Diseases with normal CXR : serious resp. disease may have normal CXR, sometimes
only possible to detected abn. By compare with prev. Or later examinations, e.g.:
1- obst. Air way dis. As asthma, emphysema.
2- small lesions: us. Impossible to see solitary lung mass or consolidation less than 1 cm.
Even 2 – 3 cm CA lung may very difficult to identify.
Endobronchial lesions as CA, can not dx. On routine films unless cause collapse or
consolidation.
3- pulm. Emb. Without infarction even with life threatening emb.
4- infections: as in patient with miliary TB.
5- diffuse pulm. Fibrosis
6- pleural abn.: as dry pleurisy.
Small pl. fluid may be impossible to dx. On PA and lateral films
7- med. Masses: plain CXR very insensitive to dx. Med. Masses, LNs, med. Fluid
collections.
Abn. Chest: if the abn. Surrounded on all sides by aerated lung, it must arise within
the lung.
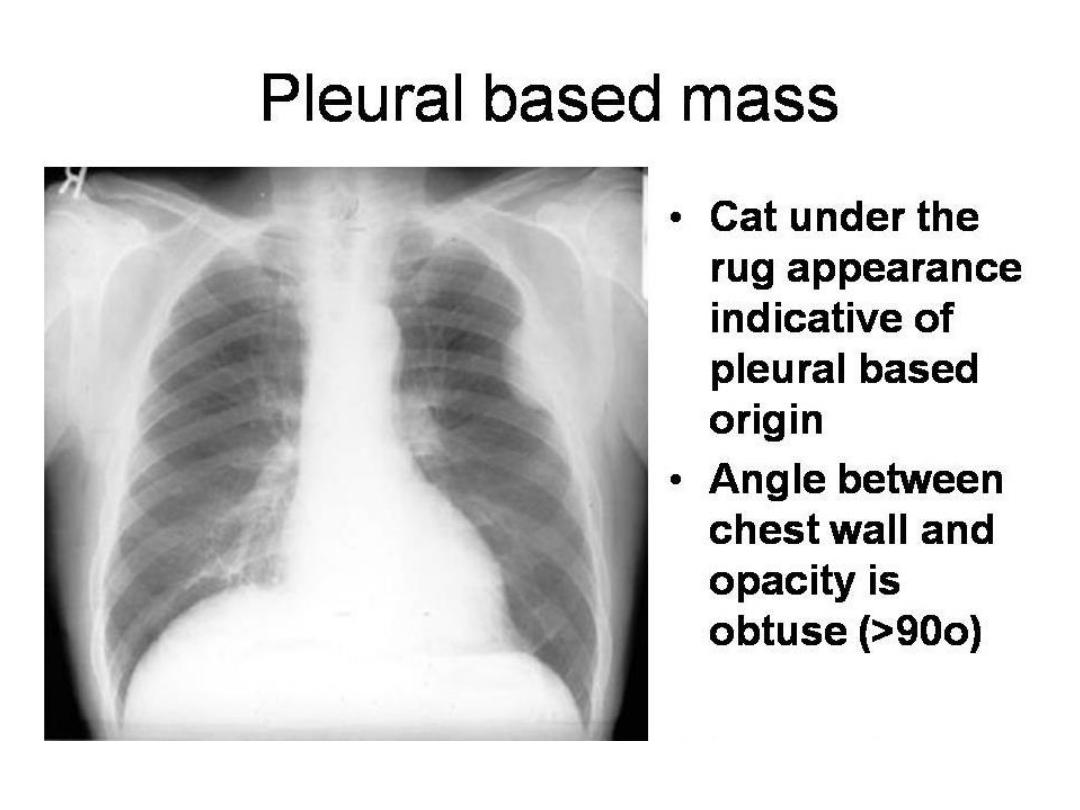
If the shadow has broad base, smooth convex border projecting into the lung, well
defined outline, so it is pl., extrapl. Or med. In origin.
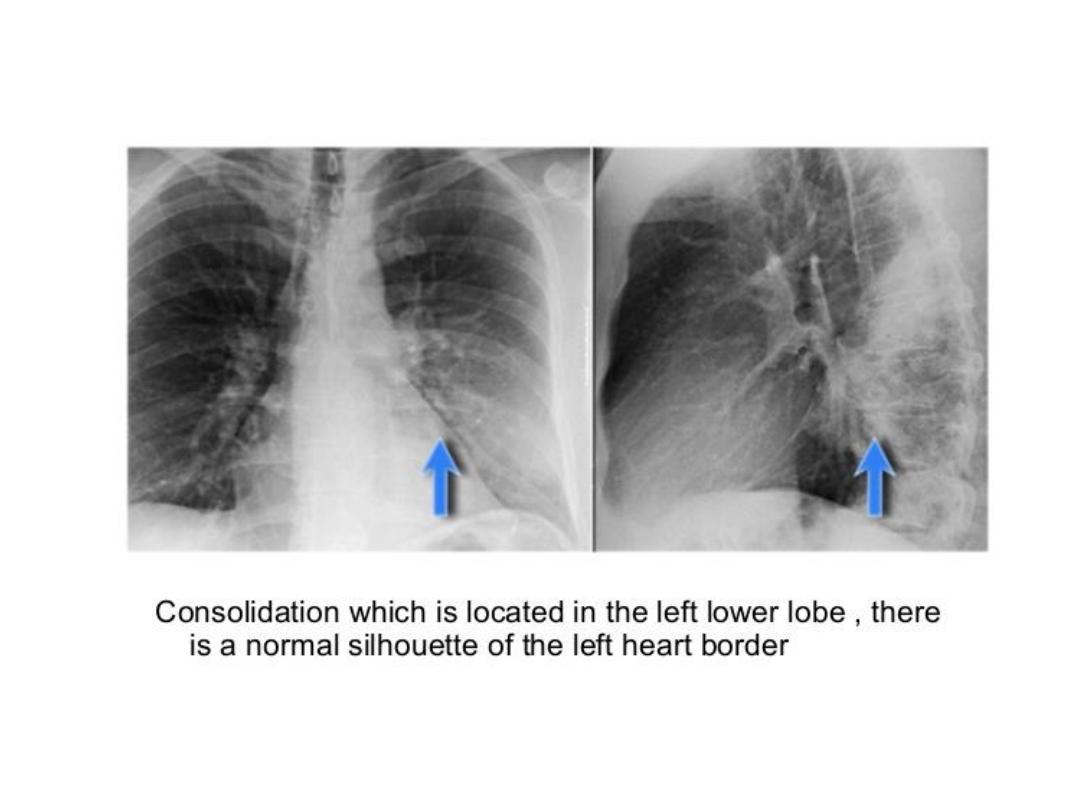
Silhouette sign: invaluable sign for localizing dis. From plain CXR.
Intrathoracic lesion touching heart, aorta or diaph. Obliterate their borders
It has two important applications:
1- localize shadow by observing which border is obliterated, e.g.: loss of heart border means the
shadow in ant. Half of the chest, loss of diaph. Outline indicate the dis. Of pl. or in lower lobes.
