ANATOMY OF THE FOREARM & HAND
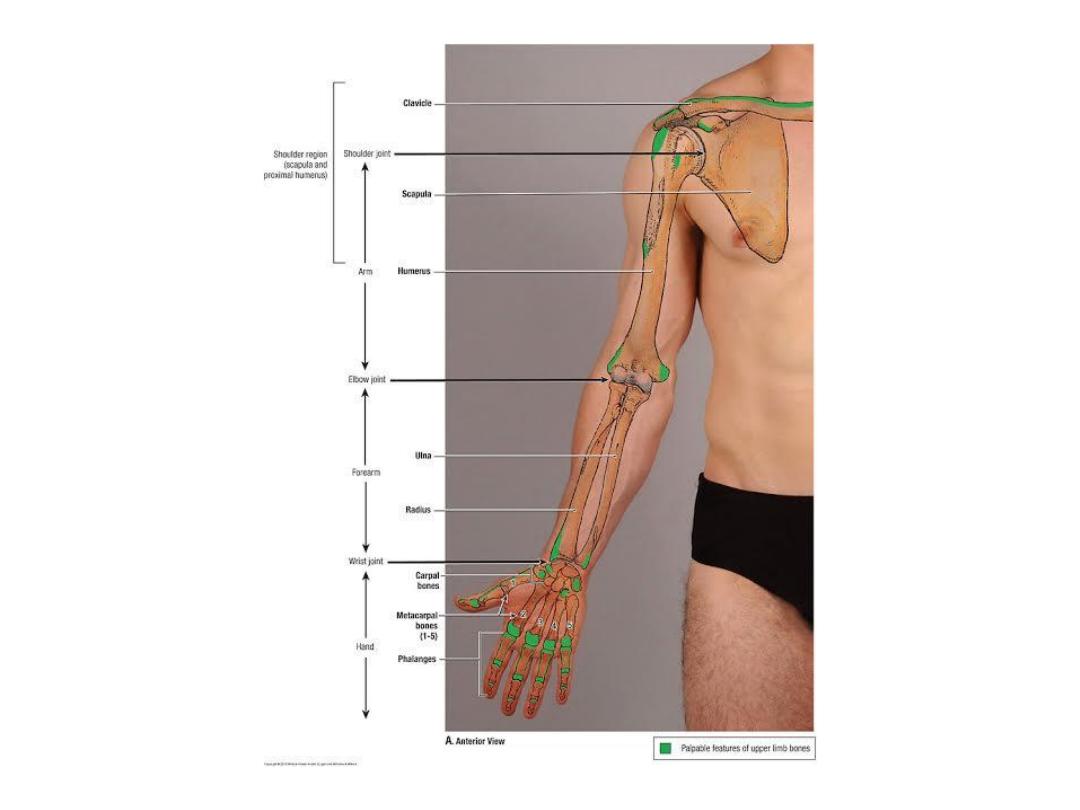
Bones of the Forearm
Radius
The radius is the lateral bone of the forearm . Its proximal end articulates with the humerus at
the elbow joint and with the ulna at the proximal radioulnar joint. Its distal end articulates with
the scaphoid and lunate bones of the hand at the wrist joint and with the ulna at the distal
radioulnar joint.
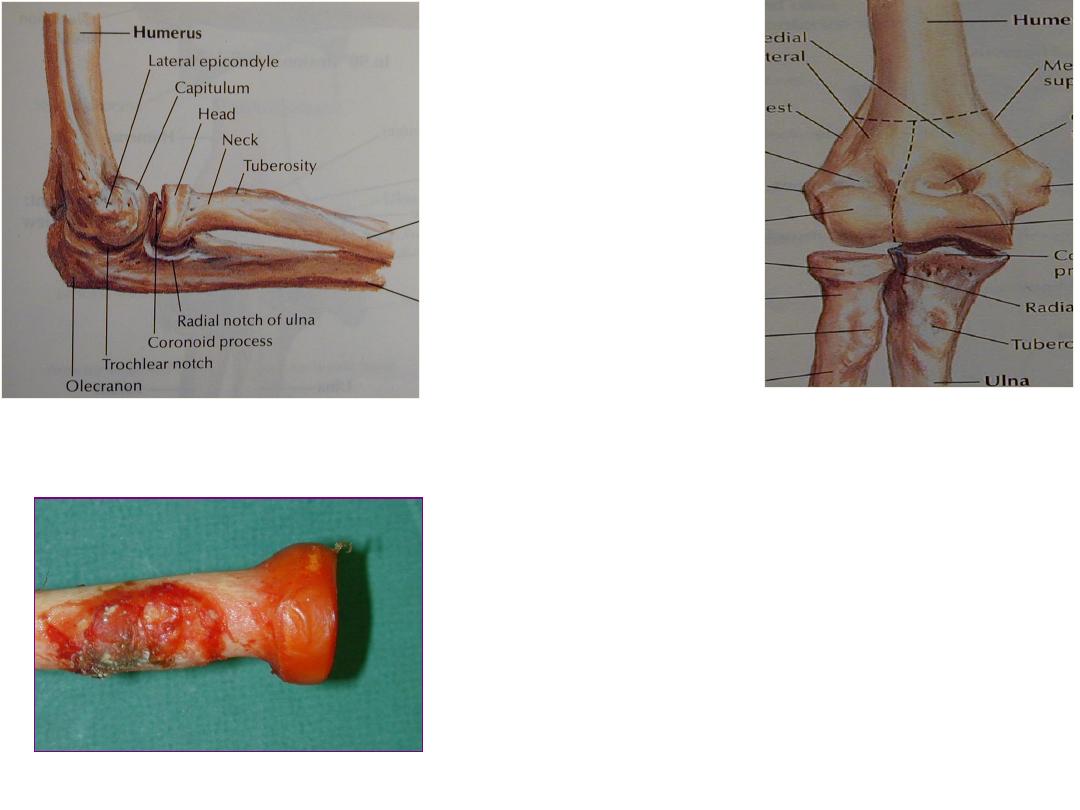
At the proximal end of the radius is the small circular head. The upper surface of the head is
concave and articulates with the convex capitulum of the humerus.
The circumference of the head articulates with the radial notch of the ulna. Below the head, the
bone is constricted to form the neck. Below the neck is the bicipital tuberosity for the insertion
of the biceps muscle.
The shaft of the radius, is wider below than above. It has a sharp interosseous border medially
for the attachment of the interosseous membrane that binds the radius
and ulna together. The pronator tubercle, for the insertion of the pronator teres muscle, lies
halfway down on its lateral side.
At the distal end of the radius is the styloid process; this projects distally from its lateral margin (
On the medial surface is the ulnar notch, which articulates with the round head of the ulna. The
inferior articular surface articulates with the scaphoid and lunate bones. On the posterior aspect
of the distal end is a small tubercle, the dorsal tubercle, which is grooved on its medial side by
the tendon of the extensor pollicis longus.
Dr. Jamal Al-Saidy
Assistant Professor and Consultant Orthopaedic Surgeon
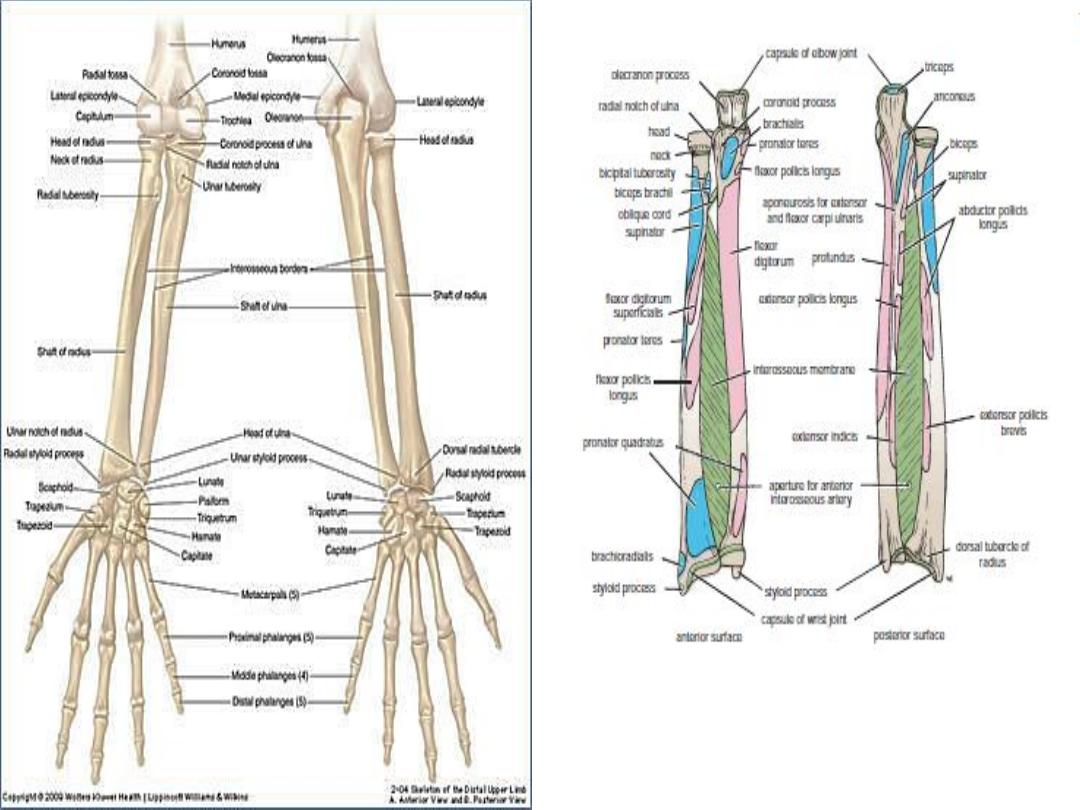
Important muscular and ligamentous
attachments to the radius and the ulna.
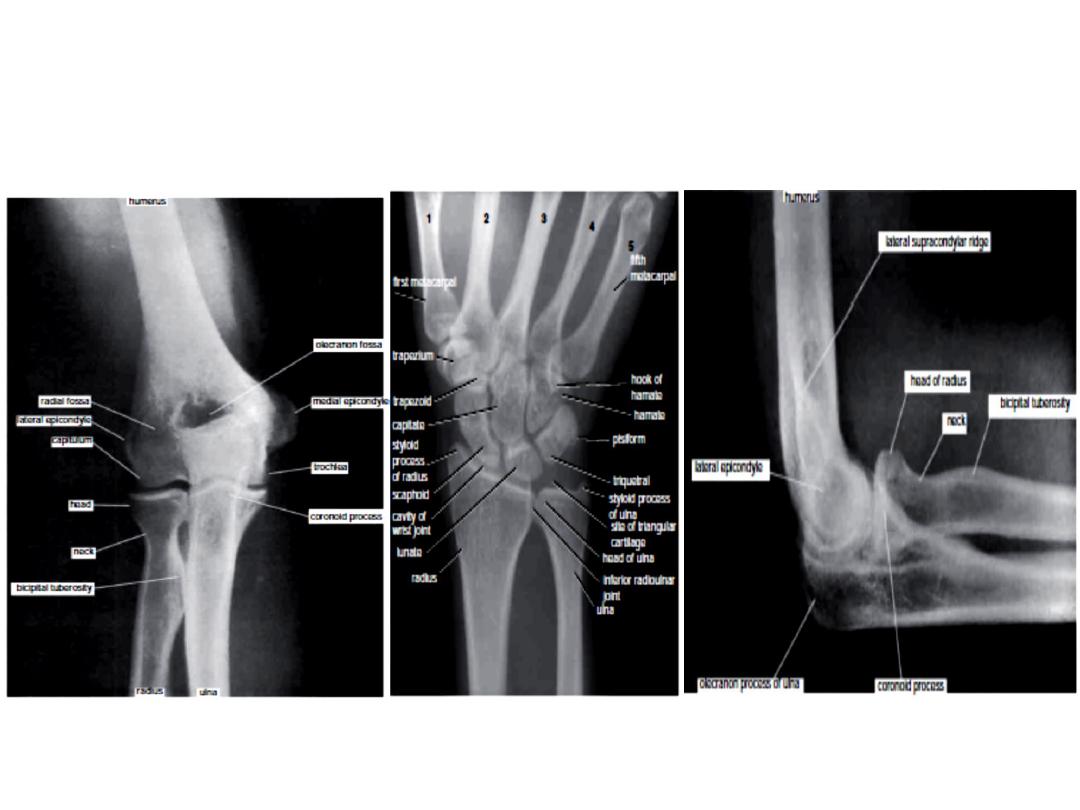
Ulna
The ulna is the medial bone of the forearm. Its proximal end articulates with the
humerus at the elbow joint and with the head of the radius at the proximal radioulnar
joint. Its distal end articulates with the radius at the distal radioulnar joint, but it is
excluded from the wrist joint by the articular disc.
The proximal end of the ulna is large and is known as the olecranon process ; this
forms the prominence of the elbow. It has a notch on its anterior surface, the
trochlear notch, which articulates with the trochlea of the humerus. Below the
trochlear notch is the triangular coronoid process, which has on its lateral surface the
radial notch for articulation with the head of the
radius.
The shaft of the ulna tapers from above down . It has a sharp interosseous border
laterally for the attachment of the interosseous membrane. The posterior border is
rounded and subcutaneous and can be easily palpated throughout its length. Below
the radial notch is the supinator crest that gives origin to the supinator muscle.At the
distal end of the ulna is the small rounded head, which has projecting from its medial
aspect styloid process
c a l n o t e s
i
n
i
C l
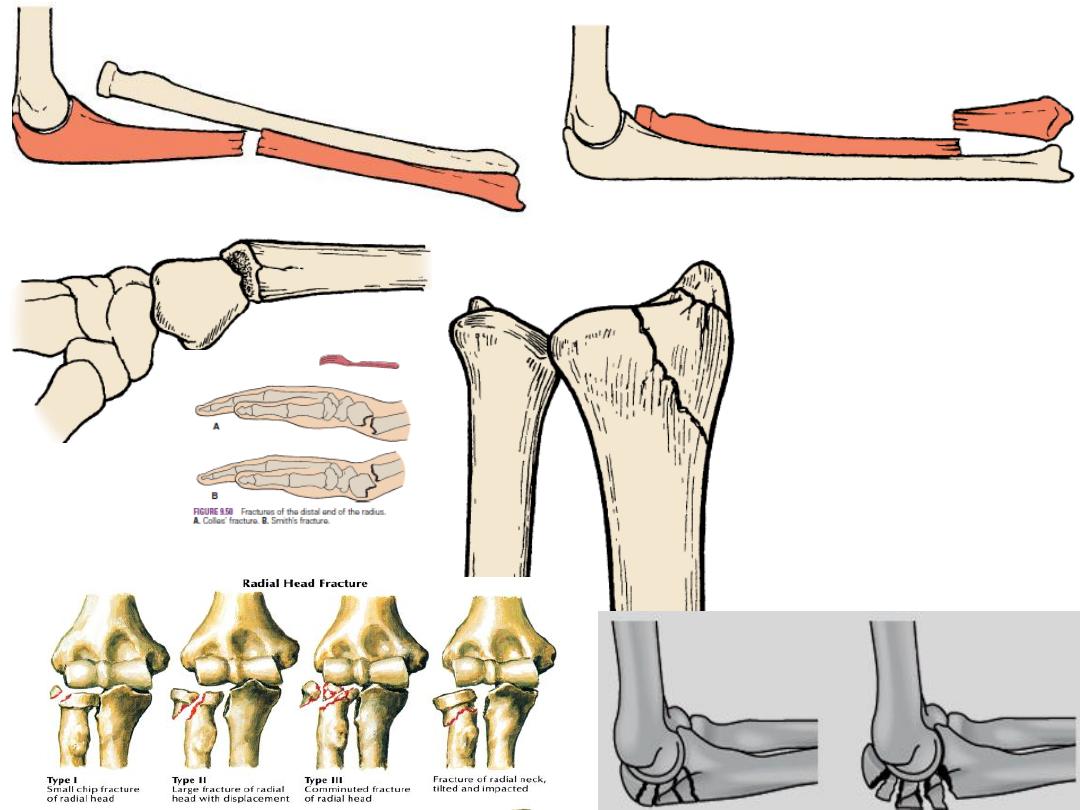
Fractures of the Radius and Ulna
Fractures of the head of the radius can occur from falls on the outstretched hand.
Fractures of the neck of the radius occur in young children from falls on the outstretched hand.
