GROUP D MKK DRAINS AND GALL BLADDER EXAMINATION
Dr. mohanad
Drains\
Indications
Surgical drains are used in a wide variety of different types of surgery
the intention is to decompress or drain either fluid or air from the area of surgery
To prevent the accumulation of fluid (blood, pus and infected fluids).
To prevent accumulation of air (dead space).
To characterize fluid (for example, early identification of anastomotic leakage)
To remove existing abnormal collections of fluid, blood, pus, air
RX in any abscess is incision and drainage
Types of drain
1 – open drain:
gauze
,
corrugated
2 – close drain: tubes draining, sumb drain,
Complication of drains
1. Hemorrhage
2. Injury to the nearby structure
3. Obstruction
4. Infection
5. Slipping or dislodgment of the drain
6. Incisional hernia
7. Kinking
Risk of reoccurrence of DVT increase in
1. Def of c,s protein
2. Elderly
3. Obesity
4. Pelvic surgery
5. Fracture surgery
GROUP D MKK DRAINS AND GALL BLADDER EXAMINATION
GA no C.I in case of operation in epileptic patient
GA contra indicated in upper respiratory tract infection
Q: what is the time requires for removing of stitches in post-operative patient
Abdominal stitches removed after (7-10 days)
Head stitches (5 days)
Leg stitches (12 days)
Back stitches (14 days)
Gall stones
Right hypochondriam pain, dyspepsia, flatulence, radiation to the back (biliary colic)
Types
1.
Cholesterol stones: the occurrence affected by bile salt
2.
Pigmented (brown, black)
3.
Mixed
Bile stone and acid prevent stone formation, while cholesterol cause stone
Factors affecting the formation of gall stone
1. Obesity
2. Contraceptive pills
3. Defects motility in gall bladder
4. Abnormal function terminal ilium (previous surgery. disease)
5. Rapid weight loss
6. High caloric intake
7. Five - f – fairy, fat, female, forty and fertile
Examination of the gall bladder
1. General: jaundice, criteria chronic liver dis, ascites, anemia ………….
2. Inspection: if their abdominal distension (ascites), asymmetrical abdominal right hypocondrium, dilated
vein caput medusa, changing color of the skin, any previous scar and hernia.
3.
Palpation : superficial and deep palpation for tenderness and superficial or colonic
mass , not tender with mass in case CPD , tender abdomen with mass indicates gall
bladder (cholecystitis) , exception gall bladder mucocele palpable but not tender ,
murphy's sign press the
hand just below the costal margin, approximately mid-clavicular (this is
just above the gallbladder);
-Then instruct the patient to slowly breath in; A positive Murphy’s sign is identified when the
GROUP D MKK DRAINS AND GALL BLADDER EXAMINATION
patient stops breathing in due to pain -- this is caused by the move of the diaphragm pushing the
inflamed gallbladder into the palpating hand. A negative Murphy’s sign is identified when the patient
comfortable breaths all the way in without any pain -- in this case, the diaphragm pushes the non-
inflamed gallbladder into the palpating hand with nil changes in the patient’s level of comfort. A
positive Murphy’s sign often indicates Cholycystitis, where as a negative Murphy’s sign may suggest
pyelonephritis, and ascending cholangitis.
4.
Complication, cholangitis, pancreatitis due to alcohol, jaundice
5.
Management – CBC, US, (MRCP and ERCP) in case of sever complication not
always, admission, fluid, best analgesia (NSAID), or anti spasmotic buscopan,
antibiotic like metronidazole or third generation cephalosporin and these are
conservative treatment giving four weeks before the surgery to avoid surgical injury,
in experience doctors they make the surgery directly even if their risk of iatrogenic
injury
6.
Complication of the surgery: bleeding, slipping clips duct (bile leak, biliary
peritonitis) biliary fistula, iatrogenic injury to the surrounding organs, slipping stone
from G. Bladder to the bile duct, post cholesystomy syndrome, bile leak
7.
Bile leak: if major bile duct injury (800 – 1000cc/d) need reconstructive surgery if
mild (400 -600 cc/day) need conservative treatment only
8.
Another anomaly abscess, accessory cholecysto hepatic duct, atresia, choledocal cyst
(idiopathic), tumor (malignancy), CPD
Dr. Muslim mkk hernia/examination
Dr. Muslim
Hernia:
- abnormal protrusion of content through abnormal opening
common sites
- inguinal canal usually obliterated and weak
- Umbilicus mostly because ascites
- Femoral canal
- Incisional hernia after surgery
Hernia consist of
1 - sac (fundus, body, neck of the sac)
2 - covering
3 - content
Generally divided into
1- reducible hernia
2- irreducible hernia (omentum , short segment of bowl)
3- obstructive hernia: - obstruction of the organs, movable content e.g. omentum, transvers
. colon, sigmoid, small bowl, fimbriae, and ovary
4- strangulated hernia
5- inflamed hernia
6- rechtor hernia: part of the wall will be herniated, not associated with obstruction except in
advance stages may cause obstruction, diarrhea is common
* most common hernia inguinal and femoral hernia
Inguinal hernia divided to direct and indirect
Indirect Inguinal Hernias
This classification of hernia is the more common. It has a congenital origin
– due to the
failure of the processus vaginalis to regress.
