of 5 months, the anterior opening of the mouth will facilitate the feeding process without discomfort to the mother, at this age usually the labial frenum is attached to the incisive papillary region and after the eruption of the deciduous it will migrate in upward direction and gives the incisive papillary attachment this is due to alveolar bone formation in association with the development of the deciduous teeth.
Occasionally a child is born with teeth already present or that undergo precocious eruption within the oral cavity
• Natal teeth are present at birth.
• Neonatal teeth erupt within the first month of life; and
• Pre-erupted teeth appear within the second and third months of life.
Natal and neonatal teeth occur in around 1: 3000 children and are usually mandibular primary incisors, although rarely they can be supernumerary teeth. They are often poorly developed, mobile and can cause ulceration of the mouth and nipple during suckling. If these teeth give rise to problems, they should be removed.
Deciduous Dentition
Usually the deciduous teeth begin to erupt at the sixth months of age until 2.5 – 3 years of age. (All the deciduous teeth will be erupted, completely, at the age of third years), and can be a source of some malaise for the child. Teething is associated with tender swollen gums, irritability, finger sucking, drooling and nocturnal crying. It is generally selflimiting but can be relieved by allowing the child to chew on clean, hard, cool objects and the provision of appropriate analgesia, either in the form of an elixir or lignocaine based teething gel. Occasionally, primary tooth eruption is preceded by the appearance of aneruption cyst, a small bluish-type swelling, which overlies the erupting tooth. These generally disappear, but can be excised if they persist.
Eruption sequence of deciduous dentition:
This includes:Lower (As) at 6th month,
Lower (Bs) at 7th month,
Upper (As) at 8th month,
Upper (Bs) at 9th moth,
Lower (Ds) at 12th month,
Upper (Ds) at 14th month,
Lower (Cs) at 16th month, upper (Cs) at 18th month,
Lower (Es) at 20th month,
Then finally, upper (Es) at 24th month.
The first sign of the formation of the deciduous teeth is at the age of 4-6 months IUL, and their roots will be completely formed after 12 – 18 months after their eruption. When these teeth erupt in the mouth, they will erupt in a vertical direction i.e. the upper long axes of the centrals coincide with the long axis of the lower incisors, and usually there is slightly increase in the over-jet.
These teeth usually present in their crept in a rotated manner, this is to occupy a less space in the child’s mouth; so that, when they erupt, they will erupted in a spaced conditions, and these spaces usually present at the mesial aspect of the upper canine and the distal aspect of the lower canine.
These spaces are termed as primary spaces or anthropoid spaces, since it looks like the spaces that are present between the teeth of the higher Apes.
Such spaces also present mesial to the Ds, these spaces that are anterior to the Ds, try to close in a way that: the distal surface of the D (upper and lower) will be located on the same terminal plane and usually the lower D is larger in mesiodistal dimension than the upper D. The Es when erupt, they erupt in the same terminal plane (flush terminal).
In summery the complete primary dentition is classically associated with a number of characteristic features:
• The arches are semi-circular in shape;
• The incisors are spaced, upright and associated with a positive overjet and overbite;
• Primate or anthropoid spaces are present, mesial to the maxillary primary canines and distal to the mandibular canines;
• The molar and canine relationship is class I; and
• The distal edges of the second primary molars are flush in the vertical plane.
Changes in spaces:
The spaces of the deciduous teeth try to increase with age due to the growth of the jaws in: antroposterior, transverse and vertical direction, and due to: attrition; since the shape of the deciduous teeth is triangular and these teeth will be subjected to a great amount of attrition due to wear at the incisal edges; so, the spaces will be increased, especially anteriorly due to the attrition. This attrition will occur at the incisal edges and the proximal surfaces since the deciduous teeth mostly converted into edge to edge relationship at a later stage.At the age of 5.5 - 6 years the permanent teeth begun to erupt, and these teeth contains an eruptive cyst, and this is filled with fluid, this fluid will exert a pressure on the roots of the deciduous teeth causing their resorption with the aid of special enzyme which is produced at this stage of age.
The roots resorption of the deciduous teeth means decrease in the root length and since the occlusal forces at the age of 5-6 years are more than those of 3 years; so, these occlusal forces together with the root resorption will increase the mobility of the deciduous teeth and if the deciduous teeth in closed case (without spacing), this will produce attrition of the proximal surfaces due to friction produced by movement during mastication, as the mobility progress the spaces will be increased and this will facilitate the process of normal shedding of the incisors.
Usually, the permanent teeth when erupt ,they are located at the palatal or lingual aspect of the deciduous incisors, causing their resorption during eruption, but sometimes, the permanent teeth could be deflected from the roots of incisors; therefore, this process will not happen in the normal way, and the permanent erupt ,while the deciduous is stay in its space.
Permanent Teeth:
Variations in the eruption sequence of the permanent teeth are common, but as a rule, the mandibular teeth erupt prior to the maxillary. Permanent teeth begin their eruption once crown formation is completed, taking between 2 and 5 years to reach the alveolar crest and a further 1 to 2 years to reach occlusion. Root development is usually completed within 2 years of eruption.Permanent teeth replace the deciduous teeth (A, B, C, D and E) by (1, 2, 3, 4 and 5); while, the molars (6, 7 and 8) are developed in a separate entity.
The sequence and timing of emergence of permanent teeth include:
1-First stage for permanent teeth emergence development).Lower 6 ⇒ at 6 years
Upper 6 ⇒ at 6 – 6.2 years
Lower 1 ⇒ at 6.5 years
Upper 1& lower 2 ⇒ at 7.5 years
Upper 2 ⇒ at 8.5 years.
There is a silent period extend from 8.5 years of age to 10 years of age, this period is called (Lull period). In this stage: there is no teeth emergence (development) or exfoliation, but there is changes in the occlusion including the anteroposterior and vertical dimension.