Fractures of the shafts of the radius and ulna may or may not occur together. To restore the
normal movements of pronation and supination, the normal anatomic relationship of the radius,
ulna, and interosseous membrane must be regained. A fracture of one forearm bone may be
associated with a dislocation of the other bone.
Monteggia’s fracture, for example, the shaft of the ulna is fractured and dislocation of the radial
head.
Galeazzi’s fracture, the proximal third of the radius is fractured and the distal end of the ulna is
dislocated at the distal radioulnar joint.
Fractures of the olecranon process can result from a fall on the flexed elbow or from a direct
blow. Depending on the location, the bony fragment may be displaced by the pull of the triceps
muscle, which is inserted on the olecranon process
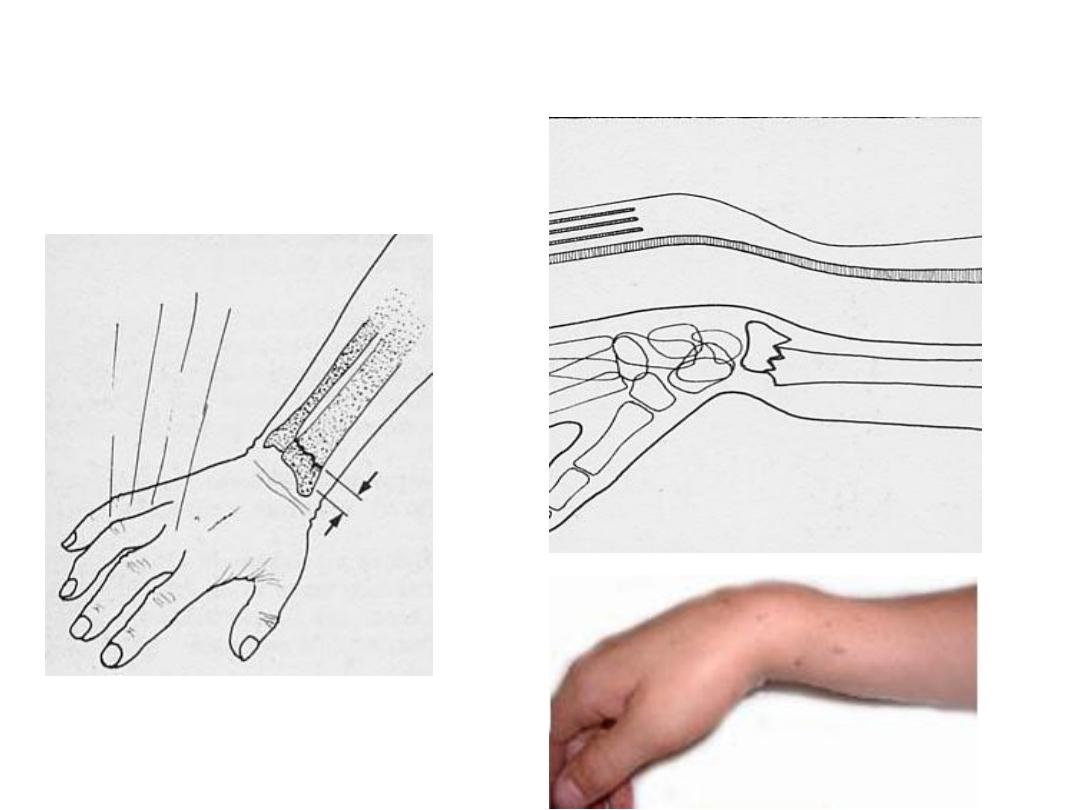
Colles’ fracture is a fracture of the distal end of the radius resulting from a fall on the
outstretched hand. It commonly occurs in patients older than 50 years. The force drives the
distal fragment posteriorly and superiorly “dinner-fork deformity”.
Smith’s fracture is a fracture of the distal end of the radius and occurs from a fall on the back of
the hand. It is a reversed Colles’ fracture because the distal fragment is displaced anteriorly.