The peritoneal sac enters the inguinal canal via the deep inguinal ring. The degree to
which the sac herniates depends on the amount of processus vaginalis still present.
As the sac moves through the inguinal canal, it acquires the same three coverings as
the contents of the canal.
Dr. Muslim mkk hernia/examination
Direct Inguinal Hernias
In contrast to the indirect hernia, this is acquired in origin, due to weakening in the
abdominal musculature.
The peritoneal sac originates from an area medial to the epigastric vessels and bulges
into the inguinal canal via the posterior wall.
Inguinal hernia is more common in male than female
Grade of inguinal hernia
1. Bubonocid hernia
2. Funicular hernia
3. Scrotal hernia (complete)
Femoral hernia
: - Defect occurs below and medial to the femoral V.A.N and lateral to the
pubic symphysis and it common in female than male
During examination
1- the most important part of hernia ex, will be cough impulse
in inspection in any abdominal examination should ask about cough impulse in standing and
supine position
common hernia – inguinal, femoral, and epigastric hernia -
- In standing position cough impulse positive in these D.D but they are rare like pulging
varicose vein, psoas abscess (abscess behind psoas muscle)
2- the cough reducible or irreducible, in supine position if return to normal after coughing it is
reducible if not irreducible
Positive cough impulse = inguinal hernia until prove other wise
Negative cough impulse = other types of hernia like obstructive hernia
Differentiation between direct, in direct and femoral hernia using three finger test -
Zieman's
technique Index finger
- or invagination test
(old way)
How to differentiate between inguinal hernia and scrotal hernia
- If return may be inguinal hernia if not may indicate scrotal hernia or hydrocele
And to differentiate between scrotal hernia (complete hernia) and hydrocele by three steps
- Reducibility
- Scrotal hernia cannot get above while hydrocele can get above it
- Translumination test
Dr. Muslim mkk hernia/examination
D.D of hernia
- lymph node
- pus, abscess
- lipoma
Complication of intestinal obstruction
1. Vomiting
2. Constipation
3. Distention
4. Colic pain
5. Dehydration
In men, the spermatic cord passes through the inguinal canal, to supply and drain the
testes. In women, the round ligament of uterus traverses through the canal.
Boundaries of inguinal canal
The inguinal canal is made up of:
Anterior and posterior walls
Superficial and deep rings (openings)
Roof and floor (or superior and inferior walls)
We shall go through each component in turn.
The anterior wall is formed by the aponeurosis of the external oblique, and reinforced by the
internal oblique muscle laterally.
The posterior wall is formed by the transversalis fascia.
The roof is formed by the transversalis fascia, internal oblique and transversus abdominis.
The floor
is formed by the inguinal ligament (a ‘rolled up’ portion of the external oblique
aponeurosis) and thickened medially by the lacunar ligament.
The mid-inguinal point is halfway between the pubic symphysis and the anterior
superior iliac spine. The femoral artery crosses into the lower limb at this anatomical
landmark.
The midpoint of the inguinal ligament is exactly as the name suggests. The inguinal
ligament runs from the pubic tubercle to the anterior superior iliac spine, so the midpoint
is halfway between these structures. The opening to the inguinal canal is located just
above this point.
