1
ACUTE ST ELEVATION MYOCARDIAL INFARCTION(STEMI)
By The End of This Lecture You Should Be Able To
Differentiate ACS from other acute chest pain emergency conditionsDiagnose STEMI using clinical, ECG, and biochemical tools
Recognize the various steps of management of the patients before and after reaching hospital
2
Objectives
Appreciate the vital importance of time in the proper management of STEMIAppreciate that STEMI is caused by complete obstruction of a coronary artery by thrombus
Understand that thrombus removal is the cornerstone of management
When the ECG shows ST elevation, attempts at reperfusion should take priority over further investigations
Clinical Scenario 1
A 60-year-old man with Hx of diabetes, hypertension, and smoking is brought to the emergency room by his family because of severe chest pain
What Conditions Cause Acute chest pain?
ACS (STEMI, NSTEMI)Aortic dissection
Acute pericarditis
Pulmonary embolism and infarction
Pneumothorax
Extracardiac causes: esophageal spasm, visceral obstruction or perforation, musculo-skeletal chest pain
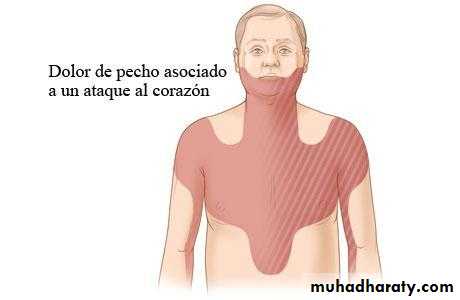
Clinical Presentation of ACS, including STEMI
Pain:Chest, back, shoulder, epigastrium, neck, throat, mandible, arms, hands
Prolonged
Severe
Not relieved!
7
ACS (STEMI): Clinical features
Other features
Severe anxiety
Nausea and vomiting
Breathlessness
Collapse
Syncope

8
STEMI: PHYSICAL SIGNS
Signs of sympathetic activation:
Pallor
Sweating
Tachycardia
Signs of vagal activation
Vomiting
Bradycardia
9
STEMI: PHYSICAL SIGNS
Signs of impaired myocardial function
Hypotension, oliguria, cold sweat
Narrow pulse pressure
Raised JVP
S3
Faint S1
Diffuse apical impulse
Lung crepitations
10
STEMI: DIFFERENTIAL Dx
Aortic dissection:
Pain is abrupt & severe from the onset, tearing in nature, more in the back
Pulmonary embolism
Dyspnea, tachypnea, tachycardia, hypotension
Acute pericarditis:
Important to differentiate, as thrombolytic therapy may cause cardiac tamponade
Pain is sharp, related to breathing , posture and swallowing
Pericardial friction rub
STEMI: Diagnosis & Basic Investigations
Clinical presentationECG
Troponin (indicating myocardial cell injury)
Enzymes indicating myocardial cell necrosis: CPK, AST, LDH
STEMI Diagnosis, additional investigations
EchocardiographyCXR
Blood tests: WBC, ESR
Tetrad of Diagnosis
Chest painClassical ECG showing ST elevation
Raised troponin
Raised markers of myocardial cell necrosis

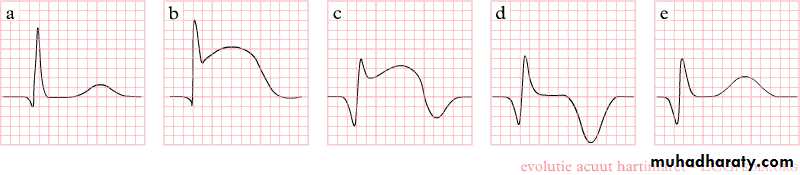
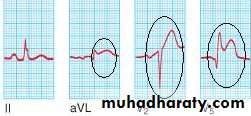
The ECG in STEMI
• Sequence of changes in STEMI:• Tented, peaked T waves
• Acute ST elevation (the current of injury)
• Loss of amplitude of the R wave
• Development of a Q wave
• T wave inversion
• Reduction in the magnitude of the ST elevation (ST resolution)
• Deepening of Q waves
The ECG in STEMI
Hyperacute T waves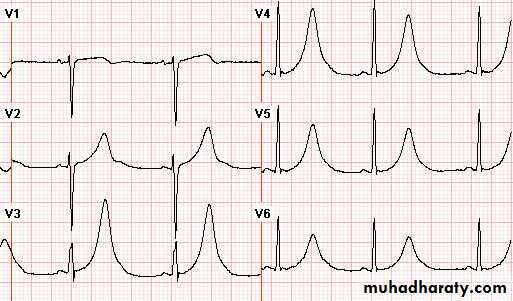
16
STEMI: ECG
ST segment elevation: the earliest ECG change
STEMI
normal angina