Olecranon Bursitis A small subcutaneous bursa is present over the olecranon process of the
ulna, and repeated trauma often produces chronic bursitis.
Monteggia’s fracture
Smith’s fracture
Fractures of the olecranon process
Fractures of the styloid process
Galeazzi’s fracture,

Fractures of both radius& ulna
a fall on the outstretched hand
Forearm deformity due to trauma
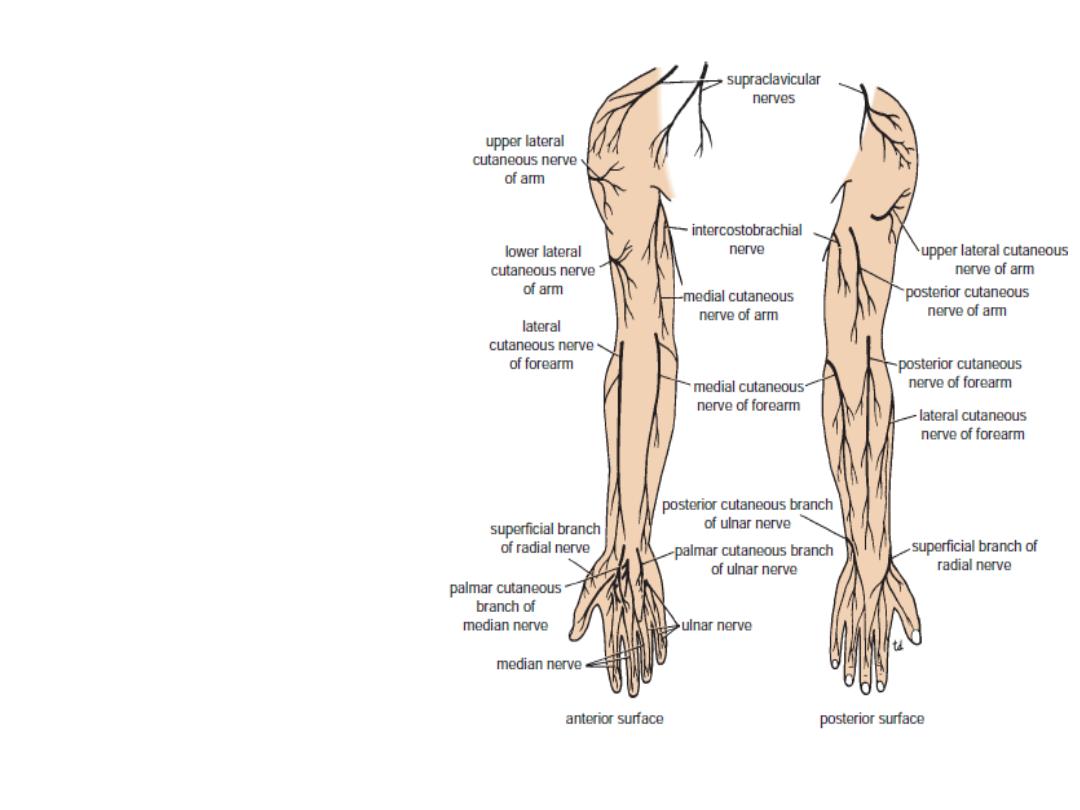
The
sensory nerve supply
to
the skin of the forearm
is from the anterior and posterior
branches of the lateral cutaneous
nerve of the forearm,
a continuation of the
musculocutaneous
nerve, and from the anterior and
posterior
Branches of the medial cutaneous
nerve of the forearm .
A narrow strip of skin down the
middle of the posterior
surface
of the forearm is supplied by the
posterior cutaneous
nerve of the forearm.
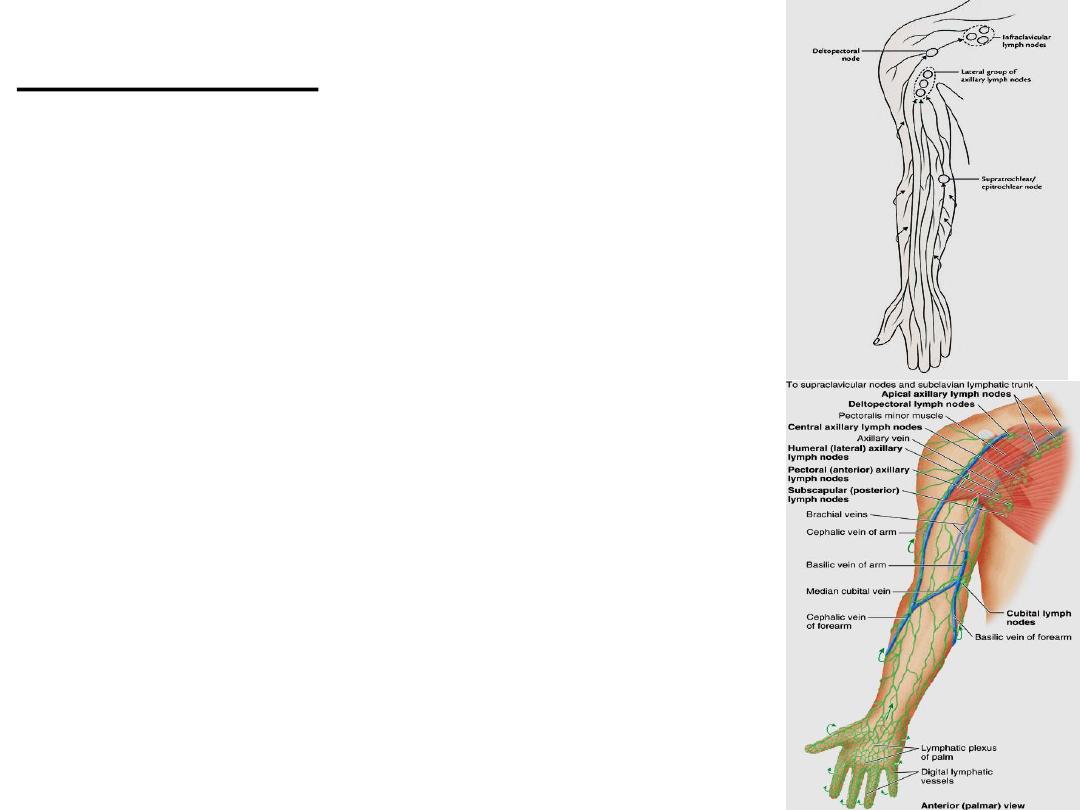
Draing
Lymphatic
• The superficial lymph vessels from the thumb and
lateral fingers and the lateral areas of the hand and forearm
follow the cephalic vein to the infraclavicular group
of nodes .
• Those from the medial fingers and the medial areas
of the hand and the forearm follow the basilic vein to the
cubital fossa.
• Here, some of the the vessels drain into the
supratrochlear lymph node.