2-Second stage of permanent teeth emergence:
Upper 4& lower 3⇒ at 10 yearsLower 4⇒at 10.5 years
Upper & lower 5⇒ at 11 years
Upper 3⇒ at 11.5 years
Upper & lower 7⇒at 12 years
3-Third stage of permanent teeth emergence:
It is the stage of emergence of the third molars at the age between 18 to 24 years of age (some time above 25).The sequence of teeth emergence:-
For the upper permanent teeth is (61245 3 7) ⇒ 100%. While the sequence of emergence of the lower permanent teeth is either: (6123457) ⇒ in 50% of cases, or: (6124357).In the lower arch, the first premolar may erupt after the emergence of the lower canine or before it.
Normal emergence at the first stage of permanent teeth
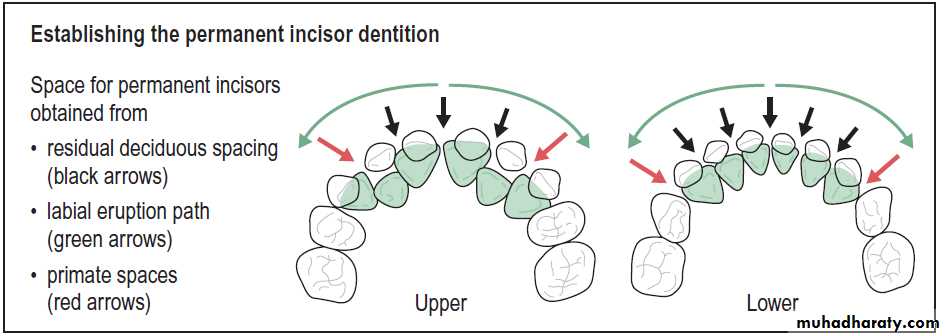
The permanent central incisors will replace the deciduous central incisors, and the deciduous lateral incisors also will be replaced by the permanent lateral incisors. Now: the question is that: How the central incisors erupt in a normal condition in spite of their mesiodistal collective width is larger than that of the deciduous teeth?
This normal emergence will occur due to these reasons:
1- Utilization of all the spaces that is present between the deciduous teeth.2- Due to proclination of the incisors during the eruption.
3- Due to the secondary spaces.
4- Transverse increase in the intercanine arch width.
About the first reason: usually there is a space mesial to the upper deciduous canine and distal to the lower deciduous canine and this space will be utilized by the incisors during their eruption. However, the space distal to the lower canine can be utilized by the buccal segment teeth during (the early mesial shift).
About the second reason: the incisors erupt in a proclined situation and this will increase the available arch length present for the permanent incisors, and this proclination is mainly due to the increase in activity of the tongue at this period (8.5 years) due to the increased amount of the growth stimulation hormone at this period.
About the third reason: during the eruption of the lower incisor, the lower deciduous canine will be pushed in a distal and buccal direction due to the fact that: the collective mesiodistal width of the permanent incisors is more than the collective mesiodistal width of the deciduous incisors, and since there is a contact between the lower deciduous canine and the upper canine during the lateral extrusion and during the protrusion ⇒ so, the upper deciduous canine will be pushed in a lateral and distal direction and this will produce an additional spaces named as: secondary spaces, which will be utilized by the permanent incisors. This will permit the permanent incisors of the adult face which is present in a small child face to erupt in a normal way.
Variations (changes) exist during the eruption of incisors:
The permanent central incisors and the lateral incisors erupt palatal to the deciduous incisors in the upper arch, and lingual to the deciduous incisors in the lower arch, and in their development (eruption), they should be guided into a downward and forward direction to contact the roots of the deciduous incisors causing their resorption.Additionally the permanent incisors located in their crypts in a (zigzag) fashion, and the lateral usually trapped by the central incisors.
Anyhow, if the incisors deflected from this path of eruption, ⇒ they will erupt lingual and/or palatal to the deciduous incisors and this will lead to “anterior cross bite”, but if there is normal path of eruption, they will erupt in a normal way. Since the lateral incisor situated lingual or palatal to the central incisor, therefore they may be influenced by: malocclusion more than the centrals; because they erupt later and if there is no available space in the dental arch ⇒the centrals will occupy the available space, and the remnant of the space may be not enough for the eruption of the lateral incisors. Therefore, they will be erupted in a rotated or cross bite condition. In the normal way: the lateral escapes from the central incisors at the time the centrals begun to erupt.
A transient anterior open bite can be associated with eruption of the incisors as they approach the occlusal plane and this invariably improves with time.