17
STEMI: ECG
Next: reduction of R wave amplitude, appearance of Q waves, T inversion




18
STEMI: ECG
Then: deepening of Q waves, T inversion & resolution of ST segment
19
STEMI: ECG
12 weeks after MI, the ST segment returns completely to normal
20
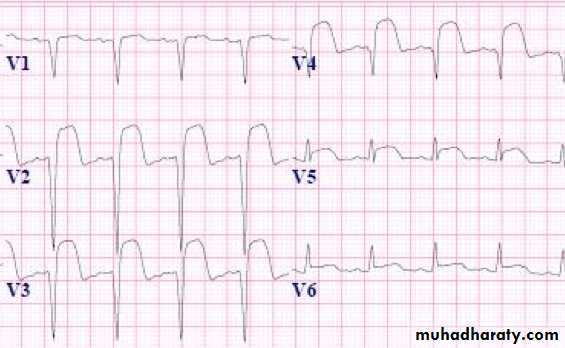
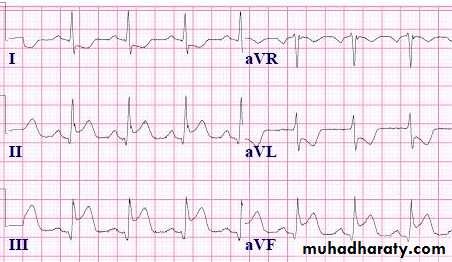
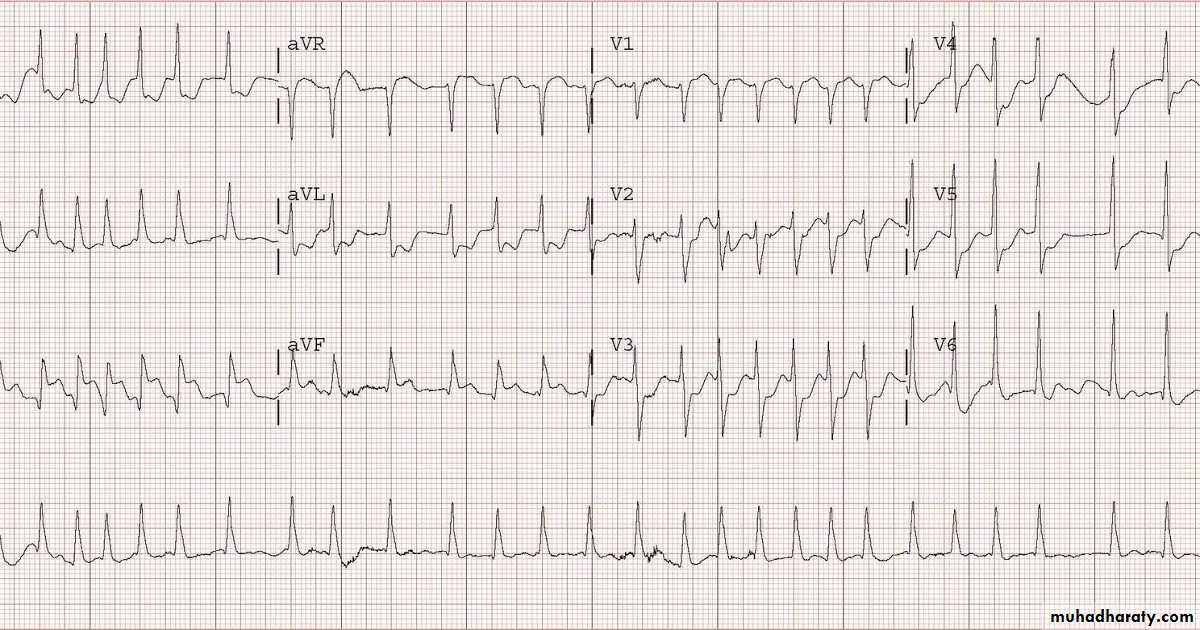
Acute Anterior MI
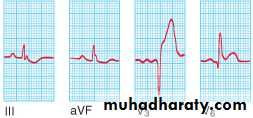
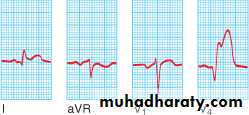

21
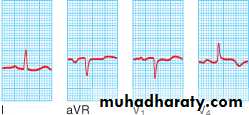
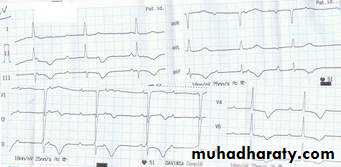
Acute inferior MI


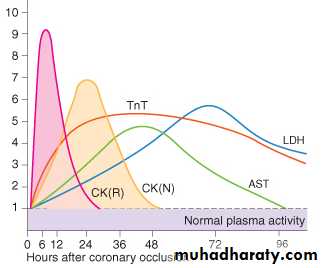
STEMI Diagnosis: Biochemical markers
26Biochemical markers
Troponin T (Tn T)
Troponin I (Tn I)
Creatinine Kinase (CK)
Creatinine kinase MB (CK-MB)
Others: AST, LDH
27
Biochemical Markers
28
Biochemical Markers: Troponins
cTn-T & cTn-I:
More specific than CK & CK-MB
Start to rise in 4-6 hours
Persist in the circulation for 2 weeks
Troponins are elevated in unstable angina but to less severe degree.
29
Biochemical Markers
CK (creatinine kinase):
Found in skeletal muscles (MM isoenzyme), in the brain (BB isoenzyme) and in the myocardium (MB isozyme)
Starts to rise at 4-6 hours,
peaks at 12 hrs, and
disappears in 36-48 hrs
30
Biochemical Markers
CK is not specific for cardiac muscle, it may rise in
Intramuscular injection
Physical exercise
Defibrillation
CK-MB is more specific and sensitive for cardiac muscle injury
31
Biochemical Markers
CK-MB is not elevated with the administration of DC shock or skeletal muscle injury.
Further Testing?
If the ECG shows ST elevation, time should be reserved for immediate management!Other investigations should be done after reperfusion therapy
33
Other Blood Tests
Leukocytosis:
Neutrophilia
Reaches a peak on the first day
Correlates with the extent of myocardial damage, i.e. with prognosis
Erythrocyte Sedimentation Rate (ESR)
C-Reactive Protein (CRP)
34
Chest X-Ray
Pulmonary edema
Heart size:
Usually normal
Cardiomegaly due to old myocardial infarctions
35
Echocardiography
Usually done after reperfusion therapy
Can be performed at the bedside
Useful to assess the status of the LV & RV
Detects mechanical complications
LV mural thrombus
Ventricular septal rutpture
Mitral regurgitation
Pericardial effusion
RV infarction
Clinical Scenario 2
A 70-year-old man suffers severe chest pain with sweating and severe weakness while at rest.