• whereas others bypass the node and accompany
the basilic vein to the axilla, where they drain into the
lateral group of axillary nodes.
• The efferent vessels from the supratrochlear node
also drain into the lateral axillary nodes.
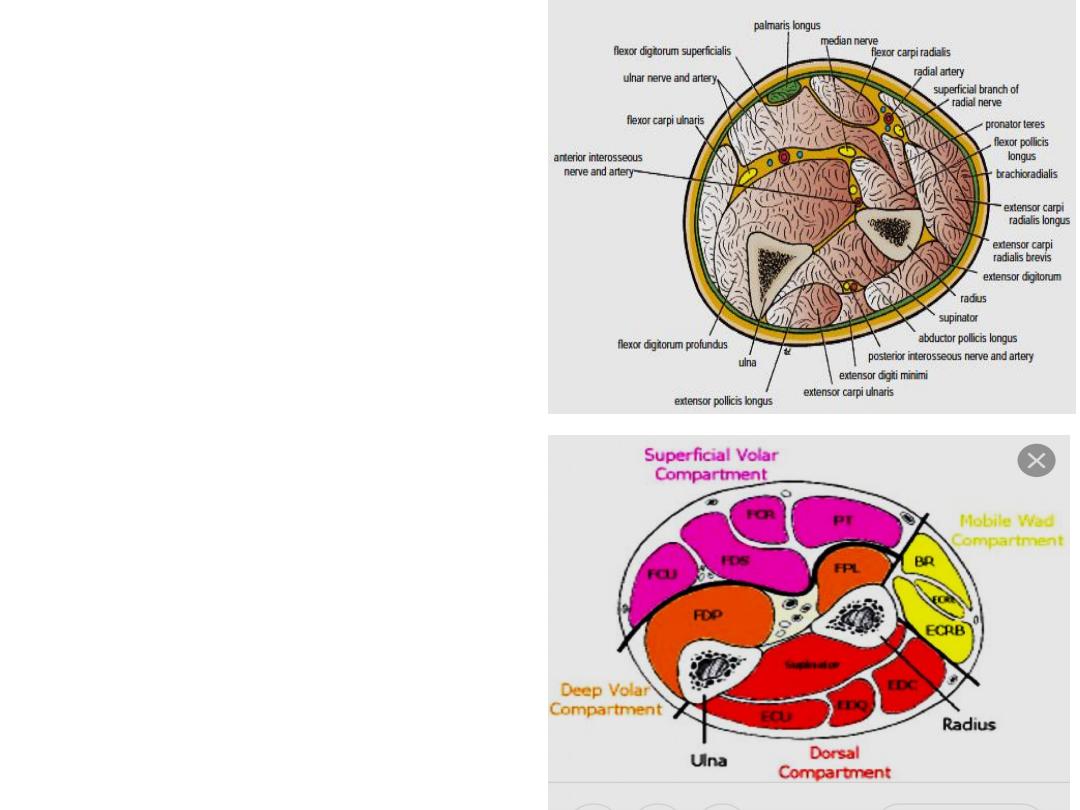
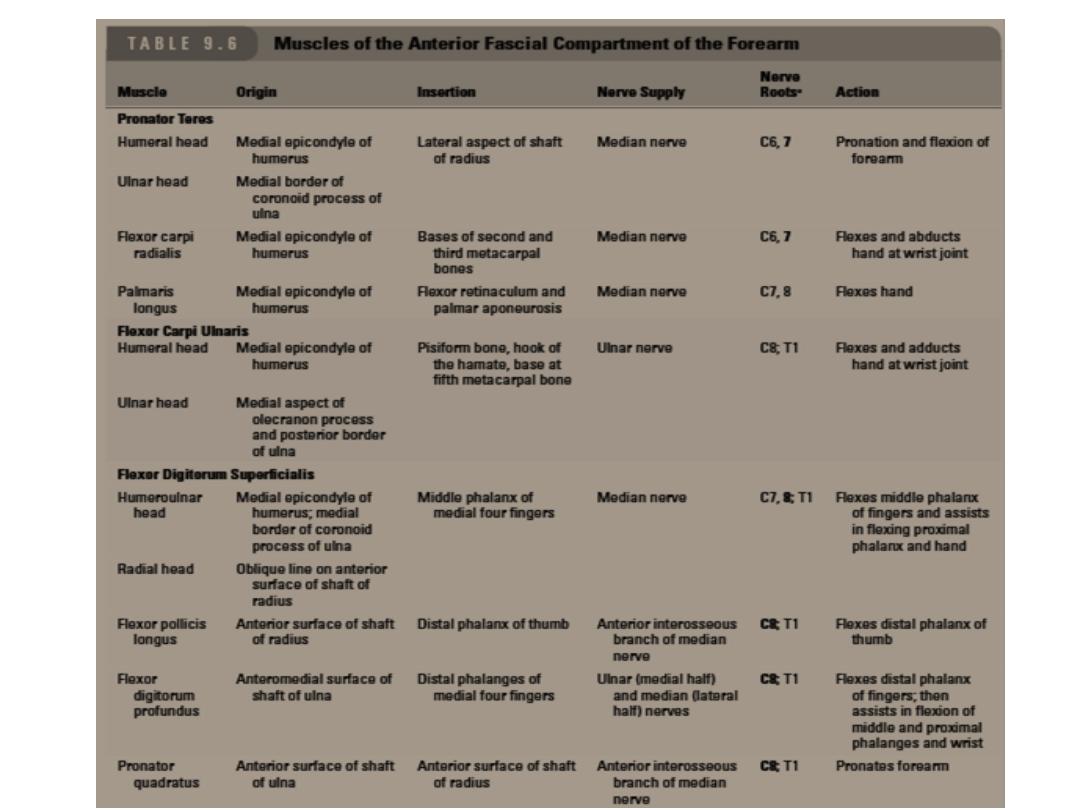
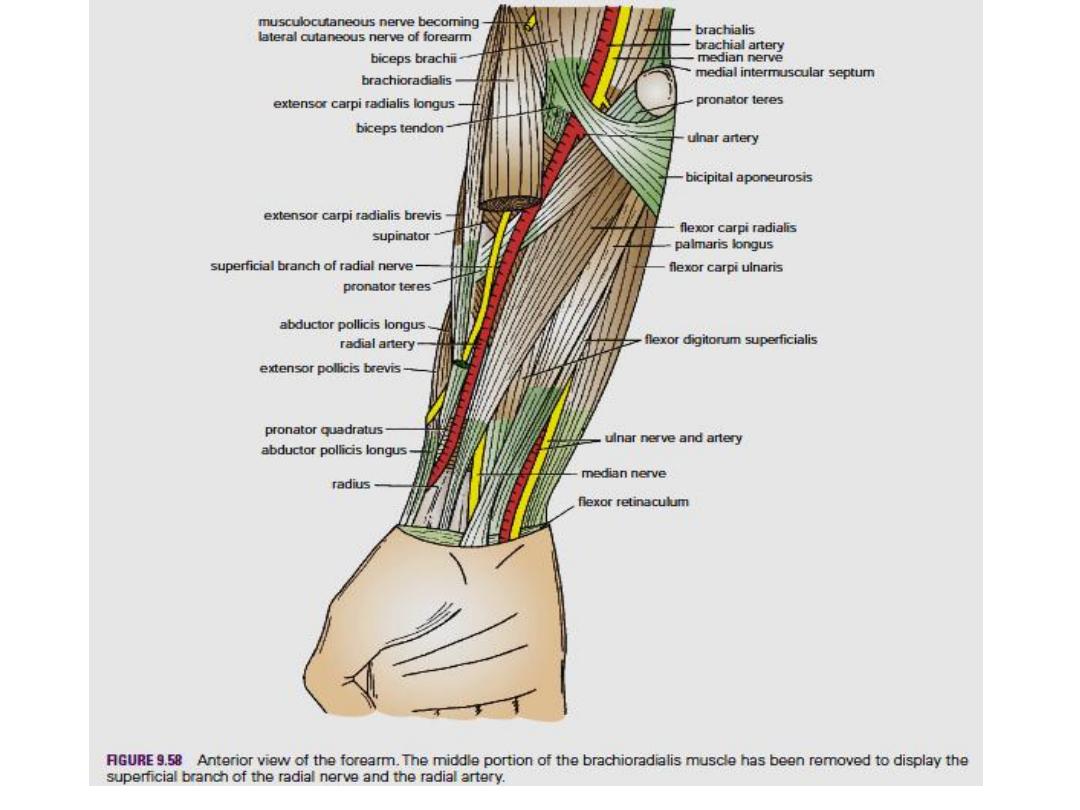
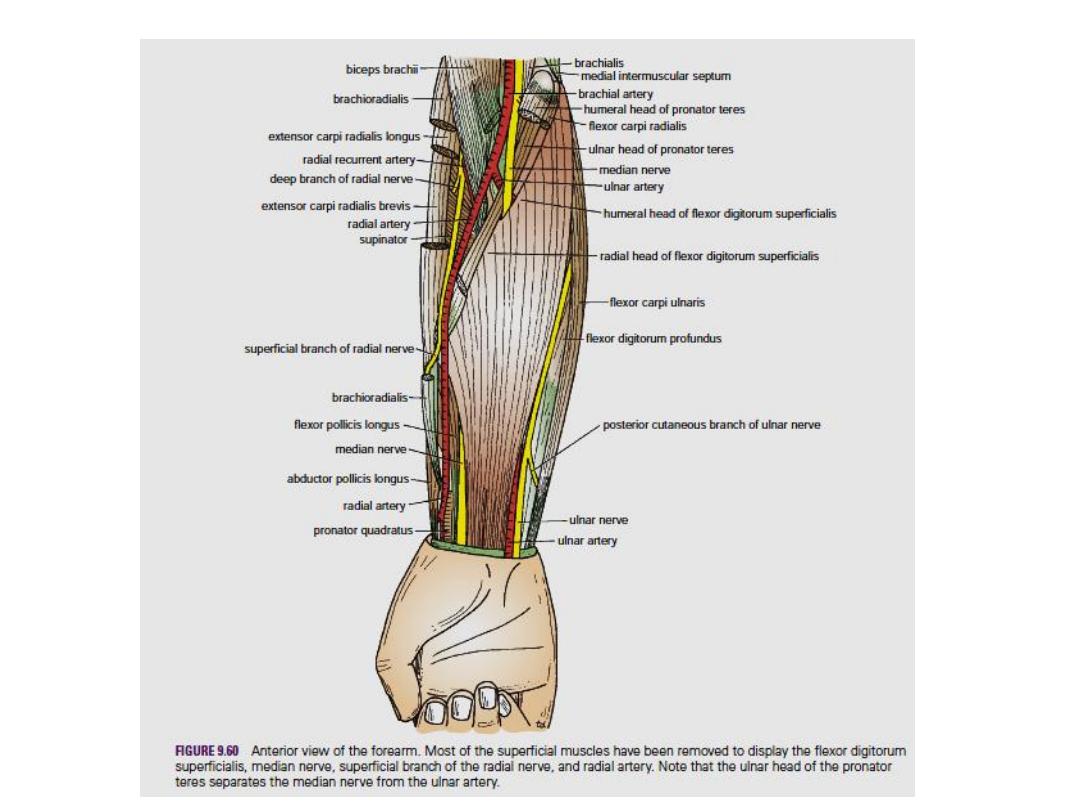
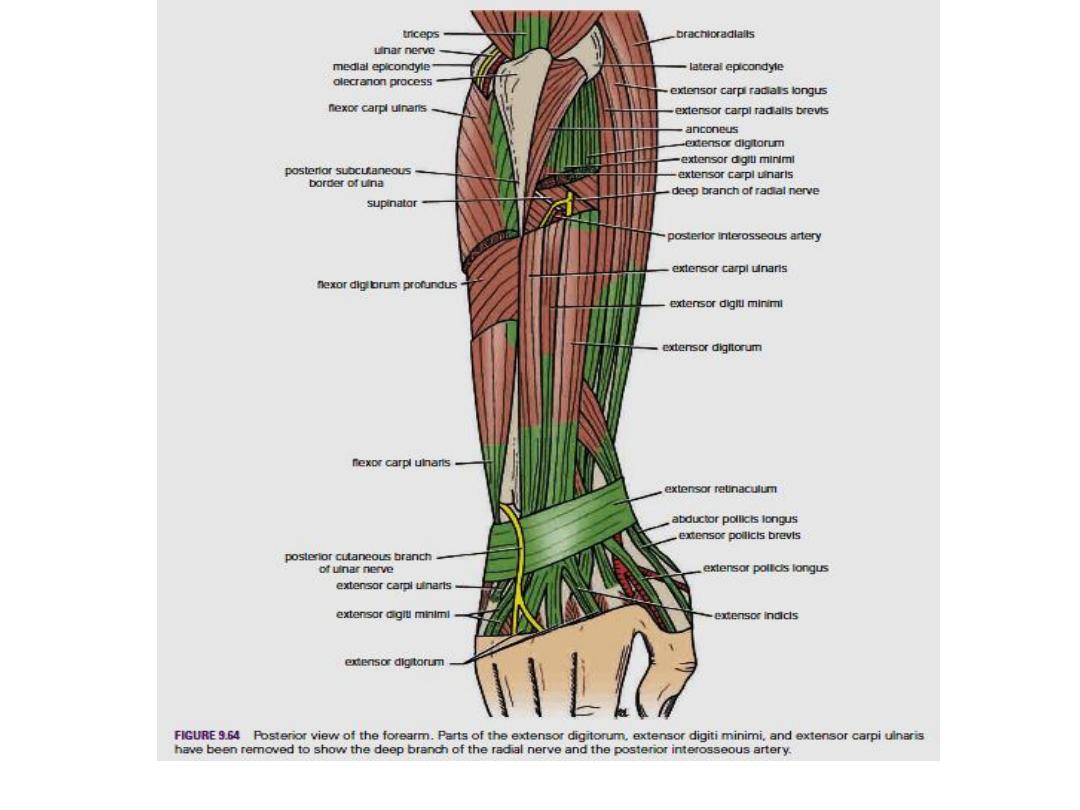
Compartments of the forearm
The forearm is enclosed in a sheath of
deep fascia, which is attached to the
periosteum of the posterior subcuta-
neous border of the ulna . This fascial
sheath, together with the interosseous
membrane and fibrous intermuscular
septa, divides the forearm into several
compartments, each having its own
muscles, nerves, and blood supply.
There is very little room within
each compartment, and any edema
can cause secondary vascular compression
of the blood vessels, and therefore causing a
condition known as Compartment Syndrome .
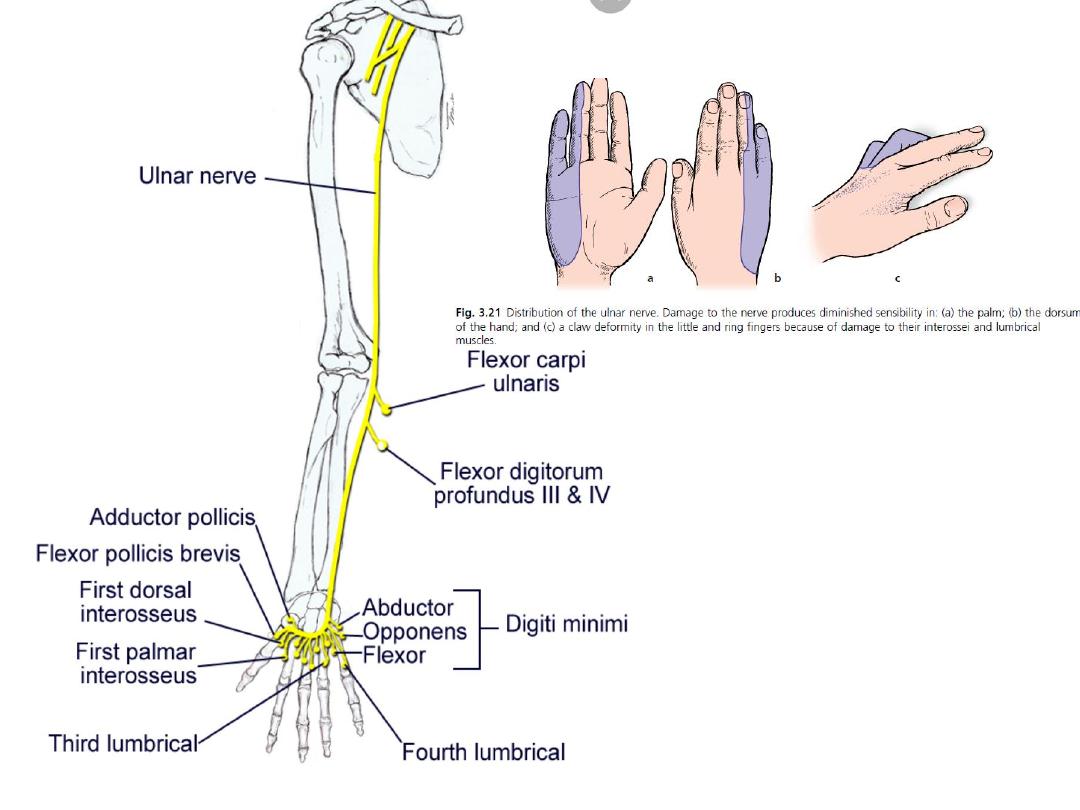
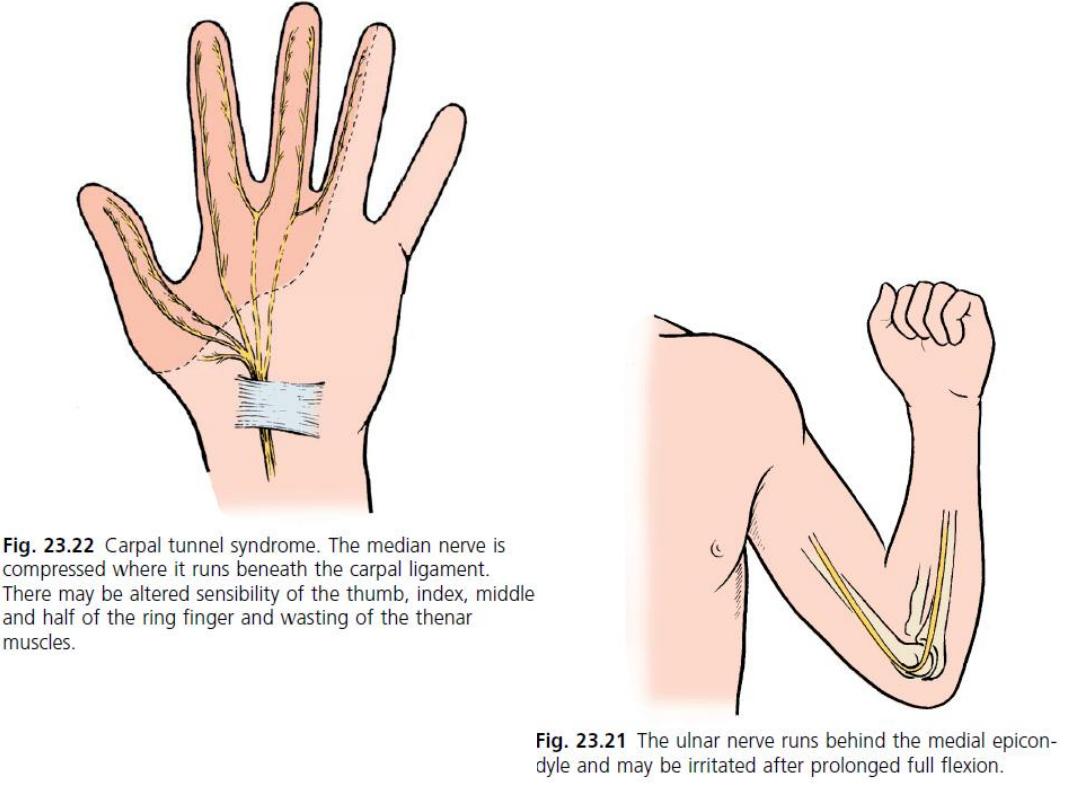
Ulnar nerve
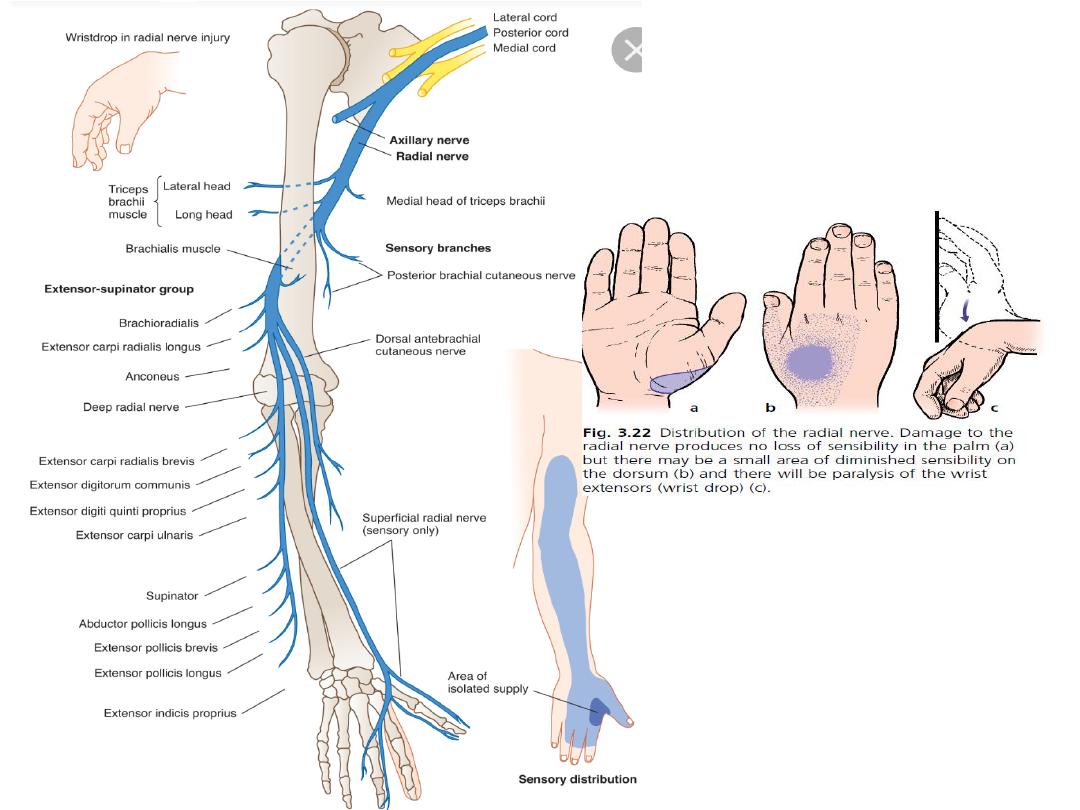
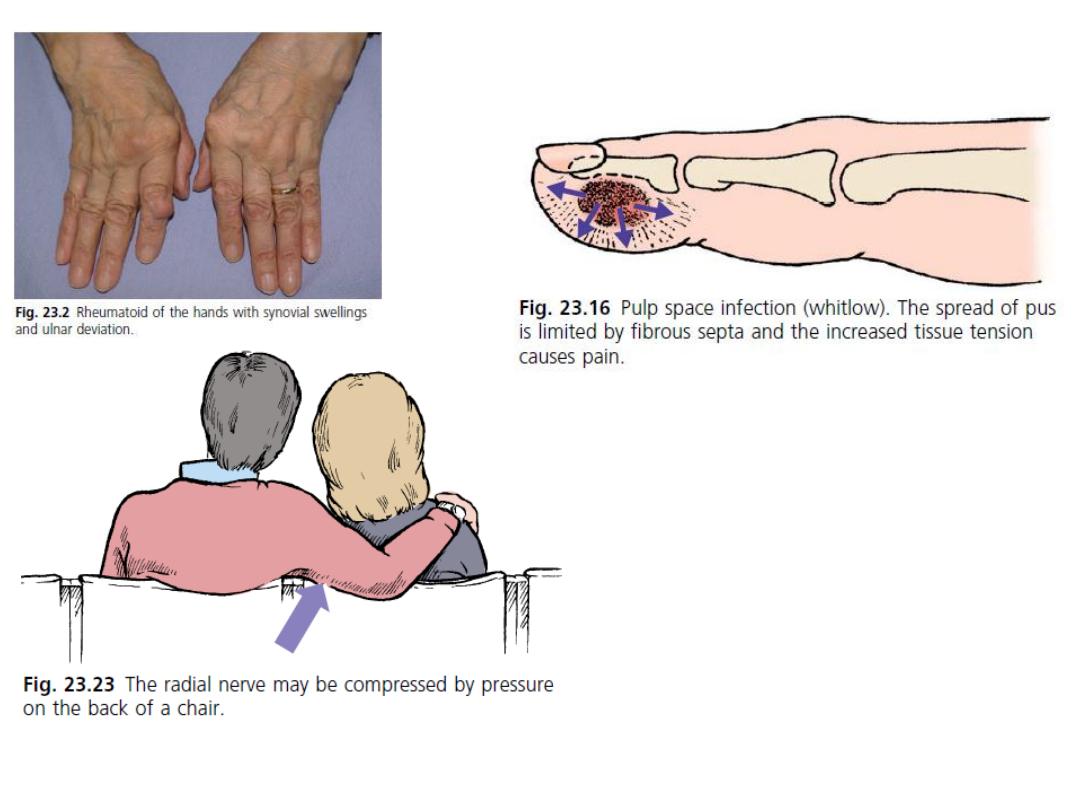
Radial nerve
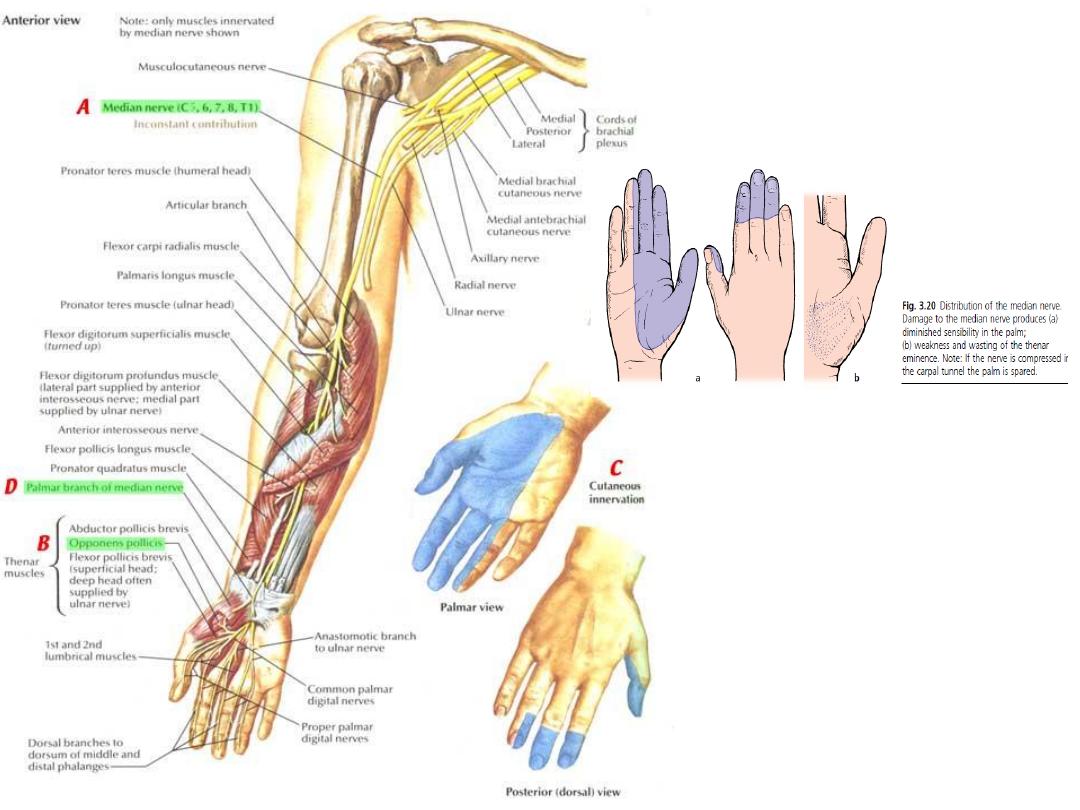
Median nerve
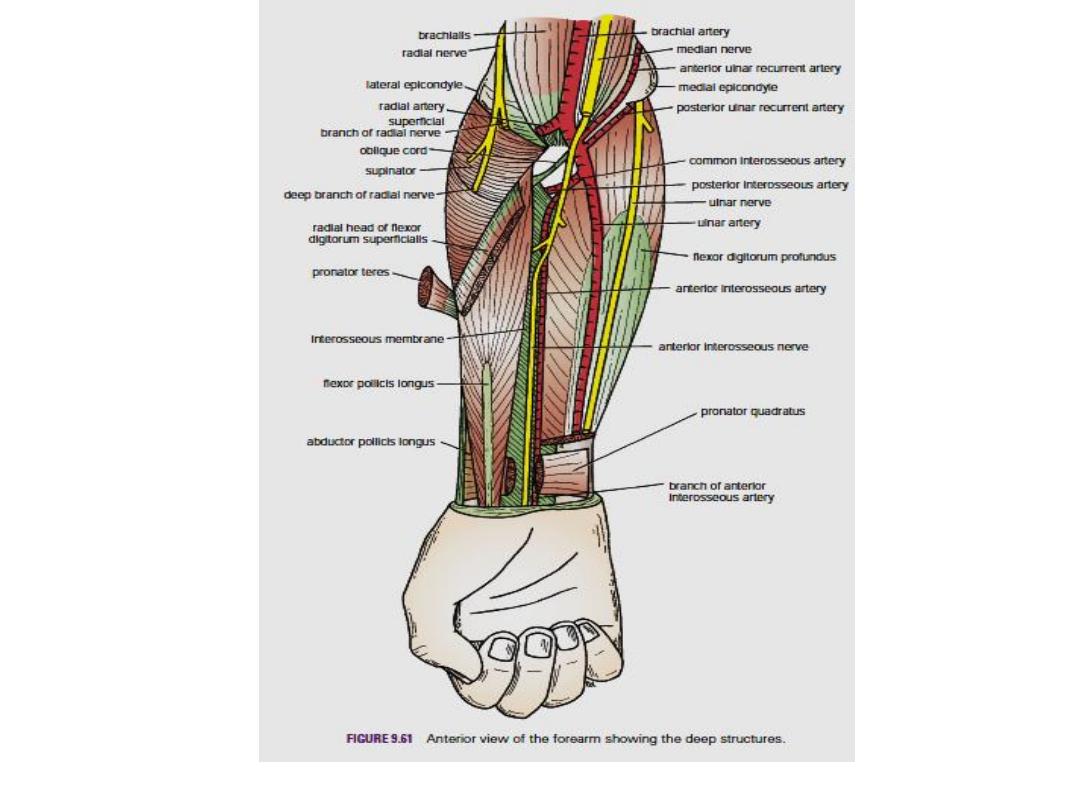