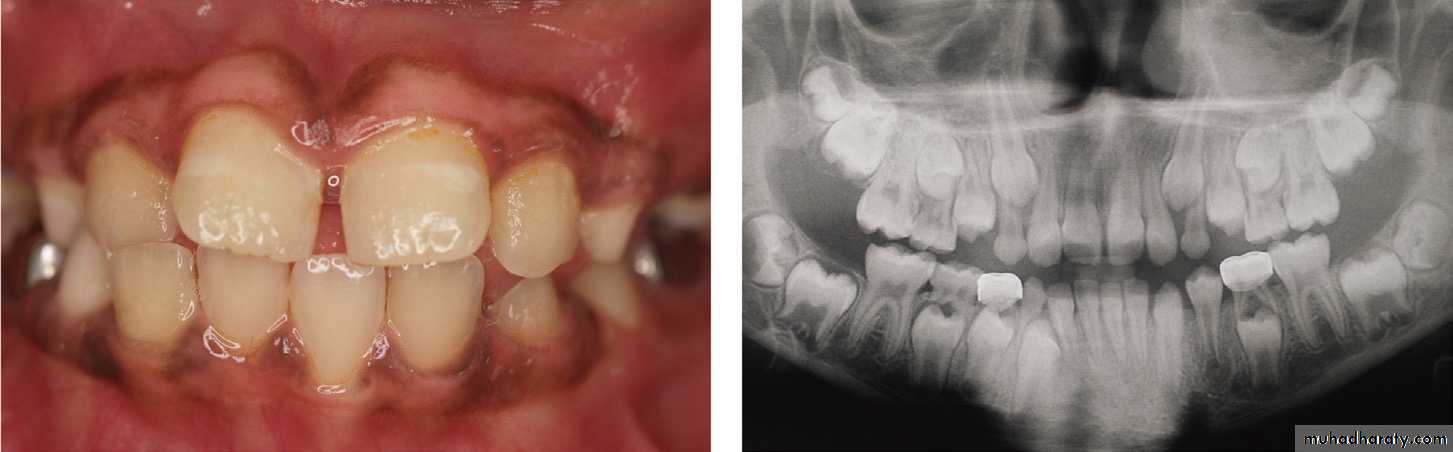
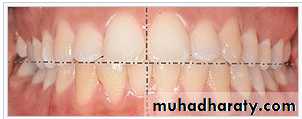
The maxillary central incisors can also be quite distally inclined when they first erupt,which produces a midline diastema between them. This physiological spacing or ‘ugly duckling’ stage is thought to be due to the combined effect of the maxillary incisor apices being initially quite close together in the anterior maxilla as the incisors erupt and lateral pressure from the erupting maxillary lateral incisors and canines. As these teeth erupt, this pressure is transferred from the apical region of the maxillary incisors more coronally, improving their inclination and usually closing the diastema.
The first molars eruption:
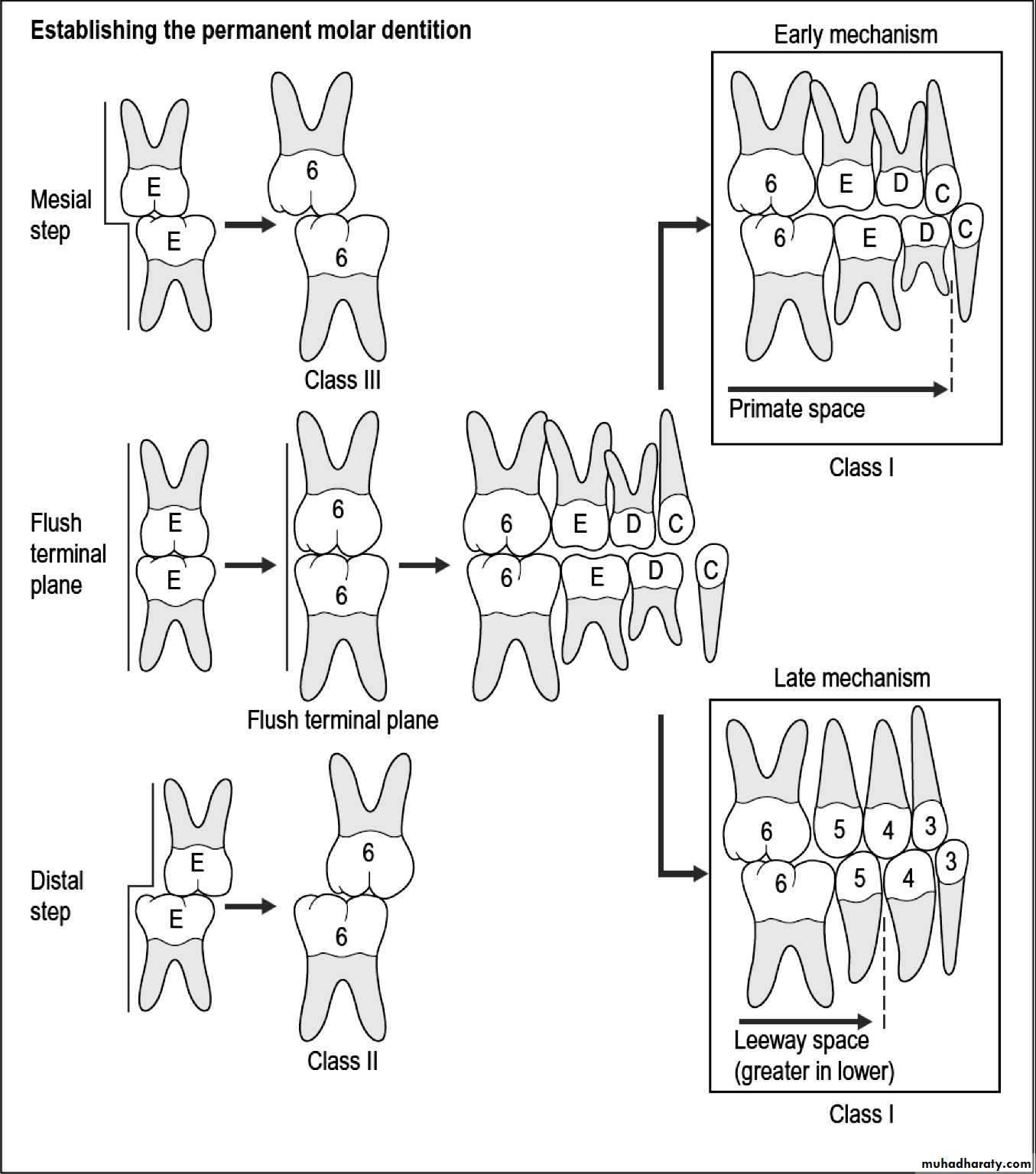
These teeth erupt as the upper and lower Es are still present. If the Es present with an cusp to cusp relationship (flush terminal plane) ⇒ the 6s will erupt cusp to cusp relationship and this is the normal situation for eruption of 6s which will developed as a Cl I in 76% of cases, Cl III in 14% and Cl II in 10%.The initial occlusal relationship of the first permanent molars is directly influenced by the primary second molar position. If these teeth are flush in the terminal plane then the first permanent molars assume a cusp-to-cusp relationship when they erupt. In order to establish a class I molar relationship, some mesial movement of the mandibular first permanent molar will be required. This is achieved by two possible mechanisms:
Early mesial shift, where the lower primate space (distal to the mandibular canine and therefore adjacent to the primary molar occlusion) is closed by forwards movement of the mandibular molar as the first permanent molar erupts; and
• Late mesial shift, where the mandibular first molar only moves in a mesial direction after loss of the second primary molar; because the mesiodistal length of the mandibular second primary molar crown is greater than the maxillary, the loss of these teeth results in greater mesial movement of the mandibular first molar.