This patient Probably Sustained ACS (Infarction, Heart Attack)

Immediate (Prehospital) management
DO NOT PANIC!Call for help, ambulance
Transfer to a safe place, remove tight clothes, administer sublingual angised if available…..

Immediate (Prehospital) management
Observe pulse, BP (if possible) and level of consciousnessTransfer to hospital as soon as possible

What is the immediate danger to the patient?

What is the imminent danger to this patient?
Acute cardiovascular collapse & death, caused byArrhythmia (VF)
Cardiac standstill
Patient becomes pulseless and unconscious

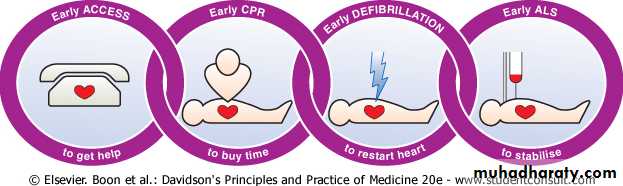
Immediate (Prehospital) management: CPR
In case patient becomes pulseless and unresponsive: administer CPR (cardio-pulmonary rescuscitation)



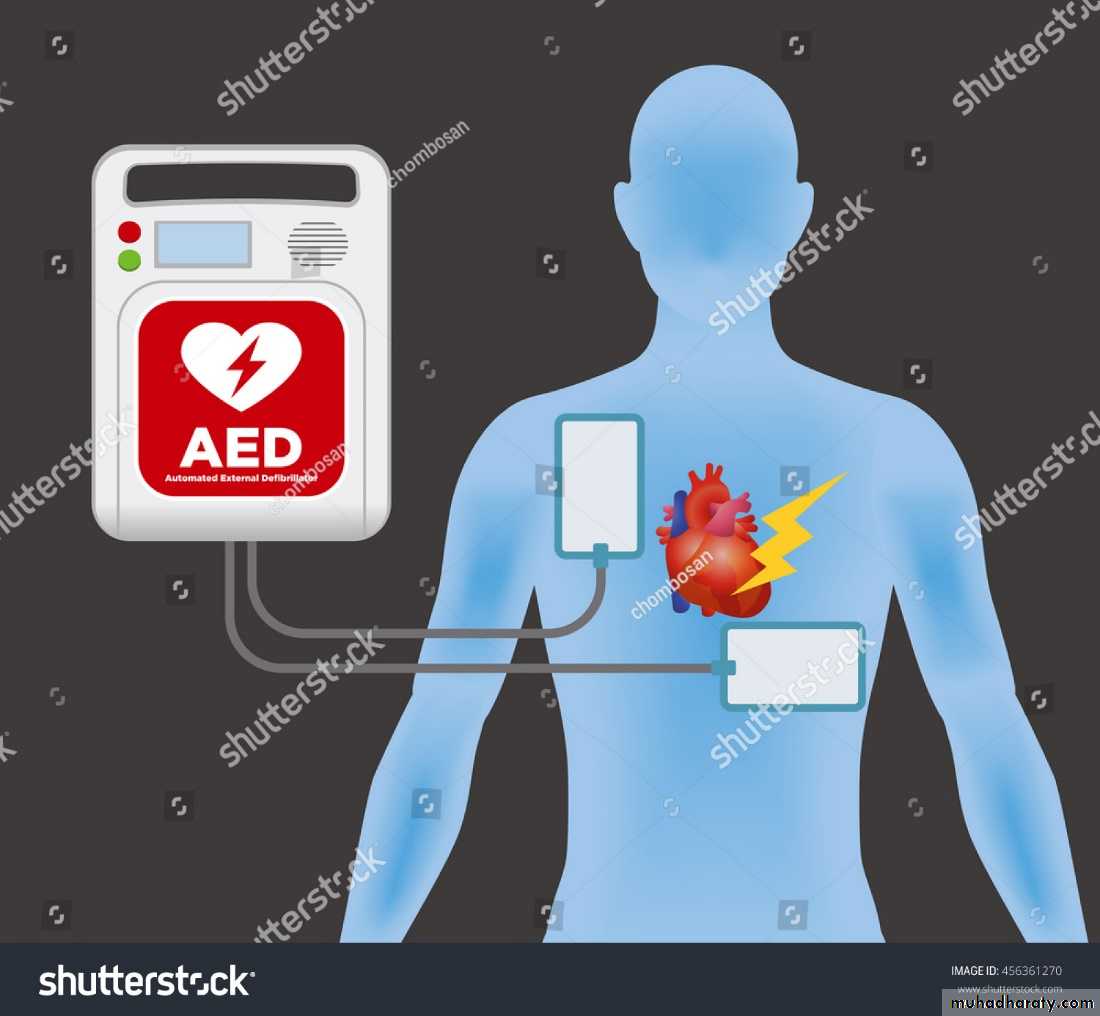
Immediate (Prehospital) management
AED: automatic external Defibrillator: If available, give DC shock, continue CPR until restoration of pulse, repeat DC if necessary
46
Prehospital management
Advanced Life Support (ALS)
47
Transferring The Patient
Rapid transfer of the patient to hospital: ambulance


Ambulance should be well equipped:
DefibrillatorsAnalgesia
Oxygen
Monitors
ECG machines
Thrombolytic therapy?