2- it makes possible on occasions to dx. Disorders as consolidation or collapse even when its
presence is uncertain, when it is in contact with med. Or diaph., losing their sharp outlines.
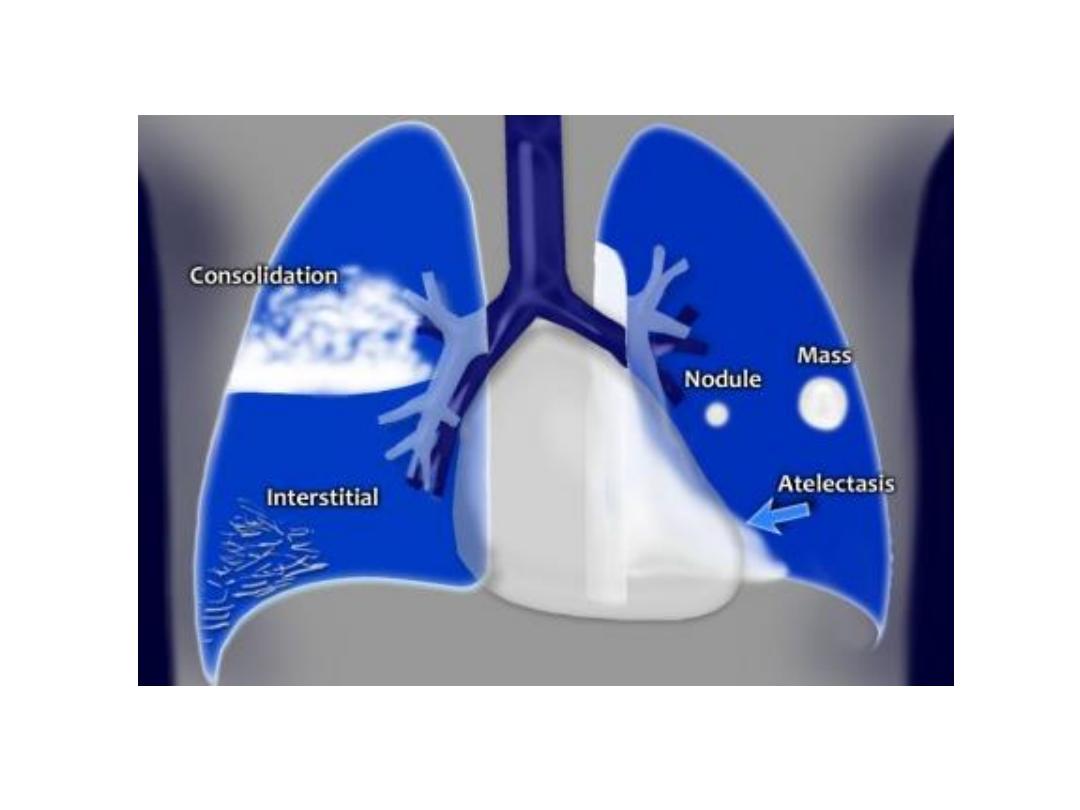
Radiological signs of lung dis. :
Air space filling: means replacement of air in alveoli by fluid or rarely by other materials.
The fluid either exudate : often called consolidation, or transudate: pulm. Edema.
Signs of consolidation: 1- a shadow with ill defined borders except when in contact with
fissure.
2- air bronchogram: if alveoli filled with fluid, the air within bronchi contrasts with fluid in
adjacent lung.