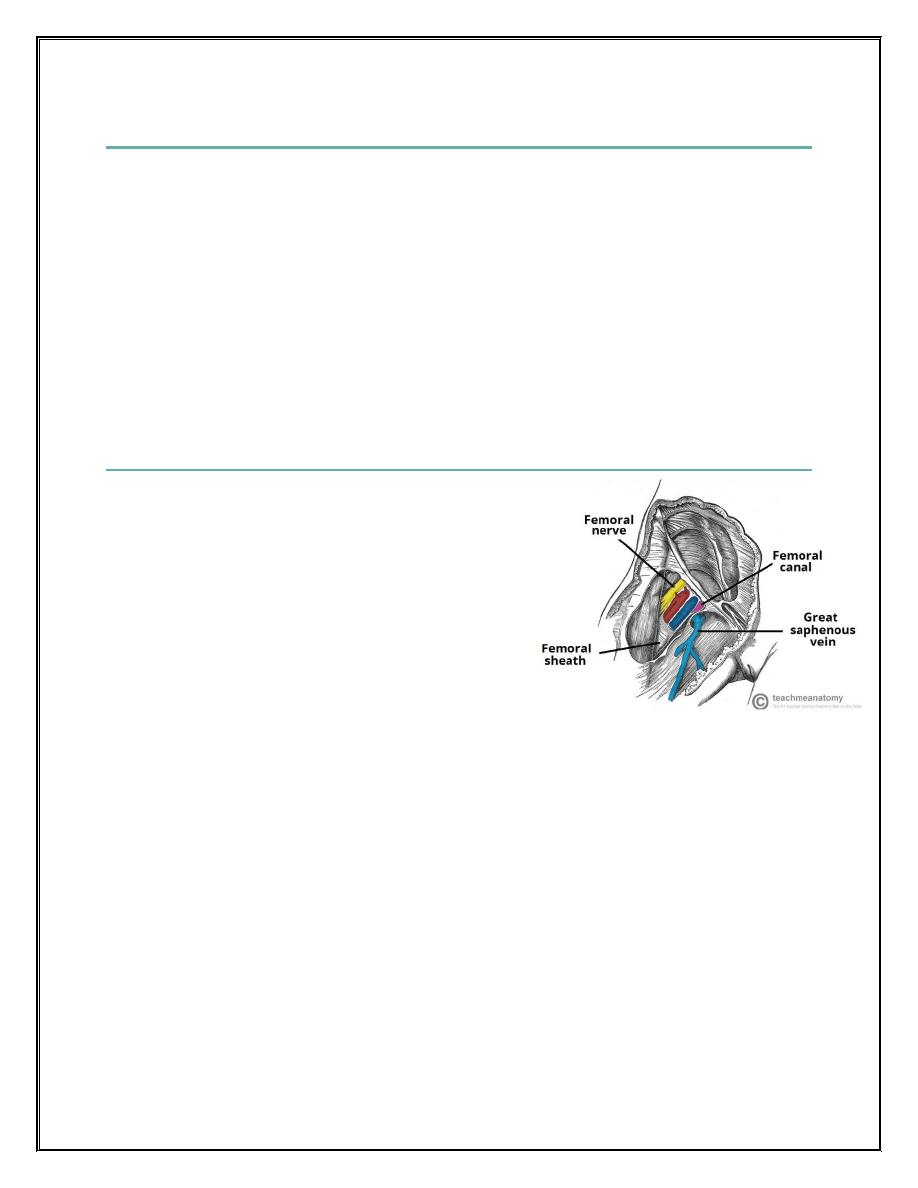
The femoral canal is an anatomical compartment, located in the anterior thigh. It is the smallest
and most medial part of the femoral sheath. It is appr
oximately 1.3cm long.
Dr. Muslim mkk hernia/examination
Borders of femoral canal
The femoral canal is located in the anterior thigh, within the femoral triangle. It can be
thought of as a rectangular shaped compartment.
It has four borders and an opening:
Medial border
– Lacunar ligament.
Lateral border
– Femoral vein.
Anterior border
– Inguinal ligament.
Posterior border
– Pectineal ligament, superior ramus of the pubic bone, and the pectineus
muscle
The opening to the femoral canal is located at its superior border, known as the femoral
ring. The femoral ring is closed by a connective tissue layer
– the femoral septum.
This septum is pierced by the lymphatic vessels exiting the canal.
Contents
The femoral canal contains:
Lymphatic vessels
– draining the deep inguinal
lymph nodes.
Deep lymph node
– the lacunar node.
Empty space.
Loose connective tissue.
The empty space allows distension of the adjacent
femoral vein, so it can cope with increased venous
return, or increased intra-abdominal pressure.