49
Early managemnt: immediate measures
Cannula
Oxygen
ECG monitoring
Standard (12-lead) ECG
Analgesia: morphine sulphate
50
REPERFUSION THERAPY
51
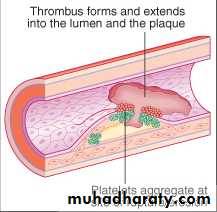
STEMI
Myocardial necrosis caused by thrombotic occlusion of a coronary artery
Occlusive thrombus is formed at site of rupture of atherosclerotic plaque
Reperfusion
Once diagnosis is established, reperfusion should be attemptedShould be done as soon as possible
The situation is an emergency: minutes mean muscle
THE KEY TO PROPER MANAGEMENT OF ACUTE MYOCARDIAL INFARCTION IS THE TIMELY AND IMMEDIATE REMOVAL OF THROMBUS OBSTRUTION AND RESTORATION OF BLOOD FLOW TO THE INFARCTED SEGMENT. THIS IS EXPECTED TO PREVENT LOSS OF MYOCARDIUM, IMPROVE LV FUNCTION, IMPROVE QUALITY OF LIFE, AND PROLONG SURVIVAL.
53
54
Reperfusion
Restoration of coronary patency
Resolution of acute ST elevation
Reduces myocardial infarct size
Relieves pain
Preserves LV function
Improves survival
55
Reperfusion
May reduce arrhythmias, but may exacerbate these arrhythmias (reperfusion injury)
Should be administered as soon as possible to achieve maximal salvage of myocardium (minutes mean muscle)
Methods of Reperfusion
Pharmacological (thrombolytic therapy)