3- silhouette sign: i.e. loss of visualization of adjacent med. Or diaph. Outline.
Consolidation of a whole or majority of a lobe is virtually diagnostic of bacterial pneumonia.
Lobar consolidation produce opaque lobe except for air bronchogram.
Patchy consolidation: one or more patches of ill defined shadowing, is usually due to: pn.,
infarction, contusion, and immunological disorders.
Cavitation(abscess formation) : within consolidated areas in the lung may occur with many
bact. And fungal infections, occasionally in infarction and Wegener granulomatosis.
Abscess formation only recognizable once there is communication with bronchial tree,
allowing liquid Centre to coughed up and replaced by air, the air then seen as transradiancy
within consolidation, and air fluid level may be present.
CT is better and more sensitive than plain CXR for cavitation.
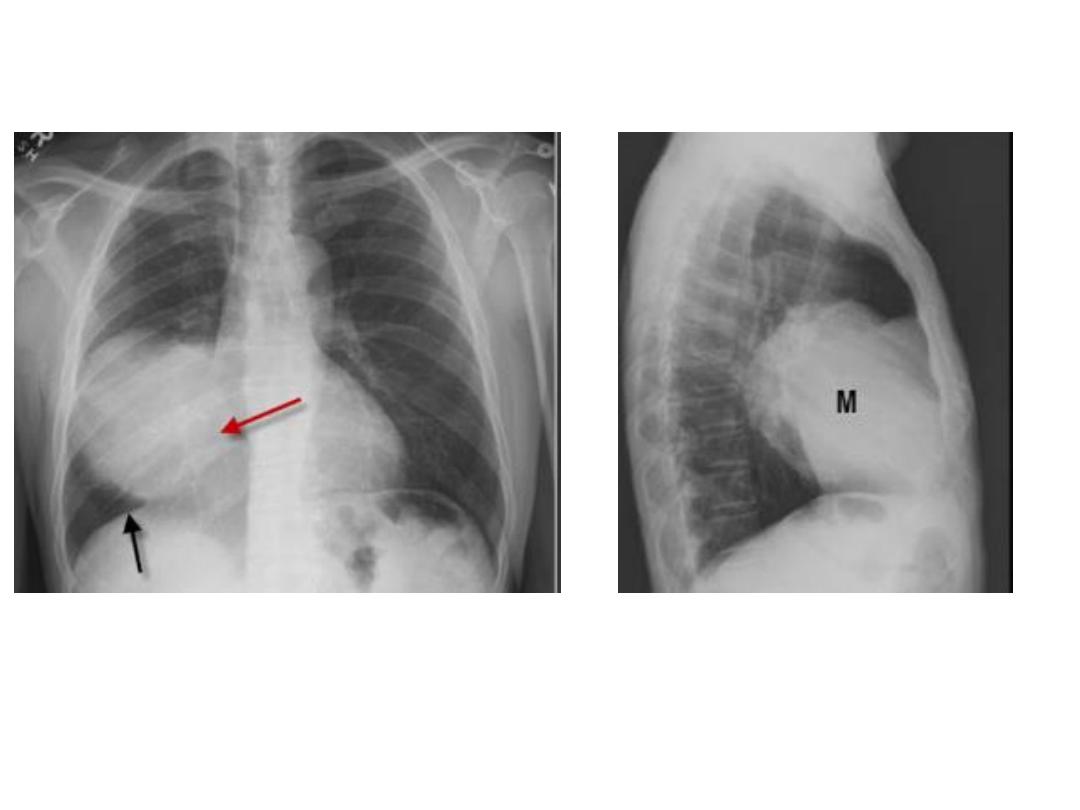
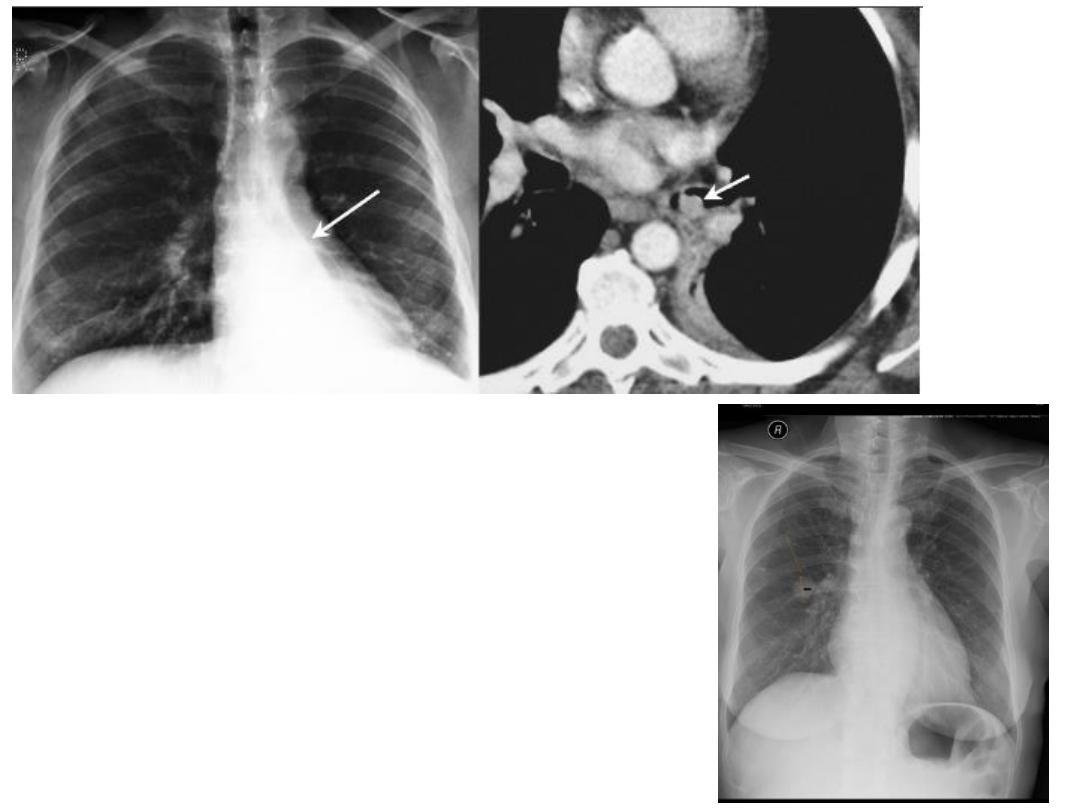
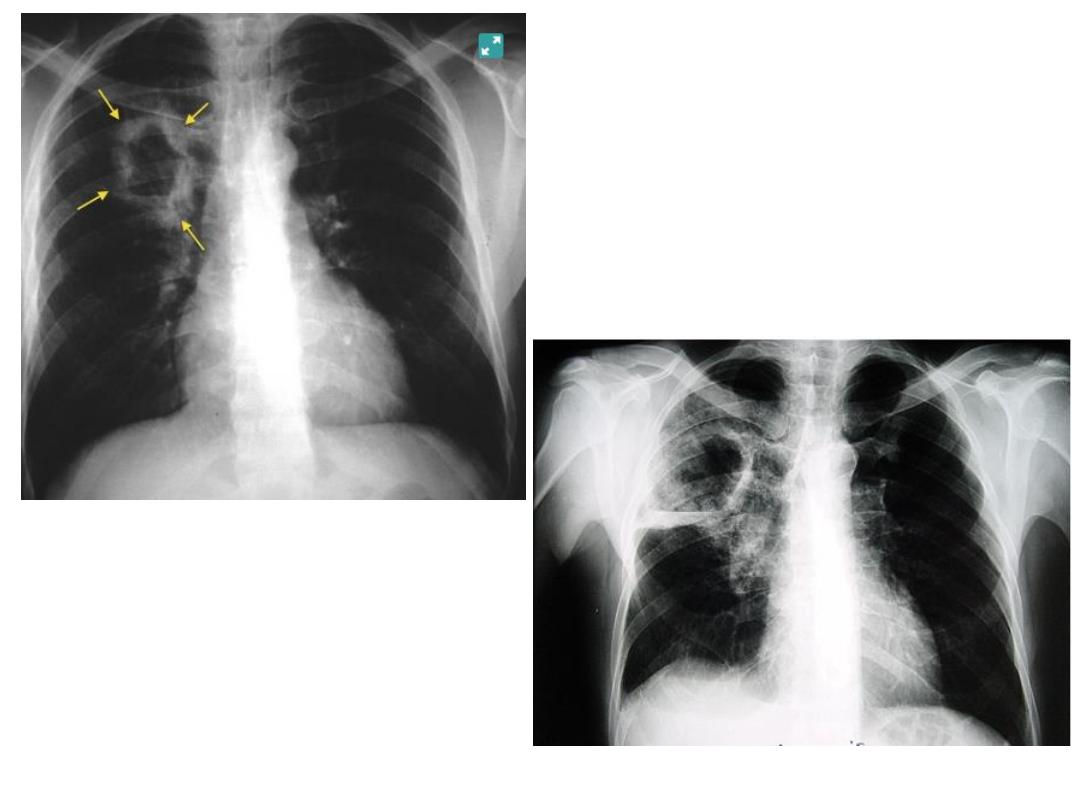
Rt. Ant. Med. Mass silhouette rt. Cardiac border
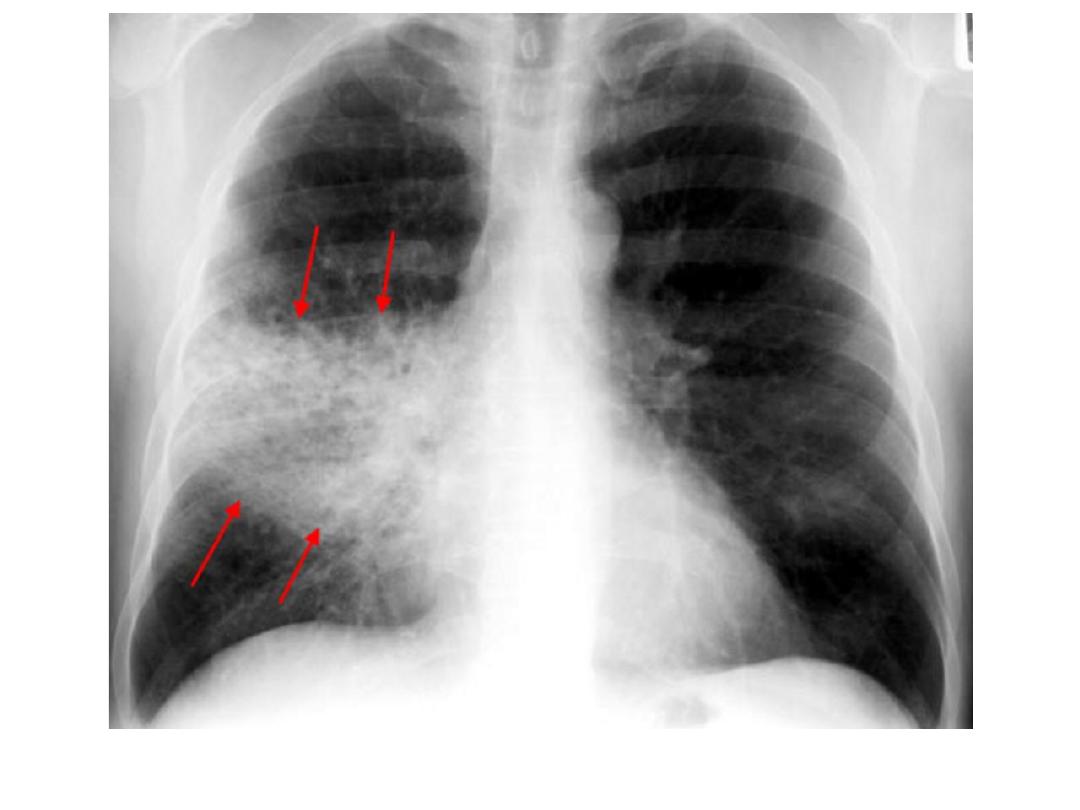
Pneumonia, with air bronchogram, partly ill defined, silhouette positive
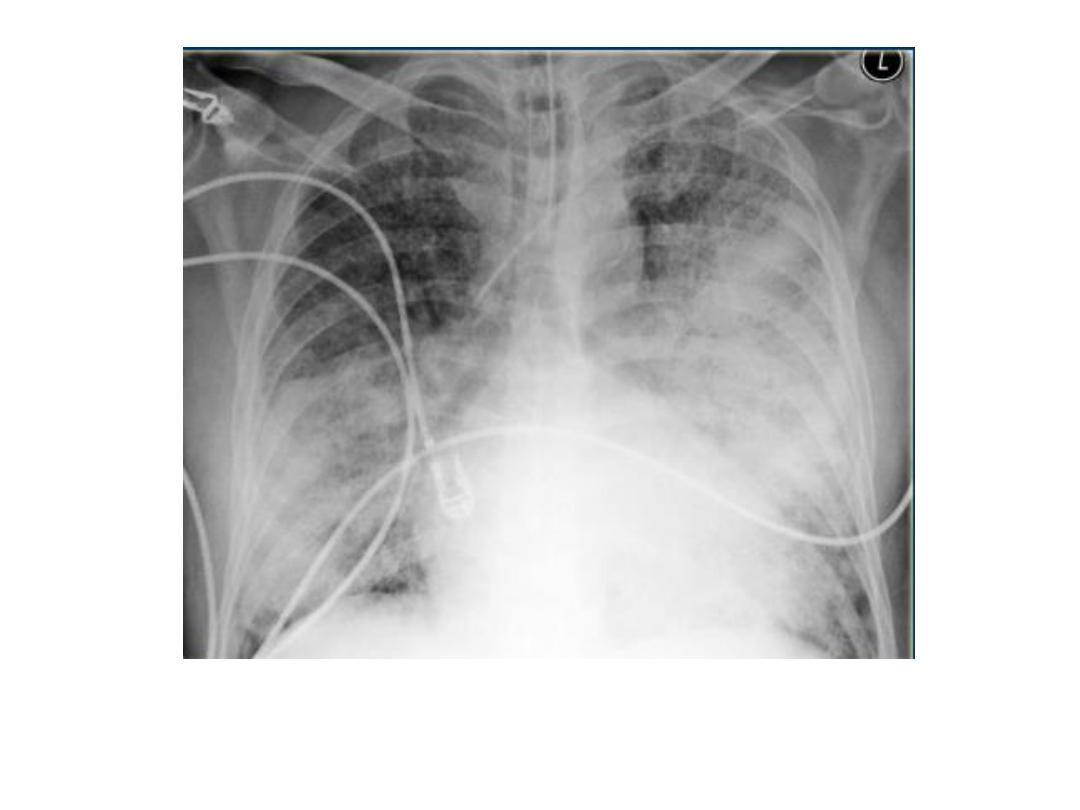
bronchopneumonia
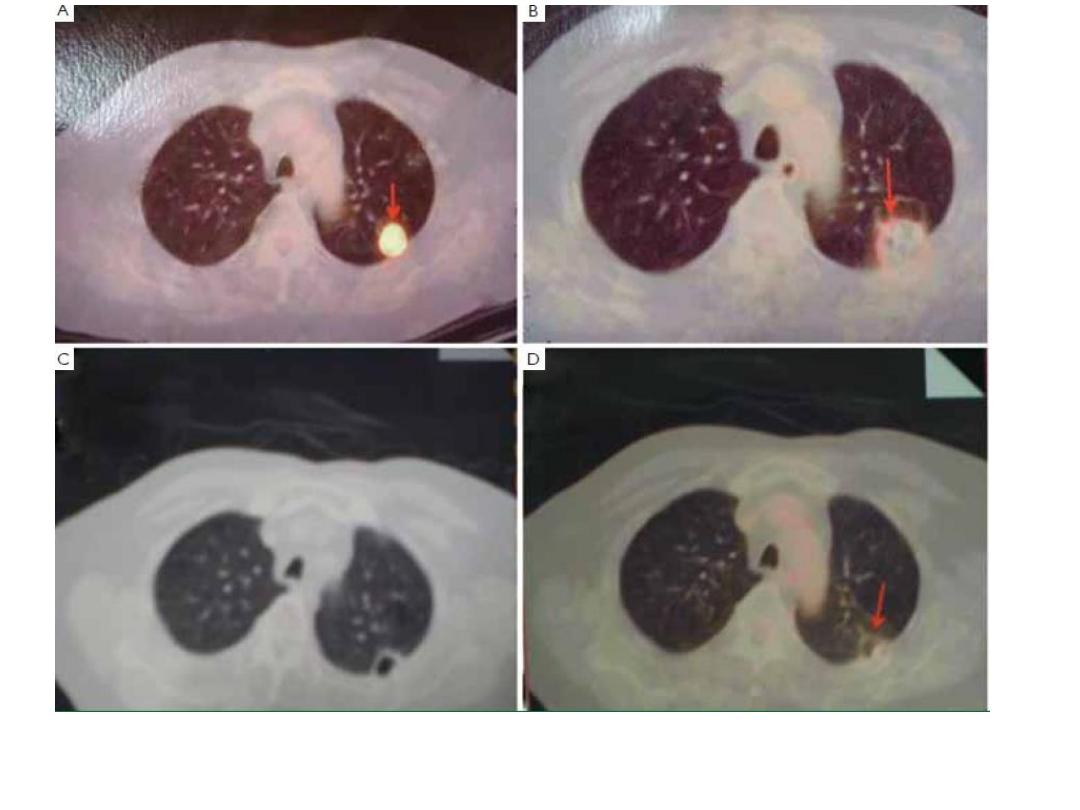
Cavity + air fluid level
CT lung cavity
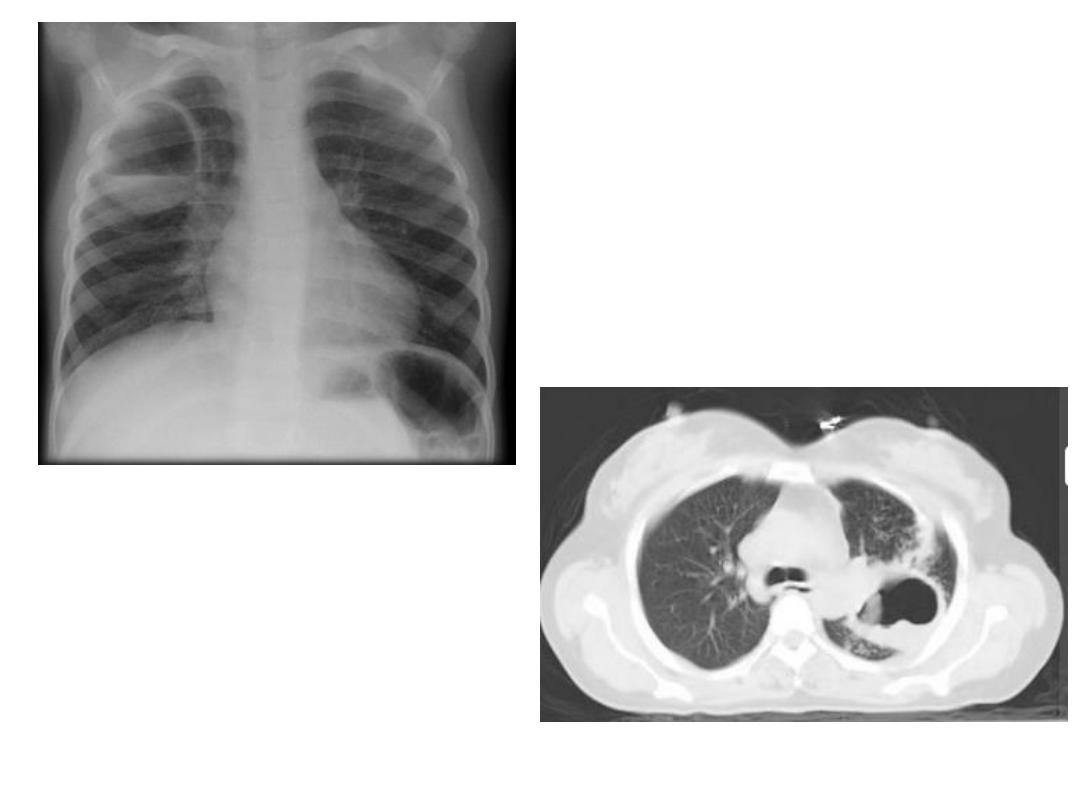
Pulmonary collapse(atelectasis): loss of volume of a lobe or lung, common causes: bronchial obst.,