Occasionally, a mesial step occlusion of the primary molars might have been established prior to eruption of the permanent molars; in these cases they will tend to erupt directly into a class III occlusal relationship. Alternatively, there may be a distal step occlusion, in which case the first molars will erupt into a class II relationship. However, it should be remembered that all of these relationships affecting the primary molars and therefore establishment of the molar occlusion will be significantly influenced by the relative amounts of forwards maxillary and mandibular growth that occur during this time.
The second stage of development
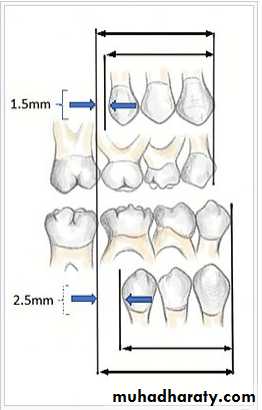
In the second stage of permanent teeth development: the C, D and E are replaced by 3, 4, and 5. In contrast to the incisor dentition, the combined mesiodistal length of the primary canine and molar teeth is greater than that of the permanent canine and premolars, an excess known as the leeway space. In the maxilla, this is approximately 1.5 mm per quadrant, whereas in the mandible it is closer to 2.5 mm, because of the increased size of the lower second primary molar.This difference in space is very important for the development of normal occlusion during late mesial shift.
The variation exist in this period includes:
Impaction of lower 5(s) due to lack of space for it due to or since it is the latter tooth which is erupted in the lower jaw mesial to the lower seven. While in the upper jaw, the lack of space will influence the canine eruption, since the latter tooth erupts prior to the upper seven in maxilla.For the lower second premolar: it may be erupted in the lingual direction or it may be impacted under the first permanent molar; while, for the upper canine: it could be erupted to the buccal direction or it could be impacted if it is directed palatals. Also in this period the reduction of the arch size “lack of space” is seen if one of these reasons is/are occur.
In Iraq, the malposed canine can be seen in female more than in male and if it is erupted into a buccal direction it takes a mesiobuccal angulation and a buccal inclination. But, if it is directed palatally then, it will be mostly impacted because the masticatory mucosa cannot be pierced by the canine due to the presence of high amount of collagen fibers. The upper canine is influenced by the problem of malocclusion in a great amount in comparison to the other teeth due to its long path of eruption “ development” since its early development occur under the orbit.
For the canine to developed normally, it should firstly directed mesially until it touches the apical part of the root of the lateral incisors, then it directed into a downward direction, and lateral direction till reaches the occlusal level. If the root of the lateral incisor is abnormal or the lateral is missed, then the canine will loss its guidance plane of eruption and it will be erupted in any direction or in any situation; therefore it will be subjected to more problem of malocclusion due to its tortuous path of eruption and due to the lack of space available for it, and due to its dependence on the presence or absence of the permanent lateral incisors.
In this stage, there is a reduction in arch length as a result of;
v Premature loss of primary second molars.v Ectopic eruption of the permanent maxillary first molar.
v Reduction in arch length as a result of caries.
About the eruption of Sevens (upper & lower):
They erupt at the age of 12 years old, and they occupy the same position of the 6s and usually the upper seven developed below the maxillary antrum and situated in a high level in the maxillary tuberosity and it takes a long path of eruption, but it is less than the canine.In comparison with canine’s path of eruption is twice as long as the second molar’s path of eruption. Therefore, it is subjected ‘7’ to a less amount of crowding in comparison with the canine.
Usually the upper sevens when erupt, they directed distally, occlusally and buccally, but for the lower sevens, they have a short path of eruption in spite of they developed at the anterior border of the ramus, but they are directed mesially and occlusally. Therefore, they are “lower 7s” subjected to a less amount of crowding in comparison with the upper sevens.
The upper 7s in their eruption try to move in a faster rate to compensate for the downward and backward growth of the maxilla at the pterygomaxillary fissure = maxillary tuberosity.
For the lower sevens: the ramus will increase in its width by bone resorption at the anterior part, and bone deposition at the posterior part. I.e. posterior border. This will provide a space for the eruption of the lower sevens.
The malocclusion of the sevens is very rare and the impaction of the upper sevens is very rare, while the lower sevens may be impacted in some instances.
Third stage of development:
The eight try to erupt between the ages of 18- 24 years of age. The path of eruption of the 8s is nearly similar to the path of eruption of the 7s. The upper 8s developed at the posteroinferior position of the maxillary tuberosity, so, these teeth are subjected to a high amount of crowding in comparison with the 6s or 7s ⇒ due to the lack of space available for them. The lower third molar may be subjected to impaction due to lack of space. These teeth may be absent congenitally due to etiological reasons since the human jaws tend to be reduced in size while, the size of teeth are remaining as it is.Occlusal changes in the permanent dentition
The dentition does not remain static throughout life. Crowding of the mandibular incisors is one of the most common problems encountered in the permanent dentition and lower incisor alignment is one of the most likely things to relapse after orthodontic treatment.Studies of untreated subjects followed from the mixed dentition into adulthood have shown a tendency for the width and length of the mandibular arch to decrease and for crowding of the anterior teeth to increase .
Primary crowding refers to a discrepancy of tooth dimension and jaw size, mainly determined genetically. Secondary crowding is caused by environmental factors, including local space conditions in the dental arches and the position and function of the tongue, the lips and the buccal musculature. Tertiary crowding occurs during adolescence and post-adolescence with a predilection for the lower labial segment.