Mechanical (primary PCI)
Mechanical (primary PCI)
58
Reperfusion: Thrombolytic therapy
Thrombolytic agents:
Streptokinase
Alteplase (tPA)
Tenecteplase (TNK)
Reteplase (rPA)
59
Reperfusion: Thrombolytic therapy
Thrombolysis is of no benefit (and may be harmful):
If given > 12 hours from the onset of STEMI
(preferably given within the first 6 hours)
In cases of NSTEMI or unstable angina
60
Thrombolytic Complications
Bleeding:
Cerebral hemorrhage :
It may be wise to withhold treatment if there is significant risk of bleeding
With streptokinase:
the development of antibodies to the drug that render future administration of the drug ineffective
hypotension
61
Thrombolysis: Contraindications
Absolute contraindications:
Known bleeding tendency
Active bleeding (except menstruation)
History of cerebrovascular occlusion within the previous year
History of intracranial hemorrhage
Cerebral or spinal tumor
63
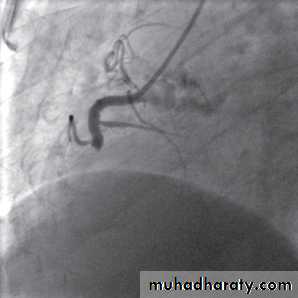
Reperfusion therapy: primary PCI
Associated with better results than thrombolytic therapy
Requires specialized experience and expensive equipment
Should be performed as soon as possible (minutes mean muscles)
Indicated in cases of failure of thrombolytic therapy or when such therapy is contraindicated.
64
Objectives
Be familiar with the management of the patient with established myocardial infarction
Understand STEMI complications in the CCU: Mechanical and electrical
Appreciate the long-term management of patients with STEMI
Clinical Scenario 3:
A 63-year-old diabetic woman sustained an anterior wall STEMI.Was transferred in time to hospital
Received thrombolytic therapy with t-PA with resolution of ST changes and disappearance of chest pain
Was transferred to the CCU
Echo showed mild hypokinesia of the anterior wall with good systolic function
What is the next step in management?
67
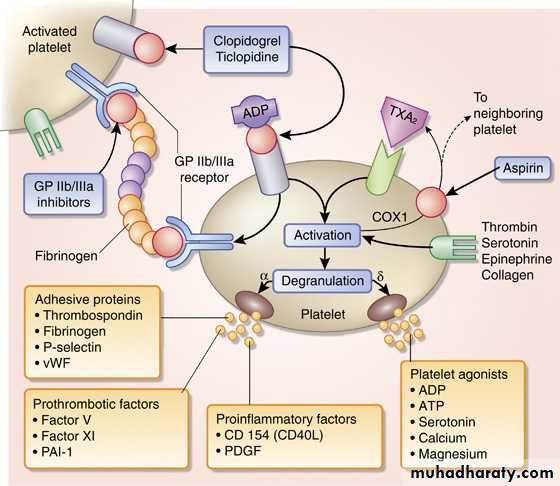
Maintaining Vessel Patency
Aspirin
Clopidogrel
Anticoagulants
68
Maintaining Vessel Patency: ASA
Oral ASA (75-350 mg/day)
Reduces mortality
Should be continued for life
Combination with clopidogrel: improves outcome
69
70
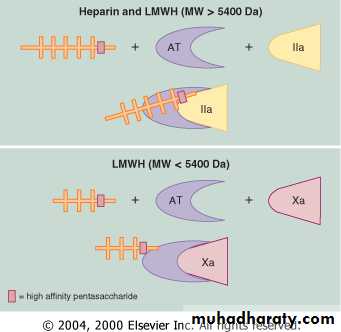
Maintaining Patency: Anticoagulants
Heparin:
Unfractionated heaprin and LMWH
Improve survival of patients with STEMI
Slight increase in the risk of intracranial bleeding
Not given after successful primary PCI
71
Antithrombotic therapy
72
Oral Antithrombotic therapy?
Warfarin
Direct acting oral anti-coagulants:
Direct thrombin inhibitors: dabigatran
Factor Xa inhibitors: apixaban, rivaroxaban
Indications:
Atrial fibrillation
Extensive anterior wall MI with LV dysfunction
The demonstration of mobile thrombus on echocardiography
73
Management of STEMI
Early management
Maintaining vessel patency
Adjunctive therapy
74
Adjunctive Therapy
β-blockers
Nitrates (?)
ACE inhibitors
Lipid-lowering agents (statins)
75
Adjunctive Therapy: β-blockers
During the acute presentation:
i.v. administration
Atenolol or metoprolol
Reduce pain
Reduce arrhythmia
Improve short term survival
Contraindicated:
Congestive heart failure
Heart block
bradycardia
76
Adjunctive Therapy: β-blockers
• Long term use of β-blockers :
Should be given to ALL patients unless contraindicated
Improve long term survival
Adjunctive Therapy: ACE inhibitors, Statins
Essential for the secondary prevention of atherosclerosisACE inhibitors are also useful to maintain LV function
When side-effects develop to ACE inhibitors, ARBs should be used
Complications of STEMI: Clinical Scenario 4
A 55-year-old hypertensive and smoker sustains an extensive anterior infarction. He is only transferred to hospital 24 hours after the attack. The ECG shows established anterior wall MI, with deep Q waves, ST elevation, and T inversion in the anterior leads. No thrombolytic therapy was administeredWhat are the expected complications?
79
COMPLICATIONS OF STEMI
Short-term complications
Arrhythmias
Mechanical complications
Residual ischemia
Pericarditis
embolism
Long term complications
Recurrnet ischemia
LVdysfunction
80
complications
Arrhythmias
Mechanical complications
Acute circulatory failure
Residual ischemia
Pericarditis
embolism
81
complications
tachy arrhythmias
ventricular
Arrhythmias atrial
brady arrhythmias
82
Tachyarrhythmias
Ventricular:
Premature ventricular ectopics (PVCs)
Accelerated idioventricular rhythm
Ventricular tachycardia
Ventricular fibrillation
Atrial
Atrial fibrillation
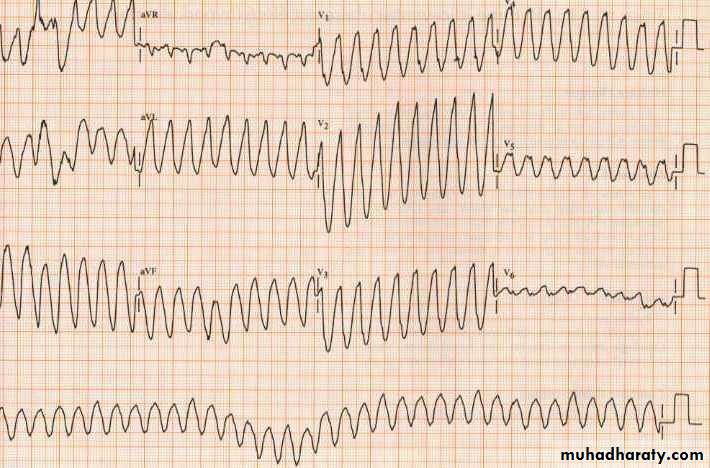
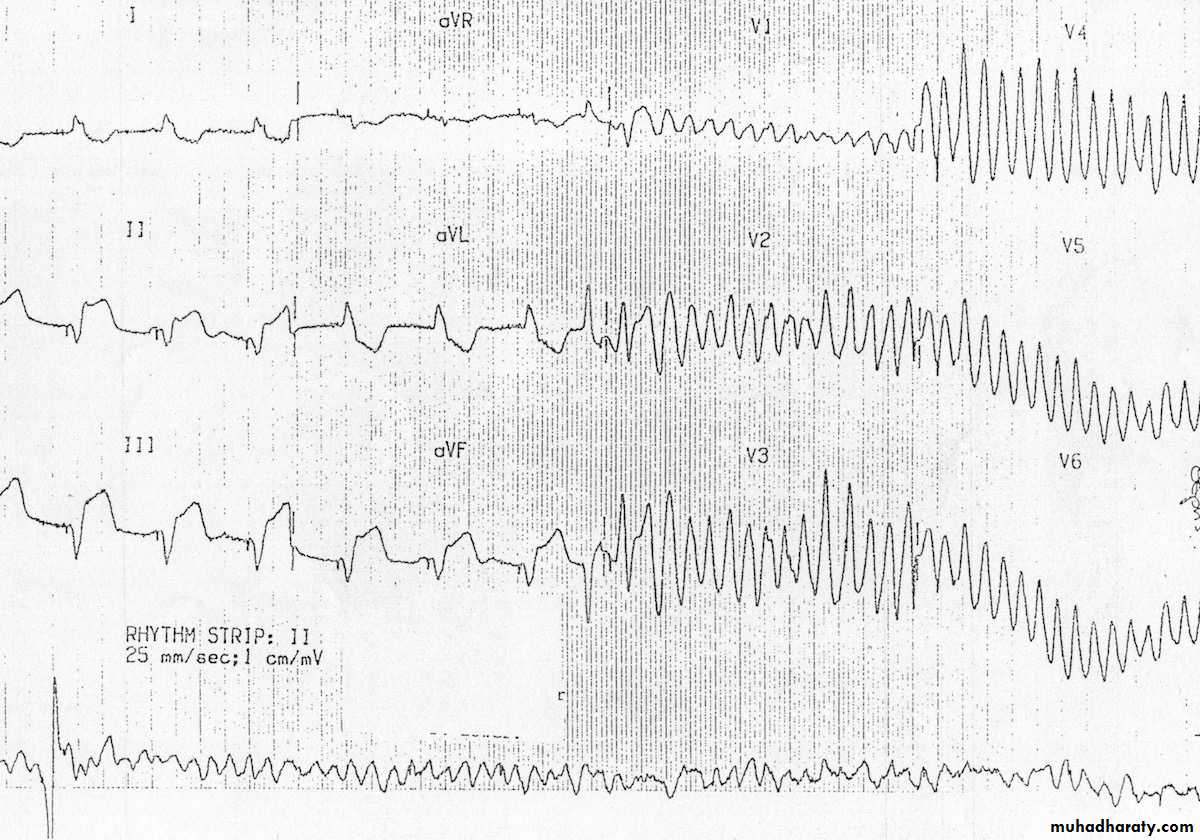
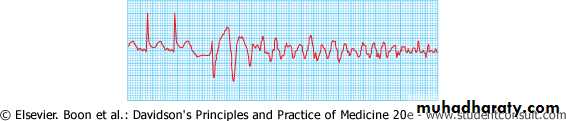
Tachyarrhythmias
The patient collapsed in the CCU!What is the diagnosis
What’s the urgent treatment?
What drug is given to prevent recurrence?
Tachyarrhythmias
Ventricular fibrillation:The major cause of death in patients with STEMI before reaching hospital
Occurs in 5-10% of patients who reach hospital
Lethal arrhythmia unless treated by prompt defibrillation
Does not affect the long term prognosis of acute MI.