pneumothorax or pl. effusion, linear(discoid) atelectasis.
Collapse caused by bronchial obst.: occurs due to air can not get into the lung in sufficient amount to
replace the air absorbed from alveoli.
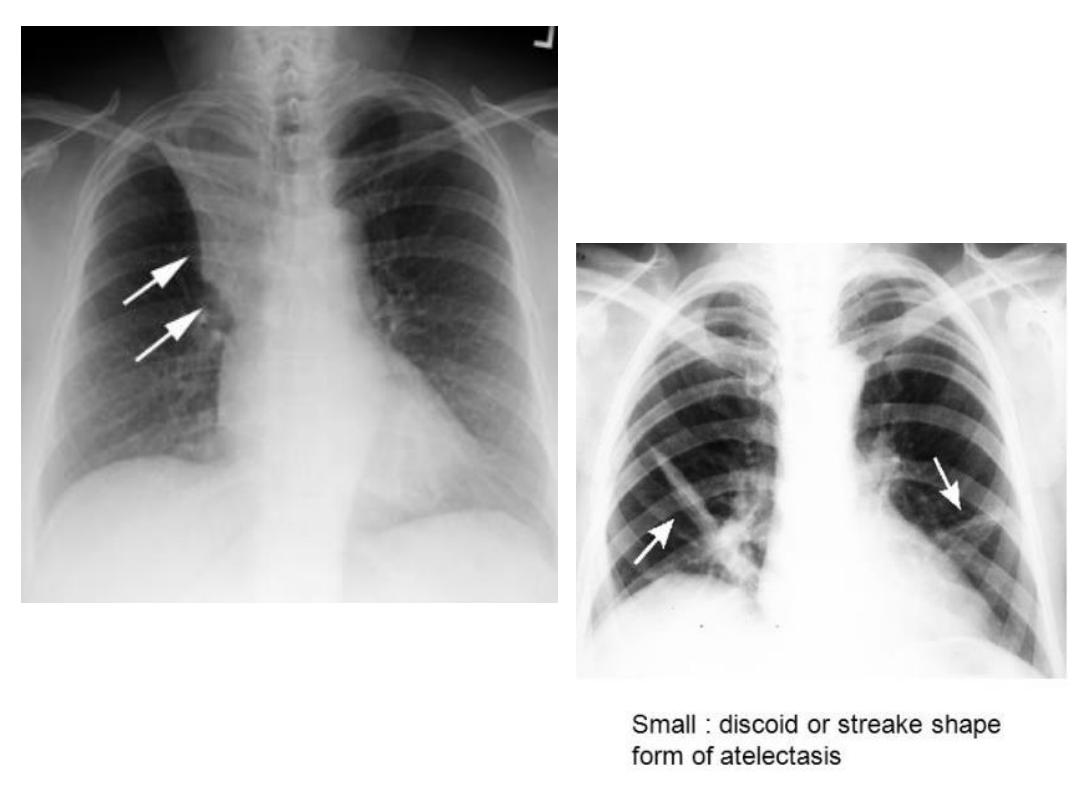
Signs of lobar collapse:
1- displacement of structures
2- shadow of collapsed lobe/ consolidation, almost invariably accompanies lobar collapse.
3- Silhouette sign: A- help to dx. Lobar collapse when resulting shadow is difficult to appreciated. B- decide
which lobe is collapsed.
Collapse of ant. Located lobes, upper and middle, obliterate portions of med. And heart outlines,
whereas collapse of lower lobes obscure diaph. And descending aorta.