Factors contributing to late lower incisor crowding may include:
• Mandibular growth rotations;• Physiologic mesial drift;
• Soft tissue maturation;
• Degenerative periodontal changes allowing teeth to drift under light pressures;
• Change in diet and lack of interproximal wear;
• Tooth size and shape;
• Tooth loss and drifting leading to changes in occlusal function; and
• Mandibular third molars – presence and position.
In reality, all of these factors may contribute to the development of late lower incisor crowding but the contribution of developing third molars is regarded as being minimal as crowding can develop even in the absence of their development. The prophylactic removal of developing third molars is not recommended to prevent late lower incisor crowding.

Tooth eruption
Although researchers agree that tooth eruption is a complex process, there is little agreement on the identity of the mechanism that controls eruption.[Some commonly held theories that have been disproven over time include: (1) the tooth is pushed upward into the mouth by the growth of the tooth's root, (2) the tooth is pushed upward by the growth of the bone around the tooth, (3) the tooth is pushed upward by vascular pressure, and (4) the tooth is pushed upward by the cushioned hammock.
The cushioned hammock theory, first proposed by Harry Sicher, was taught widely from the 1930s to the 1950s. This theory postulated that a ligament below a tooth, which Sicher observed under a microscope on a histologic slide, was responsible for eruption. Later, the "ligament" Sicher observed was determined to be merely an artifact created in the process of preparing the slide.
The most widely held current theory is that while several forces might be involved in eruption, the periodontal ligaments provide the main impetus for the process. Theorists hypothesize that the periodontal ligaments promote eruption through the shrinking and cross-linking of their collagen fibers and the contraction of their fibroblasts.
• Although tooth eruption occurs at different times for different people, a general eruption timeline exists. Typically, humans have 20 primary (baby) teeth and 32 permanent teeth.
• Tooth eruption has three stages. The first, known as deciduous dentition stage, occurs when only primary teeth are visible. Once the first permanent tooth erupts into the mouth, the teeth are in the mixed (or transitional) dentition. After the last primary tooth falls out of the mouth—a process known as exfoliation—the teeth are in the permanent dentition.
• Primary dentition starts on the arrival of the mandibular central incisors, usually at eight months, and lasts until the first permanent molars appear in the mouth, usually at six years. The primary teeth typically erupt in the following order: (1) central incisor, (2) lateral incisor, (3) first molar, (4) canine, and (5) second molar.
•
• As a general rule, four teeth erupt for every six months of life, mandibular teeth erupt before maxillary teeth, and teeth erupt sooner in females than males.
• During primary dentition, the tooth buds of permanent teeth develop below the primary teeth, close to the palate or tongue.
•
• Mixed dentition starts when the first permanent molar appears in the mouth, usually at six years, and lasts until the last primary tooth is lost, usually at eleven or twelve years.

• Permanent teeth in the maxilla erupt in a different order from permanent teeth on the mandible. Maxillary teeth erupt in the following order: (1) first molar (2) central incisor, (3) lateral incisor, (4) first premolar, (5) second premolar, (6) canine, (7) second molar, and (8) third molar. Mandibular teeth erupt in the following order: (1) first molar (2) central incisor, (3) lateral incisor, (4) canine, (5) first premolar, (6) second premolar, (7) second molar, and (8) third molar. Since there are no premolars in the primary dentition, the primary molars are replaced by permanent premolars.
• The permanent dentition begins when the last primary tooth is lost, usually at 11 to 12 years, and lasts for the rest of a person's life or until all of the teeth are lost (edentulism). During this stage, third molars (also called "wisdom teeth") are frequently extracted because of decay, pain or impactions. The main reasons for tooth loss are decay and periodontal disease.
•
Eruption times for primary and permanent teeth [52]
Primary teethTeeth
Centralincisor
Lateralincisor
Canine
Firstpremolar
Secondpremolar
Firstmolar
Secondmolar
Thirdmolar
Maxillary teeth
10 mo
11 mo
19 mo
-
-
16 mo
29 mo
-
Mandibular teeth
8 mo
13 mo
20 mo
-
-
16 mo
27 mo
-
Permanent teeth
Teeth
CentralincisorLateralincisor
Canine
Firstpremolar
Secondpremolar
Firstmolar
Secondmolar
Thirdmolar
Maxillary teeth
7–8 yr
8–9 yr
11–12 yr
10–11 yr
10–12 yr
6–7 yr
12–13 yr
17–21 yr
Mandibular teeth
6–7 yr
7–8 yr
9–10 yr
10–12 yr
11–12 yr
6–7 yr
11–13 yr
17–21 yr
Occlusion
• Dental Occlusion, means simply the contact between teeth. More technically, it is the relationship between the maxillary (upper) and mandibular (lower) teeth when they approach each other, as occurs during chewing or at rest.
• Static occlusion refers to contact between teeth when the jaw is closed and stationary,
• while dynamic occlusion refers to occlusal contacts made when the jaw is moving.
• The masticatory system also involves the periodontium, the TMJ (and other skeletal components) and the neuromusculature, therefore the tooth contacts should not be looked at in isolation.
•
• As the primary (baby) teeth begin to erupt at 6 months of age, the maxillary and mandibular teeth aim to occlude with one another. The erupting teeth are moulded into position by the tongue, the cheeks and lips during development.
• Upper and lower primary teeth should be correctly occluding and aligned after 2 years whilst they are continuing to develop, with full root development complete at 3 years of age.
Development of occlusion
• Around a year after development of the teeth is complete, the jaws continue to grow which results in spacing between some of the teeth (diastema). This effect is greatest in the anterior (front) teeth and can be seen from around age 4 – 5 years. This spacing is important as it allows space the permanent (adult) teeth to erupt into the correct occlusion, and without this spacing there is likely to be crowding of the permanent dentition.