84
Tachyarrhythmias
Atrial fibrillation:Common in acute MI
Frequently transient
May be serious if it occurs in the context of LV failure
85
87
Atrial Fibrillation: Treatment
May be transient and needs no treatment
Indications to treat:
Rapid ventricular rate
Hemodynamic deterioration (hypotension, CHF, pulmonary edema)
Emergency treatment:
Synchronized DC shock
Non-emergency situation:
Infusion of β-blocker or amiodarone
Bradyarrhythmia: AV block
In the setting of inferior MI:Usually temporary
Resolves with thrombolytic therapy
May need atropine if persists
If there is hemodynamic deterioration:
temporary pacemaker insertion
88
89
Bradyarrhythmia: AV block
In the setting of anterior wall MI:
More serious than in inferior MI
May be complicated by sudden asystole
Prophylactic temporary pacemaker should be inserted
90
complications
Arrhythmias
Mechanical complications
Acute circulatory failure
Residual ischemia
Pericarditis
embolism
91
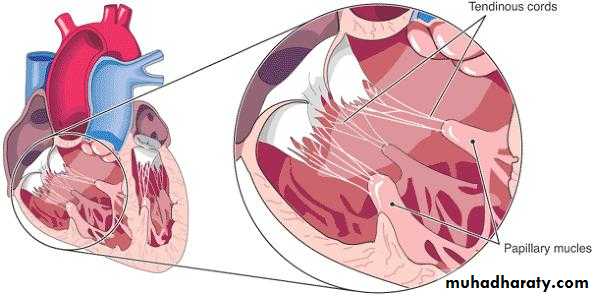
Mechanical complications
Papillary muscle rupture
Interventricular septal rupture
Ventricular free wall ruputre
Papillary Muscle Rupture
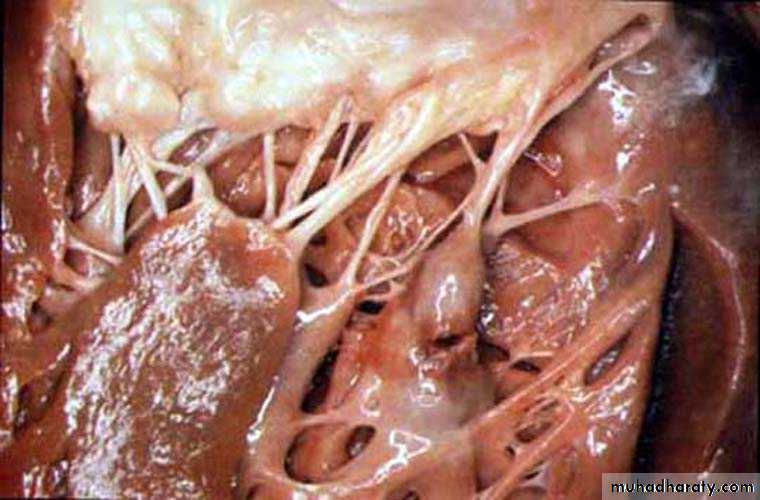
93
Papillary muscle rupture
Sudden severe mitral regurgitation (MR)
Presents with pulmonary edema & shock
O/E: pansystolic murmur at the apical area radiating to the axilla or back. S3 & S4
The murmur is frequently faint or even absent
Dx: echo and Doppler
Treatment: urgent surgery
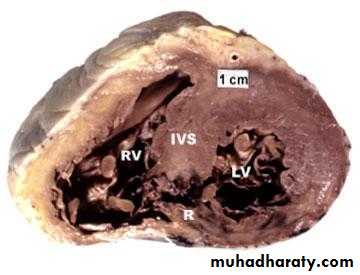
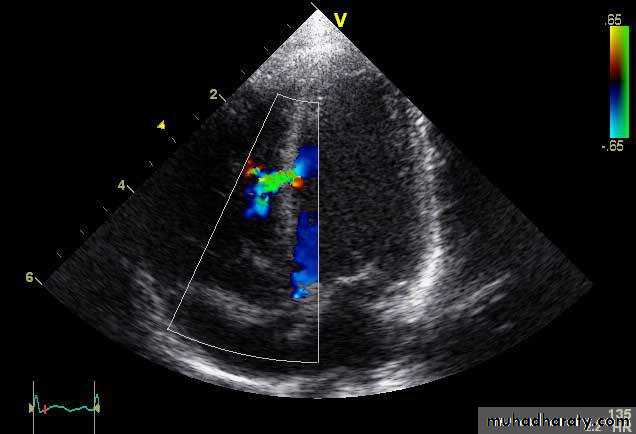
Ventricular Septal Rupture
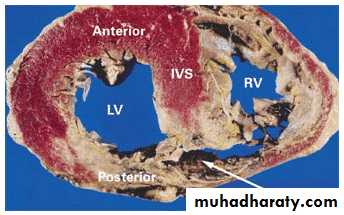
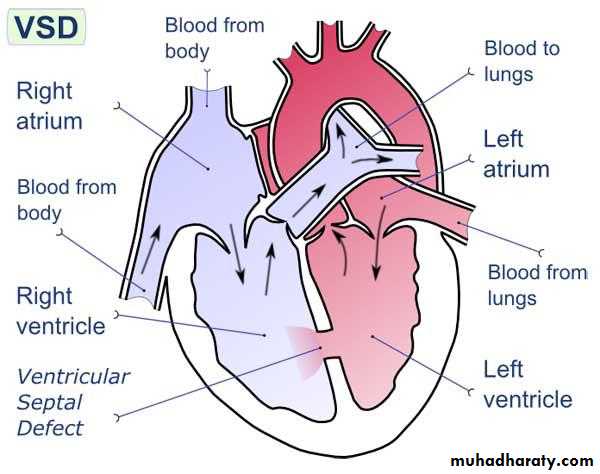
Ventricular Septal rupture
Sudden deterioration: hypotension, right ventricular failure, shockClinically: pansystolic murmur at the left sternal border
Diagnosis: echo and Doppler
Treatment: surgery
95
96
complications
Arrhythmias
Mechanical complications
Acute circulatory failure
Residual ischemia
Pericarditis
Embolism
97
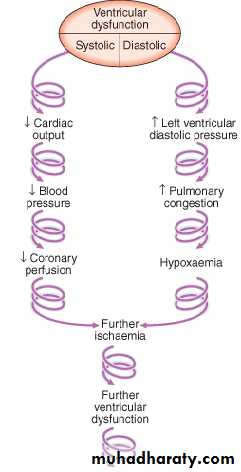
Acute circulatory failure(Cardiogenic Shock)