Most common questions at the examination in the hospital
1. Degree of hernia , or its type
2. Grading of inguinal hernia
3. Inguinal canal content, deep ring and superficial ring
4. Wall of inguinal canal
5. Femoral canal content
Group D MKK anorectal diseases
Dr. ali kadhim
History
1. Name
2. Age
3. Sex
4. Religion: some relation to high consumption of alcohol
5. Occupational status:
6. Chief complain: what is the patient say
7. History of present illness: asking about pain its sites, radiation, severity, relieving factor,
aggravating factor. ask also about the bowl motion, if there are fever and palpitation
and others associated phenomena
8. Review of systems: - review of system – GIT, Respiratory, CVS, CNS, GUT,
Musculoskeletal system
9. Past medical history: diabetic and hypertension
10. Past surgical history: if there are any previous surgery or previous hernia may reoccur
11. Drug history: allergy to specific drug such as penicillin and steroid
12. Social history: smoking and alcohol
13. Family history: hereditary disease, if their death in father or mother
Review of systems
1. GIT: - Constipation, vomiting
2. Respiratory: dyspnea, cough, sputum and wheezing
3. CVS: Edema cyanosis
4. CNS: headache, dizziness
5. GUT: dysuria, hematuria
6. Musculoskeletal system: joint pain
Anorectal disease
Rectum about [
12 cm ] long while anal canal [ 4 cm] in neonate [2cm]
The rectum is retro and intraperitoneal organ
The upper 1/3 of the anterior rectum is covered by peritoneum
but the lower third of rectum devoid from the peritoneum
The rectum lined by columnar epithelium while the anal canal [ start from anorectal ring to the anal verge]
consist from upper part columnar epithelium and lower part squamous epithelium
Blood supply: inferior mesenteric artery [ to the rectum and anal canal]
Group D MKK anorectal diseases
Symptoms appears in patient with anorecatal disease
1. Pain
2. Bleeding
3. Anal discharge
4. Mass lesion
5. Pruritus anal
The patient may complain from pain during defecation, bleeding during defecation or pre defecation
or after defecation
Upper GIT bleeding [melena] [black color stool]: caused by DU, Gastric ulcer, gastric CA, lower
esophageal varices and injury to the wall of small bowl
Fresh blood [ hematochezia] lower GIT bleeding like angioma , hemorrhoids
Anal discharge: caused by rectal CA, hemorrhoid, anal CA, adenoma, rectal polyp, infection
Mass lesion: in hemorrhoid, anal CA, rectal CA,
Pruritus anal: warms, hemorrhoid, mucous discharge
PR examination consist of
1. inspection
2. palpation
3. PR and
4. proctoscopy
1-inspection we look to the anal verge, natal cleft and
gluteal region, looking for any scar, orifice or
fistula, any skin tag related to fissure, for bile hemorrhoid, for any abnormal puss, scratch mark
[especially in children or in elderly], any change in color due to [erythema, cellulitis of ano rectal
region in diabetic pt. and old patient or patient subjected to ano rectal dis]
2- palpation: you should have [ gloves, xylocaine with cotton] with you during examination, we
palpate both gluteal region for any hardness, any masses, for any bile hemorrhoid, skin tag
presentation
And after that we make PR examination to the patient,
3- PR examination is well indicated in hemorrhoid, fistula in ano [ to check the internal orifice], benign
prostatic hyperplasia, prostatic nodule
PR examination is also important to determine if painful or painless, if the anal verge tight or spatulas,
if there palpable masses like sub mucous abscess for rectal CA, Anal canal CA present as a mass
legion, for internal orifice of fistula in ano, also it is palpable o PR
After PR examination we take piece of stool looking if there black color, or dry stool,
Group D MKK anorectal diseases
4- Proctoscopy: contra indicated if there are fissure in ano or if there any pain or in anal stenosis, the
idea of this instrument to find if there any bleeding, ulceration, infection, internal hemorrhoid
If we used proctoscopy and we found lower rectal mass, what are the next step?
Answer: sigmoidoscopy. [ two type rigid and flexible type] rigid sigmoidoscopy consists
of [20-25cm]
it passes through anal canal
– rectum - sigmoid to the colon to look for any mass, ulceration, any
pathology while the flexible sigmoidoscopy about [60cm] reaching left colon to the splenic flexure
looking for diverticula, etc.
Contra Indication for PR examination
1. Anal stenosis
2. Sever pain due to fissure in ano
Relation to the anal canal
Post:
coccyx and sacrum
Laterally: ischiorectal fossa and fat content of the ischiorectal fossa
Ant: different in male from female
Notice: examination differ if the examiner asks about general examination or abdominal
examination or PR examination
Before any examination we must take permission, position, Abdominal examination in supine
position
PR Position either: knee elbow position, left lateral position or supine position
Dr. abd alhussein MKK group D
History
Diabetic foot
1. Permission
2. Do you have diabetes
3. When the D.M diagnosed
4. How was diagnosed as DM
5. What is the treatment was on
6. Type of Treatment now
7. Incidence of hypo/hyperglycemia
8. Have a follow up program
9. How start foot problem
10. Feeling of foot [ numbness -------]
11. Kind of treatment received
Grading of D.M
1. Grade -0- just erythema
2. Grade -1- skin and subcutaneous tissue involvement
3. Grade -2- skin +subcutaneous tissue +underlying structure [muscles]
4. Grade -3- involvement of bone
5. Grade -4- pregangre
6. Grade -5- gangrene
Treatment of diabetic foot
1. Control of blood sugar
2. Antibiotic
3. Surgical debridement
Dr. abd alhussein MKK group D
History of jaundice
1. Take permission, introduce yourself
2. Onset [ sudden, gradual]
3. Pain [ if he has abdominal pain or not
4. Fluctuation يجي ويروح
5. Progression
6. Duration
7. Fever, rigor
8. Loss of appetite
9. Loss of weight
10. Pruritus, itching [ became in obstructive j because bile salt accumulates in the skin]
11. Change in color of stool [ in obstruction = cloudy stool]
12. Change in color of urine [ in obstruction = tea color urine]
13. Medical history
14. Surgical history
15. Blood transfusion, drugs [ especially anesthetic drugs like halothane]
16. Family history
17. Social history [ smoking, alcohol]
18. Foreign travel [ risk of HIV infection]
T.S.B Clinical exam [ 2-2.5 mg/dl] to appear in the sclera.