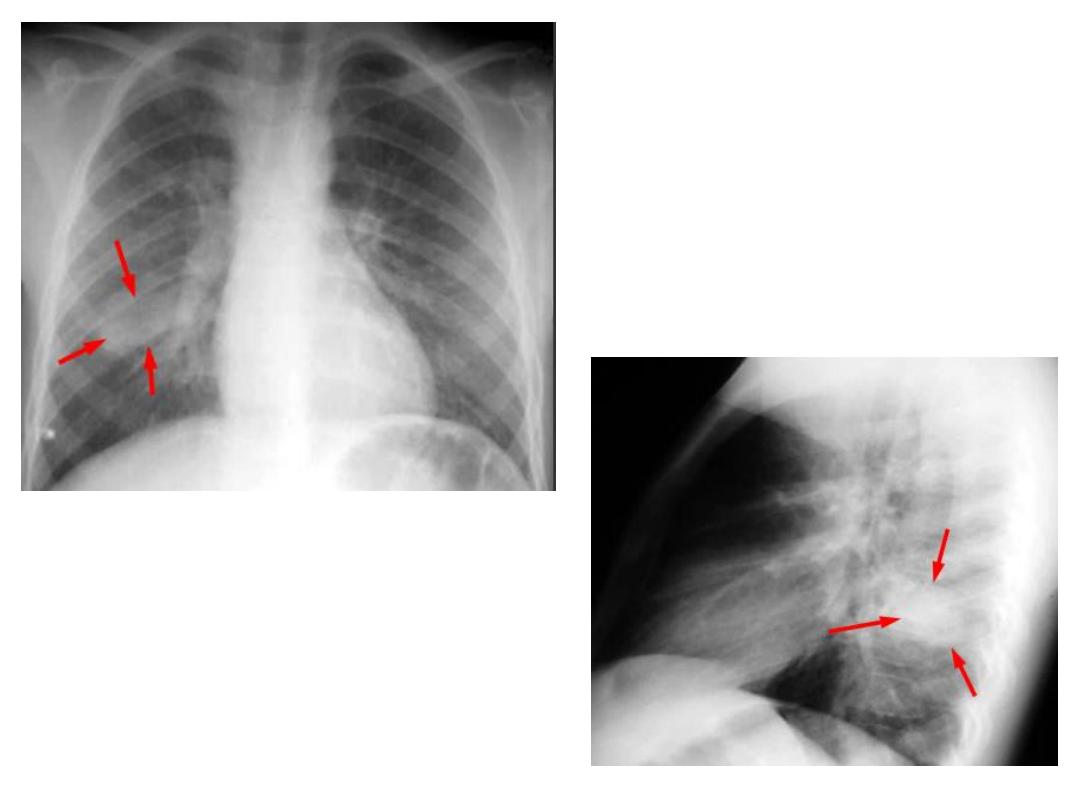
commoner causes of lobar collapse: 1- bronchial wall lesions: us. Primary CA, occasionally others as
carcinoid.
2- Intraluminal occlusion: us. FB. Or retained mucus plugs, part. Postop., asthmatic or unconscious pat.,
patient with artificial vent.
3- invasion or compression by adjacent malig. Tumors, rarely enlarged LNs.
When lobe collapse, the unobst. lobe(s) on the side of collapse undergo compensatory expansion, the
displaced fissure seen as well defined boundary to airless lobe, the med. And diaph. May move towards
collapsed lobe.
With collapse of whole one lung, the entire hemithorax is opaque, and there is substantial med. And
tracheal shift.
CT shows lobar collapse very well, but rarely necessary simply to dx. Collapsed lobe.
Collapse with pneumothorax or pl. effusion : presence of air or fluid in pl. cavity allows lung to collapse.
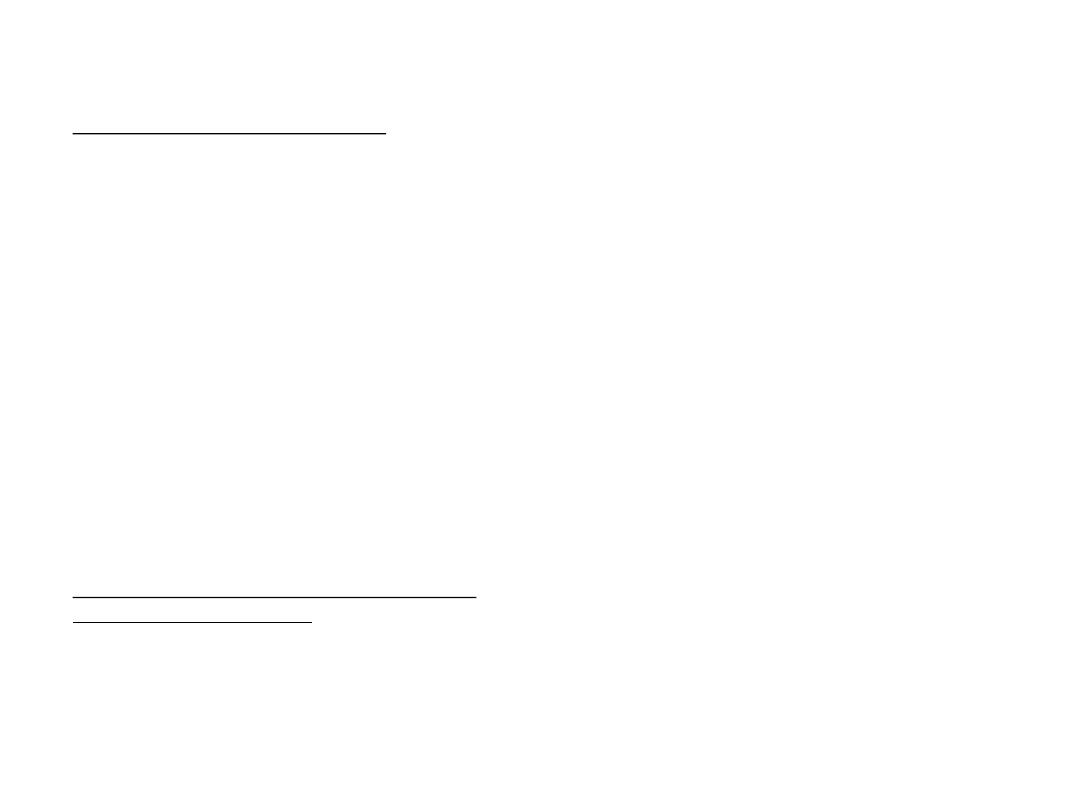
Linear(discoid)atelectasis : is not secondary to bronchial obst., but due to hypoventilation, commonest
cause is postop. Or post traumatic pain. The result is horizontally oriented band or disc of collapse
RUL collapse +Golden S sign
•
Spherical shadows(lung masses/ nodules) : the usual causes for SPN:
1- CA bronchus/ bronchial carcinoid.
2- Benign tu., hamartoma being the most common.
3- infective granuloma: TB, fungal infection.
4- metastasis.
5- lung abscess.
6- spherical(round)pneumonia, rare.
When a nodule is discovered in smoker patient, age over 50y, CA bronchus is major
consideration, but below 35y primary CA is highly unlikely.
Obv. Symptom of chest infection in patient with lung abscess.
Often no relevant symptoms even in patient with CA bronchus.
Metastasis very unlikely in patient without a known extra thoracic primary malignant tu.
Carful consideration of followings may be help in diagnosis:
1- comparison with previous films: failure to grow over a period of 18 months or more is a strong
pointer to either benign tu. Or inactive granuloma.
1-18 months usually is doubling time for CA bronchus, below 1m doubling time: infection,
infarction, lymphoma, rapid growing metastasis.
2- calcification: substantial virtually rules out malignant lesion.
Calc. is common in hamartoma, tuberculoma and fungal granulomas.
In hamartomas: often popcorn calc.
CT is of great value in detecting calc.