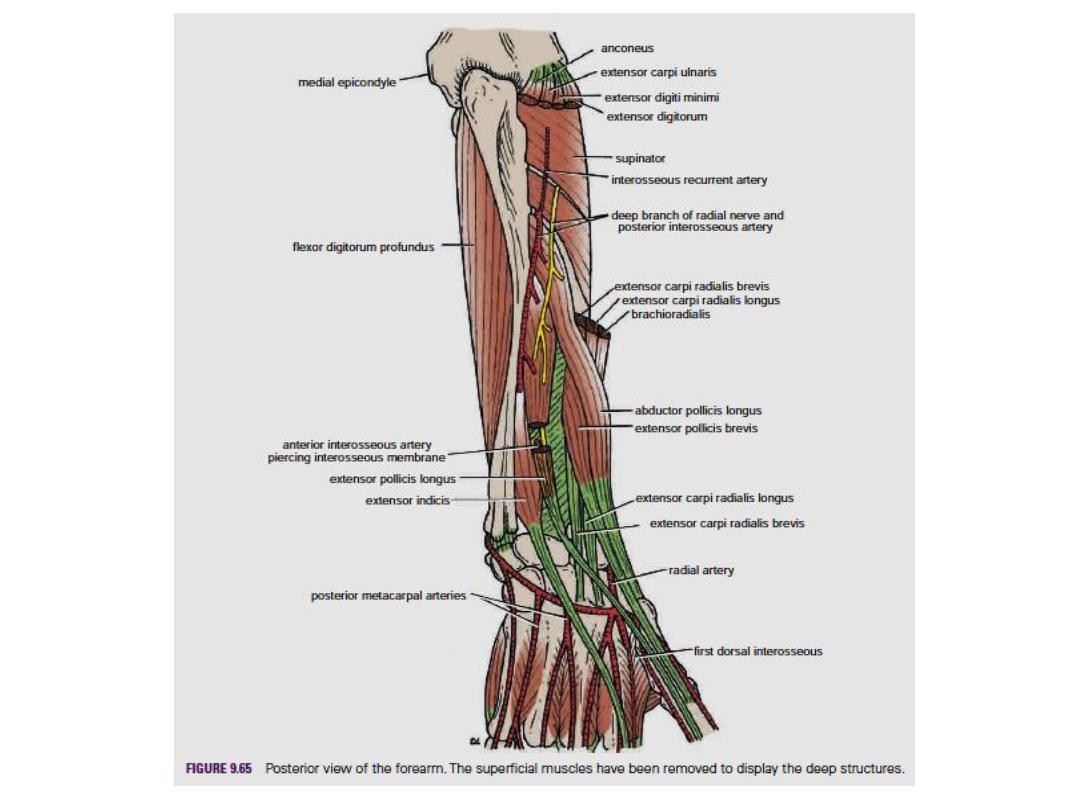
The interosseous membrane :- It is a strong membrane that unites the shafts of the radius
and the ulna; it is attached to their interosseous borders and provides attachment for
neighboring muscles.
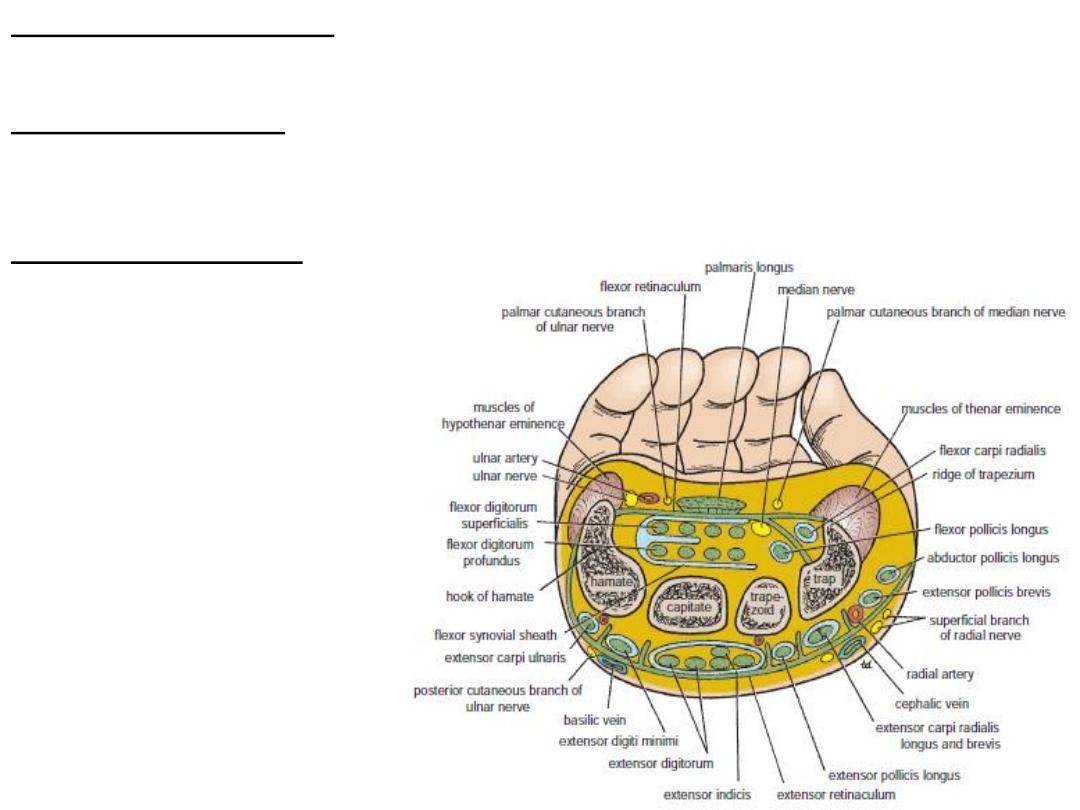
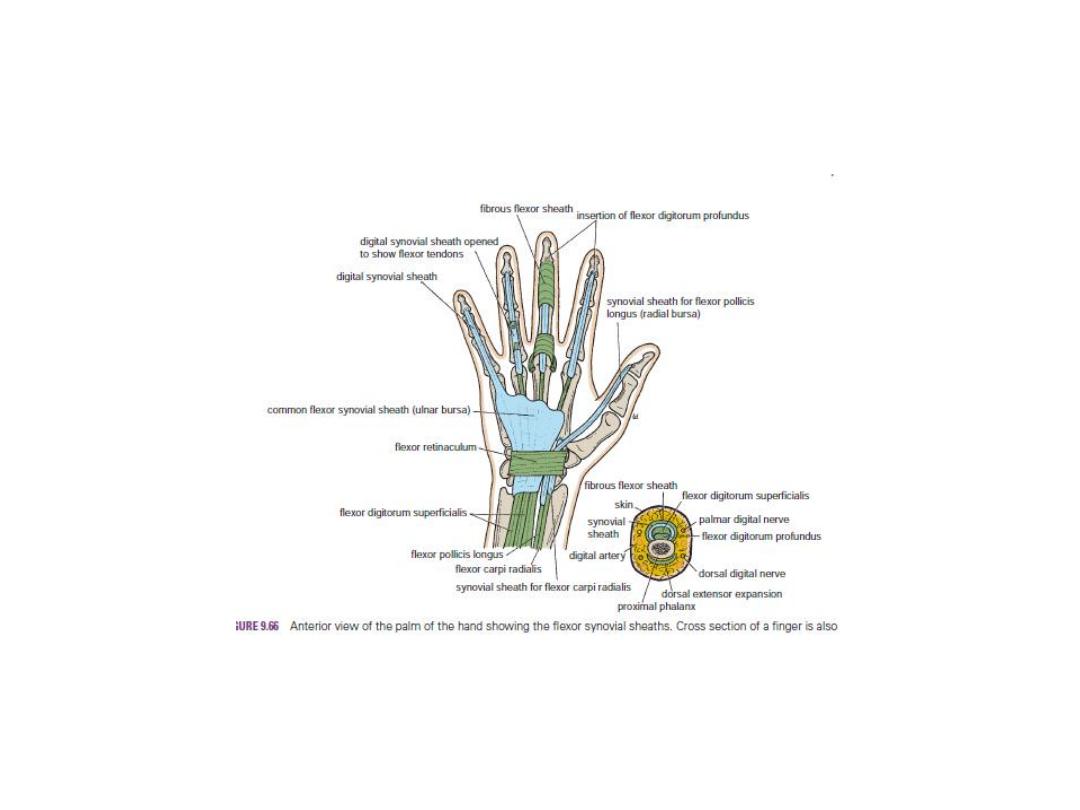
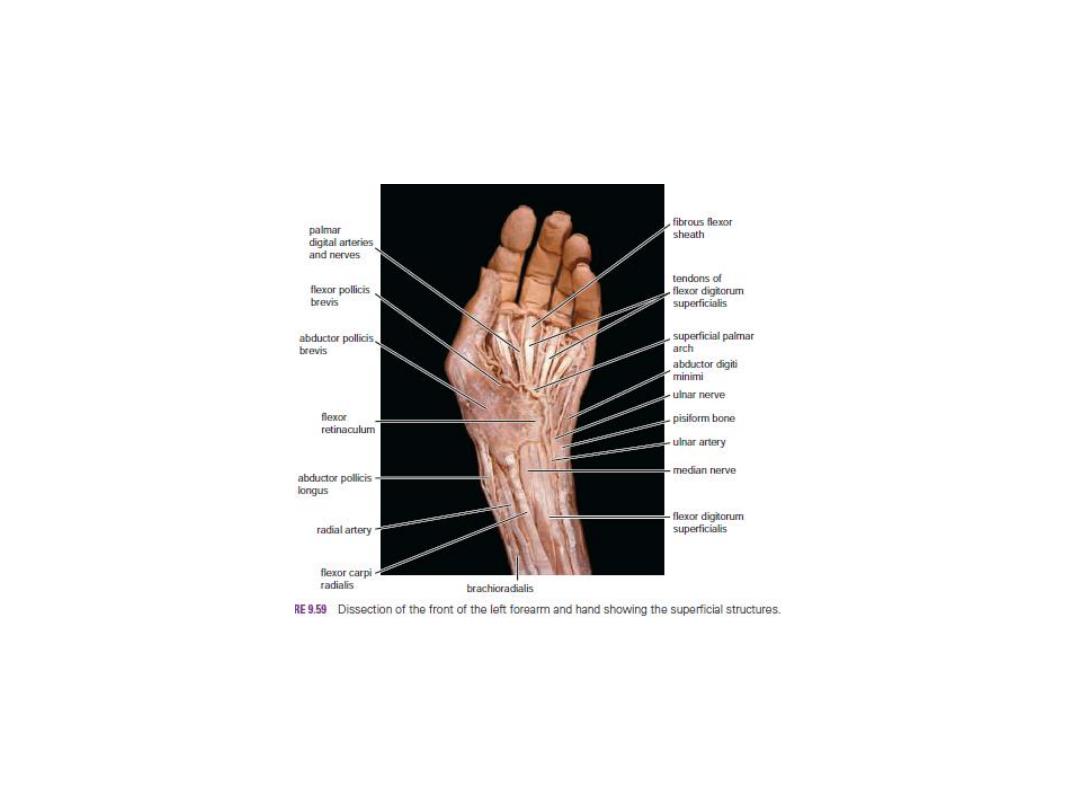
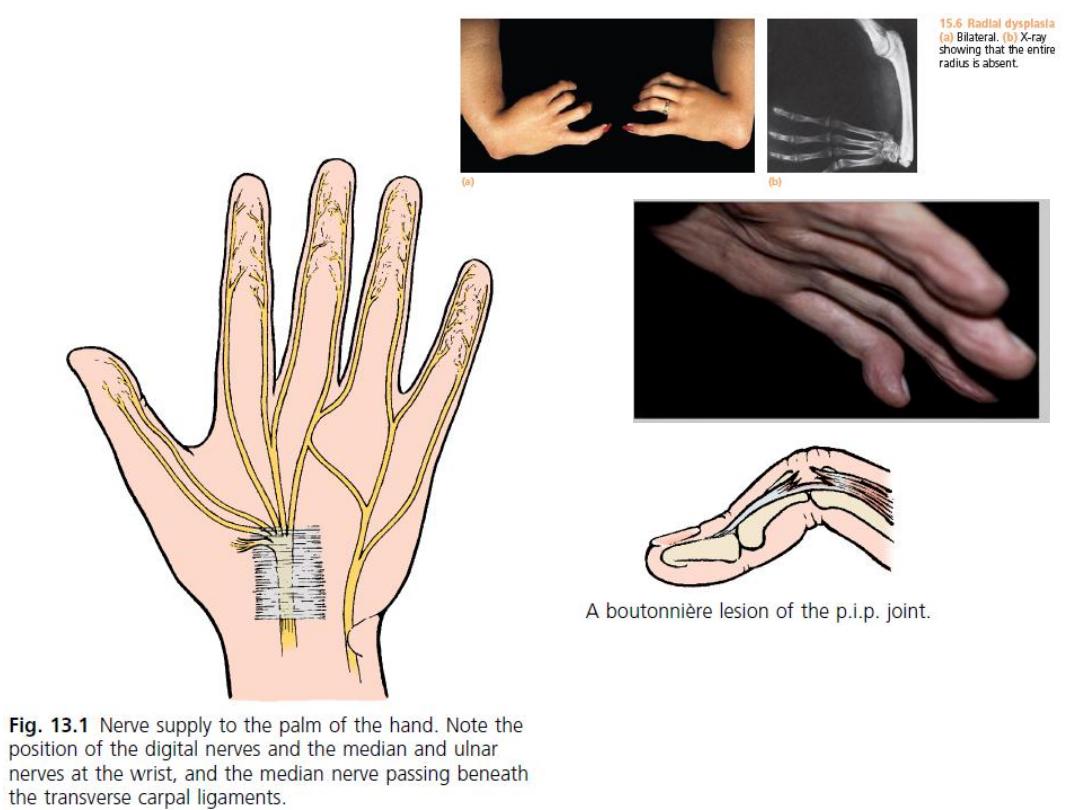
The flexor retinaculum :- It is a thickening of deep fascia that holds the long flexor tendons
in position at the wrist. It stretches across the front of the wrist and converts the concave
anterior surface of the hand into an osteofascial tunnel, the carpal tunnel, for the passage of
the median nerve and the flexor tendons of the thumb and fingers.
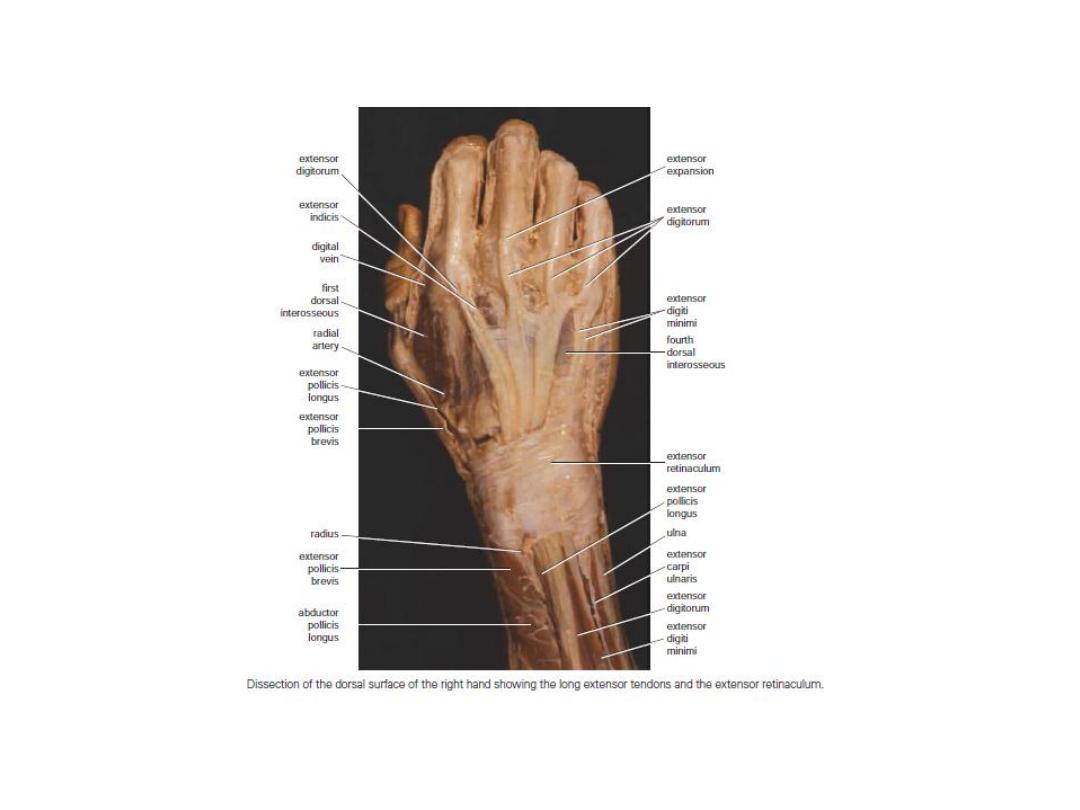
The extensor retinaculum :-
It is a thickening of deep fascia
that stretches across the back
of the wrist and holds the long
extensor tendons in position.
It converts the grooves on the
posterior surface of the distal
ends of the radius and ulna into
six separate tunnels for the
passage of the long extensor
tendons.
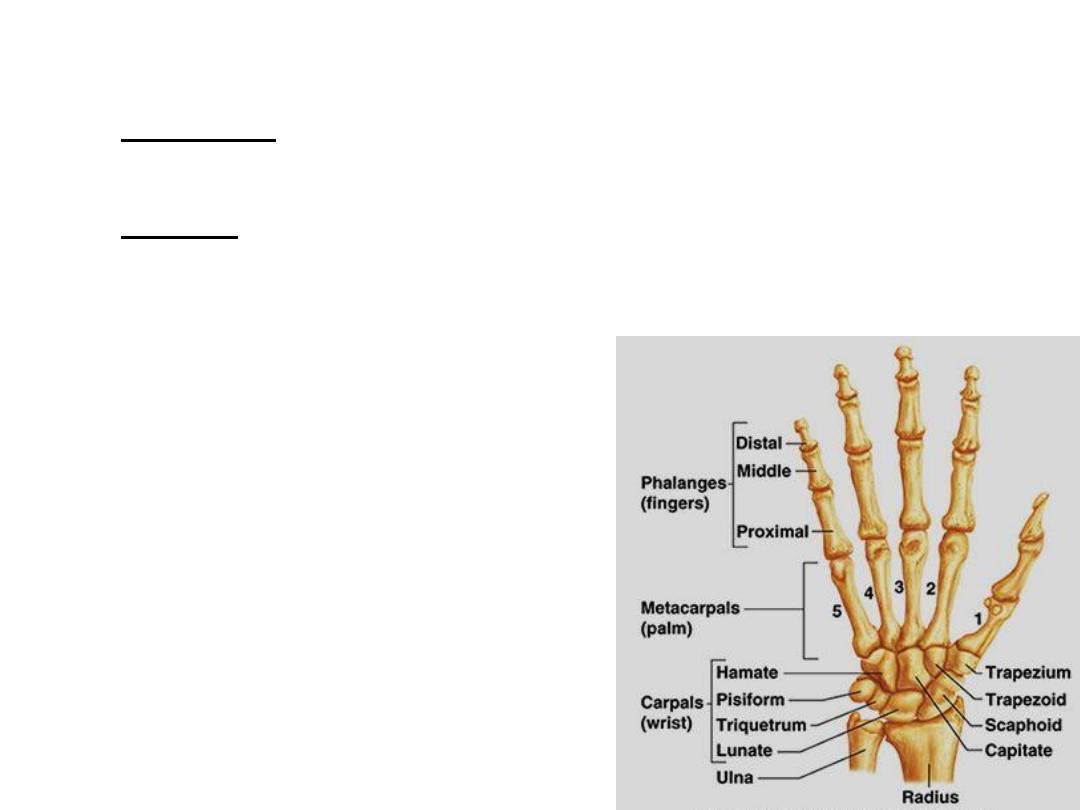
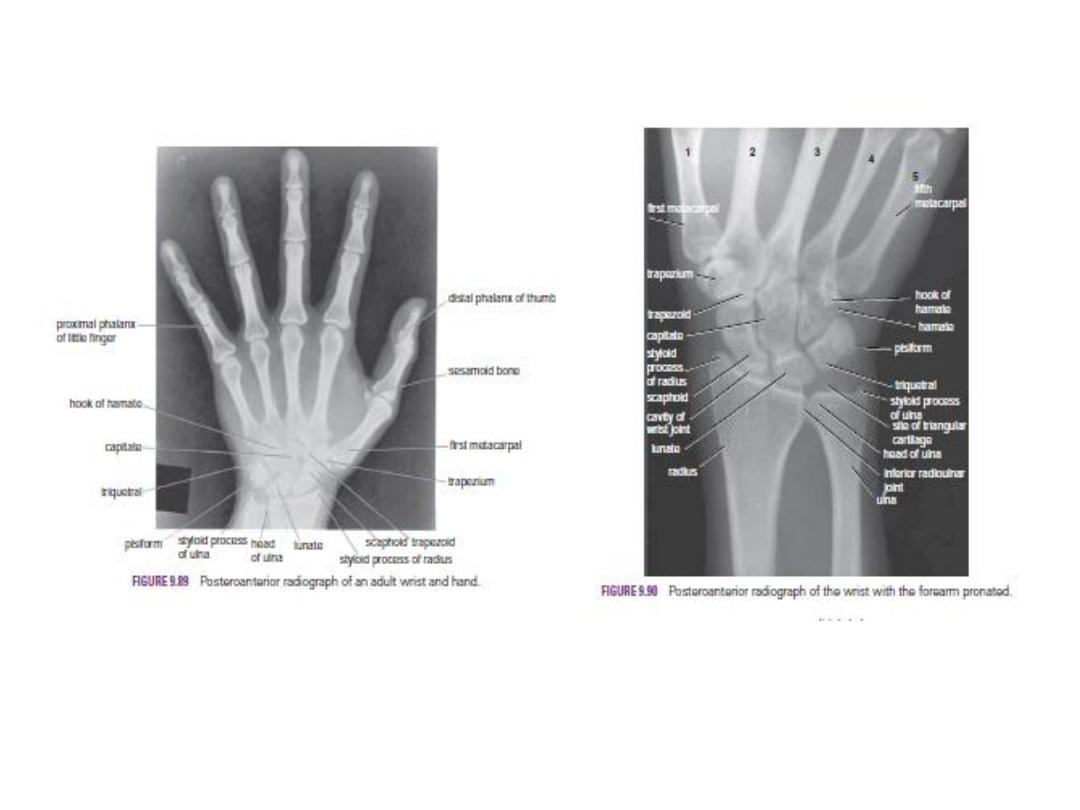
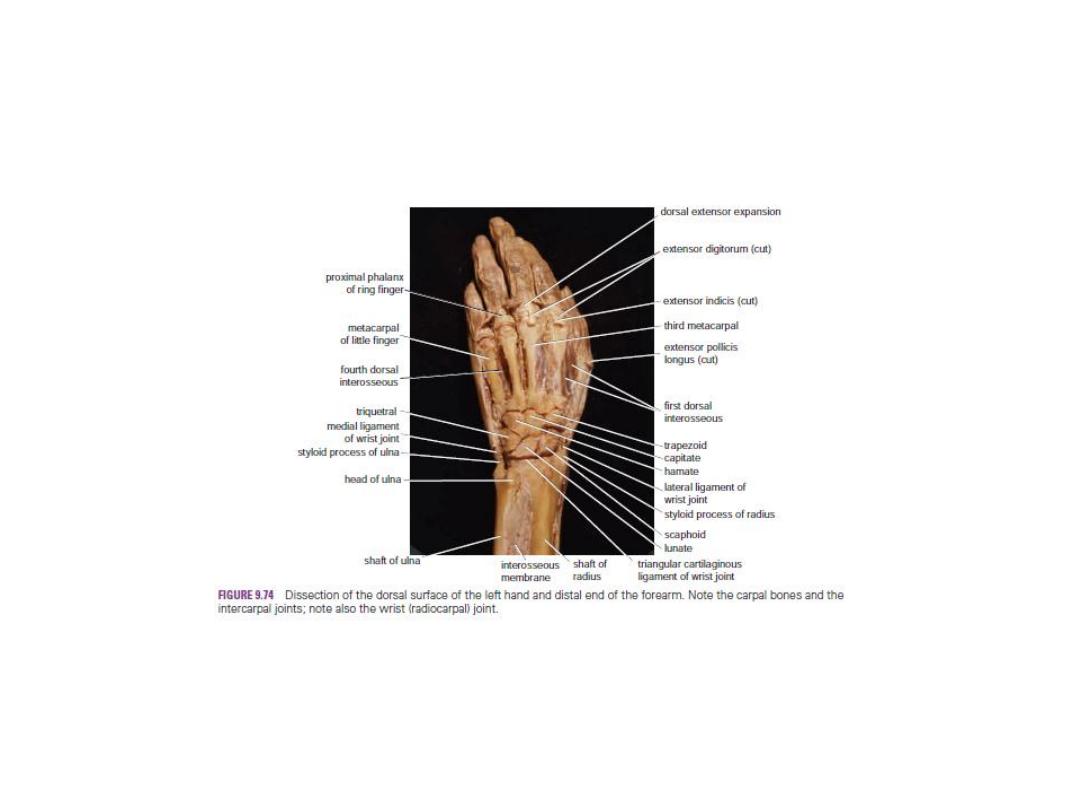
Bones of the Hand
There are eight carpal bones, made up of two rows of four.