Rates of hepatitis in blood transfusion [ HA = 0.3% , HB = 30% , HC = 3% ]
If the patient after surgery developed jaundice about [ 36 -48 h ] half of the jaundice remove after that 8%
every day until disappear after one week If the jaundice not disappear after one week this mean there are
another cause albumin combine with gamma bilirubin and its half-life 18 days to disappear In obstructive
jaundice [ T.S.B = 30-35 ]
Explain the reason that make T.S.B more than 40
1. Hemolysis
2. Renal insufficiency
3. Hepatospleenfistula
How to prepare patient with obstructive jaundice for surgery? We give vitamin k [ i.m], cannot given
him orally because cannot absorb it [ fat soluble] also cannot give to him i.v, it causes hemolysis
Causes of post-operative jaundice
1. Blood transfusion
2. Too much bleeding
3. Hematoma, absorption
4. Drugs [ anesthetic like halothane]
5. Injury common bile duct C.B.D
6. D.I.C [Disseminated intravascular coagulopathy]
Dr. abd alhussein MKK group D
History of breast lump
1. Permission and introduce yourself
2. Age
3. Lump site
4. Single or multiple
5. Onset of growth
6. Rate
7. Presence or absence of pain
8. Nipple discharge [ serous, green, milky, bloody]
9. Temperature, fever
10. Weight loss
11. Bone abdominal pain [ may be there a metastasis]
12. Arm swelling [ arm swelling due to obstruct lymphatic vessels, surgery destruct vessels]
13. Previous radiation or surgery
14. M.C history
15. Obstetric history
16. Family history [ breast tumor, ovary tumor]
17. Symptom of possible metastasis
Triple assessment of breast disease including – history – clinical examination – investigation
Investigation
Radiology: - ultrasound, mammogram and MRI
Pathology: - FNAC, tru-cut needle biopsy, incisional, excisional and mastectomy
Dr. abd alhussein MKK group D
Nipple discharge history
1. Permission
2. Type of nipple discharge [nature, bloody, milky, -----]
3. Color
4. Associated mass
5. Unilateral or bilateral breast
6. Single or multiple duct discharge [ 7-8 duct] the most serious single duct
7. Contraceptive use
8. Pain, tenderness
9. Fever
10. History of trauma
11. Family history
12. Age of pt.
How to differentiate between Paget disease and eczema of the nipple
1. In eczema affect lactating young female while in Paget dis affecting elderly
2. In eczema bilateral itching with vesicle while in Paget dis lateral no itching no vesicles
3. In eczema no underlying mass while in Paget dis there underlying mass
4. In eczema nipple intact, in Paget dis nipple involve
Postoperative fluid: - major operation
- First 24h = 2L [glucose water], why giving them G. water? because of the
anaesthetization of post-operative patient will have retention so G. water considered as
diuretic
- Second 24h = 2L g. water +1L normal saline
- Third day = 2Lg.water +1Lnormal saline + potassium 60ml daily
Parkland formula = 4ml *weight *percentage of burn
We give crystalloid in first 24h half amount at the first 8h and the remaining in the next 16h
Second day = 0.3ml *weight *%+daily requirement
Dr. abd alhussein MKK group D
history / dr. a abd alhussein
thyroid history / toxic goiter
1. Permission
2. Location of goiter
3. Duration
4. Change in size
5. Painless or painful
6. Intolerance to cold or hot environment [ hypo cannot bear cold, hyper cannot bear hot]
7. Anxiety, sleep disturbance
8. Palpitation
9. Diarrhea and constipation
10. Menstrual disturbance in female
11. Mischarage, fertility and abortion
12. Fever
13. sweaty palm
14. dry skin
15. Change in speech, voice
16. Respiratory change, dyspnea
17. Drug history especially anti thyroid
18. History of radiation exposed [ risk factor]
19. Past medical, special cardiac problem
20. Family history of goiter
Retrosternal goiter = repiratory obstruction
Pamperton test: asking the patient to rise his hand above the head for one minute it will cause
1. Dyspnea
2. Neck vein engorgement
3. Stridor
4. Cyanosis
Differential diagnosis for mass that move with swallowing
1. Pretracheal lymph node
2. Thyroglossal cyst
3. Sub hyoid bursa
4. extrinsic c a of larynx
5. Goiter
If the patient suffers from dyspnea [ cyanosis] after surgery, almost likely he has hematoma, and the drain
doesn’t working properly so opening the stitches and limiting the hematoma and prepare him for emergent
surgery
Dr. abd alhussein MKK group D
Type of incision:
collar incision
Common nerve injury: recurrent laryngeal nerve [ hoarseness of the voice] and external branch
of superior thyroid nerve [ the patient cannot elevate his voice] others non common nerve [
supraclavicular nerve] and [ transvers cervical nerve]
History of abdominal pain
1. Permission
2. Onset , duration
3. Location and severity of pain
4. Radiation [ acute cholecystitis pain radiated to the shoulder because they have the same
nerve supply c3, c4, c5
5. Time related to food [ in PU increase pain while in DU eating retire pain]
6. Aggravating and relieving factors
7. Associated fever and rigor
8. Nausea and vomiting
9. Change in bowl motion and stool
10. Weight loss
11. Past history and previous episode
12. Past surgical, medical history
13. Drug history
14. Jaundice
15. Social history
Q: how to differentiate between intra-abdominal pain or extra abdominal pain?