•

In order to fully understand the development of occlusion and malocclusion, it is important to understand the premolar dynamics in the mixed dentition stage (when both primary and permanent teeth are present). The permanent premolars erupt ~9–12 years of age, replacing the primary molars. The erupting premolars are smaller than the teeth they are replacing and this difference in space between the primary molars and their successors (1.5mm for maxillary, 2.5mm for mandibular[), termed Leeway Space. This allows the permanent molars to drift mesially into the spaces and develop normal alignment.
Leeway space is the size differential between the primary posterior teeth (C,D,E) and the permanent teeth (canine, first and second pre-molar). Maxillary space of 1.5mm, mandibular 2.5mm can be seen.
Incisor and molar classification
• In order to describe the relationship of the maxillary molars to the mandibular molars, the Angle’s classification of malocclusion has commonly been used for many years.• This system has also been adapted in an attempt to classify the relationship between the incisors of the two arches.
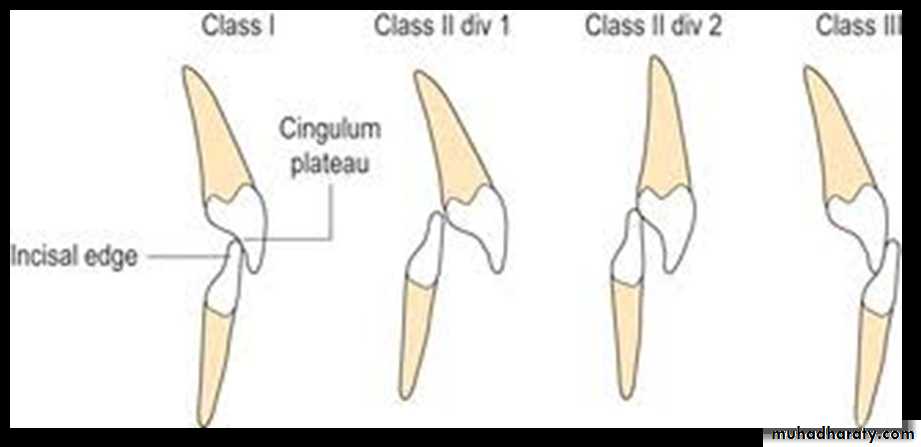
Incisor Relationship
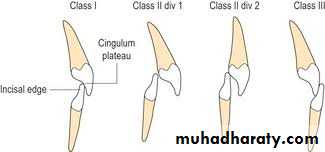
When describing the relationship between maxillary and mandibular incisors, the following categories may be referred to:• Class I: Mandibular incisors contact the maxillary incisors in the middle third or on the cingulum of the palatal surface
Incisor Relationship
• Class II: Mandibular incisors contact the maxillary incisors on the palatal surface, in the gingival third or posterior to the cingulum. This class may be further subdivided into division I and division II:• Division I includes maxillary incisors which are proclined (90%) and these individuals have a greater (overjet) horizontal overlap
• Division II includes those with retroclined (10%) incisors, which leads to an increase in (overbite) vertical overlap
Incisor Relationship
• Class III: Mandibular incisors occlude with the maxillary incisors on the palatal surface, in the incisal third specifically or anterior to the cingulum• In some cases the overjet is reversed (<0mm) and the mandibular incisors lie anterior to the maxillary incisors
Molar Relationship
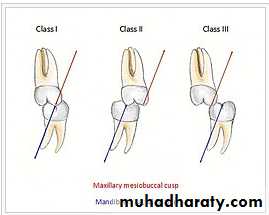
classification, observed when locating the mesial buccal cusp of the maxillary first molar and buccal groove of the mandibular first molar.
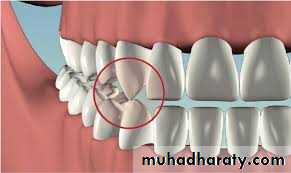
Class I: The mandibular first molar occludes mesially to the maxillary first molar, with the mesiobuccal cusp of maxillary first molar occluding in the buccal groove of mandibular first molar
• Class II: The mesiobuccal cusp of the maxillary first molar occludes anterior to the buccal groove of the mandibular first molar
• Class III: If the mesiobuccal cusp of the maxillary first molar occludes posterior to the buccal groove of the mandibular first molar.
• Classification of occlusion and malocclusion play an important role in diagnosis and treatment planning in orthodontics.
• Class I relationships are thought to be “ideal”, however this classification does not take into consideration the positions of the two TMJ’s .
• Class II and III molar and incisor relationships are thought to be forms of malocclusion, however not all of these are severe enough to require orthodontic treatment.