Benign patterns of calc. on CT: uniform calc. thought out the nodule, concentric ring calc.,
popcorn calc.

3- involvement of adjacent chest wall: destruction of adjacent ribs is virtually
diagnostic of invasion by CA.
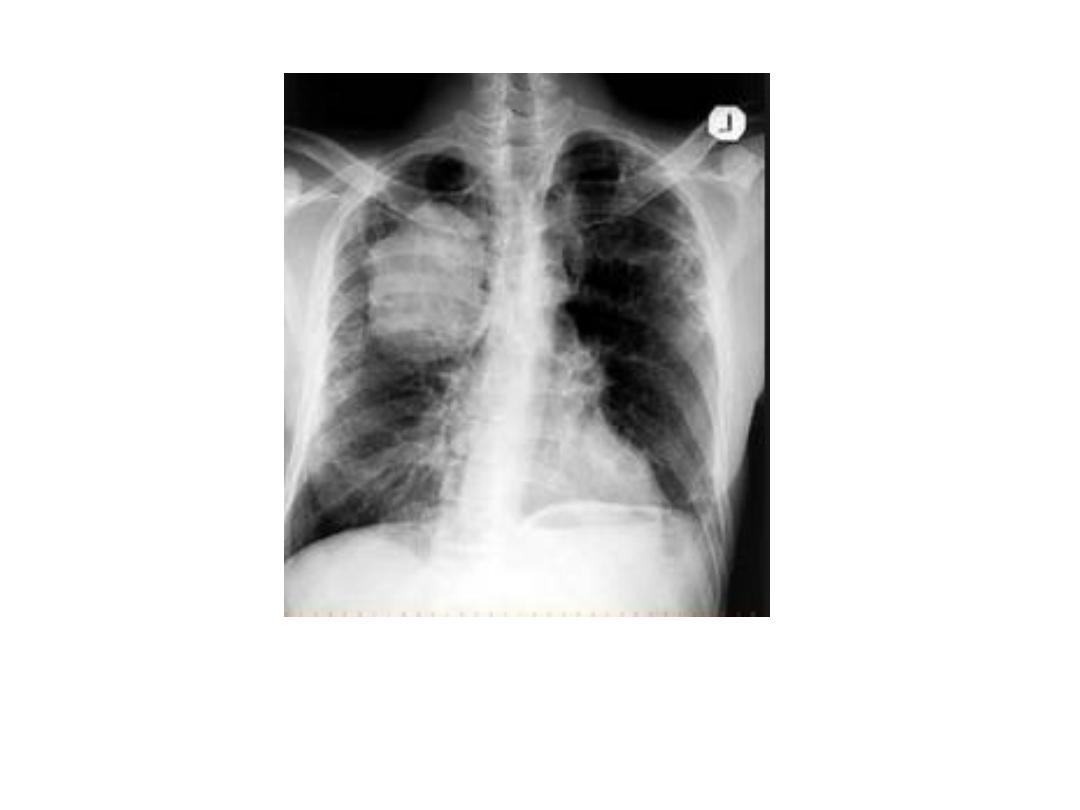
Tumors of lung apex are part. Liable to invade chest wall and adjacent bones,
Pancoast tumor.
4- shape of nodule: primary CA are nearly always rounded with lobulated, notched
or infiltrating outline.
even if only one small portion of round lesion has irregular or lobulated edge, Dx
of primary CA is seriously considered.
5- cavitation: if center of mass undergo necrosis, and cough up, air seen within the
mass.
Air fluid level may be seen on erect CXR .
These feature seen part. Well on CT scan.
Cavitation almost always indicates a significant lesion.
It is very common in lung abscess, relatively common in primary CA, occasionally
seen with metastasis, it does not occur in benign tu. Or inactive granulomas.
Cavity wall 4 mm or below usually caused by non malignant causes, 5 – 15 mm:
mixed malignant and non malignant causes, if more than 15 mm usually
malignant.
If however either inner our outer walls are irregular , DX of CA is highly likely.

6- size: a solitary pulm. Mass over 4 cm in diameter, which does not contain calc. is
nearly always primary CA, lung abscess or rarely spherical pneumonia.
Lung abscess of this size virtually always show cavitation, and spherical pn.
Causes obv. Clinical features of acute pn.
7- other lesions: the rest of the film should be checked carefully after single pulm.
Mass has been found.
Metastasis are common cause of multiple nodules.
Role of CT scan:
1- demonstrate calc. in the nodule, but CT scan not worth doing if nodule is clearly
calc. on plain films, as extensive calc……….
2- estimate rate of growth of very small asymptomatic nodules.
Follow up is better option than resection for most nodules below 1 cm, because
high probability of such small nodules being incidentally discovered benign
lesions.
3- stage the extent of disease in those cases where the nodule is likely to be primary
CA.
4- accurate localization of nodule prior to bronchoscopic or PC needle biopsy.
5- established weather or not the nodule is solitary or multiple.
Role of PET: most lung cancers conc. PET agent FDG, only small proportions
notably very small tu. And slowly growing CA do not show increase uptake.
Negative PET is useful evidence favor of benign lesions or very slowly growing tu.
Positive PET is less reliable in dx. Lung cancers in dx lung CA, because active infl.
Dis. Cause increase uptake.
Combination of a mass on CT scan with features of malignancy and positive FDG
uptake provide reasonable of CA lung.