Answer: using carnet’s sign. the patient can be asked to lift the head and shoulders from
the examination table to tense the abdominal muscles. An alternative is to ask the
patient to raise both legs with straight knees.
A positive test increases the likelihood that the abdominal wall and not the abdominal
cavity is the source of the pain (for example, due to rectus sheath hematoma instead
of appendicitis).
A negative
Carnet’s sign is said to occur when the abdominal pain
decreases when the patient is asked to lift the head; this points to an intra-abdominal
cause of the pain.
Q: how to differentiate between intra and extra abdominal mass
Answer: the same test above if the mass disappears during contraction it will be intra-
abdominal mass if not will be extra
Group [ D] MKK Dr. Ali Abd Albaqi
Stone types
Urolithiasis
:
stone disease of the urinary system, occurs because of the chemical component of the urine
urine has special PH and specific conc.
There are saturation and super saturation state, in case of super saturation and the component cannot resolve
in urine this will cause crystallization
In urine, the PH is acidic [less than 4.5] and the ability to resolve these component will be very slow and
increase if the urine become alkaline, and this is the reason why we ask any patient with renal stone dis to
drink a lot of water for making dilution and increasing the ph. of urine
The accumulation of crystals will lead to the formation of stones, another theory indicates: there are a
component like the nucleus called [ Nagus] around it accumulate the crystals and lead to the formation of the
stones
The most common type of stone in our country [ infected stone] struvite stone
Types of stone
1. Calcium phosphate: very rare
2. Calcium oxalate [ more common]
3. Uric acid stone
4. MAP stone [ magnesium, ammonium and phosphate]
5. Cysteine stone
6. Indinavire stone [ very rare]
Calcium phosphate very rare stone because it will never happen unless there are structural problem or
physiological problem in your body like [ RTA] renal tubular acidosis
RTA: in ability of the kidney of the patient for acidification of urine
Cysteine stone: occurs in case of inborn error metabolism, it is a specific syndrome in children caused by in
ability of the liver to metabolize special type of amino acid, and there are four amino acid involved COLA [
cysteine, ornithine, glycine and arginine] and in this dis the cysteine doesn’t metabolize and appear in the
urine to form the stone
Calcium oxalate: control of calcium by renal and parathyroid gland hormones, oxalate metabolism in the liver
and the production in male more than in female. in some patient with short bowl syndrome the absorption of
oxalate will decrease, so the causes of calcium oxalate either increase in oxalate level or decrease in calcium
level, and to prevent the occurrence of these stones by giving citrate, the citrate combine with calcium and
prevent the connection between calcium and oxalate and to alkalination of urine
Uric acid stone: can be controlled by good hydration to the patient and alkalination of urine
Group [ D] MKK Dr. Ali Abd Albaqi
Types of stone according to radiolucency
1. Radio lucent
2. Radio opaque
3. Faint radio opaque
Radio opaque stone: anything contains calcium like calcium phosphate, calcium oxalate, struvite stone
Radio lucent: uric acid stone, xanthine stone
Faint radio opaque: cysteine stone can see it because it contains Sulphur
All must all types of stones can be identified by [CT-scan] except indinavir stone
Indinavir stone occurs in some patient taking drug for HIV dis.
[ MAP = struvite stone = infected stone]: come from chronic urinary tract. and called stag horn stone
Stone range from [ 4mm – 5cm] may occur in kidney, ureter and pelvic region
Signs and symptoms
1. Pain: if there are incomplete obstruction the pain will be moderate
2. Nausea, vomiting
3. Type of pain: if occurs in ureter the pain will be colicky in nature, sharp, continuous not relief by changing
the position
4. Fever: on case of infection
5. Pain in kidney dull in nature
Investigation
1. Urinalysis: RBCs
2. US [ detect 99% of renal cases]
3. IVU for radio lucent stones
Q: if we make IVU for a patient and we found obstruction, what are the D.D for this obstruction
1. Radiolucent stone
2. Clot
3. Tumor
4. Sluffed papilla
Management
1. Cannula
2. Analgesia
3. NSAID if there are no c.i for it
4. Alpha blocker [ smooth muscle relaxant]
5. Anti-emetics
Group [ D] MKK Dr. Ali Abd Albaqi
Treatment
if the stone in the kidney
1. Less than 1 cm by ESWL only
2. [ 1 – 2 cm] double j insertion then to ESWL
3. More than 2 cm percutaneous nephrostomy, the position will be lateral position and
the incision called [ flank incision]
The layers opened through surg.