Indicates extensive myocardial damage
Usually fatal without intervention
Mortality of 90% if untreated
With primary PCI: can be reduced to 25%
98
99
Management of cardiogenic shock
Calculating cardiac output & systemic vascular resistance (Swan-Ganz catheter)
The use of inotropic drugs, diuretics, &/or vasodilators according to the calculations
Circulatory assistance with intra-aortic balloon pump
Primary PCI
100
complications
Arrhythmias
Mechanical complications
Acute circulatory failure
Residual ischemia
Pericarditis
Embolism
101
Residual Ischemia
Presents as post infarction angina
Causes of residual ischemia:
Significant stenosis of an artery after successful thrombolysis
Blockage of an artery that was responsible for the collateral supply of another coronary artery
Occurs in ~ 50% of patients with AMI
102
Residual Ischemia: Management
High risk group of unstable angina
i.v. nitrates, β-blockers, Oxygen (if necessary)
Aspirin
Clopidogrel
Anticoagulation
Invasive strategy (PCI or CABG)
103
complications
Arrhythmias
Mechanical complications
Acute circulatory failure
Residual ischemia
Pericarditis
embolism
Pericarditis Following STEMI
Acute pericarditisPost MI syndrome (Dressler’s Syndrome)
105
Acute Pericarditis
Usually occurs in the 2nd & 3rd days
Chest pain of different quality than ischemic:
Sharp
Localized
Positional
Related to breathing: worse on inspiration
Pericardial friction rub
ECG changes of acute pericarditis
106
Acute Pericarditis: Management
The use of steroids or NSAID is contraindicated in AMI:
Weakening of scar
Increase the risk of aneurysm formation
Aspirin in high dose
colchicine
Opiate-based analgesia
107
Post-MI-Pericarditis(Dressler’s syndrome)
Auto-immune reaction
May occur 6 days-6 months after MI
Pain (pleuro-pericarditis)
Pyrexia
Pericarditis
Pleurisy
Treatment: High dose ASA, NSAID, colchicine, or even steroids
108
Complications: Ventricular Remodelling
Infarct expansion: thinning
& stretching of the
infarcted segment
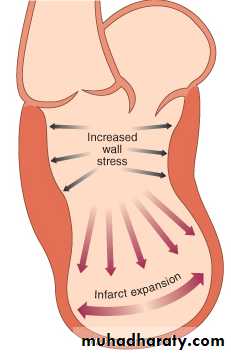
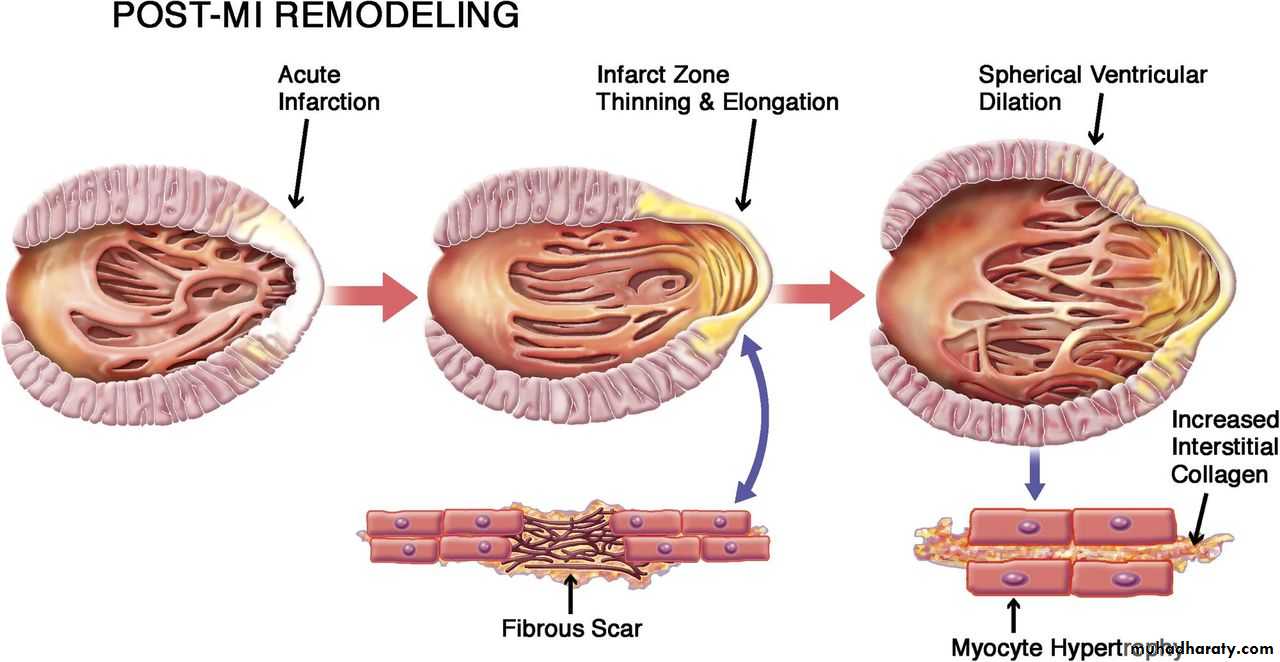
Complications: Ventricular Remodelling