•
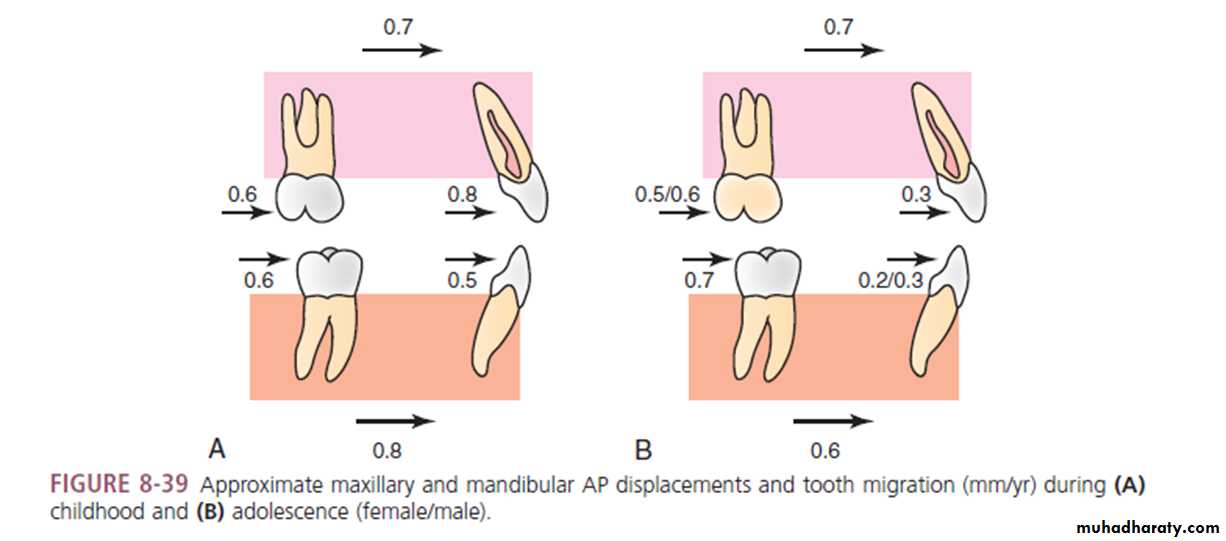
Arch Development, ToothMigration, and Eruption
The oral apparatus is the region of the craniofacial complex that holds the greatest potential for adaptive changes. Dental arch width and perimeter change dramatically, especially during the transitions to the early mixed and permanent dentitions.• Maxillary intercanine width increases approximately 3 mm during the transition to early mixed dentition and an additional 2 mm with the emergence of permanent canines).
• Mandibular intercanine width increases approximately 3 mm during initial transition but shows little or no change with the eruption of the permanent canines.
• Intermolar widths progressively increase during childhood and adolescence, approximately 4 to 5 mm for the maxilla and 2 to 3 mm for the mandible between 6 and16 years of age
• Maxillary arch depth (incisors to molars) decreases slightly during the transition to the early mixed dentition, increases 1 to 2 mm with emergence of permanent incisors, and then decreases approximately 2 mm with loss of the deciduous first and second molars.
• Mandibular arch depth decreases slightly during the transition to mixed dentition, maintains its dimension during most of the mixed dentition, and then decreases 2 to 3 mm with the loss of the deciduous first and second molars.
• Maxillary arch perimeter from first molars to first molars increases 4 to 5 mm during early mixed dentition and then decreases approximately 4 mm during late mixed dentition, resulting in only a slight overall increase between 5 and 18 years of age).
• Mandibular arch perimeter, from first molar to first molar, on the other hand, increases approximately 2 mm during early mixed dentition and decreases 4 to 6 mm during late mixed dentition, resulting in overall decreases of 3.5 and 4.5 mm in males and females, respectively.
• Perhaps most important from a clinical perspective, the teeth continue to migrate and erupt throughout childhood and adolescence, even after they have attained functional occlusion. The posteruptive movements of teeth are directly related to the spaces created by growth displacements and movements of other teeth.
Dentoalveolar compensation is the mechanism that coordinates their eruption and migration relative to their jaw bases; it maintains the relationships of teeth within and between the upper and lower dental arches. Dentoalveolar compensation depends on a normal eruptive system, dental equilibrium, and influences of neighboring teeth.
• During childhood, the maxillary incisor drifts anteriorly at a greater rate than the maxillary molar (0.8 vs. 0.6 mm/yr, respectively), which accounts for the arch depth increases evident between 6 and 12 years of age.
• In contrast, the mandibular molars drift anteriorly at a slightly greater rate than the incisors,resulting in a net loss of arch depth. Between 10 and 15 years of age, the molars (0.5 to 0.7 mm/yr) show significantly greater amounts of anterior drift than the incisors (0.3 mm/yr).
• Substantial amounts of eruption occur throughout growth.
• During childhood, the maxillary first molars and incisors erupt at a rate of approximately 1.0 mm/yr, while their mandibular counterparts erupt at a rate of approximately 0.5 mm/yr.• During adolescence, the maxillary molars and incisors erupt at rates of 1.2 to 1.4 mm/yr and 0.9 mm/yr, respectively. The mandibular molars and incisors erupt at a rate of 0.5 to 0.9 mm/yr, with little or no differences between incisor and molar eruption.
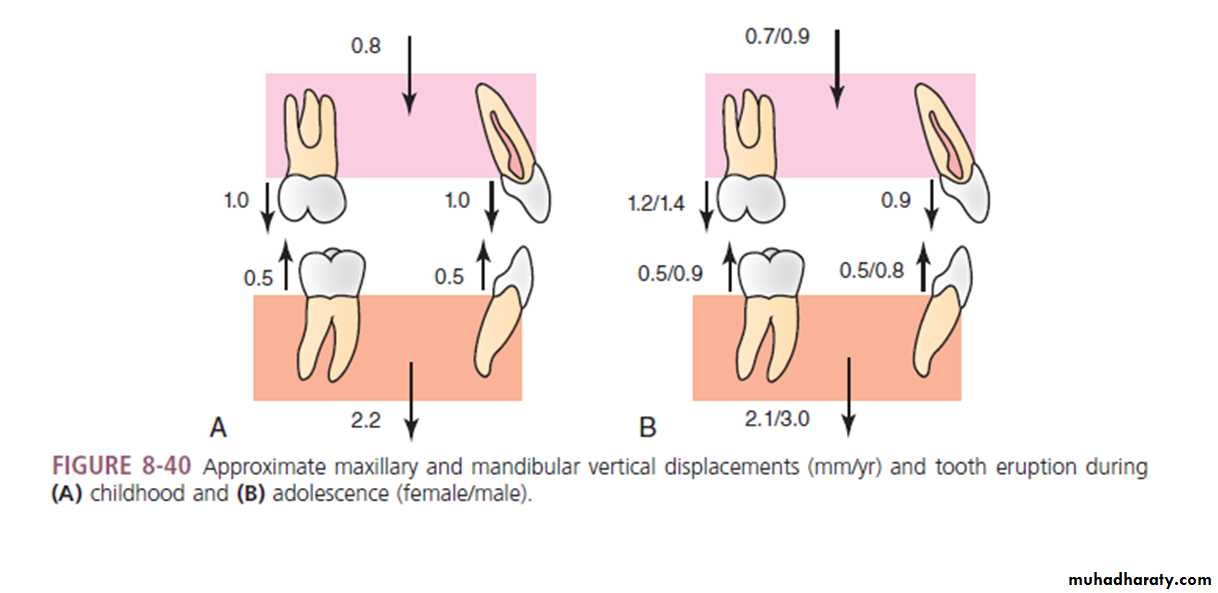
• The amounts of eruption that occur are associated closely with the inferior displacements of the midface and, especially, the mandible.