1. Skin
2. Subcutaneous tissue
3. External oblique m.
4. Internal oblique m
5. Latissimus dorsi m
6. Serratus ant and post
7. Pyelotomy
Contraindication of ESWL
1. Bleeding tendency
2. Pregnancy [ absolute c I]
Side effects of ESWL
1. Hematuria
2. Hematoma
3. Destruction of renal tissue
4. Hypertension
5. D.M [ very rare]
Types of ESWL
1. Electromagnetic
2. Hydroelectric
3. Basoelectric
Shock Wave Lithotripsy (SWL) is the most common treatment for kidney stones in the U.S. Shock
waves from outside the body are targeted at a kidney stone causing the stone to fragment. The stones
are broken into tiny pieces. lt is sometimes called ESWL: Extracorporeal Shock Wave Lithotripsy.
These are what the words mean:
extracorporeal: from outside the body
shock waves: pressure waves
lithotripsy (the Greek roots of this word are "litho" meaning stone, "tripsy" meaning crushed)
Group [ D] MKK Dr. Ali Abd Albaqi
So, SWL describes a nonsurgical technique for treating stones in the kidney or ureter (the tube
going from the kidney to the bladder) using high-energy shock waves. Stones are broken into
"stone dust" or fragments that are small enough to pass in urine. lf large pieces remain, another
treatment can be performed
Double j: length [ 15 – 25 cm] diameter [ 3,4,5,6,8] according to the patient
Group D MKK thyroid
Thyroid / history /examination
history / dr. a abd alhussein
1. Permission
2. Location of goiter
3. Duration
4. Change in size
5. Painless or painful
6. Intolerance to cold or hot environment [ hypo cannot bear cold, hyper cannot bear hot]
7. Anxiety, sleep disturbance
8. Palpitation
9. Diarrhea and constipation
10. Menstrual disturbance in female
11. Mischarage, fertility and abortion
12. Fever, sweaty palm and dry skin
13. Change in speech, voice
14. Respiratory change, dyspnea
15. Drug history especially anti thyroid
16. History of radiation exposed [ risk factor]
17. Past medical, special cardiac problem
18. Family history of goiter
Retrosternal goiter: symptoms including dyspnea, dysphagia, obstruction of venous return at the thoracic
inlet from a substernal goiter results in a positive Pemberton’s sign—facial flushing and dilatation of cervical
veins upon raising the arms above the head for [ 1 min], causing [dyspnea, neck vein ingorigment, stridor,
cyanosis]
Recurrent nerve paralysis (rare)
Treatment:
In obstructive symptoms and associated with thyrotoxicosis usually not treated with anti-thyroid drug or
radioiodine because it may cause enlarge of goiter.
Surgical operation through neck incision rarely need sternatomy
D.D FOR mass that move with swallowing
1. Pre tracheal lymph node
2. Thyroglossal cyst
3. Sub hyoid bursa
4. Extrinsic CA of larynx
5. goiter
If the patient suffers from dyspnea [ cyanosis] after surgery, almost likely he has hematoma, and the drain
doesn’t working properly so opening the stitches and limiting the hematoma and prepare him for emergent
surgery
Group D MKK thyroid
Type of incision:
collar incision
Common nerve injury: recurrent laryngeal nerve [ hoarseness of the voice] and external branch
of superior thyroid nerve [ the patient cannot elevate his voice] others non common nerve [
supraclavicular nerve] and [ transvers cervical nerve]
Dr. alaa / thyroid examination
Review to the history
During history ask the patient about previous drug, if he taking drug specific for the thyroid gland or
not, radiation therapy, chemical therapy, if there previous surgery or not, all these are signs due to
hyperthyroidism
If there are numbness in his finger [ carpal tunnel syndrome] if female, ask about menstrual
irregularity
If the patient says that there is palpitation, tachycardia, increasing appetite, cold region in the body,
increase in body weight all these are signs and symptom of toxic goiter [ hyperthyroidism]
We should examine the patient to see if there any abnormalities because it may be toxic goiter,
graves’ disease, diffuse toxic goiter, may be toxic nodule, multinodular goiter or due to the
malignancy due to certain disease
Examination of the thyroid
1. Inspection: to see if there any swelling of the thyroid gland, dilated veins or not, looking for
any previous scar. if there swelling we should describe it like for example :-
there are swelling in the right side of the thyroid gland or at the left , and the swelling about
[ 5-6cm ] and the skin above the swelling it normal , no dilated veins and should ask the
patient to take water to see if it move with swallowing or not, Pemberton’s sign—
facial flushing and dilatation of cervical veins upon raising the arms above the head
for [ 1
min ] and this examination specific for retrosternal goiter which cause facial flushing of the face and
engorgement of the vein of the neck
2. Palpation: we have two procedures for palpation of the thyroid gland either from the front
or from behind, usually from behind
i) First thing take permission from the patient
ii) Ask the patient if there any tenderness
iii) If we start palpation of the left side we press in the right side to make the left side more
prominence and checking the site, nodularity, attachment to the skin or not, no
palpable swelling
Group D MKK thyroid
Q: if the left side of the gland normal should I examine the regional lymph node or note
Ans: you should examine the regional lymph node [ preauricular, postauricular, sub mental, submandibular,
cervical, superficial cervical, deep cervical and supraclavicular lymph node] because of the lateral appearance,
may be the thyroid normal but there are cervical lymph node enlargement and when sending the patient to
the FNA to find that he has papillary carcinoma of the thyroid gland.