Compensatory hypertrophyof the remaining muscle
Increased myocardial wall
tension
109
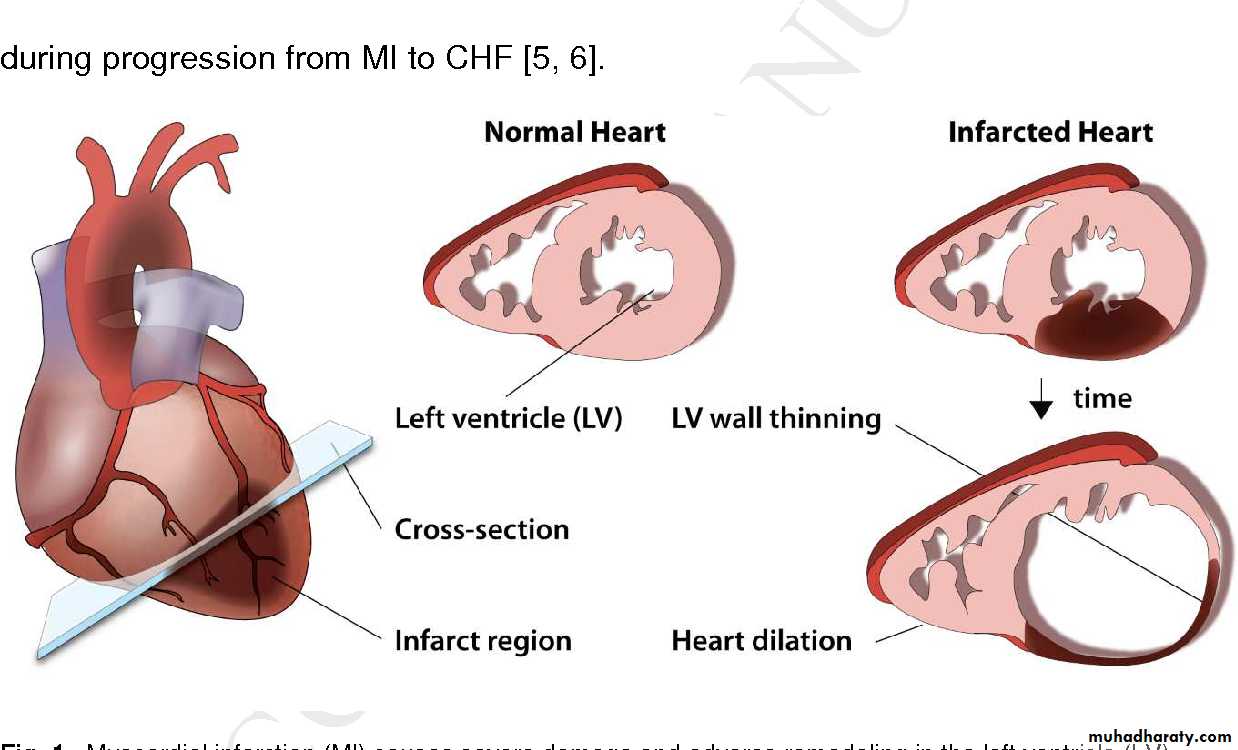
Complications: Ventricular Remodelling
Eventual dilatation anddysfunction of LV,
with the formation
of aneurysm
110
Drugs Used to Prevent Remodelling
Angiotensin converting enzyme inhibitorsAngiotensin receptor blockers
Beta receptor blockers
Mineralocorticoid antagonists
Neprilysin inhibitors (sacubitril)
112
Management After Discharge From Hospital
Risk stratification
Secondary prevention
Rehabilitation
113
Risk Stratification after MI
Assessment for
Residual ischemia
Left ventricular function
arrhythmias
114
Residual Ischemia
Symptomatic patient: Coronary angio with a view to revascularization
Asymptomatic:
Stress testing: routinely done after 4 weeks
If high risk criteria coronary angio
If not repeat ETT every year or if new symptoms appear

115
Assessment of LV function
Clinically
ECG
CXR
Echo
Radioisotope study



116
In Patients with LV dysfunction
Look for reversible ischemia: coronary angio
ACE inhibitors (captopril, enalapril, lisinopril)
Angiotensin receptor blocker (ARBs) (valsartan, losartan, candisartan) in patients who can’t tolerate ACEI
β-blockers: metoprolol, bisoprolol, & carvedilol
Aldosterone receptor antagonist: spironolactone, eplerenone
ARB/neprilysin inhibitor (valsartan/sacubitril)
117
Arrhythmias
Recurrent ventricular arrhythmias, causes:
Residual ischemia
LV dysfunction
The presence of scar tissue
Significant ventricular arrhythmias: mangement
Treatment of LV dysfunction, residual ischemia
Electrophysiological study
Specific anti-arrhythmic therapy
Implantable cardiovertor-defibrillator (ICD)
118
Natural history & prognosis
25% of patients die within a few minutes
40% die within first month
Early death is usually caused by arrhythmia
Later on: the outcome is determined by the extent of myocardial damage
119
Determinants of poor prognosis
Poor LV function
Arrhythmias
Persistent AV block
Anterior infarction > inferior infarction
Old age
Depression
Social isolation