• During childhood, there is little or no evidence of sexual dimorphism in the migration and eruption of teeth. In contrast, there is a relatively high degree of dimorphism during adolescence in mandibular eruption, with boys showing almost twice as much eruption as girls. The maxillary teeth show only limited sex differences, pertaining primarily to the molars.
Occlusal terminology
Intercuspal Position - The complete intercuspation of opposing teeth independent of condylar position.
Intercuspal Position (ICP), also known as Habitual Bite, Habitual Position or Bite of Convenience , is defined at the position where the maxillary and mandibular teeth fit together in maximum interdigitation. This position is usually the most easily recorded and is almost always the occlusion the patient closes into when they are asked to 'bite together'. This is the occlusion that the patient is accustomed to, hence sometimes termed the Habitual Bite.
Centric Relation (CR) describes a reproducible jaw relationship (between the mandible and maxilla) and is independent of tooth contact. This is the position in which the mandibular condyles are located in the fossae in an antero-superior position against the posterior slope of the articular eminence. It is said that in CR, the muscles are in their most relaxed and least stressed state. This position is not influenced by muscle memory, but rather by the ligament which suspend the condyles within the fossa. Therefore it is the position that dentist’s use to create new occlusal relationships as for example, while making maxillary and mandibular complete dentures.
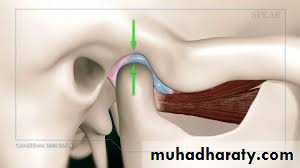
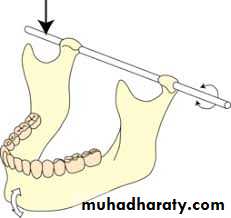
When the mandible is in this retruded position, it opens and closes on an arc of curvature around an imaginary axis drawn through the centre of the head of both condyles. This imaginary axis is termed the terminal hinge axis.
Centric Occlusion (CO) refers to the occlusion where the teeth are in maximum intercuspation in CR. Posselt (1952) determined that only in 10% of natural tooth and jaw relationships does (intercuspal position)ICP = CO (maximum intercuspation in CR).
Guidance, natural teeth and function
Bennet Angle - The angle formed between the sagittal plane and the condyles, as the mandible moves laterally.Mandibular movements are guided by two different systems; the ‘posterior’ guidance system and the ‘anterior’ guidance system
Posterior guidance system
Posterior guidance refers to TMJ articulations and associated structures . It is the condyles within the fossa and the associated muscles and ligaments together with its neuromuscular link that determines mandibular movements. Lateral, protrusive and retrusive excursions of the mandible are guided by the posterior system.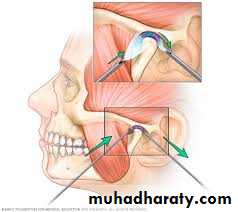
Lateral excursions
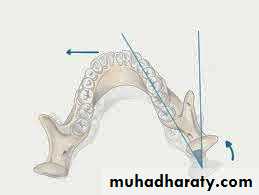
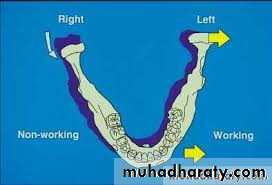
• The maximum lateral movement of the mandible to the left or right side is approximately 10-12mm• The primary movement in lateral excursions occurs on the non-working side (NWS) condyle (also called the balancing or orbiting condyle). The NWS condylar head moves in a downward, forward and medial direction. This movement is defined against two separate planes, the vertical and horizontal plane
Protrusive movements
• The condylar heads predominantly translate forwards and downwards along the distal face of the articular face in the glenoid fossa. Protrusive movements are restricted by the ligamentous structures to a maximum of ~8-11mm (depending on skull morphology and size of subject)
Retrusive movements
• As for protrusion, this movement is restricted by the ligamentous structures and the maximum retrusive limit is usually ~1mm however 2-3mm is rarely seen in some patients.
We can not influence the posterior guidance system through dental restorative treatment.

Anterior guidance system
Anterior guidance refers to the influence of contacting teeth limiting mandibular movements, whether that may be anterior or posterior tooth contacts, these determinants are anterior to the TMJ. This can be further classified into:Canine Guidance
• Dynamic occlusion that occurs on the canines during lateral excursions of the mandible.• These teeth are best suited to accept horizontal forces in eccentric movements due to their long roots and good crown/root ratio
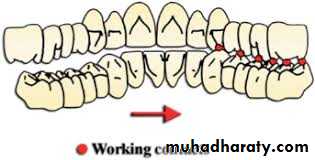
Group Function
• Multiple contact relations between the maxillary and mandibular teeth in lateral movements on the (working side)WS whereby simultaneous contact of several teeth acts as a group to distribute occlusal forces.
• It is preferable for this guidance to be as anterior as possible e.g. premolars rather than molars, as there is increased force applied when the contacts are closer to the TMJ.

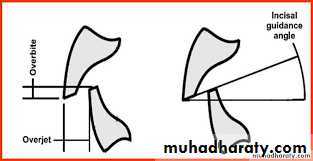
Incisal Guidance
• The influence of the contacting surfaces of the mandibular and maxillary anterior teeth on mandibular movements is characterised by the overbite and overjet of the maxillary incisors.