Then you have to go to the other side and where the swelling is found you must make good description
about it like for example there is swelling about [2cm] in the right lobe of the gland
In any swelling there are three important things
1) Not comprisable: swelling of the artery when pressure on it, it will disappear
2) Not reducible [ mean not hernia]
3) Not pulsated [ not aneurysm]
And see if the swelling move with the skin or not, if attached to the underlying structure and ask the patient to
swallow to see if it move with swallowing or not, and finally examine the regional lymph node
3. percussion: we have to make percussion to see if the patient has retrosternal goiter or not so we make
percussion in the [ sternum] it must be resonance because there are lung and air in this region in normal state
but if it became dullness it means soft tissue in this region and this is called retrosternal goiter
4. auscultation: we need auscultation in case of toxic goiter, because in toxic goiter there are over
activity, and need more blood flow in superior thyroid artery [ carotid artery] so we auscultate in the upper
lobe of the thyroid gland to find the blood push strongly on the wall of the blood vessels
Now we finished examination of the thyroid gland and need to describe if the patient in the euthyroid,
hyperthyroid [toxic goiter] or hypothyroidism
If asked from you examine the thyroid of the patient:
1) General examination
2) Thyroid examination
3) Signs of the hyperthyroidism
4) Then ask the patient questions related to the condition like, appetite, allergic history, past
history, carpal tunnel, surgical history and bowl
If the patient has pain [ tenderness] it must likely inflammation [ thyroiditis] and also you need to do the
examination gently
Some notes about abdominal examination from dr. alaa
1) During abdominal examination we start from the nipple to the mid-thigh
2) Why we start from the nipple or second intercostal space [In female]. Ans: because there are some
conditions related to the abdomen like gynecomastia in male because of high level of estrogen due to liver
abnormalities
Group D MKK thyroid
3) Why we expose the patient to the mid-thigh to check the genitelia to find if there any abnormalities,
because some abnormalities in genitelia may affect the abdomen like [ extended testis, obstructive hernia,
tumor of the testis because the lymphatic drainage of the testis goes to the para aortic region so it causes
enlargement and compression on the inferior vena cava
4) Palpation start away from the region of the pain
5) If there cannula the needle put in median cupital vein
6) Spleen level in ribs [9,10,11]
7) Examination of the spleen usually started from the umbilicus because the enlargement of the spleen
will go diagonally to the umbilicus
8) Palpation during inspiration the diaphragm will be low level and the organ will hit your finger and during
each inspiration you should press to see if there any tenderness
9) Not enlarge or not palpable spleen: palpable spleen when the size more than double but not enlargement
may be one and half more than the normal size but not palpable
10) How to differentiate between the enlargement of the spleen and enlargement of the kidney clinically
Answer:
1) Enlargement of the spleen goes diagonally while in the kidney vertically
2) The spleen has splenic notch while the kidney has no notch
3) The spleen cannot get above it [ between the spleen and costal margin] while the kidney can get
above it [ because it is retro peritoneum]
4) On percussion the spleen dull because tissue while kidney resonance because the colon above it
5) The kidney pallotable while spleen not
When you palpate organ
1) Press during inspiration
2) Looking to the patient face
3) To see if it palpable or not then you must make a description
Murphy’s sign: enlargement of the gall bladder [ acute cholecystitis], the finger below the costal margin and
ask the patient to take deep inspiration you will find the patient stop in half inspiration
Grid iron incision layers
Skin - Subcutaneous tissue - Superficial layer of superficial fascia - Deep layer of superficial fascia - Deep fascia -
External oblique m - Internal oblique m - Transvers abdominal m - Peritoneum
How to go directly to the appendix
First find the cecum [ has taenia coli - longitudinal fiber] and at the end of the cecum to find the ilium, the end
of the cecum is the base of the appendix
During surgery of appendicitis and when we reach to the appendix and found it normal, you become happy or
sad? Very sad because there are another pathology causing these symptoms such as diverticulum in male and
ovarian cyst in female.