The proximal row consists of (from lateral to medial) the:-
scaphoid, lunate, triquetral, and pisiform bones.
The distal row consists of (from lateral to medial) the:-
trapezium, trapezoid, capitate, and hamate bones.
Together, the bones of the carpus present on their anterior surface a concavity, to the
lateral and medial edges of which is attached a strong membranous band called the flexor
retinaculum.
In this manner, an osteofascial tunnel
the carpal tunnel is formed for the passage
of the median nerve and the
flexor tendons of the fingers.
The bones of the hand are cartilaginous at birth.
The capitate begins to ossify during the first year,
and the others begin to ossify at intervals thereafter
until the 12th year, when all the bones are ossified.
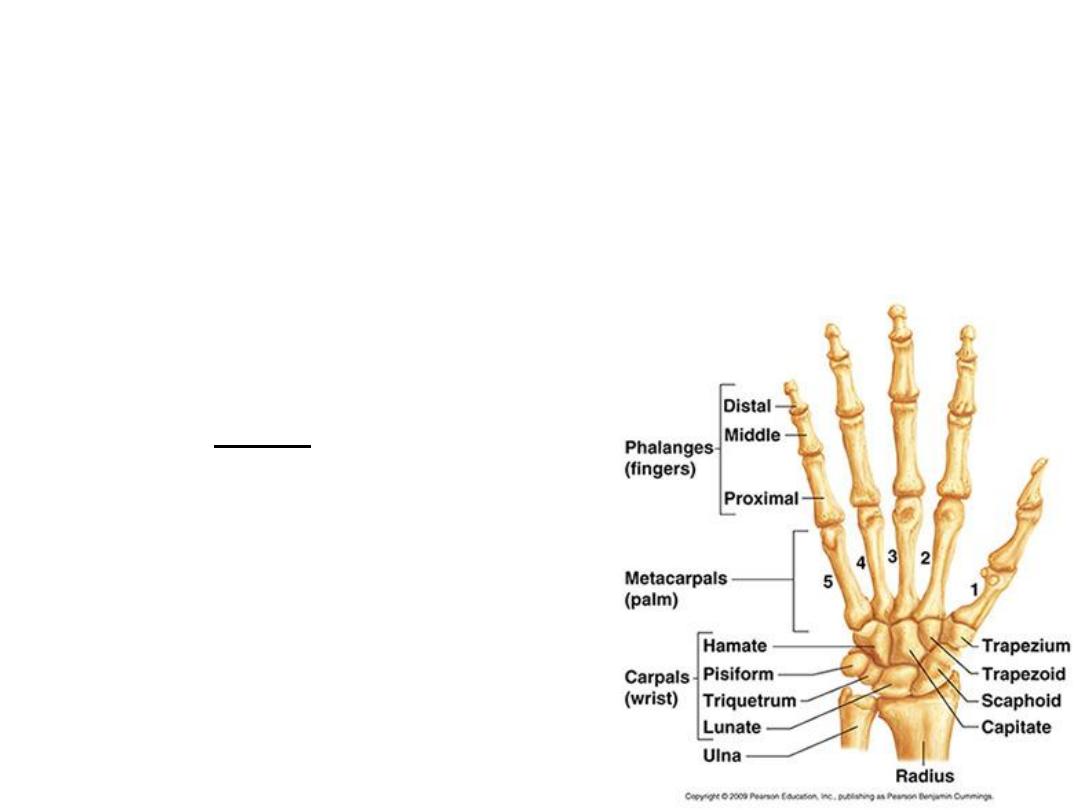
The Metacarpals and Phalanges
There are five metacarpal bones, each of which has:-
a base, a shaft, and a head
The first metacarpal bone of the thumb is the shortest and most mobile. It does not lie in
the same plane as the others but occupies a more anterior position. It is also rotated
medially through a right angle so that its extensor surface is directed laterally and not
backward.
The bases of the metacarpal bones articulate
with the distal row of the carpal bones the heads
which form the knuckles articulate with the
proximal phalanges . The shaft of each metacarpal
bone is slightly concave forward and is triangular