Multiple pulmonary nodules: multiple well defined spherical shadows in the
lungs are virtually dx. Of metastasis, occasionally: lung abscesses, other neoplasm
or with granulomas caused by fungal infection, TB or collagen vs. disease
Large CA bronchus

CA bronchus
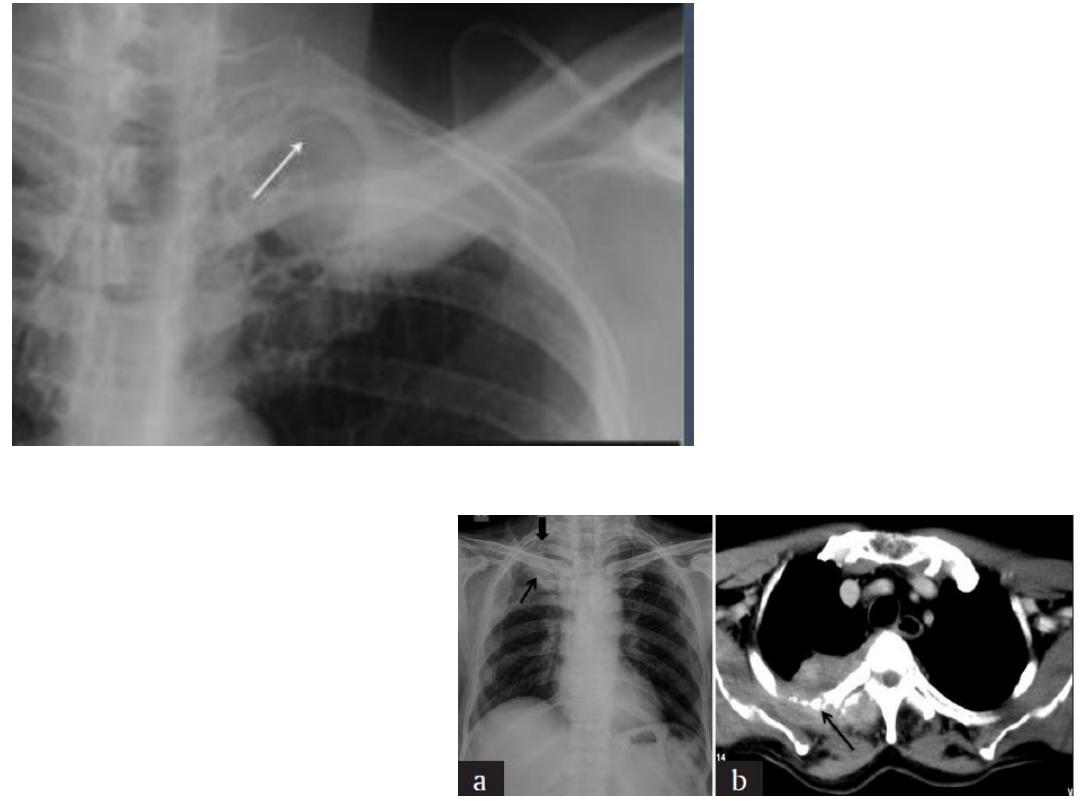
Pancoast tumor
Round pneumonia
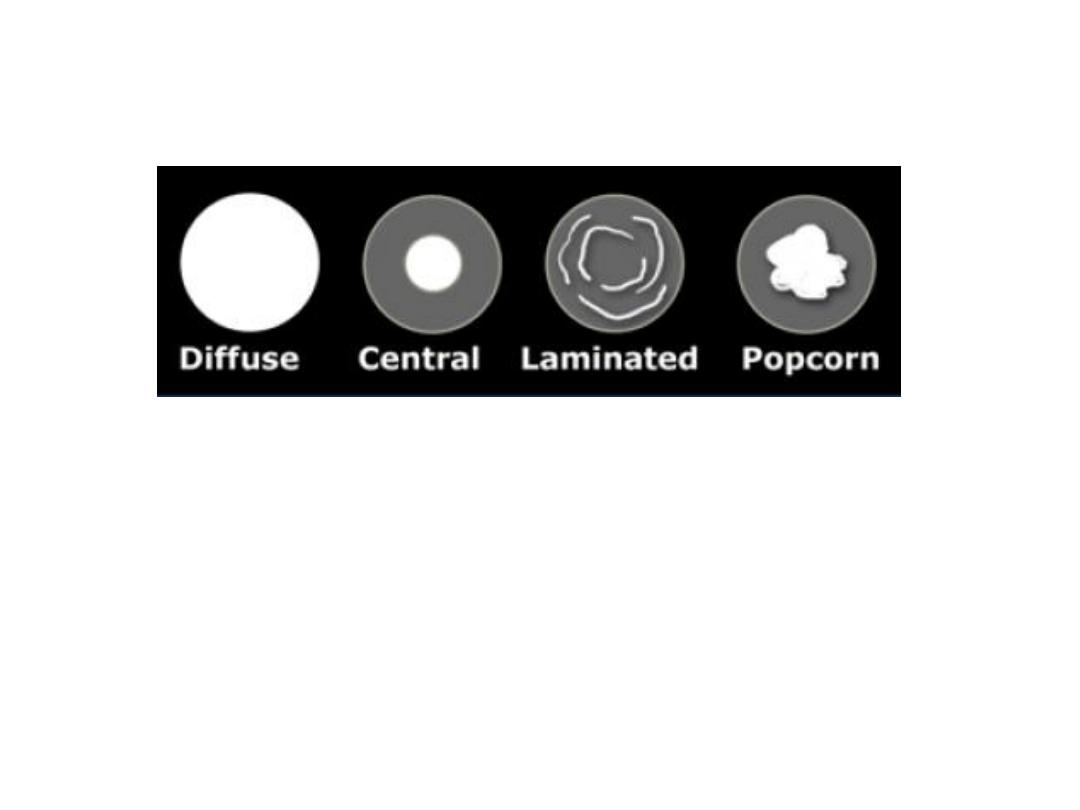
Benign calcification
carcinoid
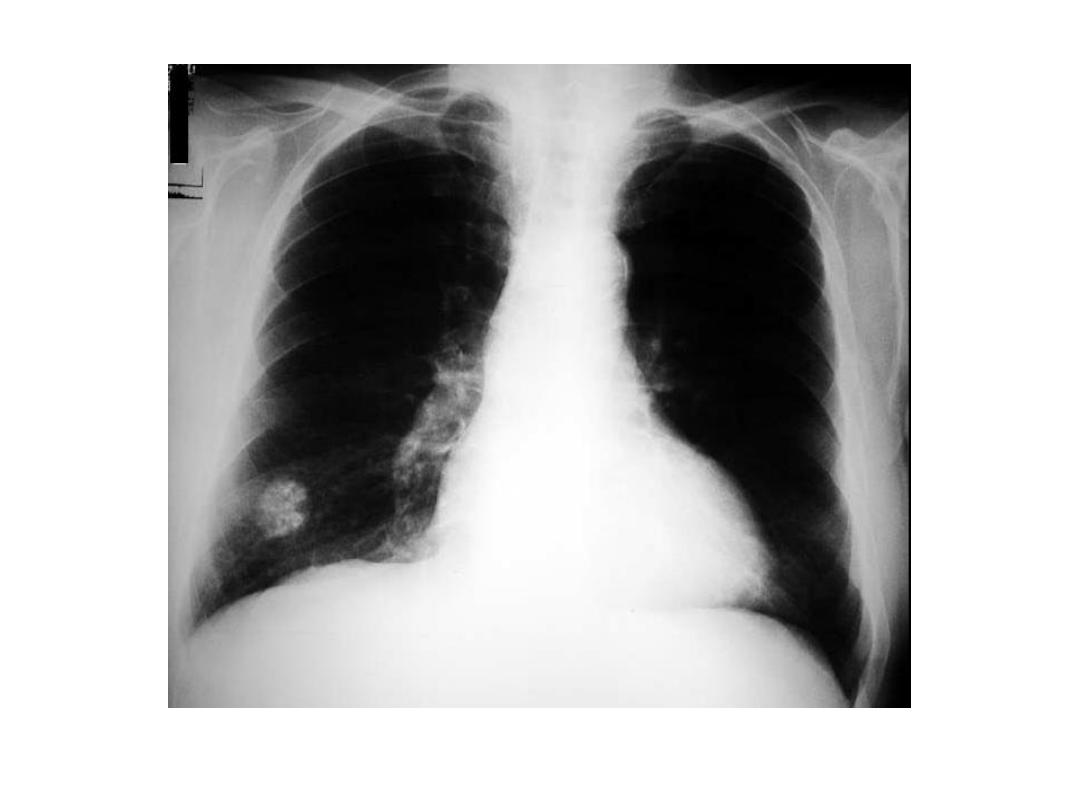
Hamartoma
Cavitary CA bronchus
Lung abscess
PET CT scan CA bronchus pre and post cryoembolisation , lower images after 5y