in transverse section. Its surfaces are posterior
lateral, and medial.
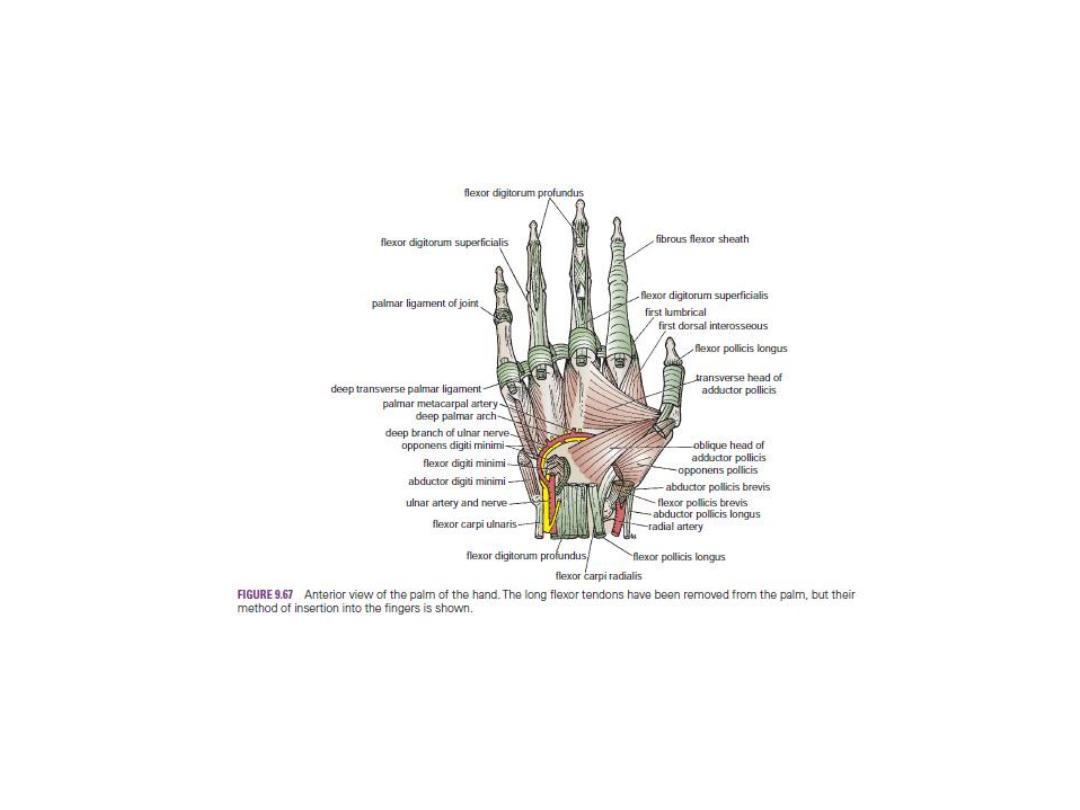
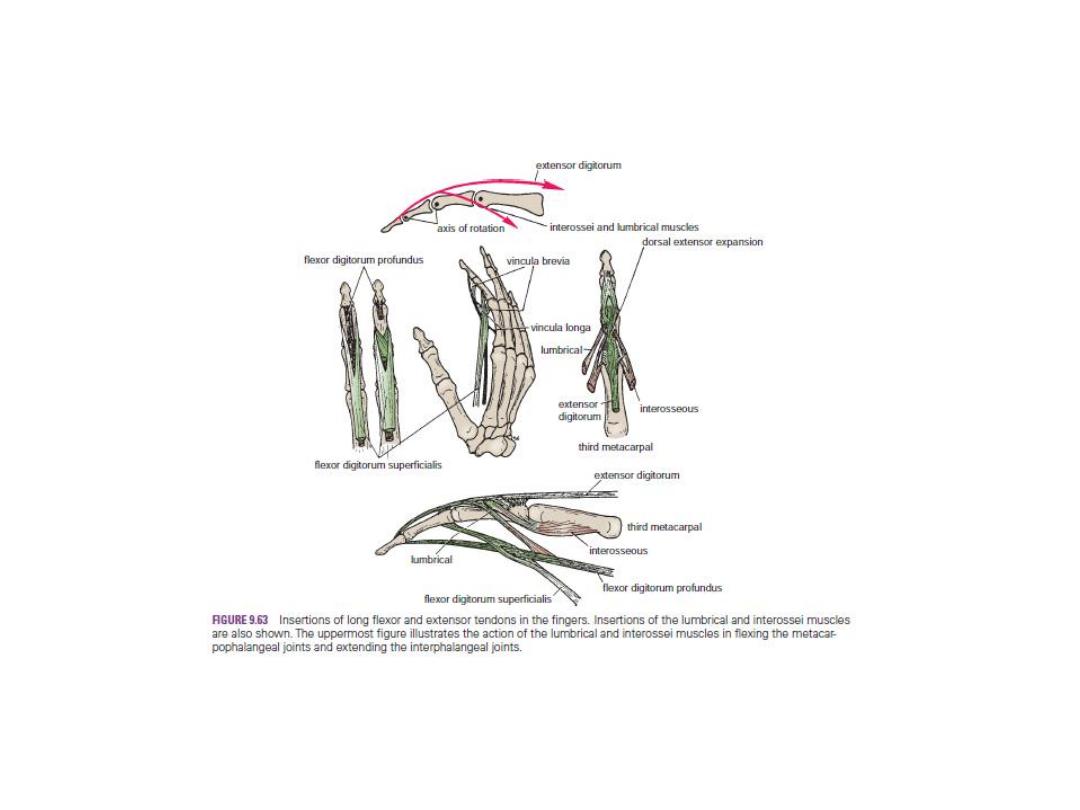
There are three phalanges for each of the
fingers but only two for the thumb.
The important muscles attached to the
bones of the hand and fingers are shown below
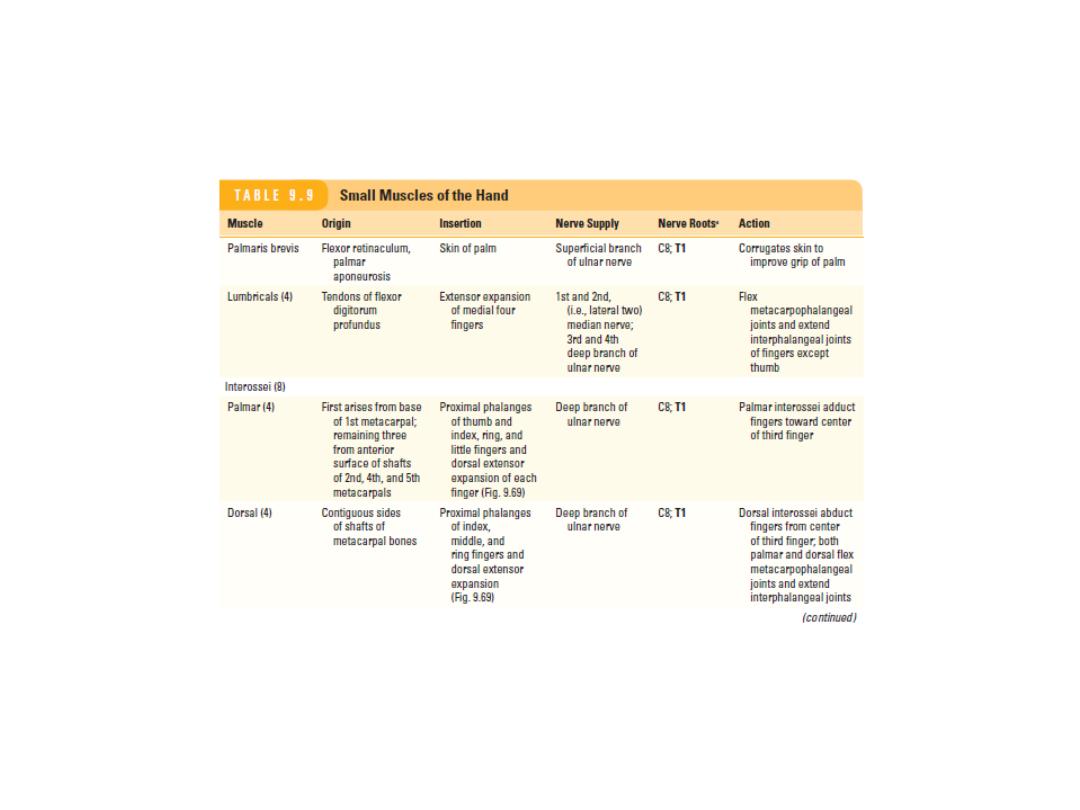
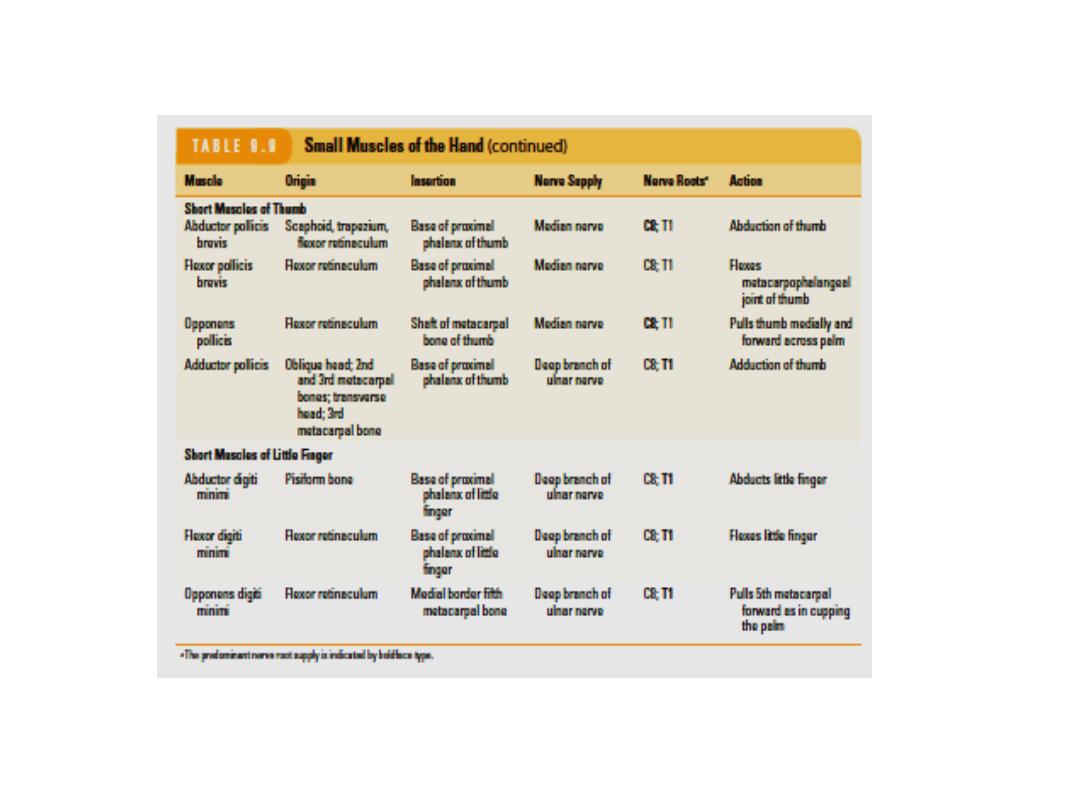
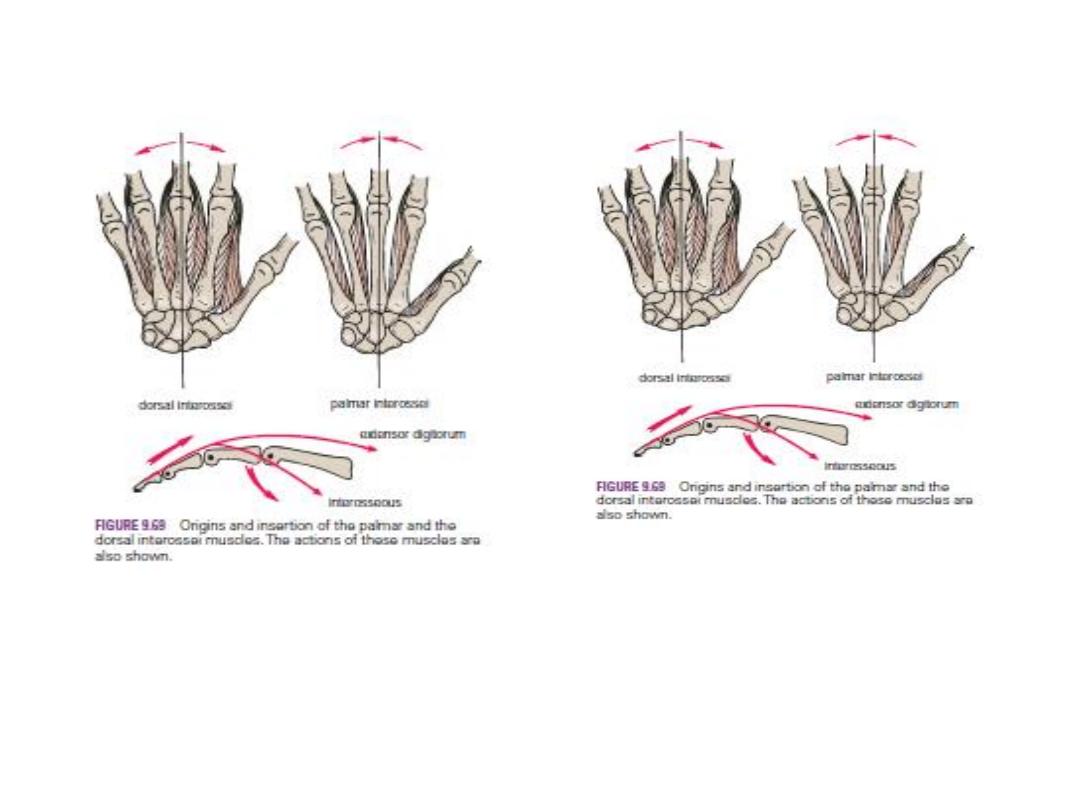
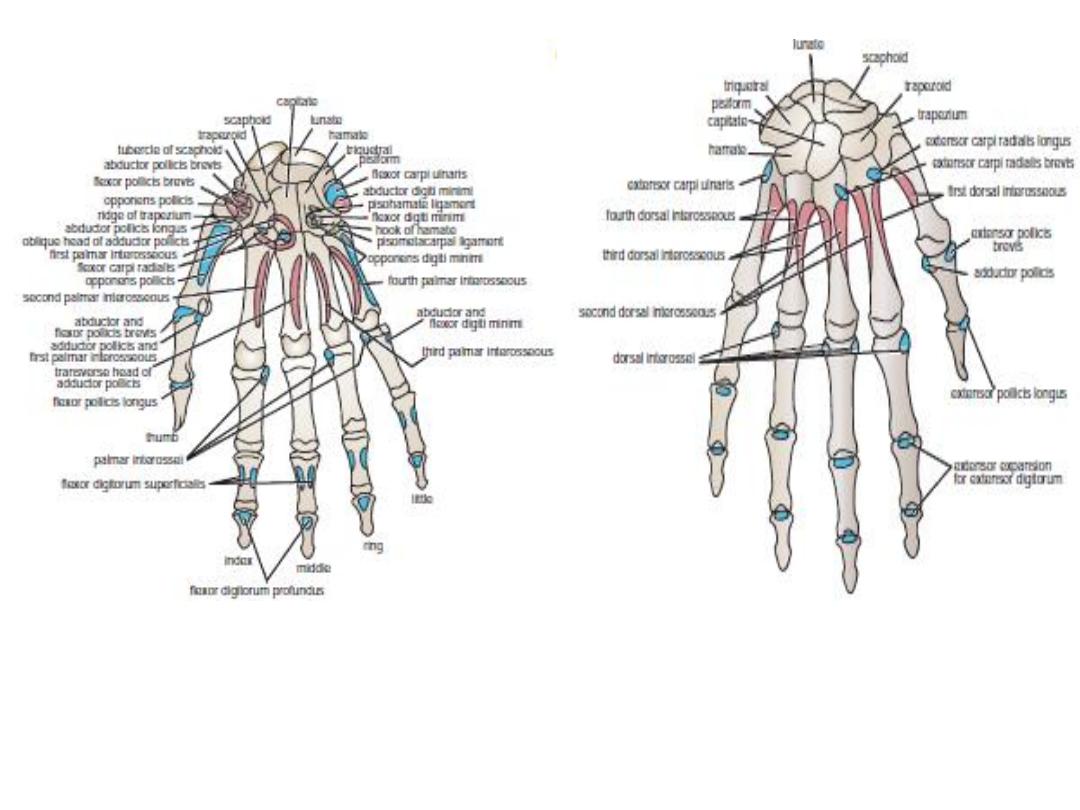
Important muscular attachments to the
anterior surfaces of the bones of the hand.
Important muscular attachments to the
posterior surfaces of the bones of the hand.
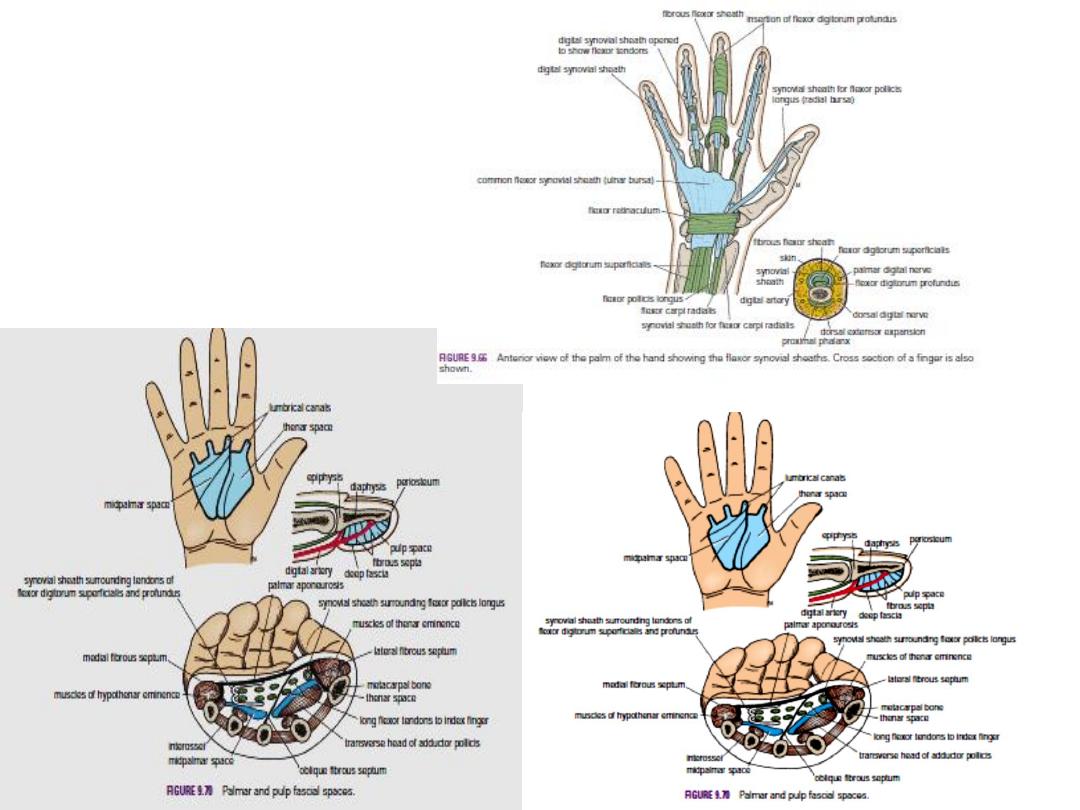
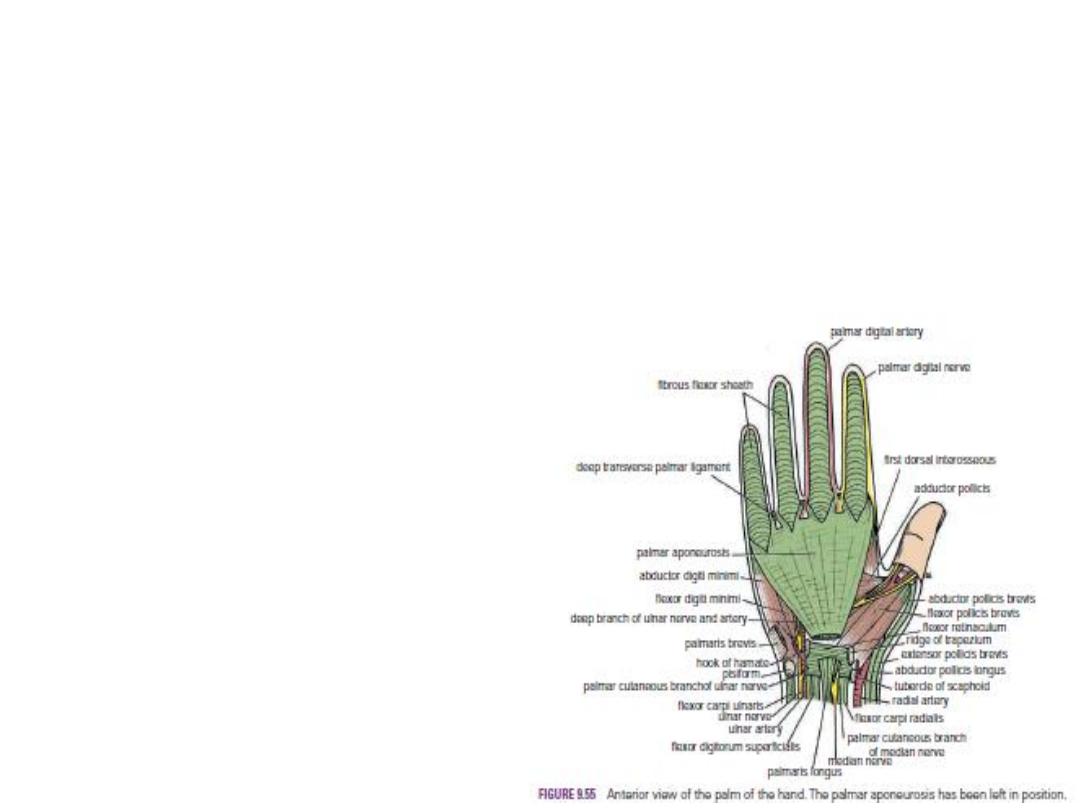
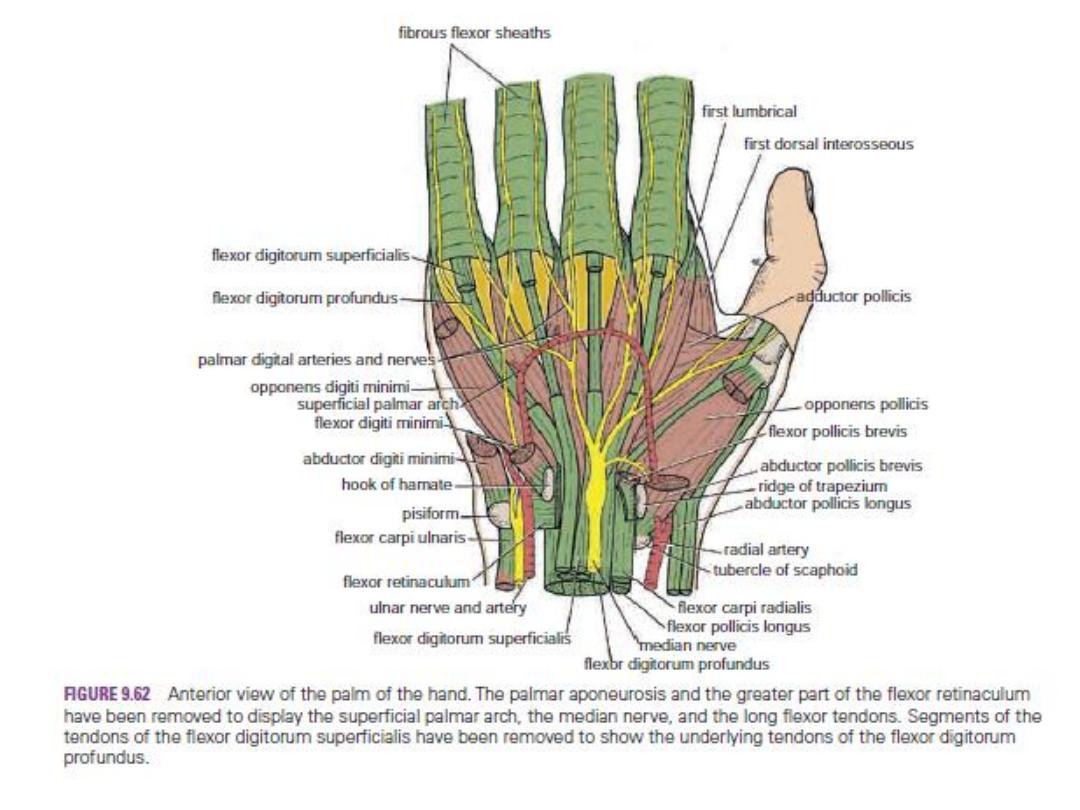
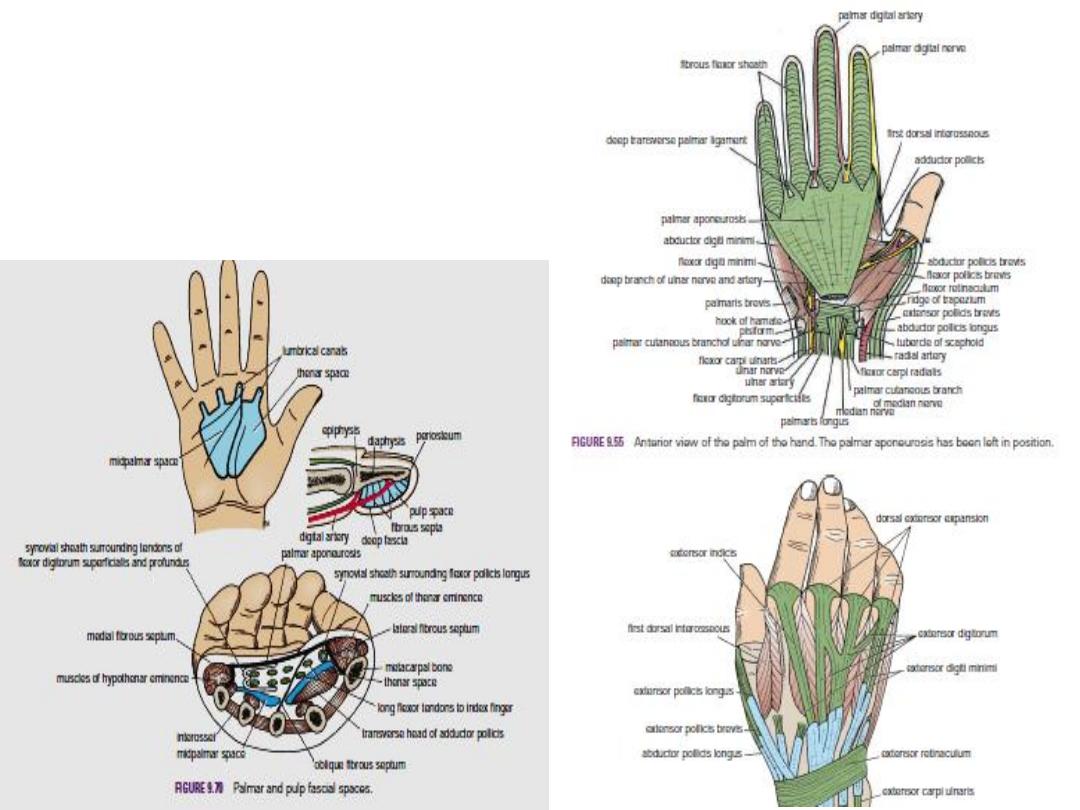
The Palmar Aponeurosis
The palmar aponeurosis is triangular and occupies the central area of the palm. The apex of is
attached to the distal border of the flexor retinaculum and receives the insertion of the
palmaris longus tendon. The base of the aponeurosis divides at the bases of the fingers into
four slips. Each slip divides into two bands, one passing superficially to the skin and the other
passing deeply to the root of the finger; here each deep band divides into two, which diverge
around the flexor tendons and finally fuse with the fibrous flexor sheath and the deep
transverse ligaments.
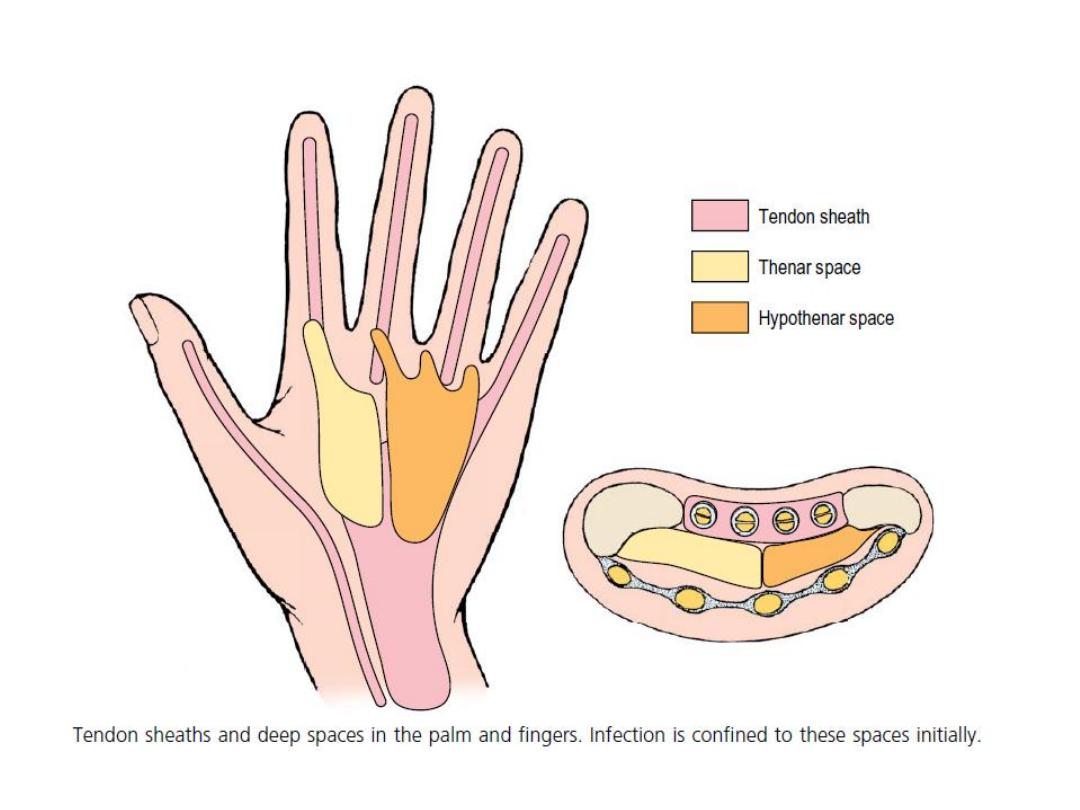
The medial and lateral borders of the
palmar aponeurosis are continuous
with the thinner deep fascia covering
the hypothenar and thenar muscles.
From each of these borders, fibrous
septa pass posteriorly into the palm
And take part in the formation of the
palmar fascial spaces.
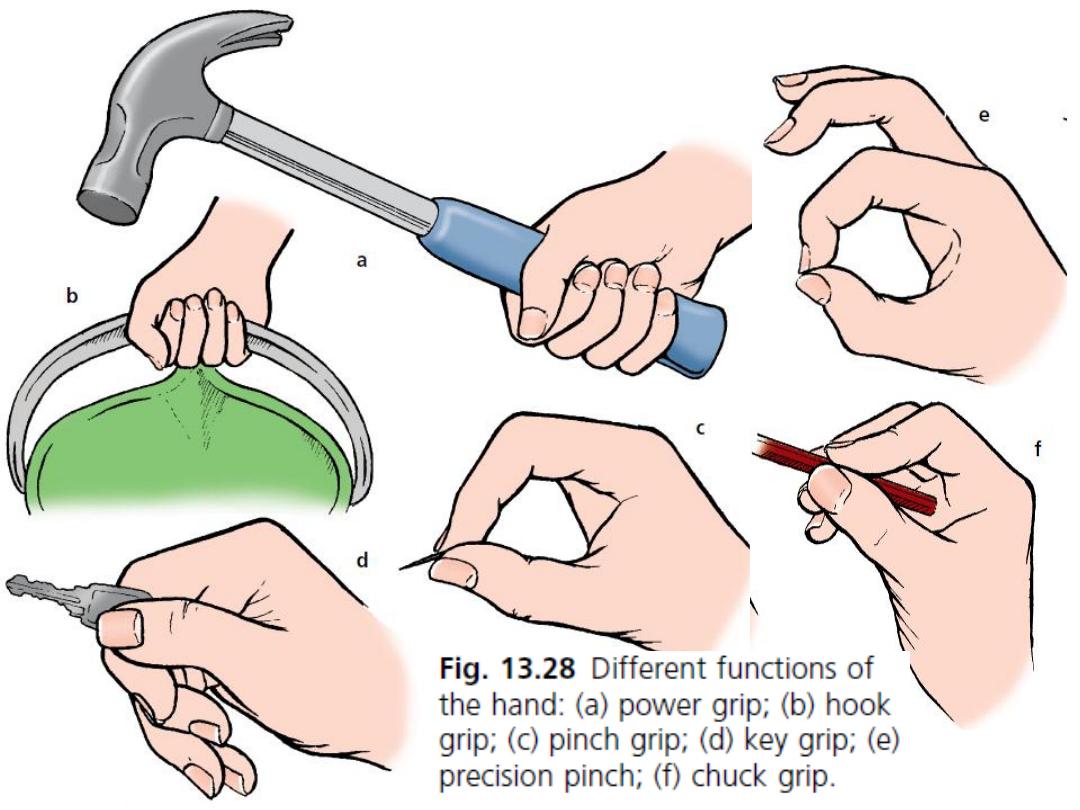
The function of the palmar aponeurosis
is to give firm attachment to the overlying
skin and so improve the grip and to protect
the underlying tendons.
Injuries to the Bones of the Hand
-
:
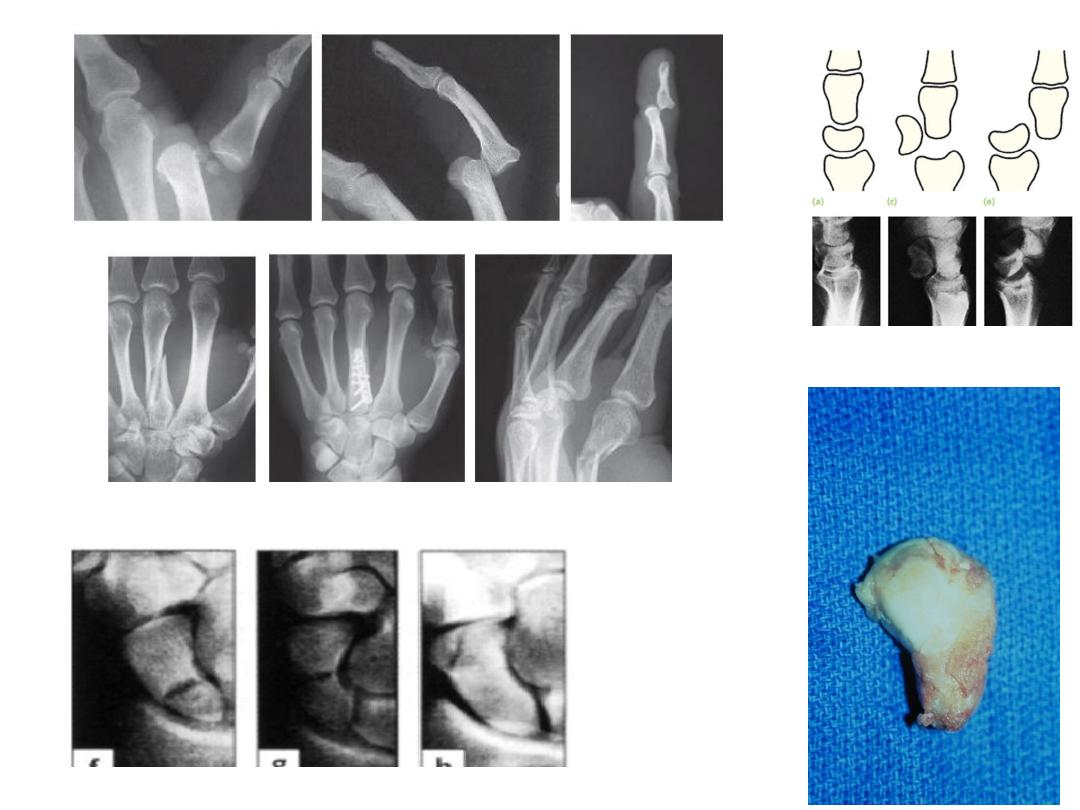
Fracture of the scaphoid bone
is common in young adults; unless treated effectively, the fragments will not unite,
and permanent weakness and pain of the wrist will result, with the subsequent
development of osteoarthritis. The fracture line usually goes through the narrowest
part of the bone. The blood vessels to the
scaphoid enter its proximal and distal ends, a fracture deprives the proximal fragment
of its arterial supply, and this fragment undergoes avascular necrosis.
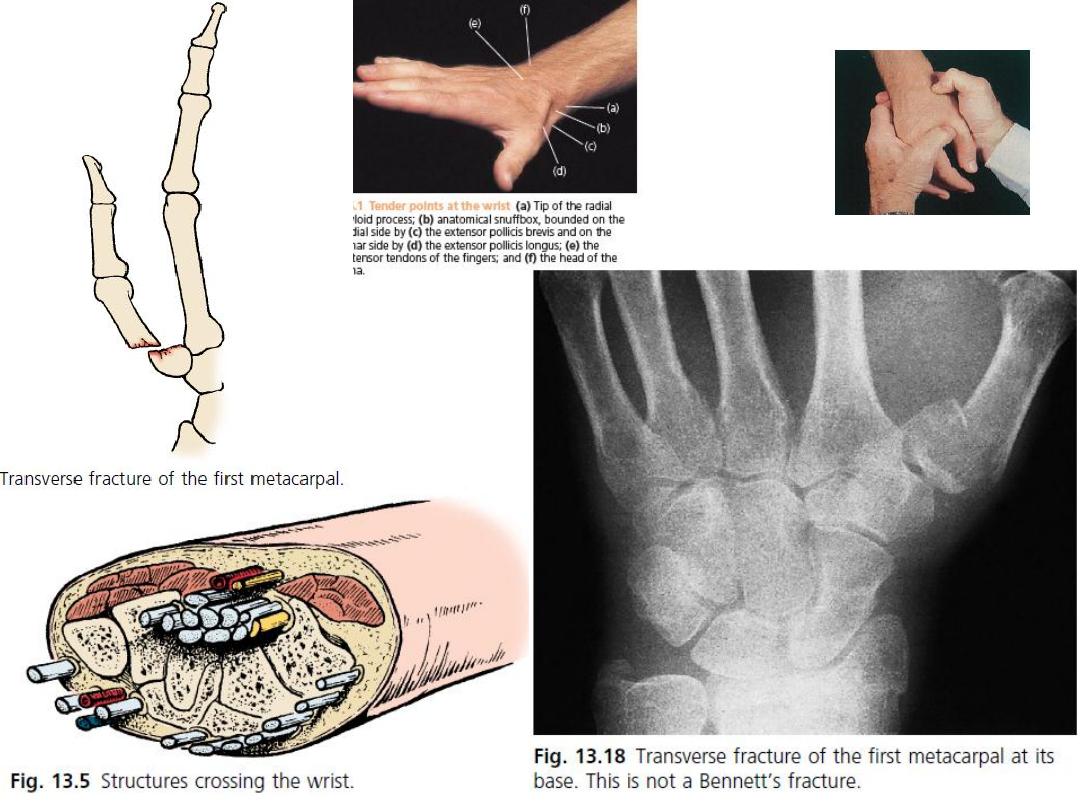
Deep tenderness in the anatomic snuffbox after a fall on the
outstretched hand in a young adult makes one suspicious of a fractured scaphoid.
Dislocation of the lunate bone occasionally occurs in young adults who fall on the
outstretched hand in a way that causes hyperextension of the wrist joint. Involvement
of the median nerve is common.

Fractures of the metacarpal bones can occur as a result of direct violence, such as the
clenched fist striking a hard object.The fracture always angulates dorsally. The “boxer’s
fracture”commonly produces an oblique fracture of the neck of the fifth and sometimes the
fourth metacarpal bones. The distal fragment is commonly displaced proximally, thus
shortening the finger posteriorly.
Bennett’s fracture is a fracture of the base of the metacarpal of the thumb caused when
violence is applied along the long axis of the thumb or the thumb is forcefully abducted. The
fracture is oblique and enters the carpometacarpal joint of the thumb, causing joint instability.
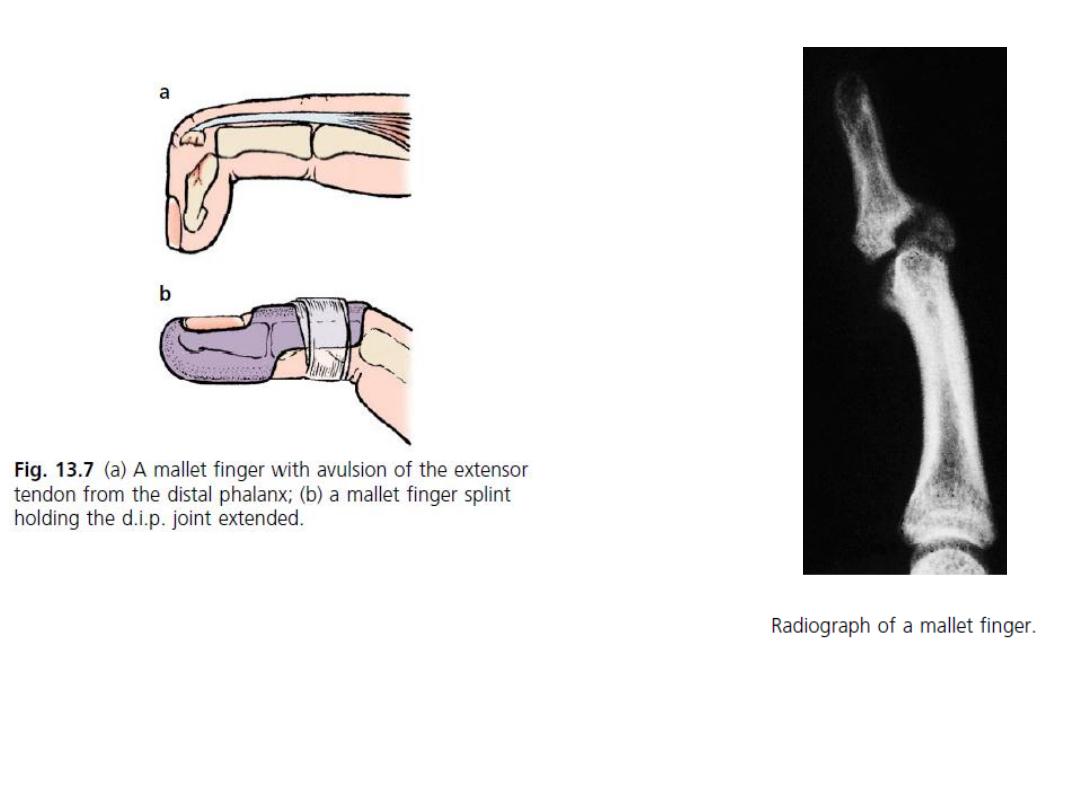
Fractures of the phalanges are common and usually follow direct injury.


THANK YOU
Dr. Jamal Al-Saidy
Assistant Professor and Consultant Orthopaedic Surgeon